
Manufacturable 32-Channel Cochlear Electrode Array and Preliminary Assessment of Its Feasibility for Clinical Use


Abstract
1. Introduction
2. Materials and Methods
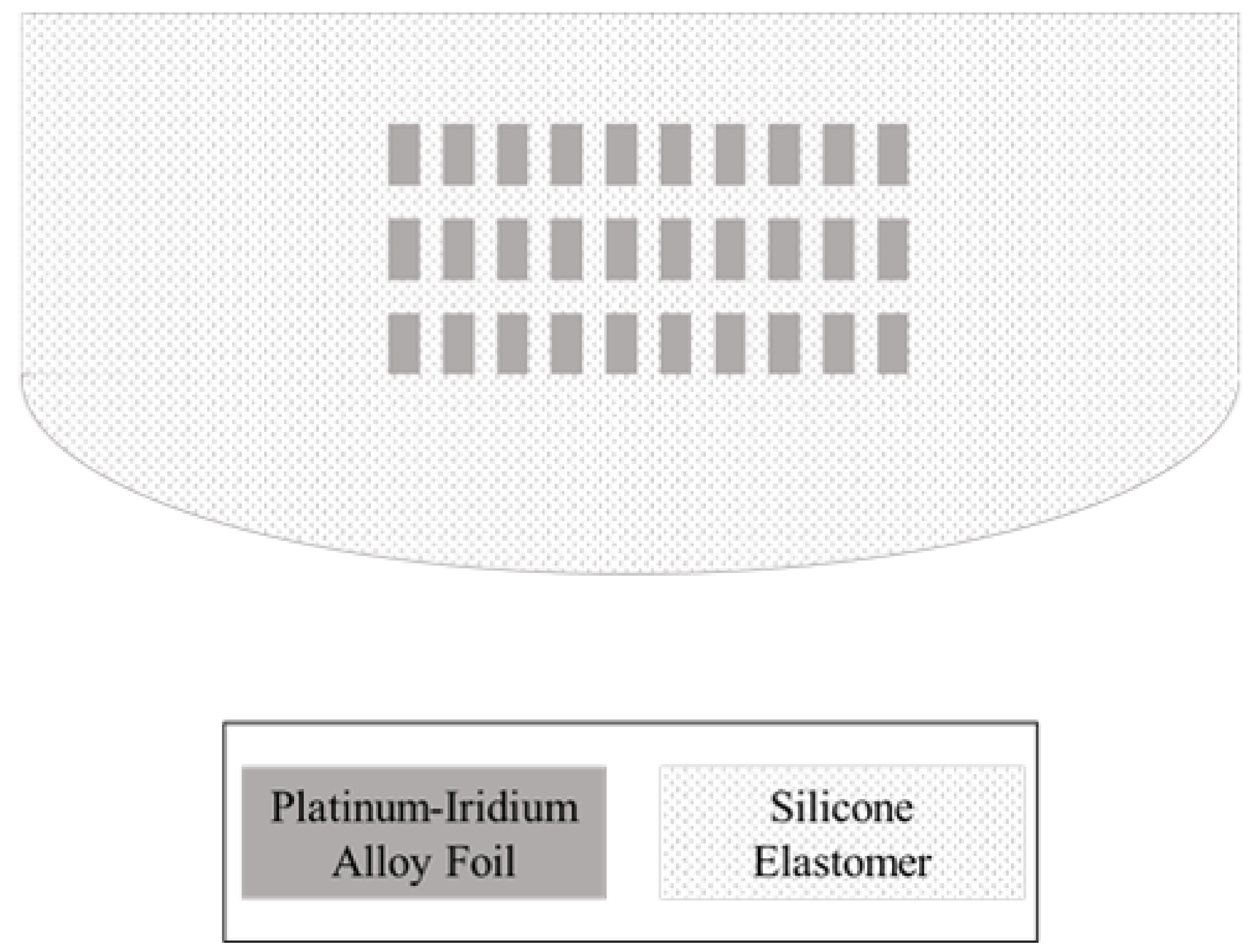
2.1. Design and Structure
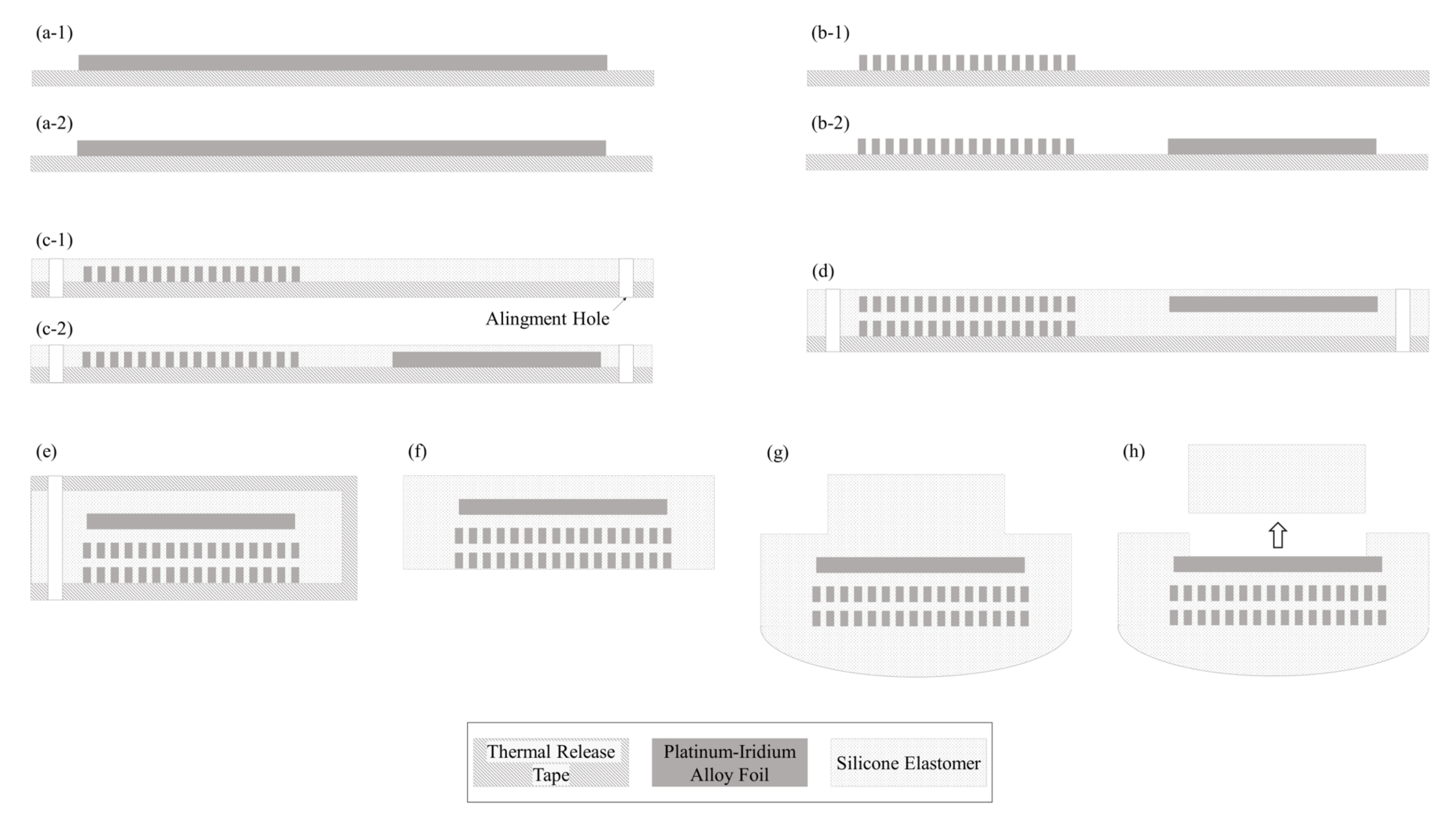
2.2. Fabrication
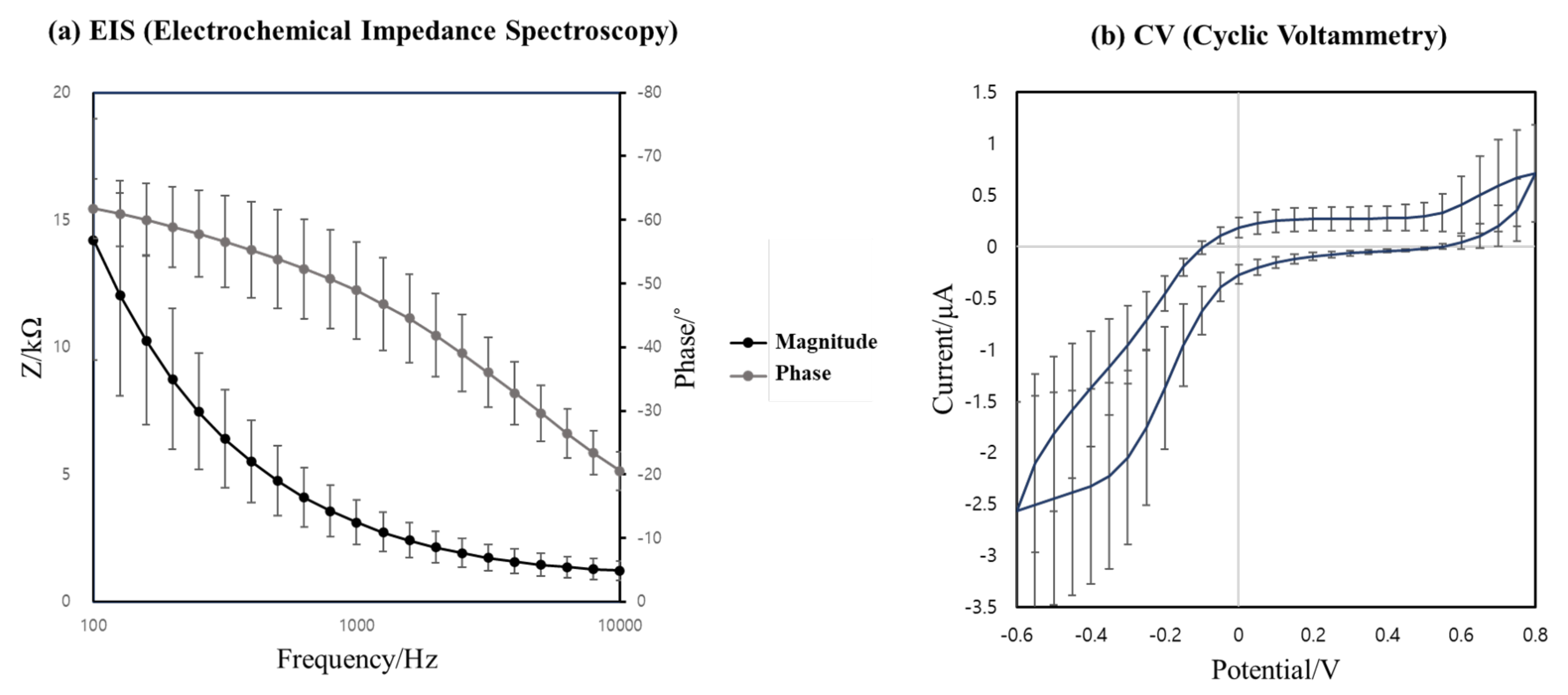
2.3. Electrochemical Evaluation
2.4. Stiffness Measurement
2.5. Insertion and Extraction Force Measurement
3. Results
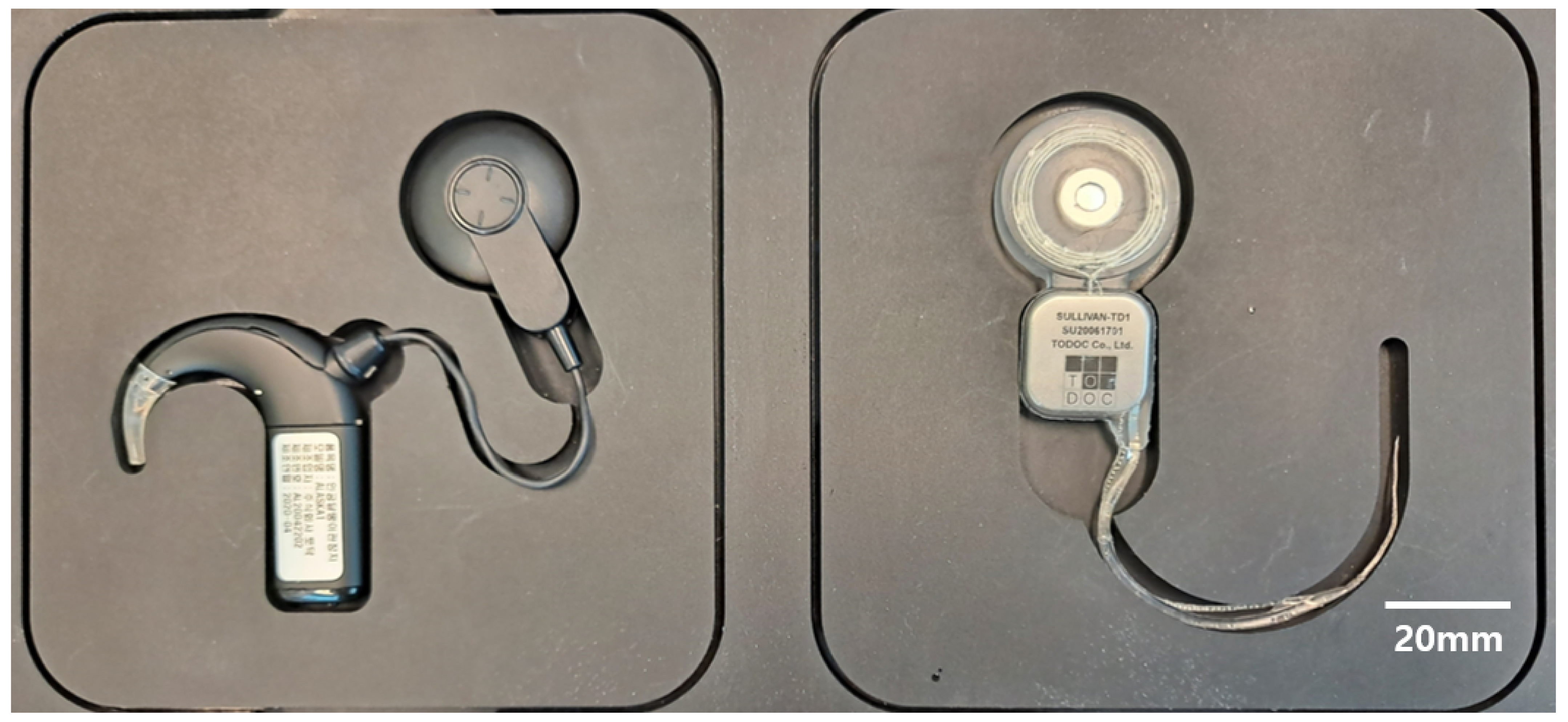
3.1. Thirty-Two-Channel Cochlear Electrode Array
3.2. Electrochemical Evaluation
3.3. Stiffness Measurement
3.4. Insertion and Extraction Force Measurement
4. Discussion
4.1. Cost and Feasibility
4.2. Design Challenges for High-Density CI Electrode Array
4.3. Mechanical Property
4.4. Future Research Direction
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Magro, I.; Emmett, S.D.; Saunders, J. Cost-effectiveness of CI in developing countries. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Emmett, S.D.; Tucci, D.L.; Bento, R.F.; Garcia, J.M.; Juman, S.; Chiossone-Kerdel, J.A.; Liu, T.J.; De Muñoz, P.C.; Ullauri, A.; Letort, J.J.; et al. Moving beyond GDP: Cost effectiveness of cochlear implantation and deaf education in Latin America. Otol. Neurotol. 2016, 37, 1040–1048. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saunders, J.E.; Barrs, D.M.; Gong, W.; Wilson, B.S.; Mojica, K.; Tucci, D.L. Cost effectiveness of childhood cochlear implantation and deaf education in Nicaragua: A disability adjusted life year model. Otol. Neurotol. 2015, 36, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Bento, R.F.; Bahmad, F.; Hippolyto, M.A.; Da Costa, S.S. Overcoming developing-world challenges in cochlear implantation: A South American perspective. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 200–208. [Google Scholar] [CrossRef]
- Kumar, R.; Kameswaran, M. Cochlear implantation in the developing world: Perspectives from the Indian subcontinent. ENT Audiol News 2017, 26, 88–89. [Google Scholar]
- Sampath Kumar, R.; Kameswaran, M. A sustainable model for cochlear implantation in the developing world: Perspectives from the Indian subcontinent. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 196–199. [Google Scholar] [CrossRef]
- Li, J.N.; Chen, S.; Zhai, L.; Han, D.Y.; Eshraghi, A.A.; Feng, Y.; Yang, S.M.; Liu, X. The advances in hearing rehabilitation and cochlear implants in China. Ear Hear. 2017, 38, 647. [Google Scholar] [CrossRef]
- Liu, C.M.; Lee, C.T.C. Association of hearing loss with dementia. JAMA Netw. Open 2019, 2, e198112. [Google Scholar] [CrossRef]
- An, S.K.; Park, S.I.; Jun, S.B.; Lee, C.J.; Byun, K.M.; Sung, J.H.; Wilson, B.S.; Rebscher, S.J.; Oh, S.H.; Kim, S.J. Design for a simplified cochlear implant system. IEEE Trans. Biomed. Eng. 2007, 54, 973–982. [Google Scholar] [CrossRef]
- Fishman, K.E.; Shannon, R.V.; Slattery, W.H. Speech recognition as a function of the number of electrodes used in the SPEAK cochlear implant speech processor. J. Speech Lang. Hear. Res. 1997, 40, 1201–1215. [Google Scholar] [CrossRef]
- Friesen, L.M.; Shannon, R.V.; Baskent, D.; Wang, X. Speech recognition in noise as a function of the number of spectral channels: Comparison of acoustic hearing and cochlear implants. J. Acoust. Soc. Am. 2001, 110, 1150–1163. [Google Scholar] [CrossRef]
- Garnham, C.; O’Driscoll, M.; Ramsden, R.; Saeed, S. Speech understanding in noise with a Med-El COMBI 40+ cochlear implant using reduced channel sets. Ear Hear. 2002, 23, 540–552. [Google Scholar] [CrossRef]
- Corbett, S.; Ketterl, J.; Johnson, T. Polymer-based microelectrode arrays. MRS Online Proceed. Library 2006, 926, 1–6. [Google Scholar] [CrossRef]
- Min, K.S.; Oh, S.H.; Park, M.H.; Jeong, J.; Kim, S.J. A polymer-based multichannel cochlear electrode array. Otol. Neurotol. 2014, 35, 1179–1186. [Google Scholar] [CrossRef]
- Gwon, T.M. A Polymer Cochlear Electrode Array: Atraumatic Deep Insertion, Tripolar Stimulation, and Long-Term Reliability; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Kim, J.H.; Min, K.S.; An, S.K.; Jeong, J.S.; Jun, S.B.; Cho, M.H.; Son, Y.D.; Cho, Z.H.; Kim, S.J. Magnetic resonance imaging compatibility of the polymer-based cochlear implant. Clin. Experiment. Otorhinolaryngol. 2012, 5, S19. [Google Scholar] [CrossRef]
- Lee, S.W.; Min, K.S.; Jeong, J.; Kim, J.; Kim, S.J. Monolithic encapsulation of implantable neuroprosthetic devices using liquid crystal polymers. IEEE Trans. Biomed. Eng. 2011, 58, 2255–2263. [Google Scholar]
- Jiang, G.; Zhou, D.D. Technology advances and challenges in hermetic packaging for implantable medical devices. In Implantable Neural Prostheses 2; Springer: Berlin/Heidelberg, Germany, 2009; pp. 27–61. [Google Scholar]
- Croghan, N.B.; Duran, S.I.; Smith, Z.M. Re-examining the relationship between number of cochlear implant channels and maximal speech intelligibility. J. Acoust. Soc. Am. 2017, 142, EL537–EL543. [Google Scholar] [CrossRef]
- Berg, K.A.; Noble, J.H.; Dawant, B.M.; Dwyer, R.T.; Labadie, R.F.; Gifford, R.H. Speech recognition as a function of the number of channels in perimodiolar electrode recipients. J. Acoust. Soc. Am. 2019, 145, 1556–1564. [Google Scholar] [CrossRef]
- Kontorinis, G.; Paasche, G.; Lenarz, T.; Stöver, T. The effect of different lubricants on cochlear implant electrode insertion forces. Otol. Neurotol. 2011, 32, 1050–1056. [Google Scholar] [CrossRef]
- Rebscher, S.J.; Hetherington, A.; Bonham, B.; Wardrop, P.; Whinney, D.; Leake, P.A. Considerations for the design of future cochlear implant electrode arrays: Electrode array stiffness, size and depth of insertion. J. Rehabil. Res. Dev. 2008, 45, 731. [Google Scholar] [CrossRef]
- Zeng, F.G.; Rebscher, S.; Harrison, W.; Sun, X.; Feng, H. Cochlear implants: System design, integration, and evaluation. IEEE Rev. Biomed. Eng. 2008, 1, 115–142. [Google Scholar] [CrossRef]
- Gollan, P.J.; Kaufman, B.E.; Taras, D.; Wilkinson, A. Voice and Involvement at Work: Experience with Non-Union Representation; Routledge: London, UK, 2014; p. 76. [Google Scholar]
- Cochlear. 2019 Annual Report; Cochlear Limited: Sydney, Australia, 2019. [Google Scholar]
- Clark, G.M.; Shepherd, R.; Patrick, J.F.; Black, R.; Tong, Y. Design and fabrication of the banded electrode array. Sci. Pub. 1983, 405, 191–201. [Google Scholar] [CrossRef]
- Merrill, D.R. The electrochemistry of charge injection at the electrode/tissue interface. In Implantable Neural Prostheses 2; Springer: Berlin/Heidelberg, Germany, 2010; pp. 85–138. [Google Scholar]
- Shepherd, R.K.; Carter, P.M.; Dalrymple, A.N.; Enke, Y.L.; Wise, A.K.; Nguyen, T.; Firth, J.; Thompson, A.; Fallon, J.B. Platinum dissolution and tissue response following long-term electrical stimulation at high charge densities. J. Neur. Eng. 2021, 18, 036021. [Google Scholar] [CrossRef]
- Dhanasingh, A.; Jolly, C. An overview of cochlear implant electrode array designs. Hear. Res. 2017, 356, 93–103. [Google Scholar] [CrossRef]
- Klein, E.; Gossler, C.; Paul, O.; Ruther, P. High-density μLED-based optical cochlear implant with improved thermomechanical behavior. Front. Neurosci. 2018, 12, 659. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.; Kim, J.Y.; Kim, Y.C.; Kim, S.; Chou, N.; Lee, S.; Choung, Y.H.; Kim, S.; Brugger, J.; Choi, H.; et al. A 3D microscaffold cochlear electrode array for steroid elution. Adv. Healthc. Mater. 2019, 8, 1900379. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, P.; Beek-King, V.; Sharpe, A.; Crawford, J.; Tridandapani, S.; McKinnon, B.; Blake, D. Highly flexible silicone coated neural array for intracochlear electrical stimulation. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Iverson, K.C.; Bhatti, P.T.; Falcone, J.; Figueroa, R.; McKinnon, B.J. Cochlear implantation using thin-film array electrodes. Otolaryngol. Head Neck Surg. 2011, 144, 934–939. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 14708-7: Implants for Surgery—Active Implantable Medical Devices—Part 7: Particular Requirements for Cochlear Implant Systems, 1st ed.; ISO: Geneva, Switzerland, 2013. [Google Scholar]
- Min, K.S. A Study on the Liquid Crystal Polymer-Based Intracochlear Electrode Array. Ph.D. Thesis, Seoul National University, Seoul, Korea, 2014. [Google Scholar]
- Bodington, E.; Saeed, S.R.; Smith, M.C.; Stocks, N.G.; Morse, R.P. A narrative review of the logistic and economic feasibility of cochlear implants in lower-income countries. Cochlear Implants Int. 2021, 22, 7–16. [Google Scholar] [CrossRef]
- Reeve, L.; Baldrick, P. Biocompatibility assessments for medical devices–evolving regulatory considerations. Expert Rev. Med. Dev. 2017, 14, 161–167. [Google Scholar] [CrossRef]
- Gwon, T.M.; Min, K.S.; Kim, J.H.; Oh, S.H.; Lee, H.S.; Park, M.H.; Kim, S.J. Fabrication and evaluation of an improved polymer-based cochlear electrode array for atraumatic insertion. Biomed. Microdev. 2015, 17, 1–12. [Google Scholar] [CrossRef]
- Moteki, H.; Nishio, S.Y.; Miyagawa, M.; Tsukada, K.; Noguchi, Y.; Usami, S.I. Feasibility of hearing preservation for residual hearing with longer cochlear implant electrodes. Acta Oto-Laryngol. 2018, 138, 1080–1085. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Vertical | Horizontal | Mean | |
|---|---|---|---|---|
| of | Stiffness | Stiffness | Stiffness | V/H Ratio |
| Manufacturer | (mN) | (mN) | (mN) | |
| TODOC Co., Ltd. | 19.8 | 15.7 | 17.8 | 1.26 |
| Nurobiosys | 25.2 | 21.4 | 23.3 | 1.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.; Ha, Y.; Choi, G.; Hyun, J.; Kim, S.; Oh, S.-H.; Min, K.-S. Manufacturable 32-Channel Cochlear Electrode Array and Preliminary Assessment of Its Feasibility for Clinical Use. Micromachines 2021, 12, 778. https://doi.org/10.3390/mi12070778
Shin S, Ha Y, Choi G, Hyun J, Kim S, Oh S-H, Min K-S. Manufacturable 32-Channel Cochlear Electrode Array and Preliminary Assessment of Its Feasibility for Clinical Use. Micromachines. 2021; 12(7):778. https://doi.org/10.3390/mi12070778
Chicago/Turabian StyleShin, Soowon, Yoonhee Ha, Gwangjin Choi, Junewoo Hyun, Sangwoo Kim, Seung-Ha Oh, and Kyou-Sik Min. 2021. "Manufacturable 32-Channel Cochlear Electrode Array and Preliminary Assessment of Its Feasibility for Clinical Use" Micromachines 12, no. 7: 778. https://doi.org/10.3390/mi12070778
APA StyleShin, S., Ha, Y., Choi, G., Hyun, J., Kim, S., Oh, S.-H., & Min, K.-S. (2021). Manufacturable 32-Channel Cochlear Electrode Array and Preliminary Assessment of Its Feasibility for Clinical Use. Micromachines, 12(7), 778. https://doi.org/10.3390/mi12070778