Effective Locations for Injecting Botulinum Toxin into the Mentalis Muscle; Cadaveric and Ultrasonographic Study



Abstract
1. Introduction
2. Results
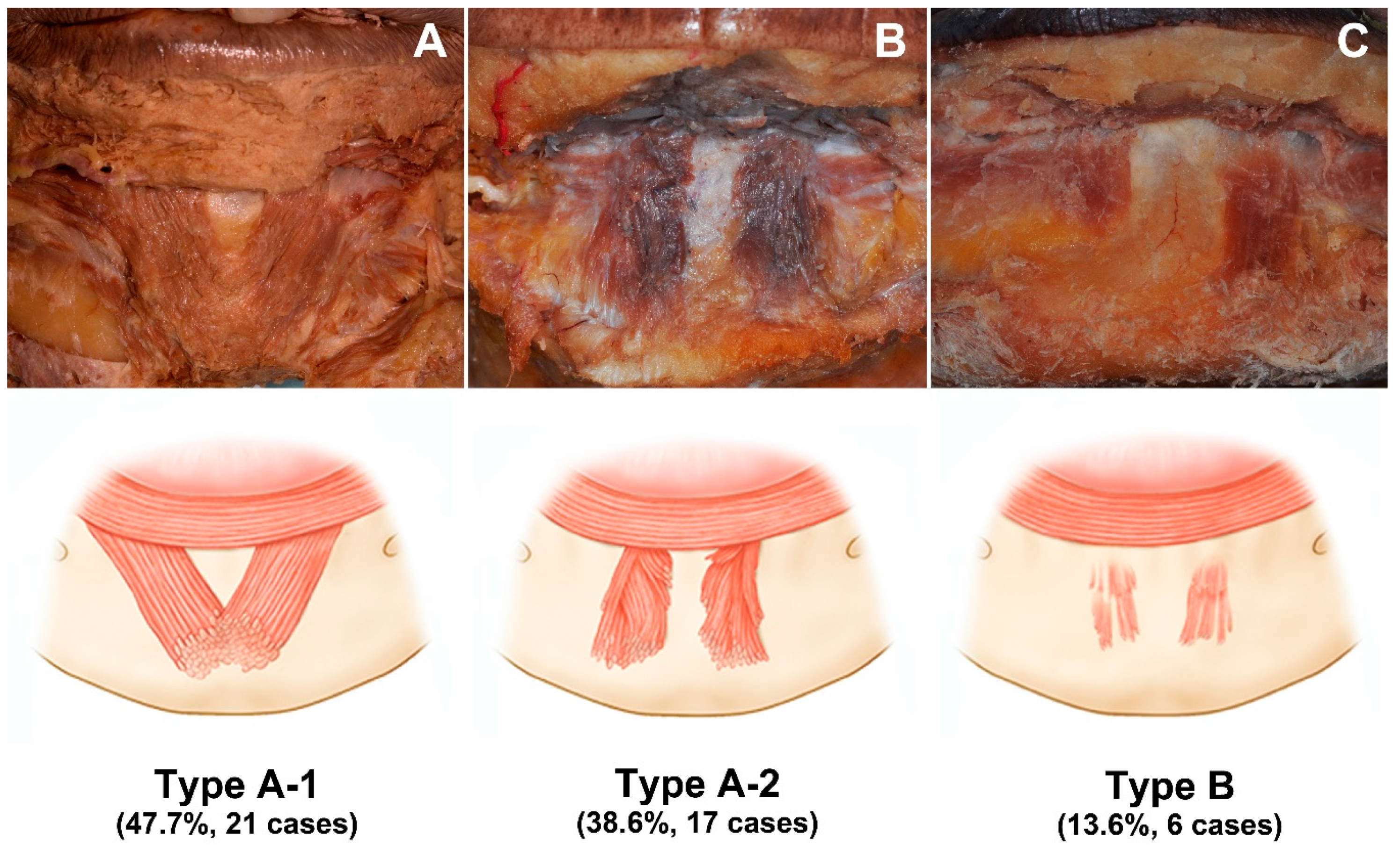
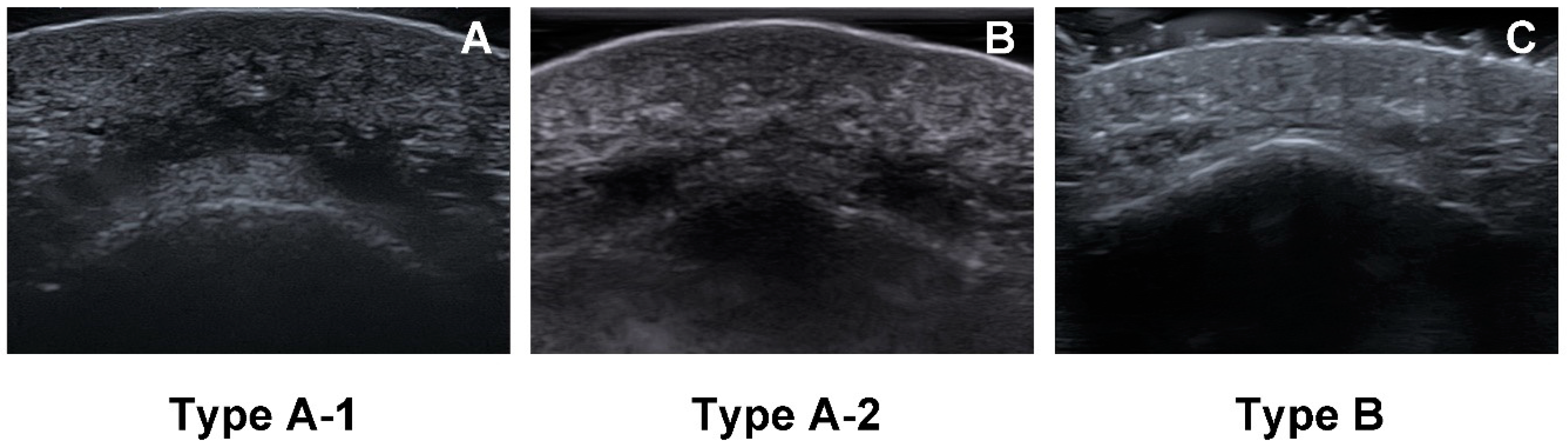
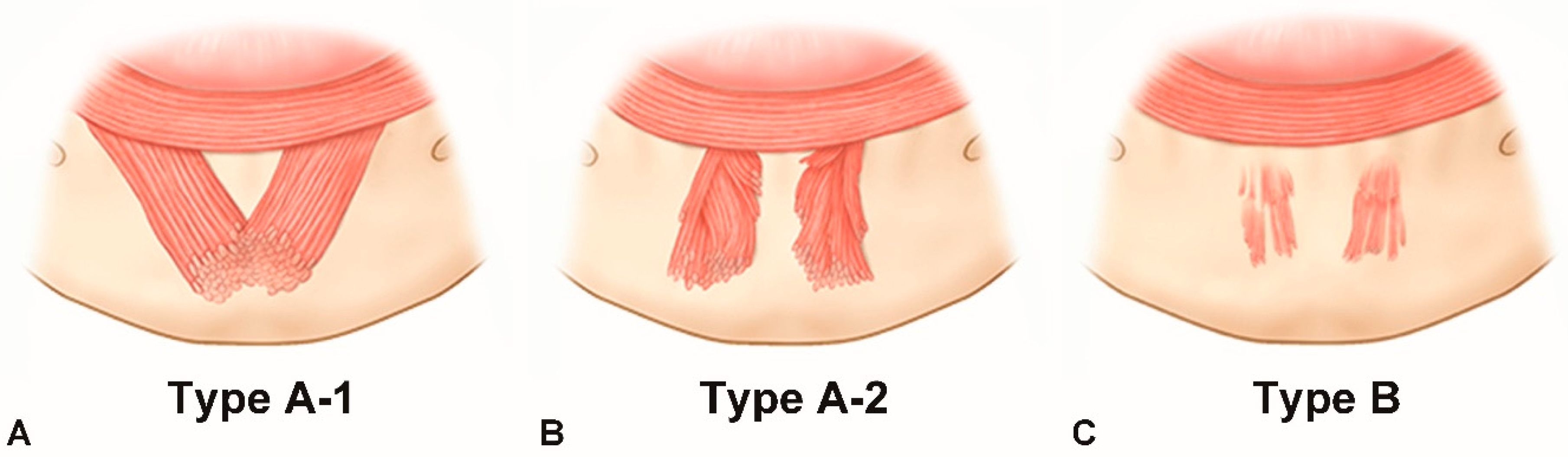
2.1. Morphology of the Mentalis Muscle
2.2. Location of the Mentalis Muscle
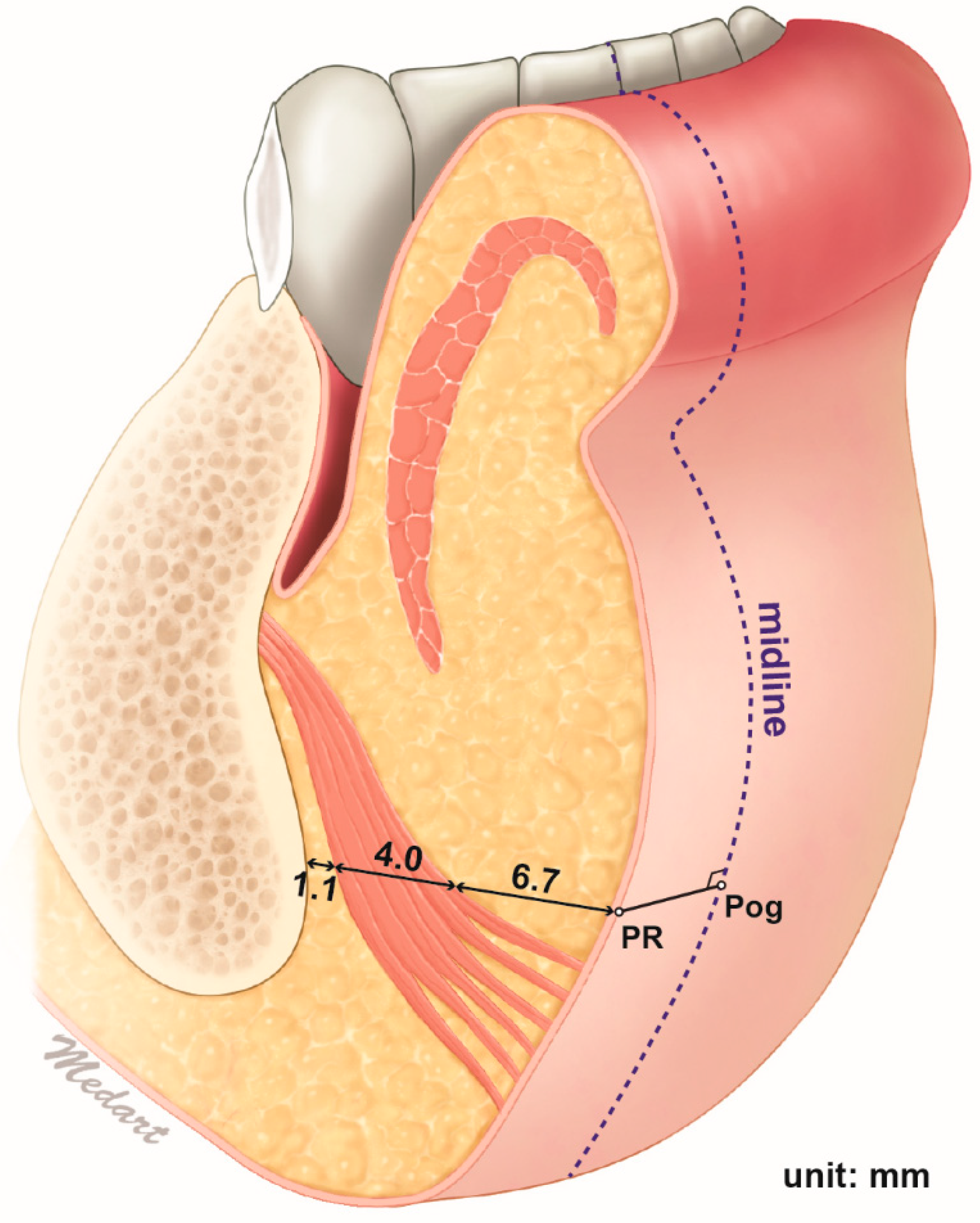
2.3. Depth of the Mentalis Muscle
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Morphology of the Mentalis Muscle
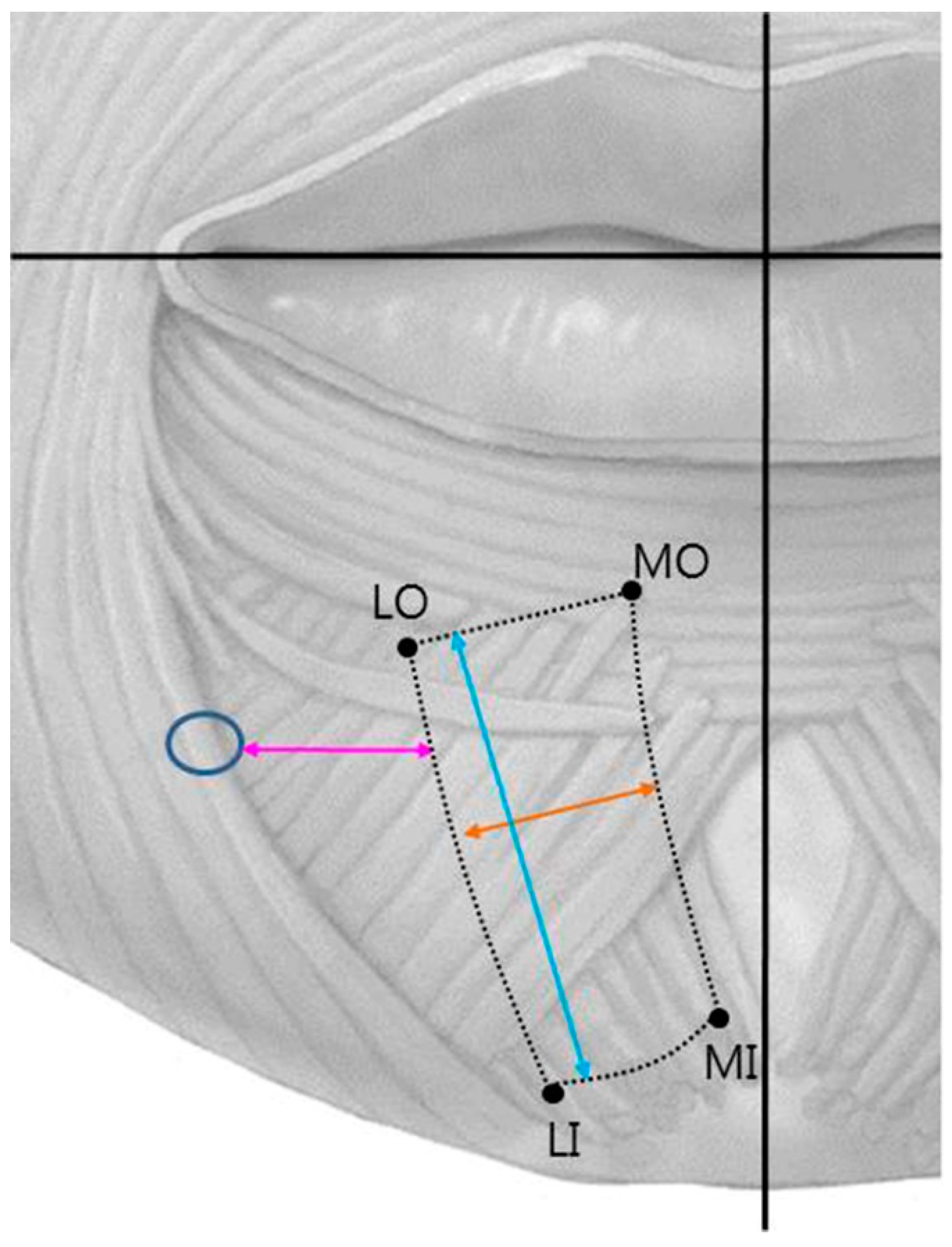
5.2. Location of the Mentalis Muscle
- MO location.
- LO location.
- MI location.
- LI location.
- Length of the mentalis muscle.
- Width of the mentalis muscle.
- Distance between the mental foramen and the lateral margin of the mentalis muscle.
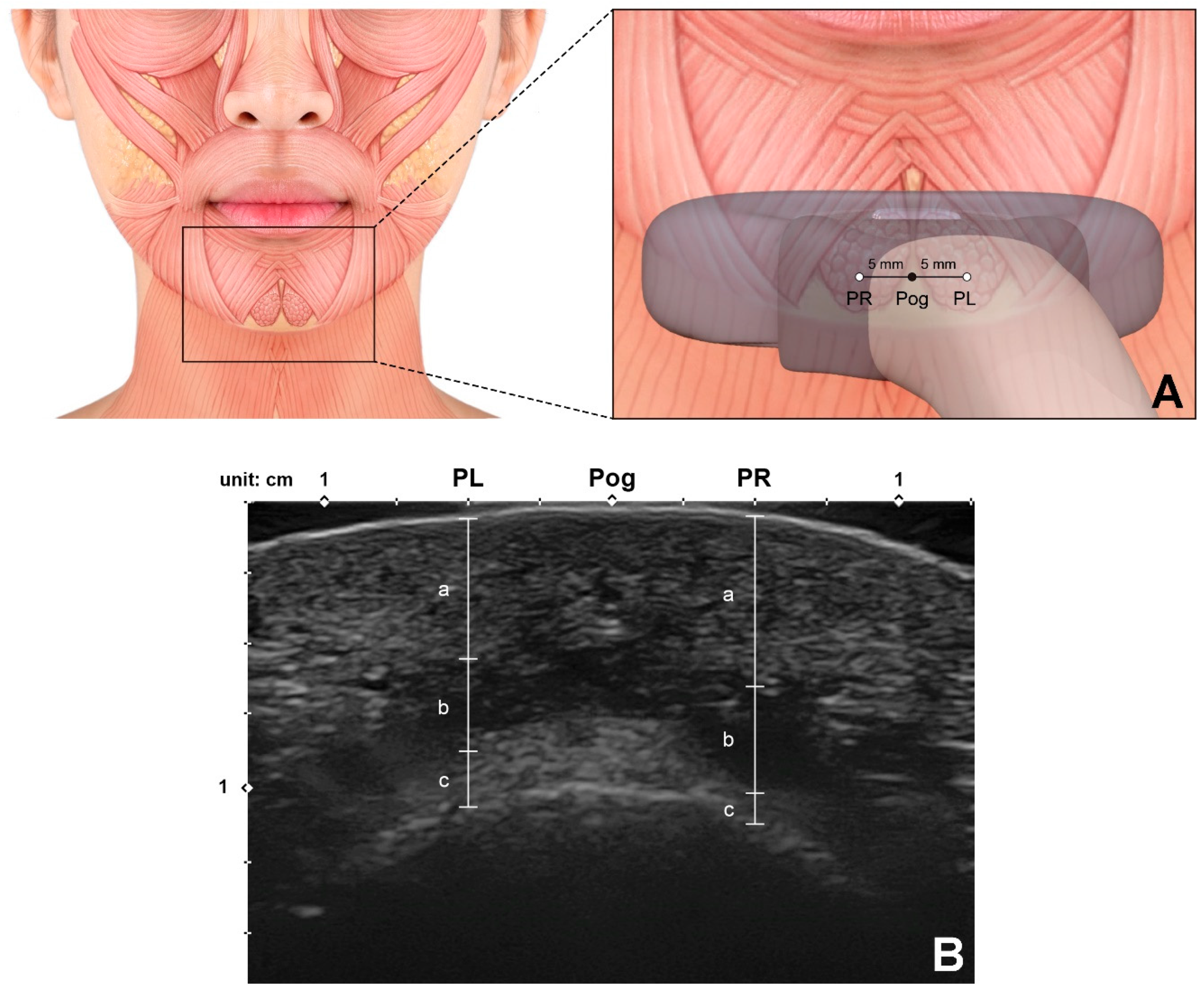
5.3. Depth of the Mentalis Muscle
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garfein, E.S.; Zide, B.M. Chin ptosis: Classification, anatomy, and correction. Craniomaxillofacial Trauma Reconstr. 2008, 1, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hur, M.-S.; Kim, H.-J.; Choi, B.-Y.; Hu, K.-S.; Kim, H.-J.; Lee, K.-S. Morphology of the mentalis muscle and its relationship with the orbicularis oris and incisivus labii inferioris muscles. J. Craniofacial Surg. 2013, 24, 602–604. [Google Scholar] [CrossRef] [PubMed]
- Zide, B.M.; McCarthy, J. The mentalis muscle: An essential component of chin and lower lip position. Plast. Reconstr. Surg. 1989, 83, 413–420. [Google Scholar] [CrossRef]
- Kim, H.-J.; Seo, K.K.; Lee, H.-K.; Kim, J. General Anatomy of the Face and Neck. In Clinical Anatomy of the Face for Filler and Botulinum Toxin Injection; Springer: Singapore, 2016; pp. 1–53. [Google Scholar]
- Coleman, K.R.; Carruthers, J. Combination therapy with BOTOX™ and fillers: The new rejuvnation paradigm. Dermatol. Ther. 2006, 19, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Ulloa, M. Ptosis of the chin: The witches’ chin. Plast. Reconstr. Surg. 1972, 50, 54–57. [Google Scholar] [CrossRef]
- Zide, B.M. The mentalis muscle: An essential component of chin and lower lip position. Plast. Reconstr. Surg. 2000, 105, 1213–1215.s. [Google Scholar] [CrossRef]
- Carruthers, J.; Carruthers, A. Aesthetic botulinum A toxin in the mid and lower face and neck. Dermatol. Surg. 2003, 29, 468–476. [Google Scholar]
- Guyuron, B.; Huddleston, S.W. Aesthetic indications for botulinum toxin injection. Plast. Reconstr. Surg. 1994, 93, 913–918. [Google Scholar] [CrossRef]
- Klein, A.W. Contraindications and complications with the use of botulinum toxin. Clin. Dermatol. 2004, 22, 66–75. [Google Scholar] [CrossRef]
- Garcia, A.; Fulton, J.E., Jr. Cosmetic denervation of the muscles of facial expression with botulinum toxin A dose-response study. Dermatol. Surg. 1996, 22, 39–43. [Google Scholar] [CrossRef]
- Alfen, N.V.; Gilhuis, H.J.; Keijzers, J.P.; Pillen, S.; Van Dijk, J.P. Quantitative facial muscle ultrasound: Feasibility and reproducibility. Muscle Nerve 2013, 48, 375–380. [Google Scholar] [CrossRef]
- Le Louarn, C. Botulinum toxin A and facial lines: The variable concentration. Aesthetic Plast. Surg. 2001, 25, 73–84. [Google Scholar] [CrossRef]
- Mahant, N.; Clouston, P.; Lorentz, I. The current use of botulinum toxin. J. Clin. Neurosci. 2000, 7, 389–394. [Google Scholar] [CrossRef]
- Klein, A.W. Complications and adverse reactions with the use of botulinum toxin. Dis.-A-Mon. 2002, 48, 336–356. [Google Scholar] [CrossRef] [PubMed]
- Standring, S. Gray’s Anatomy e-Book: The Anatomical Basis of Clinical Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Shannon, J.L. The mentalis muscle in relation to edentulous mandibles. J. Prosthet. Dent. 1972, 27, 477–484. [Google Scholar] [CrossRef]
- Iwanaga, J.; He, P.; Watanabe, K.; Kamura, Y.; Oskouian, R.J.; Tubbs, R.S. Intraoral observation of the mentalis and incisivus labii inferioris muscles. J. Craniofacial Surg. 2017, 28, 2159–2161. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Choi, Y.J.; Lee, K.W.; Hu, K.S.; Kim, S.T.; Kim, H.J. Ultrasonography of the internal architecture of the superficial part of the masseter muscle in vivo. Clin. Anat. 2019, 32, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.-J.; Lee, K.-W.; Gil, Y.-C.; Hu, K.-S.; Kim, H.-J. Ultrasonographic Analyses of the Forehead Region for Injectable Treatments. Ultrasound Med. Biol. 2019, 45, 2641–2648. [Google Scholar] [CrossRef]
- Volk, G.F.; Wystub, N.; Pohlmann, M.; Finkensieper, M.; Chalmers, H.J.; Guntinas-Lichius, O. Quantitative ultrasonography of facial muscles. Muscle Nerve 2013, 47, 878–883. [Google Scholar] [CrossRef]
- Yu, N.; Liu, Y.; Chen, C.; Dong, R.; Yang, E.; Wang, X. Paradoxical bulging of mentalis after botulinum toxin type A injection. J. Cosmet. Dermatol. 2020, 19, 1290–1293. [Google Scholar] [CrossRef]
- Borodic, G.E.; Joseph, M.; Fay, L.; Cozzolino, D.; Ferrante, R.J. Botulinum A toxin for the treatment of spasmodic torticollis: Dysphagia and regional toxin spread. Head Neck 1990, 12, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Shaari, C.M.; George, E.; Wu, B.L.; Biller, H.F.; Sanders, I. Quantifying the spread of botulinum toxin through muscle fascia. Laryngoscope 1991, 101, 960–964. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distance from Midline | Distance from Horizontal Line | |
|---|---|---|
| Point MO | 4.1 ± 1.8 | 20.5 ± 3.7 |
| Point LO | 13.1 ± 3.4 | 21.3 ± 4.0 |
| Point MI | 1.8 ± 2.0 | 32.7 ± 4.6 |
| Point LI | 10.4 ± 3.2 | 35.1 ± 4.5 |
| Length | 18.0 ± 3.9 | |
| Width | 10.9 ± 3.0 | |
| Distance from mental foramen | 16.7 ± 3.8 | |
| Depth Below Skin Surface | Muscle Thickness | Distance from Bone | |
|---|---|---|---|
| Left | 6.7 ± 1.4 | 3.9 ± 1.4 | 1.0 ± 1.1 |
| Right | 6.6 ± 1.4 | 4.0 ± 1.3 | 1.0 ± 0.9 |
| Total | 6.6 ± 1.4 | 3.9 ± 1.4 | 1.0 ± 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, D.-Y.; Bae, H.; Bae, J.-H.; Kim, H.-J.; Hu, K.-S. Effective Locations for Injecting Botulinum Toxin into the Mentalis Muscle; Cadaveric and Ultrasonographic Study. Toxins 2021, 13, 96. https://doi.org/10.3390/toxins13020096
Choi D-Y, Bae H, Bae J-H, Kim H-J, Hu K-S. Effective Locations for Injecting Botulinum Toxin into the Mentalis Muscle; Cadaveric and Ultrasonographic Study. Toxins. 2021; 13(2):96. https://doi.org/10.3390/toxins13020096
Chicago/Turabian StyleChoi, Da-Yae, Hyungkyu Bae, Jung-Hee Bae, Hee-Jin Kim, and Kyung-Seok Hu. 2021. "Effective Locations for Injecting Botulinum Toxin into the Mentalis Muscle; Cadaveric and Ultrasonographic Study" Toxins 13, no. 2: 96. https://doi.org/10.3390/toxins13020096
APA StyleChoi, D.-Y., Bae, H., Bae, J.-H., Kim, H.-J., & Hu, K.-S. (2021). Effective Locations for Injecting Botulinum Toxin into the Mentalis Muscle; Cadaveric and Ultrasonographic Study. Toxins, 13(2), 96. https://doi.org/10.3390/toxins13020096