Carbamoylated Nail Proteins as Assessed by Near-Infrared Analysis Are Associated with Load of Uremic Toxins and Mortality in Hemodialysis Patients

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Results
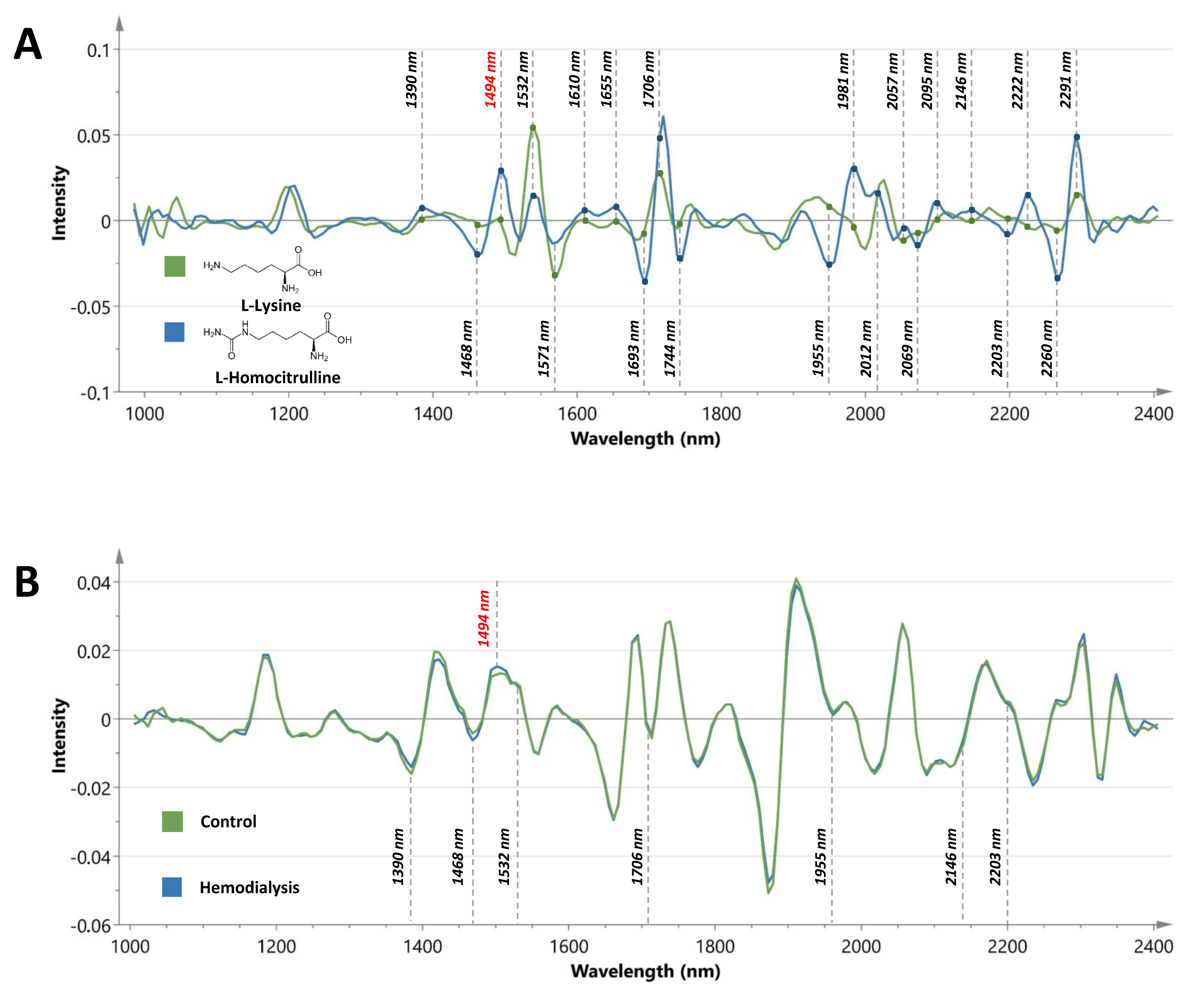
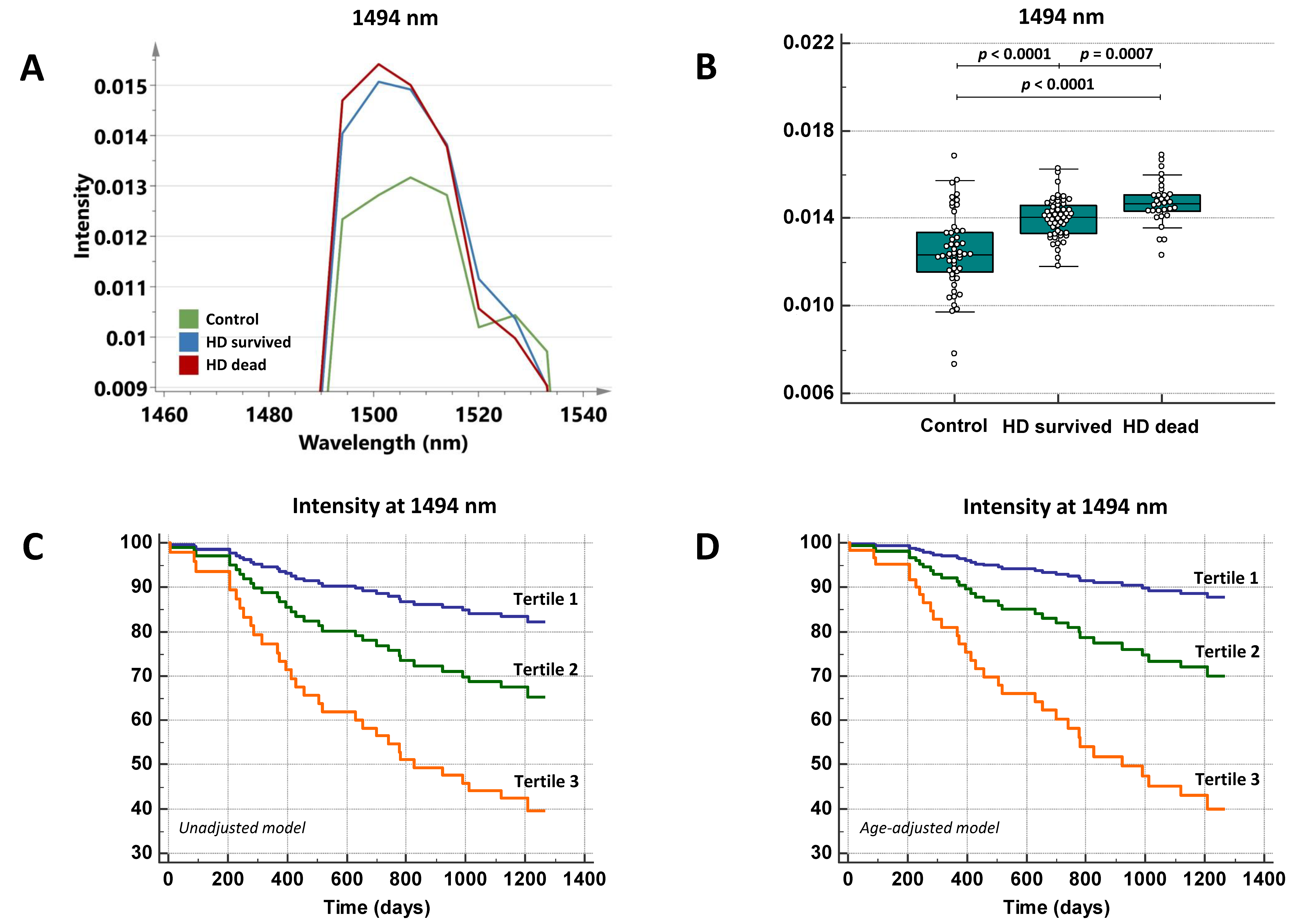
2.1. The Peak Intensity at 1494 nm Is Significantly Higher in Hemodialysis Patients Versus Controls
2.2. The Spectral Marker at 1494 nm Is Associated with Age and Uremic Toxins
2.3. The Spectral Marker Has Prognostic Utility among Hemodialysis Patients
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Research Participants and Specimen Collection
5.2. Study Parameters
5.3. Near-Infrared Spectroscopy
5.4. Spectral Data Analysis
5.5. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bruck, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Vo lzke, H.; A. rnlo v, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 2016, 27, 2135–2147. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, S.; Delanghe, J.R.; Speeckaert, R.; Van Biesen, W.; Speeckaert, M.M. Mechanisms and consequences of carbamoylation. Nat. Rev. Nephrol. 2017, 13, 580–593. [Google Scholar] [CrossRef]
- Gajjala, P.R.; Fliser, D.; Speer, T.; Jankowski, V.; Jankowski, J. Emerging role of post-translational modifications in chronic kidney disease and cardiovascular disease. Nephrol. Dial. Transplant. 2015, 30, 1814–1824. [Google Scholar] [CrossRef] [PubMed]
- Jaisson, S.; Pietrement, C.; Gillery, P. Carbamylation-derived products: Bioactive compounds and potential biomarkers in chronic renal failure and atherosclerosis. Clin. Chem. 2011, 57, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, S.; Moerman, A.; Pletinck, A.; Schepers, E.; Glorieux, G.; Van Biesen, W.; Speeckaert, M.M. Quantification of carbamylated albumin in serum based on capillary electrophoresis. Electrophoresis 2017, 38, 2135–2140. [Google Scholar] [CrossRef] [PubMed]
- Jaisson, S.; Kazes, I.; Desmons, A.; Fadel, F.; Oudart, J.B.; Santos-Weiss, I.C.R.D.; Millart, H.; Touré, F.; Rieu, P.; Gillery, P. Homocitrulline as marker of protein carbamylation in hemodialyzed patients. Clin. Chim. Acta 2016, 460, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, S.; Speeckaert, M.; De Bruyne, S.; Delanghe, J. On the nature of toenail opacities in renal insufficiency. Clin. Exp. Nephrol. 2018, 23, 146–147. [Google Scholar] [CrossRef]
- Coopman, R.; Van de Vyver, T.; Kishabongo, A.S.; Katchunga, P.; Van Aken, E.H.; Cikomola, J.; Monteyne, T.; Speeckaert, M.M.; Delanghe, J.R. Glycation in human fingernail clippings using ATR-FTIR spectrometry, a new marker for the diagnosis and monitoring of diabetes mellitus. Clin. Biochem. 2017, 50, 62–67. [Google Scholar] [CrossRef]
- Reich, G. Near-infrared spectroscopy and imaging: Basic principles and pharmaceutical applications. Adv. Drug Deliv. Rev. 2005, 57, 1109–1143. [Google Scholar] [CrossRef]
- Verbrugge, F.H.; Tang, W.H.W.; Hazen, S.L. Protein carbamylation and cardiovascular disease. Kidney Int. 2015, 88, 474–478. [Google Scholar] [CrossRef]
- Eloot, S.; Van Biesen, W.; Glorieux, G.; Neirynck, N.; Dhondt, A.; Vanholder, R. Does the adequacy parameter kt/vurea reflect uremic toxin concentrations in hemodialysis patients? PLoS ONE 2013, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Snauwaert, E.; Van Biesen, W.; Raes, A.; Holvoet, E.; Glorieux, G.; Van Hoeck, K.; Van Dyck, M.; Godefroid, N.; Vanholder, R.; Roels, S.; et al. Accumulation of uraemic toxins is reflected only partially by estimated GFR in paediatric patients with chronic kidney disease. Pediatr. Nephrol. 2018, 33, 315–323. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, S.; Speeckaert, M.M.; Delanghe, J.R. Applications of mid-infrared spectroscopy in the clinical laboratory setting. Crit. Rev. Clin. Lab. Sci. 2018, 55, 1–20. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, S.; Speeckaert, R.; Boelens, J.; Hayette, M.-P.P.M.-P.; Speeckaert, M.; Delanghe, J. Infrared spectroscopy as a novel tool to diagnose onychomycosis. Br. J. Dermatol. 2019, 180, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Cashman, M.W.; Sloan, S.B. Nutrition and nail disease. Clin. Dermatol. 2010, 24, 420–425. [Google Scholar] [CrossRef]
- Berg, A.H.; Drechsler, C.; Wenger, J.; Buccafusca, R.; Hod, T.; Kalim, S.; Ramma, W.; Parikh, S.M.; Steen, H.; Friedman, D.J.; et al. Carbamylation of serum albumin as a risk factor for mortality in patients with kidney failure. Sci. Transl. Med. 2013, 5, 175ra29. [Google Scholar] [CrossRef] [PubMed]
- Jaisson, S.; Desmons, A.; Doué, M.; Gorisse, L.; Pietrement, C.; Gillery, P. Measurement of Homocitrulline, A Carbamylation-derived Product, in Serum and Tissues by LC-MS/MS. Curr. Protoc. Protein Sci. 2018, 92, e56. [Google Scholar] [CrossRef] [PubMed]
- Gorisse, L.; Pietrement, C.; Vuiblet, V.; Schmelzer, C.E.H.; Köhler, M.; Duca, L.; Debelle, L.; Fornès, P.; Jaisson, S.; Gillery, P. Protein carbamylation is a hallmark of aging. Proc. Natl. Acad. Sci. USA 2016, 113, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Carracedo, J.; Ramírez-Carracedo, R.; de Toda, I.M.; Vida, C.; Alique, M.; De la Fuente, M.; Ramírez-Chamond, R. Protein carbamylation: A marker reflecting increased age-related cell oxidation. Int. J. Mol. Sci. 2018, 19, 1495. [Google Scholar] [CrossRef]
- Nicolas, C.; Jaisson, S.; Gorisse, L.; Tessier, F.J.; Niquet-Léridon, C.; Jacolot, P.; Pietrement, C.; Gillery, P. Carbamylation is a competitor of glycation for protein modification in vivo. Diabetes Metab. 2018, 44, 160–167. [Google Scholar] [CrossRef]
- Delanghe, S.E.; De Bruyne, S.; De Baene, L.; Van Biesen, W.; Speeckaert, M.; Delanghe, J. Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy. J. Clin. Med. 2019, 8, 774. [Google Scholar] [CrossRef] [PubMed]
- Pavone, B.; Sirolli, V.; Giardinelli, A.; Bucci, S.; Forlì, F.; di Cesare, M.; Sacchetta, P.; di Pietro, N.; Pandolfi, A.; Urbani, A.; et al. Plasma protein carbonylation in chronic uremia. J. Nephrol. 2011, 24, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Snauwaert, E.; Holvoet, E.; Van Biesen, W.; Raes, A.; Glorieux, G.; Walle, J.V.; Roels, S.; Vanholder, R.; Askiti, V.; Azukaitis, K.; et al. Uremic toxin concentrations are related to residual kidney function in the pediatric hemodialysis population. Toxins 2019, 11, 235. [Google Scholar] [CrossRef] [PubMed]
- Eloot, S.; Van Biesen, W.; Roels, S.; Delrue, W.; Schepers, E.; Dhondt, A.; Vanholder, R.; Glorieux, G. Spontaneous variability of pre-dialysis concentrations of uremic toxins over time in stable hemodialysis patients. PLoS ONE 2017, 12, e0186010. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J.; Russell, L.; Bryan, J.; Phillips, L.; Russell, G.I. Comorbidity, urea kinetics, and appetite in continuous ambulatory peritoneal dialysis patients: Their interrelationship and prediction of survival. Am. J. Kidney Dis. 1995, 26, 353–361. [Google Scholar] [CrossRef]
- Davies, S.J.; Philips, L.; Naish, P.F.; Russell, G.I. Quantifying comorbidity in peritoneal dialysis patients and its relationship to other predictors of survival. Nephrol. Dial. Transplant. 2002, 17, 1085–1092. [Google Scholar] [CrossRef]
- Monteyne, T.; Coopman, R.; Kishabongo, A.S.; Himpe, J.; Lapauw, B.; Shadid, S.; Van Aken, E.H.; Berenson, D.; Speeckaert, M.M.; De Beer, T.; et al. Analysis of protein glycation in human fingernail clippings with near-infrared (NIR) spectroscopy as an alternative technique for the diagnosis of diabetes mellitus. Clin. Chem. Lab. Med. 2018, 56, 1551–1558. [Google Scholar] [CrossRef]
- De Bruyne, S.; Van Dorpe, J.; Himpe, J.; Van Biesen, W.; Delanghe, S.; Speeckaert, M.M.; Delanghe, J.R. Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections. J. Clin. Med. 2019, 8, 1022. [Google Scholar] [CrossRef]
- Song, X.-C.; Lin, Q.-B.; Zhang, Y.-C.; Li, Z.; Zeng, Y.; Chen, Z.-F. Rapid classification of virgin and recycled EPS containers by Fourier transform infrared spectroscopy and chemometrics. Food Addit. Contam. Part. A 2018, 35, 2220–2229. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control (n = 53) | HD (n = 84) |
|---|---|---|
| Demographic and Clinical | ||
| Age (yr) | 34.8 (27.5–43.5) | 73.7 (62.0–81.3) |
| Male/female ratio | 18/35 | 52/32 |
| Caucasian (%) | 100 | 100 |
| History of CVD (%) | 0 | 59.5 |
| Diabetes mellitus (%) | 0 | 35.7 |
| BMI (kg/m2) | 23.2 (20.6–25.7) | 26.1 (23.4–29.1) |
| Laboratory | ||
| Creatinine (mg/dL) | 0.9 (0.8–1.0) | 7.0 (5.0–8.8) |
| CRP (mg/L) | 1.1 (0.7–2.8) | 4.7 (1.9–10.8) |
| Total protein (g/L) | 74.0 (69.9–81.5) | 66.0 (62.5–69.6) |
| Urea (mg/dL) | 26.7 (22.8–31.7) | 99.0 (74.5–127.0) |
| IS total (mg/dL) | 0.06 (0.04–0.08) | 1.8 (1.0–2.6) |
| IS free (mg/dL) | 0.001 (0.0005–0.001) | 0.09 (0.05–0.2) |
| PCS total (mg/dL) | 0.2 (0.1–0.3) | 3.2 (2.0–4.2) |
| PCS free (mg/dL) | 0.008 (0.003–0.01) | 0.2 (0.1–0.3) |
| PCG total (mg/dL) | 0.001 (0.001–0.001) | 0.2 (0.1–0.4) |
| PCG free (mg/dL) | 0.001 (0.001–0.001) | 0.2 (0.08–0.4) |
| IAA total (mg/dL) | 0.03 (0.02–0.03) | 0.1 (0.1–0.2) |
| IAA free (mg/dL) | 0.001 (0.001–0.002) | 0.04 (0.03–0.06) |
| CMPF (mg/dL) | 0.05 (0.01–0.1) | 0.5 (0.3–0.9) |
| HA total (mg/dL) | 0.07 (0.05–0.1) | 2.7 (1.0–4.7) |
| HA free (mg/dL) | 0.02 (0.006–0.04) | 1.1 (0.5–2.6) |
| UA (mg/dL) | 4.1 (3.4–5.3) | 5.4 (4.8–6.4) |
| Wavelength (nm) | Associated Functional Groups | Homocit vs. lys | Control (Intensity) | HD (Intensity) | p | In Line | Sign. Influence DM (p) |
|---|---|---|---|---|---|---|---|
| 1390 | C-H bands | increase | −0.012 | −0.011 | <0.0001 | yes | No (0.24) |
| 1468 | CONH2 (N-H combination band) | decrease | −0.0044 | −0.0062 | <0.0001 | yes | No (0.42) |
| 1494 | N-H amide | increase | 0.012 | 0.014 | <0.0001 | yes | No (0.90) |
| 1532 | N-H amide | decrease | 0.0097 | 0.0090 | 0.0001 | yes | Nearly sign. decrease (0.069) |
| 1571 | N-H amide | increase | 0.00034 | −0.000043 | 0.0001 | no | No (0.72) |
| 1610 | C=O/N-H combination | increase | −0.00032 | −0.0011 | <0.0001 | no | No (0.91) |
| 1655 | C-H methyl | increase | −0.024 | −0.026 | 0.0006 | no | Nearly sign. increase (0.073) |
| 1693 | CONH2 (N-H and C=O) | decrease | - | - | n.s. | - | - |
| 1706 | C-H methyl | increase | −0.0016 | −0.00054 | 0.0003 | yes | No (0.80) |
| 1744 | CONH2 (C=O hydrogen bonded to N-H) | decrease | - | - | n.s. | - | - |
| 1955 | CONH2 (N-H combination band) | decrease | 0.0040 | 0.0029 | <0.0001 | yes | No (0.83) |
| 1981 | CONH2 (N-H amide II) | increase | - | - | n.s. | - | - |
| 2012 | CONH2 (N-H/C-N combination band) | - | - | - | n.s. | - | - |
| 2057 | CONH2 (N-H/C=O amide) | increase | - | - | n.s. | - | - |
| 2069 | N-H amide (N-H deformation) | decrease | - | - | n.s. | - | - |
| 2095 | N-H | increase | - | - | n.s. | - | - |
| 2146 | N-H/C-N/C=O | increase | −0.00076 | 0.00022 | <0.0001 | yes | No (0.60) |
| 2203 | CONH2 (N-H and C=O) | decrease | 0.0048 | 0.0039 | =0.010 | yes | No (0.39) |
| 2222 | N-H combination | increase | - | - | n.s. | - | - |
| 2260 | CONH2 (N-H and C=O) | decrease | - | - | n.s. | - | - |
| 2291 | CONH2 (C=O hydrogen bonded to N-H) | increase | - | - | n.s. | - | - |
| Model | r2 (p) | Retained Variables | β (SE) | p |
|---|---|---|---|---|
| Age, DM and urea | 0.24 (<0.001) | Age (yr) | 0.038 (0.0060) | <0.0001 |
| Age, DM and IS total | 0.27 (<0.001) | Age (yr) | 0.028 (0.0067) | 0.0001 |
| IS total (mg/dL) | 0.34 (0.12) | 0.0058 | ||
| Age, DM and PCG total | 0.26 (<0.001) | Age (yr) | 0.029 (0.0072) | 0.0001 |
| PCG total (mg/dL) | 1.29 (0.58) | 0.028 | ||
| Age, DM and PCG free | 0.26 (<0.001) | Age (yr) | 0.029 (0.0071) | 0.0001 |
| PCG free (mg/dL) | 1.41 (0.63) | 0.027 | ||
| Age, DM and HA total | 0.27 (<0.001) | Age (yr) | 0.029 (0.0067) | <0.0001 |
| HA total (mg/dL) | 0.14 (0.050) | 0.0063 | ||
| Age, DM and HA free | 0.26 (<0.001) | Age (yr) | 0.030 (0.21) | <0.0001 |
| HA free (mg/dL) | 0.21 (0.082) | 0.013 |
| Models of Patient Survival (Events n = 31) | HR | 95% CI | p |
|---|---|---|---|
| Unadjusted Model | |||
| Intensity at 1494 nm (milliunits) | 1.81 | 1.26–2.58 | 0.0012 |
| Age-Adjusted Model | |||
| Intensity at 1494 nm (milliunits) | 2.05 | 1.22–3.01 | 0.0001 |
| Age (yr) | 1.07 | 1.03–1.11 | 0.0002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bruyne, S.; Himpe, J.; Delanghe, S.E.; Glorieux, G.; Van Biesen, W.; De Buyzere, M.L.; Speeckaert, M.M.; Delanghe, J.R. Carbamoylated Nail Proteins as Assessed by Near-Infrared Analysis Are Associated with Load of Uremic Toxins and Mortality in Hemodialysis Patients. Toxins 2020, 12, 83. https://doi.org/10.3390/toxins12020083
De Bruyne S, Himpe J, Delanghe SE, Glorieux G, Van Biesen W, De Buyzere ML, Speeckaert MM, Delanghe JR. Carbamoylated Nail Proteins as Assessed by Near-Infrared Analysis Are Associated with Load of Uremic Toxins and Mortality in Hemodialysis Patients. Toxins. 2020; 12(2):83. https://doi.org/10.3390/toxins12020083
Chicago/Turabian StyleDe Bruyne, Sander, Jonas Himpe, Sigurd E. Delanghe, Griet Glorieux, Wim Van Biesen, Marc L. De Buyzere, Marijn M. Speeckaert, and Joris R. Delanghe. 2020. "Carbamoylated Nail Proteins as Assessed by Near-Infrared Analysis Are Associated with Load of Uremic Toxins and Mortality in Hemodialysis Patients" Toxins 12, no. 2: 83. https://doi.org/10.3390/toxins12020083
APA StyleDe Bruyne, S., Himpe, J., Delanghe, S. E., Glorieux, G., Van Biesen, W., De Buyzere, M. L., Speeckaert, M. M., & Delanghe, J. R. (2020). Carbamoylated Nail Proteins as Assessed by Near-Infrared Analysis Are Associated with Load of Uremic Toxins and Mortality in Hemodialysis Patients. Toxins, 12(2), 83. https://doi.org/10.3390/toxins12020083