Pooled Analysis of Real-World Evidence Supports Anti-CGRP mAbs and OnabotulinumtoxinA Combined Trial in Chronic Migraine

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
2.1. Real-World Evidence
- 11 patients received erenumab 70 mg, for a total of 125 doses, thus accounting for one administration per month for 11–12 months;
- 12 patients were prescribed erenumab 140 mg, for a total of 134 doses, accounting for one administration per month for 11 months: therefore, patients most likely moved to this treatment after one month of lower dosage;
- 11 patients received 131 doses of galcanezumab 120 mg, one per month a year;
- 8 patients were treated with 72 doses of fremanezumab 225 mg and 1 dose of fremanezumab 675 mg, accounting for one year-long treatment.
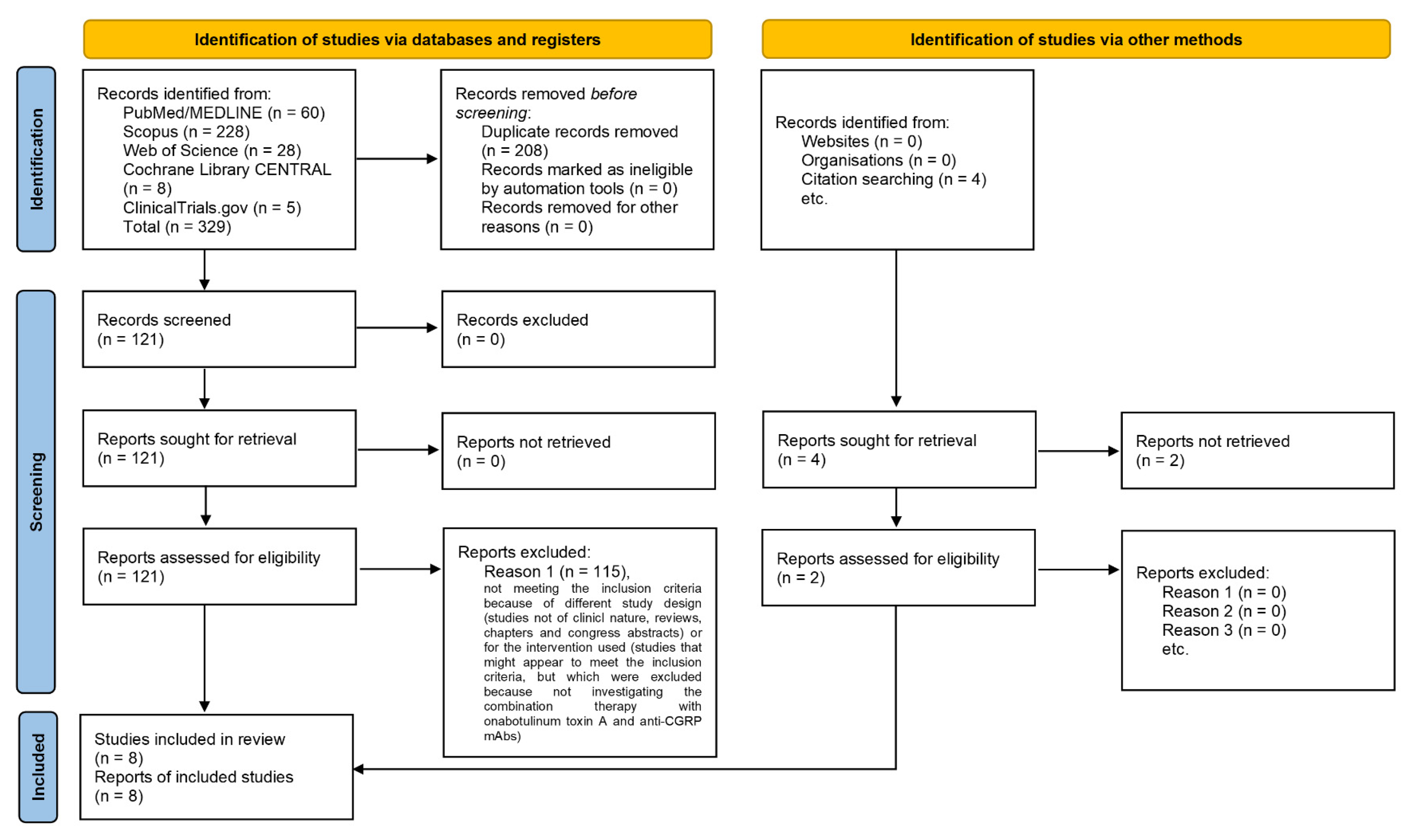
2.2. Selection of the Studies
2.3. Qualitative Analysis
2.4. Quantitative Analysis
2.5. Meta-Analysis
2.6. Assessment of Certainty of Evidence
2.6.1. Risk of Bias
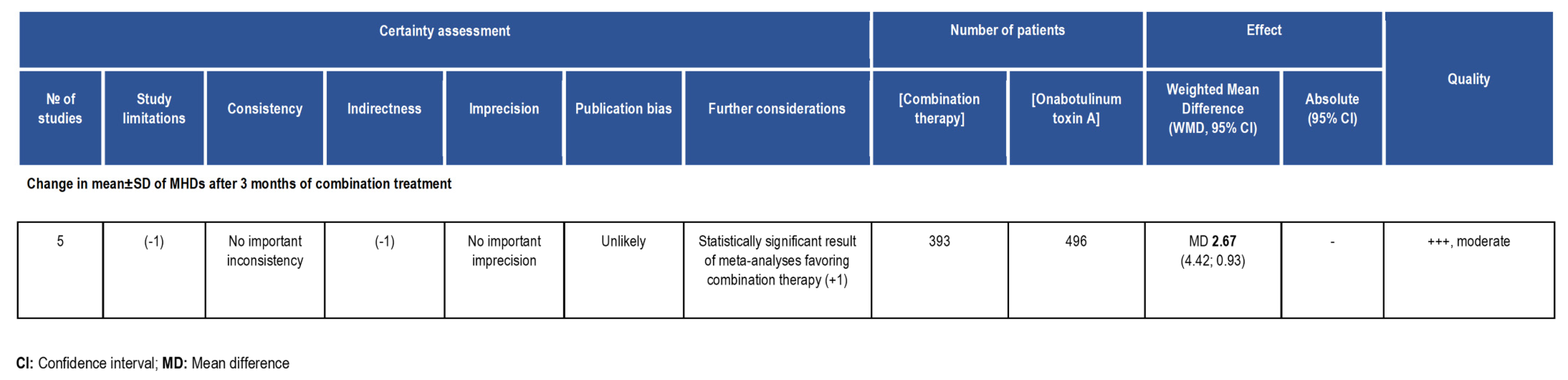
2.6.2. Summary of Findings (SoF) Grading of Recommendations Assessment, Development and Evaluation (GRADE)
3. Discussion
Registration and Protocol
4. Materials and Methods
4.1. Real-World Study Design
4.2. Objectives and Protocol
4.3. Inclusion Criteria
4.4. Information Sources
4.5. Search Strategy
4.6. Study Selection
4.7. Data Synthesis, Risk of Bias Assessment and Critical Appraisal
4.8. Statistical Analysis and Effect Measures
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leonardi, M.; Grazzi, L.; D’Amico, D.; Martelletti, P.; Guastafierro, E.; Toppo, C.; Raggi, A. Global Burden of Headache Disorders in Children and Adolescents 2007–2017. Int. J. Environ. Res. Public Health 2021, 18, 250. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Brin, M.F. Chronic Migraine: An Update on Physiology, Imaging, and the Mechanism of Action of Two Available Pharmacologic Therapies. Headache J. Head Face Pain 2017, 57, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Mathew, N.T.; Stubits, E.; Nigam, M.P. Transformation of episodic migraine into daily headache: Analysis of factors. Headache 1982, 22, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Barrodale, P.M.; Tipton, R.L.; Khodavirdi, A. Brainstem dysfunction in chronic migraine as evidenced by neurophysiological and positron emission tomography studies. Headache 2007, 47, 996–1003. [Google Scholar] [CrossRef]
- Haut, S.R.; Bigal, M.E.; Lipton, R.B. Chronic disorders with episodic manifestations: Focus on epilepsy and migraine. Lancet Neurol. 2006, 5, 148–157. [Google Scholar] [CrossRef]
- Bigal, M.E.; Liberman, J.N.; Lipton, R.B. Age-dependent prevalence and clinical features of migraine. Neurology 2006, 67, 246–251. [Google Scholar] [CrossRef]
- Villalón, C.M.; Olesen, J. The role of CGRP in the pathophysiology of migraine and efficacy of CGRP receptor antagonists as acute antimigraine drugs. Pharmacol. Ther. 2009, 124, 309–323. [Google Scholar] [CrossRef]
- Juaneda, C.; Dumont, Y.; Quirion, R. The molecular pharmacology of CGRP and related peptide receptor subtypes. Trends Pharmacol. Sci. 2000, 21, 432–438. [Google Scholar] [CrossRef]
- Poyner, D.R.; Sexton, P.M.; Marshall, I.; Smith, D.M.; Quirion, R.; Born, W.; Muff, R.; Fischer, J.A.; Foord, S.M. International Union of Pharmacology. XXXII. The mammalian calcitonin gene-related peptides, adrenomedullin, amylin, and calcitonin receptors. Pharmacol. Rev. 2002, 54, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Van Rossum, D.; Hanisch, U.-K.; Quirion, R. Neuroanatomical localization, pharmacological characterization and functions of CGRP, related peptides and their receptors. Neurosci. Biobehav. Rev. 1997, 21, 649–678. [Google Scholar] [CrossRef]
- Arulmani, U.; MaassenVanDenBrink, A.; Villalón, C.M.; Saxena, P.R. Calcitonin gene-related peptide and its role in migraine pathophysiology. Eur. J. Pharmacol. 2004, 500, 315–330. [Google Scholar] [CrossRef]
- Zhang, Z.; Winborn, C.S.; de Prado, B.M.; Russo, A.F. Sensitization of calcitonin gene-related peptide receptors by receptor activity-modifying protein-1 in the trigeminal ganglion. J. Neurosci. 2007, 27, 2693–2703. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Welch, M.J.; Purkiss, J.R.; Foster, K.A. Sensitivity of embryonic rat dorsal root ganglia neurons to Clostridium botulinum neurotoxins. Toxicon Off. J. Int. Soc. Toxinology 2000, 38, 245–258. [Google Scholar] [CrossRef]
- Sandrini, G.; Perrotta, A.; Tassorelli, C.; Torelli, P.; Brighina, F.; Sances, G.; Nappi, G. Botulinum toxin type-A in the prophylactic treatment of medication-overuse headache: A multicenter, double-blind, randomized, placebo-controlled, parallel group study. J. Headache Pain 2011, 12, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Dolly, O. Synaptic transmission: Inhibition of neurotransmitter release by botulinum toxins. Headache 2003, 43 (Suppl. 1), 16–24. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Casals-Diaz, L.; Zurawski, T.; Meng, J.; Moriarty, O.; Nealon, J.; Edupuganti, O.P.; Dolly, O. A novel therapeutic with two SNAP-25 inactivating proteases shows long-lasting anti-hyperalgesic activity in a rat model of neuropathic pain. Neuropharmacology 2017, 118, 223–232. [Google Scholar] [CrossRef]
- Burstein, R.; Zhang, X.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef]
- Aoki, K.R. Review of a proposed mechanism for the antinociceptive action of botulinum toxin type A. Neurotoxicology 2005, 26, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Sandrini, G.; De Icco, R.; Tassorelli, C.; Smania, N.; Tamburin, S. Botulinum neurotoxin type A for the treatment of pain: Not just in migraine and trigeminal neuralgia. J. Headache Pain 2017, 18, 38. [Google Scholar] [CrossRef]
- De Icco, R.; Perrotta, A.; Berra, E.; Allena, M.; Alfonsi, E.; Tamburin, S.; Serrao, M.; Sandrini, G.; Tassorelli, C. OnabotulinumtoxinA Reduces Temporal Pain Processing at Spinal Level in Patients with Lower Limb Spasticity. Toxins 2019, 11, 359. [Google Scholar] [CrossRef]
- Scuteri, D.; Corasaniti, M.T.; Tonin, P.; Bagetta, G. Eptinezumab for the treatment of migraine. Drugs Today 2019, 55, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Bagetta, G. Progress in the Treatment of Migraine Attacks: From Traditional Approaches to Eptinezumab. Pharmaceuticals 2021, 14, 924. [Google Scholar] [CrossRef] [PubMed]
- Winner, P.K.; McAllister, P.; Chakhava, G.; Ailani, J.; Ettrup, A.; Krog Josiassen, M.; Lindsten, A.; Mehta, L.; Cady, R. Effects of Intravenous Eptinezumab vs. Placebo on Headache Pain and Most Bothersome Symptom When Initiated During a Migraine Attack: A Randomized Clinical Trial. JAMA 2021, 325, 2348–2356. [Google Scholar] [CrossRef]
- Scuteri, D.; Tonin, P.; Nicotera, P.; Bagetta, G.; Corasaniti, M.T. Real world considerations for newly approved CGRP receptor antagonists in migraine care. Expert Rev. Neurother. 2022, 22, 221–230. [Google Scholar] [CrossRef]
- Scuteri, D.; Adornetto, A.; Rombolà, L.; Naturale, M.D.; Morrone, L.A.; Bagetta, G.; Tonin, P.; Corasaniti, M.T. New Trends in Migraine Pharmacology: Targeting Calcitonin Gene-Related Peptide (CGRP) With Monoclonal Antibodies. Front. Pharmacol. 2019, 10, 363. [Google Scholar] [CrossRef] [PubMed]
- Ailani, J.; Burch, R.C.; Robbins, M.S. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache 2021, 61, 1021–1039. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, E.; Guglielmetti, M.; Ornello, R.; Spuntarelli, V.; Martelletti, P.; Sacco, S. Targeting CGRP for migraine treatment: Mechanisms, antibodies, small molecules, perspectives. Expert Rev. Neurother. 2020, 20, 627–641. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M. The most important advances in headache research in 2018. Lancet Neurol. 2019, 18, 5–6. [Google Scholar] [CrossRef]
- Scuteri, D.; Corasaniti, M.T.; Tonin, P.; Nicotera, P.; Bagetta, G. Role of CGRP pathway polymorphisms in migraine: A systematic review and impact on CGRP mAbs migraine therapy. J. Headache Pain 2021, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.M.; Doan, L.P.; et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef]
- Lu, J.; Zhang, Q.; Guo, X.; Liu, W.; Xu, C.; Hu, X.; Ni, J.; Lu, H.; Zhao, H. Calcitonin Gene–Related Peptide Monoclonal Antibody Versus Botulinum Toxin for the Preventive Treatment of Chronic Migraine: Evidence From Indirect Treatment Comparison. Front. Pharmacol. 2021, 12, 631204. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Cohen, F.; Armand, C.; Lipton, R.B.; Vollbracht, S. Efficacy and Tolerability of Calcitonin Gene–Related Peptide–Targeted Monoclonal Antibody Medications as Add-on Therapy to OnabotulinumtoxinA in Patients with Chronic Migraine. Pain Med. 2021, 22, 1857–1863. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Singh, H.; Govindarajan, R. Galcanezumab in the Prevention of Chronic Migraine in Patients on Botulinum Toxin Therapy (5257). Neurology 2020, 94, 5257. [Google Scholar]
- Ozudogru, S.N.; Bartell, J.W.; Yuan, H.; Digre, K.B.; Baggaley, S.K. The Effect of Adding Calcitonin Gene-Related Peptide Monoclonal Antibodies to OnabotulinumtoxinA Therapy on Headache Burden: A Retrospective Observational Case Series. Headache J. Head Face Pain 2020, 60, 1442–1443. [Google Scholar] [CrossRef]
- Boudreau, G. Treatment of chronic migraine with erenumab alone or as an add on therapy: A real-world observational study. Anesth Pain Res. 2020, 4, 1–4. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n160. [Google Scholar] [CrossRef]
- Boers, M. Graphics and statistics for cardiology: Designing effective tables for presentation and publication. Heart (Br. Card. Soc.) 2018, 104, 192–200. [Google Scholar] [CrossRef]
- Mayo-Wilson, E.; Li, T.; Fusco, N.; Dickersin, K. Practical guidance for using multiple data sources in systematic reviews and meta-analyses (with examples from the MUDS study). Res. Synth. Methods 2018, 9, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Stovold, E.; Beecher, D.; Foxlee, R.; Noel-Storr, A. Study flow diagrams in Cochrane systematic review updates: An adapted PRISMA flow diagram. Syst. Rev. 2014, 3, 54. [Google Scholar] [CrossRef] [PubMed]
- Armanious, M.; Khalil, N.; Lu, Y.; Jimenez-Sanders, R. Erenumab and OnabotulinumtoxinA Combination Therapy for the Prevention of Intractable Chronic Migraine without Aura: A Retrospective Analysis. J. Pain Palliat. Care Pharmacother. 2021, 35, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Frishberg, B.M.; Schim, J.D.; Iannone, A.; Schneider, G.; Yedigarova, L.; Adams, A.M. Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA: A Retrospective Chart Review. Pain Ther. 2021, 10, 809–826. [Google Scholar] [CrossRef]
- Mechtler, L.; Saikali, N.; McVige, J.; Hughes, O.; Traut, A.; Adams, A.M. Real-World Evidence for the Safety and Efficacy of CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA Treatment for Migraine Prevention in Adult Patients With Chronic Migraine. Front. Neurol. 2022, 12, 788159. [Google Scholar] [CrossRef] [PubMed]
- Nandyala, A.S.; Suri, H.; Dougherty, C.O.; Ailani, J. A retrospective evaluation of the combination of erenumab and onabotulinumtoxinA for the prevention of chronic migraine. Clin. Neurol. Neurosurg. 2022, 215, 107200. [Google Scholar] [CrossRef]
- Silvestro, M.; Tessitore, A.; Scotto di Clemente, F.; Battista, G.; Tedeschi, G.; Russo, A. Additive Interaction Between Onabotulinumtoxin-A and Erenumab in Patients With Refractory Migraine. Front. Neurol. 2021, 12, 656294. [Google Scholar] [CrossRef] [PubMed]
- Toni, T.; Tamanaha, R.; Newman, B.; Liang, Y.; Lee, J.; Carrazana, E.; Vajjala, V.; Viereck, J.; Liow, K.K. Effectiveness of dual migraine therapy with CGRP inhibitors and onabotulinumtoxinA injections: Case series. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2021, 42, 5373–5376. [Google Scholar] [CrossRef] [PubMed]
- Ailani, J.; Blumenfeld, A.M. Combination CGRP monoclonal antibody and onabotulinumtoxinA treatment for preventive treatment in chronic migraine. Headache J. Head Face Pain 2022, 62, 106–108. [Google Scholar] [CrossRef]
- De Logu, F.; Nassini, R.; Hegron, A.; Landini, L.; Jensen, D.D.; Latorre, R.; Ding, J.; Marini, M.; Souza Monteiro de Araujo, D.; Ramírez-Garcia, P.; et al. Schwann cell endosome CGRP signals elicit periorbital mechanical allodynia in mice. Nat. Commun. 2022, 13, 646. [Google Scholar] [CrossRef]
- Pellesi, L.; Do, T.P.; Ashina, H.; Ashina, M.; Burstein, R. Dual Therapy With Anti-CGRP Monoclonal Antibodies and Botulinum Toxin for Migraine Prevention: Is There a Rationale? Headache J. Head Face Pain 2020, 60, 1056–1065. [Google Scholar] [CrossRef]
- Bayer, A.; Tadd, W. Unjustified exclusion of elderly people from studies submitted to research ethics committee for approval: Descriptive study. BMJ 2000, 321, 992–993. [Google Scholar] [CrossRef] [PubMed]
- Herrero, S.; Guerrero, A.L.; Ruiz, M.; Pedraza, M.I.; Mulero, P.; Barón, J.; Irene, I.; De la Cruz, C.; Peñas, M.L. Migraine in the elderly: Clinical characteristics in a series of 71 cases. J. Headache Pain 2013, 14, P152. [Google Scholar] [CrossRef][Green Version]
- Scuteri, D.; Mantovani, E.; Tamburin, S.; Sandrini, G.; Corasaniti, M.T.; Bagetta, G.; Tonin, P. Opioids in Post-stroke Pain: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 587050. [Google Scholar] [CrossRef]
- Scuteri, D.; Vulnera, M.; Piro, B.; Bossio, R.B.; Morrone, L.A.; Sandrini, G.; Tamburin, S.; Tonin, P.; Bagetta, G.; Corasaniti, M.T. Pattern of treatment of behavioural and psychological symptoms of dementia and pain: Evidence on pharmacoutilization from a large real-world sample and from a centre for cognitive disturbances and dementia. Eur. J. Clin. Pharmacol. 2021, 77, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Garreffa, M.R.; Esposito, S.; Bagetta, G.; Naturale, M.D.; Corasaniti, M.T. Evidence for accuracy of pain assessment and painkillers utilization in neuropsychiatric symptoms of dementia in Calabria region, Italy. Neural Regen. Res. 2018, 13, 1619–1621. [Google Scholar] [CrossRef]
- Scuteri, D.; Piro, B.; Morrone, L.A.; Corasaniti, M.T.; Vulnera, M.; Bagetta, G. The need for better access to pain treatment: Learning from drug consumption trends in the USA. Funct. Neurol. 2017, 22, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Berliocchi, L.; Rombolà, L.; Morrone, L.A.; Tonin, P.; Bagetta, G.; Corasaniti, M.T. Effects of Aging on Formalin-Induced Pain Behavior and Analgesic Activity of Gabapentin in C57BL/6 Mice. Front. Pharmacol. 2020, 11, 663. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Matamala-Gomez, M.; Bottiroli, S.; Corasaniti, M.T.; De Icco, R.; Bagetta, G.; Tonin, P. Pain Assessment and Treatment in Dementia at the Time of Coronavirus Disease COVID-19. Front. Neurol. 2020, 11, 890. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Contrada, M.; Tonin, P.; Corasaniti, M.T.; Nicotera, P.; Bagetta, G. Dementia and COVID-19: A Case Report and Literature Review on Pain Management. Pharmaceuticals 2022, 15, 199. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Jones, J.; Hunter, D. Qualitative Research: Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R. Cochrane Consumers and Communication Review Group: Data Synthesis and Analysis. Available online: http://cccrg.cochrane.org (accessed on 13 March 2019).
- Hultcrantz, M.; Rind, D.; Akl, E.A.; Treweek, S.; Mustafa, R.A.; Iorio, A.; Alper, B.S.; Meerpohl, J.J.; Murad, M.H.; Ansari, M.T.; et al. The GRADE Working Group clarifies the construct of certainty of evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Lièvre, M.; Cucherat, M.; Leizorovicz, A. Pooling, meta-analysis, and the evaluation of drug safety. Curr. Control. Trials Cardiovasc. Med. 2002, 3, 6. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot–Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Report (Author and Year) | Study Design | Ethical Approval | Sample Size | Inclusion Criteria for Participants (Type of Migraine and of Treatments) | Intervention (n) | Control (n) | Intervention Type, Timing and Dose | Treatment Assignment, Allocation and Concealment Mechanisms | Outcome | Results | Length of Follow-Up | Limitations of the Study | Authors’ Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Armanious et al., 2021 [46] | Retrospective cross-sectional | Approved by the university’s Institutional Review Board, Pro00036880 | All patients between the ages of 18 and 70 years of age seen in the university’s Headache Clinic (n = 78) with clinic encounters between 05/17/18 and 10/17/ 18. No sample power calculation | Patients between the ages of 18 and 70 years, with diagnosis of chronic migraine, defined as 15 or more headache days per month for three months with features of migraine headache on at least 8 days per month, and a baseline treatment with onabotulinumtoxinA for at least a nine-month duration. A total of 61.5% were actively using three or more other prophylactic migraine medications | n = 78 | No placebo group for comparison. Comparator is represented by the patient’s baseline on onabotulinumtoxinA for a minimum of nine preceding months | Erenumab 70 mg (n = 37) and Erenumab 140 mg (n = 41) in addition to onabotulinumtoxinA injections. Time points = 30, 60 and 90 days | ______ | Primary outcome measure was monthly headache days (MHDs) and monthly migraine days (MMDs) at baseline, 30-, 60- and 90-days. MHDs and MMDs | Mean of 8.1 fewer MHDs (p < 0.001) and of 7.4 fewer MMDs (p < 0.001) at 90 days. Statistically significant 30% reduction at 90-days for migraine (p = 0.008), but not for headache; no statistically significant 50% reduction at 90-days for migraine or headache | Ninety days | Observational nature; lack of comparison group; lack of control of concurrent use of additional prophylactic migraine therapies; lack of control for co-morbid conditions; missing assessment of additional variables. Data were not analyzed for parameters with ≥50% missing data points | Erenumab in combination with onabotulinumtoxinA may enhance the effect on CGRP release from peripheral unmyelinated C fibers, blocking CGRP receptors in myelinated A-delta fibers. Clinically meaningful improvement in this intractable chronic migraineurs |
| Blumenfeld et al., 2021 [47] | Retrospective, longitudinal chart review | The study was conducted in accordance with International Council for Harmonisation guidelines and local legal requirements, and complied with the ethical principles of the World Medical Assembly. The New England Independent Review Board approved the study protocol and case report form (CRF) before study initiation | Patients aged ≥18 years referred at the Neurology Center of Southern California for chronic migraine (San Diego County, CA) between 1 October 2018, and 1 November 2019. No sample power calculation. A convenience sample of approximately 300 patients based on available charts and adequate sample size to characterize the safety profile was used | Adult patients (aged ≥ 18 years) with chronic migraine presenting at least two consecutive onabotulinumtoxinA treatment cycles without concomitant CGRP mAb therapy during the 8-month qualification period prior to the index date (the initiation of combination onabotulinumtoxinA and CGRP mAb therapy), and ≥1 month of subsequent combination treatment with onabotulinumtoxinA and CGRP mAb | n = 257 | No placebo group for comparison. Comparator is represented by the patient’s baseline | Combination treatment of onabotulinumtoxinA with anti-CGRP mAbs (erenumab 70 (n = 136)/140 (n = 62) mg and galcanezumab 240 (n = 42) mg once monthly and fremanezumab 225 (n = 8)/675 (n = 7) mg once every three months as per label, instead of onabotulinum toxin not always administered per label, in dose ranging 115–200 U instead of 165U of baseline) | De-identified extracts of charts were prepared by site staff for the study | Monthly headache frequency, with intensity measured on a 0–10 scale. Migraine-related disability was captured on the Migraine Disability Assessment (MIDAS) questionnaire. Adverse events, discontinuations and reasons for discontinuation were recorded for each visit | Statistically significant and clinically meaningful reductions in mean MHDs at all visits. one-third (31.5–36.7%) of patients had a ≥50% reduction in MHDs after approximately 6 to 12 months: 43.7–45.1% of patients had a ≥5-point reduction from baseline, and 27.1–29.6% had a ≥30% reduction in MIDAS score. The mean MIDAS scores significantly decreased from baseline by 6.1 to 11.1 points during approximately 6 to 12 months of combination treatment. The 27.8% (68/245) of patients reported adverse events, with the most common being constipation (8.6% (21/245)), occurring most frequently in patients treated with erenumab (18/21). Concomitant use of other medications was recorded in 92.2% of patients at baseline, most commonly sumatriptan (20.7%) and topiramate (6.8%) | Twelve months | The onabotulinumtoxinA treatment was not always administered per label. The dates of migraine diagnosis, initiation of onabotulinumtoxinA, and headache frequency prior to onabotulinumtoxinA treatment prior to the 8-month qualification period were collected aas available. Missing data due to loss to follow-up were not included | The real-world data demonstrated that combination use of onabotulinumtoxinA and a CGRP mAb was generally well tolerated and suggestive of additive or synergistic benefit in headache frequency and migraine-related disability |
| Boudreau 2020 [41] | Prospective, observational study (NCT04152434) | All patients consented to participate to the study | No sample power calculation | Chronic migraineurs with migraine 15–30 days per month at baseline with or without an actual preventive drug, who failed more than 3 preventive drugs previously, naïve to monoclonal anti-CGRP mAbs | n = 69 nonpresenting reduction in migraine frequency at baseline out of n = 158 nonresponders | Group I On no preventive therapy at the start of Erenumab, (no Botox cohort) Group II On Botulinum Toxin type A prior to the add on therapy with Erenumab (Botox cohort). Group III On an oral preventive therapy prior to the add on therapy with Erenumab (no Botox cohort) | Botulinum Toxin type A + erenumab (70/140 mg) | ______ | The primary objective, was the reduction in the frequency of monthly migraine days. Adverse events were a secondary outcome | Forty-five patients (65%) experienced a decrease in the frequency of their monthly migraine days by 5–7 days, becoming episodic. Seventy-two adverse events were experienced during the 9 months of treatment, 56 events with the 140 mg. dose (118 patients), and 16 events with the 70 mg. dose (40 patients), the most frequent being comnstipation (34% of patients) | Nine months | Fifteen patients were lost to follow up. Fifty seven percent of patients failed to reach the primary end point | The 65% of patients receiving combination therapy achieved reduction in migraine frequency, instead of the 26% with erenumab alone or the 15% with erenumab in combination with prophylactic treatments other than botulinum toxin A |
| Mechtler et al., 2022 [48] | Retrospective, noninterventional, longitudinal study | The New England Independent Review Board (IRB) reviewed the study protocol prior to study initiation and determined the study as exempt from review. This study was conducted in accordance with current applicable regulations, International Conference of Harmonization guidelines, and local legal requirements, and complies with the ethical principles of the World Medical Assembly | All the eligible patients treated at the DENT Headache Center (Buffalo, NY, USA) between 1 June 2018 and 15 March 2020. The index date was defined as the start of combination treatment with onabotulinumtoxinA and a CGRP mAb and occurred between 1 June 2018 and 15 March 2019. The target sample size was up to ~300 patients, the expected number of eligible patients at the site | Adult patients (≥18 years) with chronic migraine treated with ≥2 consecutive cycles of onabotulinumtoxinA before ≥1 month of continuous onabotulinumtoxinA and CGRP mAb (erenumab, fremanezumab, or galcanezumab) combination treatment | n = 148 | No placebo group for comparison. Comparator is represented by the patient’s baseline. A baseline period of 1–3 months prior to index was used to assess the effectiveness of onabotulinumtoxinA treatment monotherapy. At baseline most used concomitant migraine medications (n = 143/148, 96.6%) and presented comorbid conditions (n = 142/148, 95.9%) | Continuous onabotulinumtoxinA and CGRP mAb [erenumab (70–140 mg), fremanezumab (225 mg), or galcanezumab (120 mg)] combination treatment | De-identified data were used | Headache frequency (monthly headache days). The effect on quality of life and disability was assessed with the 6-Item Headache Impact Test (HIT-6) and Migraine Disability Assessment (MIDAS), respectively. Adverse and serious adverse events were reported | After 12 months of combination therapy, MHD decreased by a mean of 4.6 days (95% CI 2.5–6.7). The 34.9% (95% CI 21.0–50.9) patientsachieved ≥50% reduction in MHD. Adverse events were reported by 18 patients (12.2%), with the most common being constipation (n = 8, 5.4% [onabotulinumtoxinA plus erenumab only]) and injection site reactions (n = 5, 3.4%) | Twelve months | Per label, erenumab, fremanezumab, and galcanezumab were administered once monthly, while OnabotulinumtoxinA was not always administered per label. Results were based on available data and missing data were not included. In fact, since paired HIT-6 and MIDAS scores from baseline and post-index assessments were only available for up to four patients, no further analyses were reported for those outcome measures | Incremental and clinically meaningful reductions in MHD are provided by combination therapy |
| Nandyala et al., 2022 [49] | Retrospective, cohort study | The study was approved by Institutional Review Board, and patient consent was deemed not needed. However, before the beginning of the therapy with erenumab, patients were provided information on expected side effects | Patients at Medstar Georgetown Headache Center. No sample size calculation | Adult (≥18 years old) patients who had a diagnosis of chronic migraine receiving onabotulinumtoxinA | n = 50 (2 patients started with 70 mg erenumab and moved to the 140 mg group) | No placebo group for comparison. Comparator is represented by the treatment with onabotulinumtoxinAlone | Erenumab [70 (n = 22)/140 (n = 26) mg) in combination with onabotulinumtoxinA, n = 50 | All data were de-identified, collected and recorded in a password protected document | Primary endpoint was decrease in number of migraine days. Secondary endpoints included a decrease in headache days and reported side effects | Significant reduction in MMDs (11.3 ± 9.3 vs. 14.9 ± 9.4, p < 0.001) and of MHDs (18.2 ± 10.3 vs. 20.7 ± 9.1, p = 0.042); 6 patients reported mild side effects including dizziness, insomnia, fatigue, skin changes, constipation and hair loss | One month | Data about demographic characteristics, other prophylactic medications, co-morbidities and number of prior treatments were not gathered | Erenumab and onabotulinumtoxinA, when used in combination, Show a decrease in migraine days per month and in headache days per month, without severe side effects |
| Ozudogru et al., 2020 [40] | Retrospective, observational, chart | _____ | Patients diagnosed with chronic migraine, having received at least two onabotulinumtoxinA treatments, after June 2018, and currently prescribed erenumab, fremanezumab or galcanezumab. No sample power calculation | Patients with a diagnosis of chronic migraine, who received at least two onabotulinumtoxinA treatments, after June 2018, and currently prescribed erenumab, fremanezumab or galcanezumab | n = 36 | No placebo group for comparison. Comparator is represented by the treatment with onabotulinumtoxinAlone | OnabotulinumtoxinA in combination with erenumab, fremanezumab or galcanezumab | ______ | 1. number of headache days; 2. number of weeks until the benefit from wear-off; 3. number of headache days after the benefit wore off | Half of the patients (n = 18) demonstrated improvement in headache burden >50% after the addition of an anti-CGRP mAb and an average increase of 2.0 weeks taken to wear-off during combination treatment | ______ | Small sample size. Retrospective, single-site study. Answers to the pre-procedure questionnaire used were based on the patients’ own recollection of events, with potential for recall bias | Potential for anti-CGRP mAbs to prolong the therapeutic benefit of onabotulinumtoxinA and to delay the wear-off by average two weeks |
| Silvestro et al., 2021 [50] | Case series | Approved by Ethical Committee of the University of Campania Luigi Vanvitelli. Each patient gave informed consent | No sample power calculation | Patients, aged between 18 and 65 years, who failed at least four or more oral preventive medication classes (propranolol or metoprolol, topiramate, flunarizine, valproate, amitriptyline, or candesartan) due to lack of efficacy or intolerable side effects, prescribed with onabotulinumtoxinA for at least 9 months (e.g., three administrations of 185 UI), interrupted in favor of a 6-month erenumab 140 mg monthly administration | n = 10 | No placebo group for comparison. Comparator is represented by baseline | Combined treatment with onabotulinumtoxinA (185 UI quarterly administration) and erenumab (140 mg monthly administration) | ______ | MHDs, severity of headache during attacks, symptomatic drug intake per month, and migraine disability | Statistically significant reduction of MHDs (p < 0.01), intensity of headache during attacks (p < 0.01), and symptomatic drug intake per month (p < 0.01), as well as MIDAS-assessed migraine disability (p < 0.01), compared to the baseline and also to onabotulinumtoxinA or erenumab alone (p < 0.01). The 30% of patients reported pain in the injection sites, without serious adverse events | Six months | Small sample size | A combined therapy may provide an additive or synergistic effect on the trigeminal nociceptive pathway |
| Toni et al., 2021 [51] | Case series | No approval since the study is based on authors’ clinical experience | Patients admitted between May 2018 to June 2020. No sample power calculation | Chronic migraine with suboptimal response to onabotulinumtoxinA | n = 17 | No placebo group for comparison. Comparator is represented by response to onabotulinumtoxinA alone | Combined therapy with onabotulinumtoxinA and fremanezumab (n = 9), erenumab (n = 4) or galcanezumab (n = 4) | Patients’ records confidentiality was maintained and data de-identified | Headache days and severity over 1–6 months | A mean improvement of +12.6 headache-free days was observed in fremanezumab patients, +6.4 in erenumab patients, and +3.8 in galcanezumab patients, for a total improvement experienced by n = 11 patients. No severe adverse side effects were experienced, with only mild irritation at the injection site and constipation. The response rate resulted of 58.82% for headache days reduction and of 64.71% for headache severity | Six months | Placebo-controlled, randomized studies are required to confirm the results | Patients suffering from severe, intractable migraine may benefit from onabotulinumtoxinA and anti- CGRP mAb dual therapy, likely due to a synergistic mechanism at receptor and ligand level |
| Study Report (Author and Year) | Intervention Dose 1 Change in MHDs | Intervention Dose 2 Change in MHDs | Intervention Dose 1 Change in MMDs | Intervention Dose 2 Change in MMDs |
|---|---|---|---|---|
| Armanious et al., 2021 [46] | Erenumab 70 mg | Erenumab 140 mg | Erenumab 70 mg | Erenumab 140 mg |
| n = 33/37 | n = 39/41 | n = 32/37 | n = 41/41 | |
| 6.8 ± 7.5 | 6.8 ± 8.0 | 9.6 ± 9.4 | 7.5 ± 7.1 | |
| Improvement in 89.2% of treated patients | Improvement in 95.1% of treated patients | Improvement in 86.5% of treated patients | Improvement in 100% of treated patients | |
| Nandyala et al., 2022 [49] | n = 22/50 (same treatment) | n = 22/50 (same treatment) | n = 26/50 (same treatment) | n = 26/50 (same treatment) |
| 2.5 ± 1.2 | 2.5 ± 1.2 | 3.6 ± 0.1 | 3.6 ± 0.1 | |
| Improvement in 44% of treated patients | Improvement in 44% of treated patients | Improvement in 52% of treated patients | Improvement in 52% of treated patients | |
| Pooled results | Improvement in 63.2% of treated patients | Improvement in 67% of treated patients | Improvement in 66.7% of treated patients | Improvement in 73.6% of treated patients |
| Study Report (Author and Year) | Comparator/Baseline Change in MHDs | Comparator/Baseline Change in MMDs | Intervention Dose 1 Change in MHDs | Intervention Dose 2 Change in MHDs | Intervention Dose 1 Change in MMDs | Intervention Dose 2 Change in MMDs |
|---|---|---|---|---|---|---|
| Armanious et al., 2021 [46] | n = 65/78 7.2 ± 8.6 | n = 66/78 6.7 ± 7.3 | Erenumab 70 mg n = 30/37 7.6 ± 8.3 Improvement over baseline in 81.1% of treated patients | Erenumab 140 mg n = 35/41 6.9 ± 9.0 | Erenumab 70 mg n = 29/37 6.6 ± 6.5 | Erenumab 140 mg n = 37/41 6.8 ± 7.9 Improvement over baseline in 90.2% of treated patients |
| Study Report (Author and Year) | Comparator/Baseline Change in MHDs | Comparator/Baseline Change in MMDs | Intervention Dose 1 Change in MHDs | Intervention Dose 2 Change in MHDs | Intervention Dose 1 Change in MMDs | Intervention Dose 2 Change in MMDs |
|---|---|---|---|---|---|---|
| Armanious et al., 2021 [46] | n = 34/78 8.1 ± 8.8 | n = 33/78 7.4 ± 6.8 | Erenumab 70 mg n = 21/37 8.3 ± 8.7 Improvement over baseline in 56.8% of treated patients | Erenumab 140 mg n = 13/41 7.8 ± 9.3 | Erenumab 70 mg n = 19/37 6.7 ± 5.6 | Erenumab 140 mg n = 14/41 8.4 ± 8.2 Improvement over baseline in 34.1% of treated patients |
| Study Report (Author and Year) | 3 Months | 6 Months | 9 Months | 12 Months |
|---|---|---|---|---|
| Blumenfeld et al., 2021 [47] | 25.7% (n = 56/218) | 36.7% (n = 66/180) | 33.3% (n = 47/141) | 31.5% (n = 33/106) |
| Mechtler et al., 2022 [48] | 21.2% (n = 24/113) | 28.9% (n = 26/90) | 29.0% (n = 20/69) | 34.9% (n = 15/43) |
| Toni et al., 2021 [51] | ____________ | 58.8% (n = 10/17) | ____________ | ____________ |
| Pooled results | 35.5% (n = 102/287) |
| Study Report (Author and Year) | 3 Months | 6 Months | 9 Months | 12 Months |
|---|---|---|---|---|
| Blumenfeld et al., 2021 [47] | 31.0% (n = 43/139) | 29.6% (n = 33/112) | 29.4% (n = 24/83) | 27.1% (n = 18/66) |
| Mechtler et al., 2022 [48] | ____________ | ____________ | ____________ | ____________ |
| Study Report (Author and Year) | 6 Months |
|---|---|
| Blumenfeld et al., 2021 [47] | 14.2% (n = 28/197) |
| Mechtler et al., 2022 [48] | 12.1% (n = 18/148) |
| Pooled results | 13.3% (n = 46/345) |
| OnabotulinumtoxinA + mAb | OnabotulinumtoxinA | Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Mean | SD | Total | Mean | SD | Total | Weight | IV, Random, 95% CI |
| Armanious et al., 2021 | 14.2 | 11.5 | 21 | 14.2 | 11.1 | 35 | 6.9% | 0.00 [−6.14, 6.14] |
| Blumenfeld et al., 2021 | 10.3 | 8 | 180 | 12.1 | 8 | 246 | 34.8% | −1.80 [−3.34, −0.26] |
| Mechtler et al., 2022 | 11.6 | 6.3 | 127 | 14 | 6.9 | 148 | 34.5% | −2.40 [−3.96, −0.84] |
| Nandyala et al., 2022 | 18.2 | 10.3 | 48 | 20.7 | 9.1 | 50 | 14.3% | −2.50 [−6.35, 1.35] |
| Toni et al., 2021 | 18.6 | 9.4 | 17 | 27.6 | 4.8 | 17 | 9.6% | −9.00 [−14.02, −3.98] |
| Total (95% CI) | 393 | 496 | 100.0% | −2.67 [−4.42, −0.93] | ||||
| [Combination therapy of onabotulinumtoxinA + anti-CGRP mAbs] compared with [baseline] for [chronic migraine] | ||
|---|---|---|
| Patient or population: [patients] with [chronic migraine] Settings: [real-world] Intervention: [Combination therapy of onabotulinumtoxinA + anti-CGRP mAbs] Comparison: [OnabotulinumtoxinA alone] | ||
| Outcomes | Effect (95% CI) | Quality of the evidence (GRADE) |
| Change in mean ± SD of MHDs after 3 months of combination treatment | MD −2.67, 95% CI −4.42 to −0.93; participants = 393 intervention and 496 baseline; studies = 5; I2 = 49% | ⊕⊕⊕⊝ moderate |
| CI: Confidence interval; MD: Mean difference. | ||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scuteri, D.; Tonin, P.; Nicotera, P.; Vulnera, M.; Altieri, G.C.; Tarsitano, A.; Bagetta, G.; Corasaniti, M.T. Pooled Analysis of Real-World Evidence Supports Anti-CGRP mAbs and OnabotulinumtoxinA Combined Trial in Chronic Migraine. Toxins 2022, 14, 529. https://doi.org/10.3390/toxins14080529
Scuteri D, Tonin P, Nicotera P, Vulnera M, Altieri GC, Tarsitano A, Bagetta G, Corasaniti MT. Pooled Analysis of Real-World Evidence Supports Anti-CGRP mAbs and OnabotulinumtoxinA Combined Trial in Chronic Migraine. Toxins. 2022; 14(8):529. https://doi.org/10.3390/toxins14080529
Chicago/Turabian StyleScuteri, Damiana, Paolo Tonin, Pierluigi Nicotera, Marilù Vulnera, Giuseppina Cristina Altieri, Assunta Tarsitano, Giacinto Bagetta, and Maria Tiziana Corasaniti. 2022. "Pooled Analysis of Real-World Evidence Supports Anti-CGRP mAbs and OnabotulinumtoxinA Combined Trial in Chronic Migraine" Toxins 14, no. 8: 529. https://doi.org/10.3390/toxins14080529
APA StyleScuteri, D., Tonin, P., Nicotera, P., Vulnera, M., Altieri, G. C., Tarsitano, A., Bagetta, G., & Corasaniti, M. T. (2022). Pooled Analysis of Real-World Evidence Supports Anti-CGRP mAbs and OnabotulinumtoxinA Combined Trial in Chronic Migraine. Toxins, 14(8), 529. https://doi.org/10.3390/toxins14080529