Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. IncoBTX-A Effect on Sweat Production
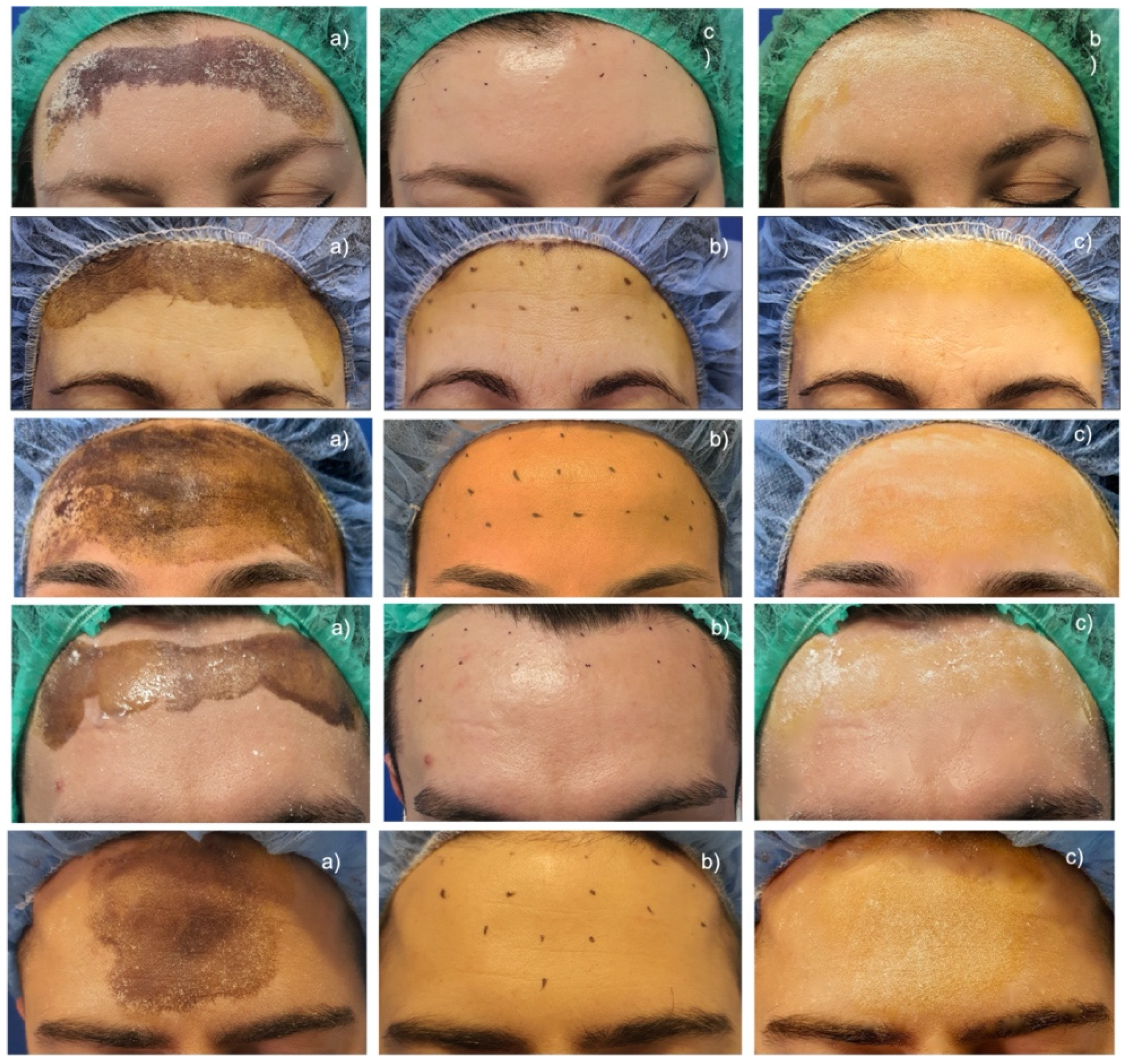
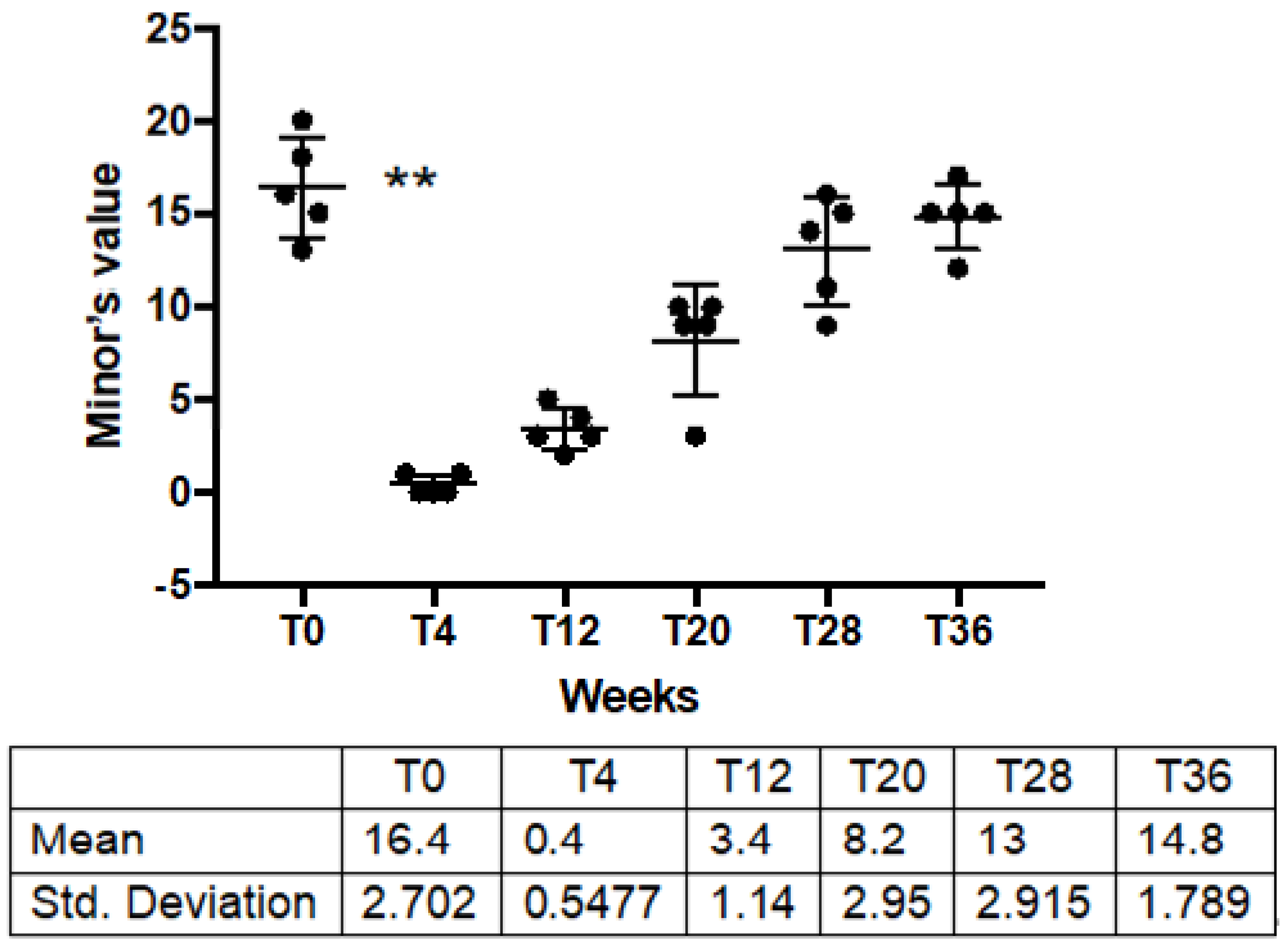
2.2. IncoBTX-A on Extent of Hyperhidrotic Area
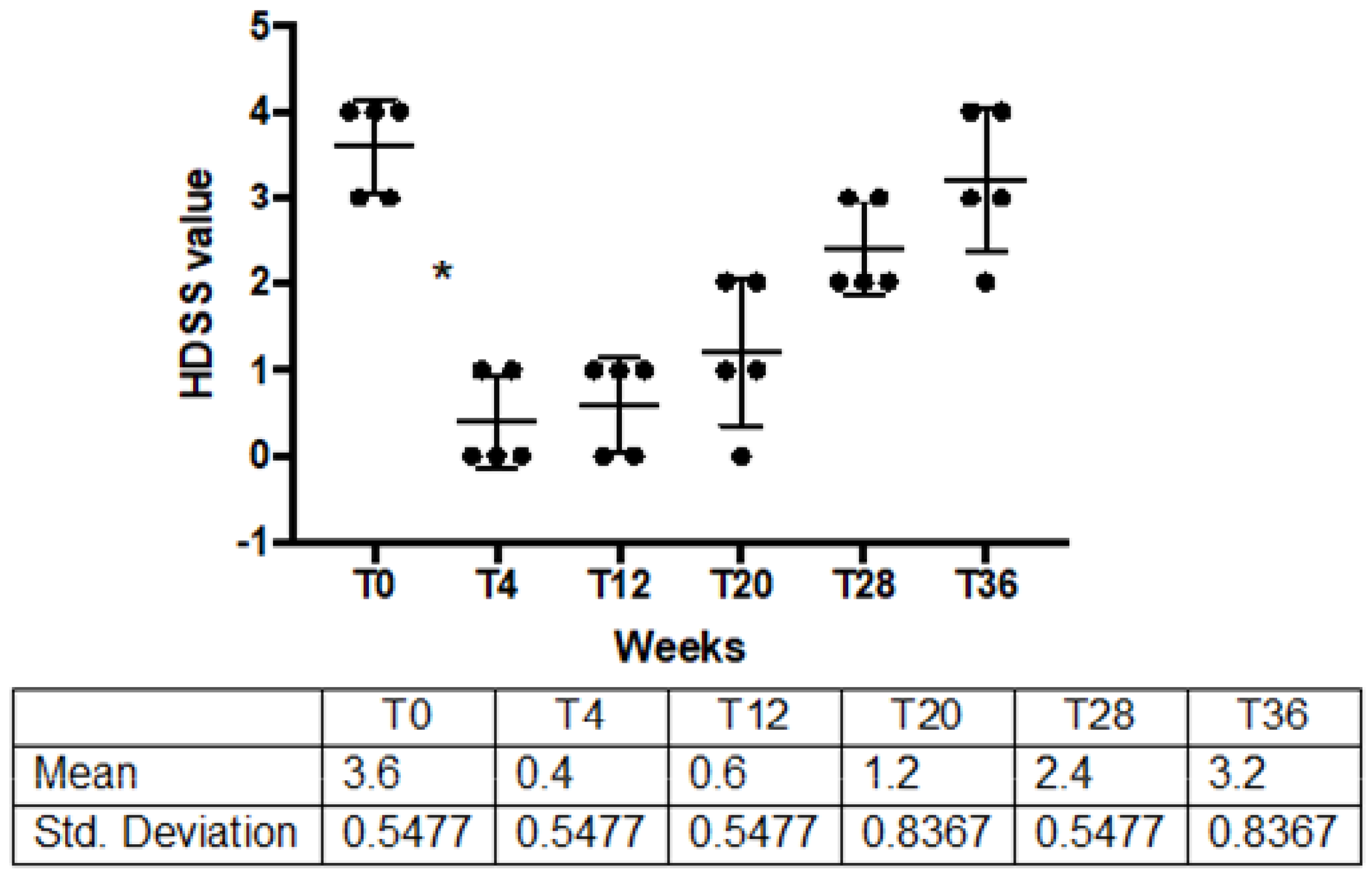
2.3. Patients’ Clinical Improvement
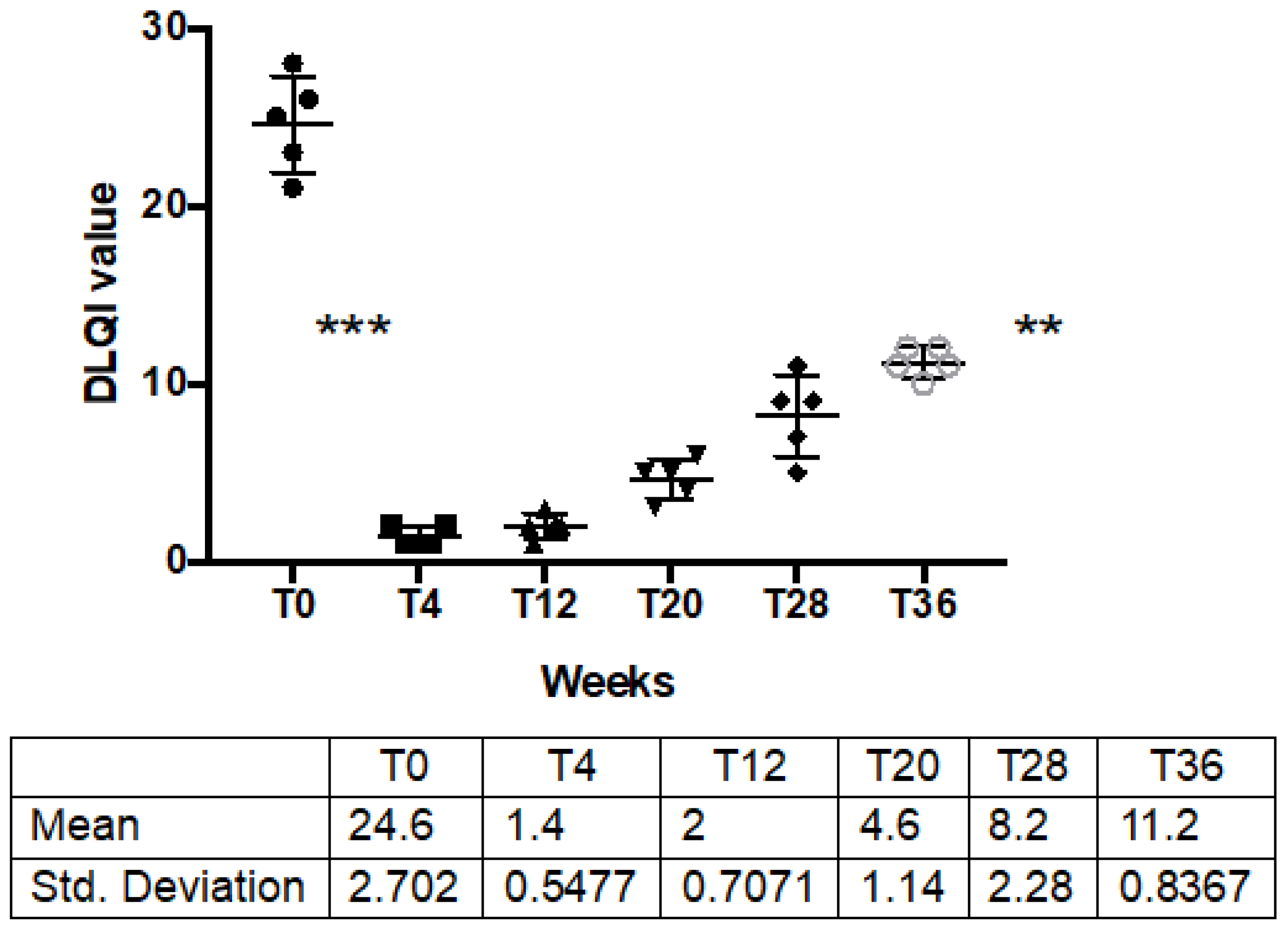
2.4. Patients’ Quality of Life
2.5. Safety Profile
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Patients | Type of BTX-A | Outcome and Methods | Results | AE |
|---|---|---|---|---|---|
| Böger et al. [17] | 12 | AboBTX-A injected in one-half of the forehead at the dosage of 2.5–4 ng | Effectiveness on frontal hyperidrosis assessed at T0 and after 4 weeks by - Minor’s iodine starch test | After 1–7 days the craniofacial sweating in the area injected had completely ceased in 11 patients and was mildly reduced in the remaining one. One patient had a relapse 9 months after treatment. | Mild weakness of frowning |
| Kinkelin et al. [18] | 10 | OnaBTX-A, injected intracutaneously at mean dosage of 86 mouse units | Effectiveness on frontal hyperidrosis assessed at T0 and after 4 weeks by: - Minor’s iodine-starch test - Gravimetric assessment - Photograph | Reduction of sweat after 4 weeks treatment, lasted at 5 months in nine of the 10 patients | Painful injections and a transient weakness of forehead muscles without ptosis |
| George et al. [19] | 4 | OnaBTX-A injected using a dose of 1–2 units per injection | Effectiveness on rarer forms of focal facial hyperidrosis (upper lip and chin, both cheeks, central face and frontal scalp respectively) assessed at T0 and after 6 weeks by Minor’s iodine-starch test | Reduction of sweat, lasted at mean 6–8 months after treatment. | Patient with frontal hyperhidrosis: loss of rhytides on her forehead and mild brow ptosis; Patient with perioral sweating: droop of his left upper lip. |
| Ko EJ et al. [20] | 2 | OnaBTX-A injected on the right of forehead (3.3 U), AboBTX-A injected on the middle (8.3 U) PraBTX-A injected on the left (3.3 U) All injections were of identical volume (0.1 mL). | Comparison of the efficacy and diffusion of three formulations of botulinum toxin type A in three different areas of the forehead by the following assesments at T0 and after 2 weeks: - Minor iodine–starch test - Transepidermal water loss (TEWL) - Corneometer | The area of diffusion appears to be greater with AboBTX-A covering 6.7% of the total area, while OnaBTX-A and PraBTX-A produced similarly sized areas of anhidrosis (2.5% and 2.6%, respectively). | Minimizing the area of diffusion is important to minimize the potential for adverse effects (AEs). |
| Ando Y et al. [23] | 15 | Not specified | Effectiveness on frontal hyperidrosis assessed at T0 and after 4 weeks by - Ventilation capsule method - Minor’s iodine-starch test. - HDSS - DLQI | Remarkable antiperspirants effect observed from 2 weeks after injection, and the effect last for approximately 30 weeks. | Two patients complained of transient mild ptosis |
4. Materials and Methods
4.1. Patients
4.2. Classification of Hyperhidrosis Severity
4.3. Quantification of Sweat Production
4.4. Identification of Hyperhidrotic Area Extension
4.5. Patients’ Quality-of-Life Evaluation
4.6. Treatment with IncoBTX-A
4.7. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, V.; Farshchian, M.; Potts, G.A. Management of Primary Focal Hyperhidrosis: An Algorithmic Approach. J. Drugs Dermatol. 2021, 20, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.A.; Galperin, T.A. Botulinum Toxin for Hyperhidrosis of Areas Other than the Axillae and Palms/Soles. Dermatol. Clin. 2014, 32, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Martina, E.; Giuliodori, K.; Consales, V.; Bobyr, I.; Offidani, A. Botulinum Toxin Off-Label Use in Dermatology: A Review. Ski. Appendage Disord. 2017, 3, 39–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanati, A.; Bernardini, M.L.; Gesuita, R.; Offidani, A. Plantar focal idiopathic hyperhidrosis and botulinum toxin: A pilot study. Eur. J. Dermatol. 2007, 17, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D. Five-year experience with incobotulinumtoxinA (Xeomin®): The first botulinum toxin drug free of complexing proteins. Eur. J. Neurol. 2012, 19, 385–389. [Google Scholar] [CrossRef]
- de Almeida, A.T.; Noriega, L.; Bechelli, L.; Suárez, M. Randomized Controlled Trial Comparing the Efficacy and Safety of Two Injection Techniques of IncobotulinumtoxinA for Axillary Hyperhidrosis. J. Drugs Dermatol. 2020, 19, 765–770. [Google Scholar] [CrossRef]
- Dressler, D. Comparing Botox® and Xeomin® for axillar hyperhidrosis. J. Neural Transm. 2010, 117, 317–319. [Google Scholar] [CrossRef]
- Dressler, D. Routine use of Xeomin® in patients previously treated with Botox®: Long term results. Eur. J. Neurol. 2009, 16 (Suppl. 2), 2–5. [Google Scholar] [CrossRef]
- Campanati, A.; Giuliodori, K.; Martina, E.; Giuliano, A.; Ganzetti, G.; Offidani, A. Onabotulinumtoxin type A (Botox®) versus Incobotulinumtoxin type A (Xeomin®) in the treatment of focal idiopathic palmar hyperhidrosis: Results of a comparative double-blind clinical trial. J. Neural Transm. (Vienna) 2013, 121, 21–26. [Google Scholar] [CrossRef]
- Bechara, F.G.; Sand, M.; Hoffmann, K.; Boorboor, P.; Altmeyer, P.; Stuecker, M. Histological and Clinical Findings in Different Surgical Strategies for Focal Axillary Hyperhidrosis. Dermatol. Surg. 2008, 34, 1001–1009. [Google Scholar] [CrossRef]
- Campanati, A.; De Blasio, S.; Giuliano, A.; Ganzetti, G.; Giuliodori, K.; Pecora, T.; Consales, V.; Minnetti, I.; Offidani, A. Topical ozonated oil versus hyaluronic gel for the treatment of partial- to full-thickness second-degree burns: A prospective, comparative, single-blind, non-randomised, controlled clinical trial. Burns 2013, 39, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.O.; Kil, H.K.; Yoon, K.B.; Yoon, D.M. Topical glycopyrrolate for patients with facial hyperhidrosis. Br. J. Dermatol. 2008, 158, 1094–1097. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.; Stewart, T.; Singh, B.; Singh, G.; Rosen, R. Retrospective analysis of the efficacy and duration of botulinum toxin A injections in 30 patients with palmar hyperhidrosis. Intern. Med. J. 2021, 51, 1517–1521. [Google Scholar] [CrossRef] [PubMed]
- Martina, E.; Diotallevi, F.; Radi, G.; Campanati, A.; Offidani, A. Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review. Toxins 2021, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Nawrocki, S.; Cha, J. Botulinum toxin: Pharmacology and injectable administration for the treatment of primary hyperhidrosis. J. Am. Acad. Dermatol. 2020, 82, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Lynch, O.E.; Aherne, T.; Gibbons, J.; Boland, M.R.; Ryan, J.; Boyle, E.; Egan, B.; Tierney, S. Five-year follow-up of patients treated with intra-dermal botulinum toxin for axillary hyperhidrosis. Ir. J. Med. Sci. 2020, 189, 1023–1026. [Google Scholar] [CrossRef]
- Wechter, T.; Feldman, S.R.; Taylor, S.L. The Treatment of Primary Focal Hyperhidrosis. Skin Ther. Lett. 2019, 24, 1–7. [Google Scholar]
- International Hyperhdrosis Society Official Website. Available online: https://www.sweathelp.org/medical-professional-resources.html (accessed on 5 May 2022).
- Böger, A.; Herath, H.; Rompel, R.; Ferbert, A. Botulinum toxin for treatment of craniofacial hyperhidrosis. J. Neurol. 2000, 247, 857–861. [Google Scholar] [CrossRef]
- Kinkelin, I.; Hund, M.; Naumann, M.; Hamm, H. Effective treatment of frontal hyperhidrosis with botulinum toxin A. Br. J. Dermatol. 2000, 143, 824–827. [Google Scholar] [CrossRef]
- George, S.M.C.; Atkinson, L.R.; Farrant, P.B.J.; Shergill, B.S. Botulinum toxin for focal hyperhidrosis of the face. Br. J. Dermatol. 2014, 170, 211–213. [Google Scholar] [CrossRef] [Green Version]
- Ko, E.J.; Mun, S.K.; Oh, I.Y.; Kwon, T.R.; Kim, B.J.; Kim, M.N. Comparison of efficacy and diffusion of three formulations of botulinum toxin type A in two patients with forehead hyperhidrosis. Clin. Exp. Dermatol. 2014, 39, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Lowe, P.L.; Patnaik, R.; Lowe, N.J. A Comparison of Two Botulinum Type A Toxin Preparations for the Treatment of Glabellar Lines: Double-Blind, Randomized, Pilot Study. Dermatol. Surg. 2005, 31, 1651–1654. [Google Scholar] [CrossRef] [PubMed]
- Aoki, R.; Francis, J.; Reynolds, H.; Leumer, D. Comparison of the therapeutic windows of different botulinum neurotoxin preparations in an animal model. Neurology 2003, 60 (Suppl. 1), A212–A213. [Google Scholar]
- Ando, Y.; Ohshima, Y.; Yanagishita, T.; Watanabe, H.; Tamada, Y.; Akiyama, M.; Watanabe, D. Clinical utility of botulinum toxin type A local injection therapy for head and forehead hyperhidrosis. J. Dermatol. 2022. Early View. [Google Scholar] [CrossRef] [PubMed]
- Frevert, J. Xeomin®: An innovative new botulinum toxin type A. Eur. J. Neurol. 2009, 16 (Suppl. 2), 11–13. [Google Scholar] [CrossRef]
- Frevert, J. Xeomin® is free from complexing proteins. Toxicon 2009, 54, 697–701. [Google Scholar] [CrossRef]
- Samadzadeh, S.; Ürer, B.; Brauns, R.; Rosenthal, D.; Lee, J.-I.; Albrecht, P.; Hefter, H. Clinical Implications of Difference in Antigenicity of Different Botulinum Neurotoxin Type A Preparations: Clinical Take-Home Messages from Our Research Pool and Literature. Toxins 2020, 12, 499. [Google Scholar] [CrossRef]
- Eisele, K.-H.; Fink, K.; Vey, M.; Taylor, H.V. Studies on the dissociation of botulinum neurotoxin type A complexes. Toxicon 2010, 57, 555–565. [Google Scholar] [CrossRef]
- Campanati, A.; Sandroni, L.; Gesuita, R.; Giuliano, A.; Giuliodori, K.; Marconi, B.; Ganzetti, G.; Offidani, A. Treatment of focal idiopathic hyperhidrosis with Botulinum Toxin Type A: Clinical predictive factors of relapse-free survival. J. Eur. Acad. Dermatol. Venereol. 2010, 25, 917–921. [Google Scholar] [CrossRef]
- Campanati, A.; Giuliodori, K.; Giuliano, A.; Martina, E.; Ganzetti, G.; Marconi, B.; Chiarici, A.; Offidani, A. Treatment of palmar hyperhidrosis with botulinum toxin type A: Results of a pilot study based on a novel injective approach. Arch. Dermatol. Res. 2013, 305, 691–697. [Google Scholar] [CrossRef]
- Solish, N.; Bertucci, V.; Dansereau, A.; Hong, H.C.-H.; Lynde, C.; Lupin, M.; Smith, K.C.; Storwick, G. A Comprehensive Approach to the Recognition, Diagnosis, and Severity-Based Treatment of Focal Hyperhidrosis: Recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol. Surg. 2007, 33, 908–923. [Google Scholar] [CrossRef] [PubMed]
- Hexsel, D.; Rodrigues, T.C.; Soirefmann, M.; Prado, D.Z. Recommendations for Performing and Evaluating the Results of the Minor Test According to a Sweating Intensity Visual Scale. Dermatol. Surg. 2010, 36, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Khan, G.K. Dermatology life quality index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]





| Pz (n) | 1 | 2 | 3 | 4 | 5 | p |
|---|---|---|---|---|---|---|
| Sweat production T0 (gr/15 min) | 0.218 | 0.201 | 0.161 | 0.155 | 0.819 | p = 0.009 |
| Sweat production T4 (gr/15 min) | 0.093 | 0.161 | 0.087 | 0.112 | 0.099 | |
| Minor’s iodine starch test T0 | 20 | 18 | 15 | 16 | 13 | p = 0.004 |
| Minor’s iodine starch test T4 | 0 | 1 | 1 | 0 | 0 | |
| HDSS T0 | 4 | 4 | 3 | 3 | 4 | p = 0.001 |
| HDSS T4 | 1 | 0 | 0 | 0 | 1 | |
| DLQI T0 | 28 | 23 | 25 | 21 | 26 | p = 0.0007 |
| DLQI T4 | 1 | 2 | 2 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campanati, A.; Martina, E.; Gregoriou, S.; Kontochristopoulos, G.; Paolinelli, M.; Diotallevi, F.; Radi, G.; Bobyr, I.; Marconi, B.; Gualdi, G.; et al. Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature. Toxins 2022, 14, 372. https://doi.org/10.3390/toxins14060372
Campanati A, Martina E, Gregoriou S, Kontochristopoulos G, Paolinelli M, Diotallevi F, Radi G, Bobyr I, Marconi B, Gualdi G, et al. Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature. Toxins. 2022; 14(6):372. https://doi.org/10.3390/toxins14060372
Chicago/Turabian StyleCampanati, Anna, Emanuela Martina, Stamatis Gregoriou, George Kontochristopoulos, Matteo Paolinelli, Federico Diotallevi, Giulia Radi, Ivan Bobyr, Barbara Marconi, Giulio Gualdi, and et al. 2022. "Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature" Toxins 14, no. 6: 372. https://doi.org/10.3390/toxins14060372
APA StyleCampanati, A., Martina, E., Gregoriou, S., Kontochristopoulos, G., Paolinelli, M., Diotallevi, F., Radi, G., Bobyr, I., Marconi, B., Gualdi, G., Amerio, P., & Offidani, A. (2022). Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature. Toxins, 14(6), 372. https://doi.org/10.3390/toxins14060372