Changes in Average Sodium Content of Prepacked Foods in Slovenia during 2011–2015






Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Data for 2015
2.2. Use of Data for 2011
2.3. Calculation of Average Sodium Content per (Sub)Category
2.4. Share in Total Sodium Sales (STSS)
2.5. Data Processing and Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- WHO. Salt Reduction Faact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs393/en/ (accessed on 27 June 2017).
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N.; Rodriguez-Fernandez, R.; Legetic, B.; McLaren, L.; Barberio, A.; Webster, J. Salt Reduction Initiatives around the World—A Systematic Review of Progress towards the Global Target. PLoS ONE 2015, 10, e0130247. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Brinsden, H.C.; Macgregor, G.A. Salt reduction in the United Kingdom: A successful experiment in public health. J. Hum. Hypertens. 2013, 28, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Puska, P. Successful prevention of non-communicable diseases: 25 year experiences with North Karelia Project in Finland. Public Health Med. 2002, 4, 5–7. [Google Scholar]
- Espeland, M.A.; Kumanyika, S.; Wilson, A.C.; Reboussin, D.M.; Easter, L.; Self, M.; Robertson, J.; Brown, W.M.; McFarlane, M. Statistical issues in analyzing 24-hour dietary recall and 24-hour urine collection data for sodium and potassium intakes. Am. J. Epidemiol. 2001, 153, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, C.; Maalouf, J.; Yuan, K.M.; Cogswell, M.E.; Gunn, J.P.; Levings, J.; Moshfegh, A.; Ahuja, J.K.C.; Merritt, R. Sodium content in major brands of US packaged foods, 2009. Am. J. Clin. Nutr. 2015, 101, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, J.K.C.; Pehrsson, P.R.; Cogswell, M. A Comparison of Concentrations of Sodium and Related Nutrients (Potassium, Total Dietary Fiber, Total and Saturated Fat, and Total Sugar) in Private-Label and National Brands of Popular, Sodium-Contributing, Commercially Packaged Foods in the United States. J. Acad. Nutr. Diet. 2017, 117, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Trevena, H.; Neal, B.; Dunford, E.; Haskelberg, H.; Wu, J.H.Y. A Comparison of the Sodium Content of Supermarket Private-Label and Branded Foods in Australia. Nutrients 2015, 7, 7027–7041. [Google Scholar] [CrossRef] [PubMed]
- Zganiacz, F.; Wills, R.B.H.; Mukhopadhyay, S.P.; Arcot, J.; Greenfield, H. Changes in the Sodium Content of Australian Processed Foods between 1980 and 2013 Using Analytical Data. Nutrients 2017, 9, 501. [Google Scholar] [CrossRef] [PubMed]
- Monro, D.; Mhurchu, C.N.; Jiang, Y.N.; Gorton, D.; Eyles, H. Changes in the Sodium Content of New Zealand Processed Foods: 2003–2013. Nutrients 2015, 7, 4054–4067. [Google Scholar] [CrossRef] [PubMed]
- Arcand, J.; Jefferson, K.; Schermel, A.; Shah, F.; Trang, S.; Kutlesa, D.; Lou, W.; L’Abbe, M.R. Examination of food industry progress in reducing the sodium content of packaged foods in Canada: 2010 to 2013. Appl. Phys. Nutr. Metab. 2016, 41, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Mhurchu, C.N.; Capelin, C.; Dunford, E.K.; Webster, J.L.; Neal, B.C.; Jebb, S.A. Sodium content of processed foods in the United Kingdom: Analysis of 44,000 foods purchased by 21,000 households. Am. J. Clin. Nutr. 2011, 93, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, J.K.C.; Pehrsson, P.R.; Haytowitz, D.B.; Wasswa-Kintu, S.; Nickle, M.; Showell, B.; Thomas, R.; Roseland, J.; Williams, J.; Khan, M.; et al. Sodium monitoring in commercially processed and restaurant foods. Am. J. Clin. Nutr. 2015, 101, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.L.; Dunford, E.K.; Neal, B.C. A systematic survey of the sodium contents of processed foods. Am. J. Clin. Nutr. 2010, 91, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.B.; Lange, K.; Hogarth, R.; Clifton, P.M. Foods contributing to sodium intake and urinary sodium excretion in a group of Australian women. Public Health Nutr. 2013, 16, 1837–1842. [Google Scholar] [CrossRef] [PubMed]
- Korosec, Z.; Pravst, I. Assessing the average sodium content of prepacked foods with nutrition declarations: The importance of sales data. Nutrients 2014, 6, 3501–3515. [Google Scholar] [CrossRef] [PubMed]
- Ribic, C.H.; Zakotnik, J.M.; Vertnik, L.; Vegnuti, M.; Cappuccio, F.P. Salt intake of the Slovene population assessed by 24 h urinary sodium excretion. Public Health Nutr. 2010, 13, 1803–1809. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Republic of Slovenia. National Action Plan for Reducing the Consumption of Salt in the Diet of the Population of Slovenia for the Period 2010–2020 (In Slovenian: Nacionalni Akcijski Načrt za Zmanjševanje Uživanja Soli v Prehrani Prebivalcev Slovenije za Obdobje 2010–2020). Available online: http://www.mz.gov.si/fileadmin/mz.gov.si/pageuploads/mz_dokumenti/delovna_podrocja/javno_zdravje/petric/Nacio_akcijski_nacrt_za_zmanj_uziv_soli_v_prehrani_preb_Slo_2010-2010.pdf (accessed on 27 June 2017).
- Republic of Slovenia. Resolution on National Programme on Nutrition and Physical Activity 2015–2025 (In Slovenian: Resolucija o Nacionalnem Programu o Prehrani in Telesni Dejavnosti za Zdravje 2015–2025). Available online: http://www.mz.gov.si/fileadmin/mz.gov.si/pageuploads/javna_razprava_2015/Resolucija_o_nac_programu_prehrane_in_in_tel_dejavnosti_jan_2015.pdf (accessed on 27 June 2017).
- Nutrition Institute. Podatkovna Baza CLAS Kot Orodje za Vrednotenje Sprememb na Področju Ponudbe Predpakiranih Živil v Sloveniji. Available online: http://www.nutris.org/clas/ (accessed on 16 August 2017).
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Ni Mhurchu, C.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.K.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Pravst, I.; Kušar, A. Consumers’ exposure to nutrition and health claims on prepacked foods: Use of sales weighting for assessing the food supply in Slovenia. Nutrients 2015, 7, 9353–9368. [Google Scholar] [CrossRef] [PubMed]
- Hlastan Ribič, C.; Zakotnik, J.M.; Seljak, K.B.; Poličnik, R.; Blaznik, U.; Mis, F.N.; Eržen, I.; Ji, C.; Cappucio, F.P. Estimation of sodium availability in food in Slovenia: Results from household food purchase data from 2000 to 2009. Slov. J. Public Health 2014, 53, 209. [Google Scholar]
- Centraal Bureau Levensmiddelenhandel. National Agreement to Improve Product Composition 2014–2020. Available online: http://www.akkoordverbeteringproductsamenstelling.nl/en (accessed on 30 June 2017).
- Sarmugam, R.; Worsley, A. Dietary Behaviours, Impulsivity and Food Involvement: Identification of Three Consumer Segments. Nutrients 2015, 7, 8036–8057. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Survey on Members States’ Implementation of the EU Salt Reduction Framework. Available online: https://ec.europa.eu/health//sites/health/files/nutrition_physical_activity/docs/salt_report1_en.pdf (accessed on 16 August 2017).
- European Commission. EU Platform for Action on Diet, Physical Activity and Health. Available online: https://ec.europa.eu/health/nutrition_physical_activity/platform_en (accessed on 16 August 2017).
- European Commission. High Level Group: Salt Campaign. Available online: http://ec.europa.eu/health/nutrition_physical_activity/high_level_group/nutrition_salt_en.htm (accessed on 29 April 2014).
- Casado, A.; Ramos, P.; Rodriguez, J.; Moreno, N.; Gil, P. Types and Characteristics of Drinking Water for Hydration in the Elderly. Crit. Rev. Food Sci. Nutr. 2015, 55, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Quattrini, S.; Pampaloni, B.; Brandi, M.L. Natural mineral waters: Chemical characteristics and health effects. Clin. Cases Miner. Bone Metab. 2016, 13, 173–180. [Google Scholar] [CrossRef] [PubMed]
- European Comission. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the Provision of Food Information to Consumers. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:02011R1169-20140219 (accessed on 29 March 2017).

{kind=link}
| Year 2015 | Year 2011 6 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Food Category | N | % LSC 1 | Average Sodium Content (mg per 100 g/mL) | SAR: SCS/SCA Ratio 4 | STSS 5 | N | % LSC 1 | Average Sodium Content (mg per 100 g/mL) | SCA Ratio 2015/2011 | SCS Ratio 2015/2011 | ||
| SCA (95% CI) 2 | SCS 3 | SCA (95% CI) 2 | SCS 3 | |||||||||
| Waters | 80 | 71% | 15 (0–42) | 47 | 321% | 9.4% | ||||||
| Bread | 126 | 83% | 546 (512–580) | 505 | 92% | 9.1% | ||||||
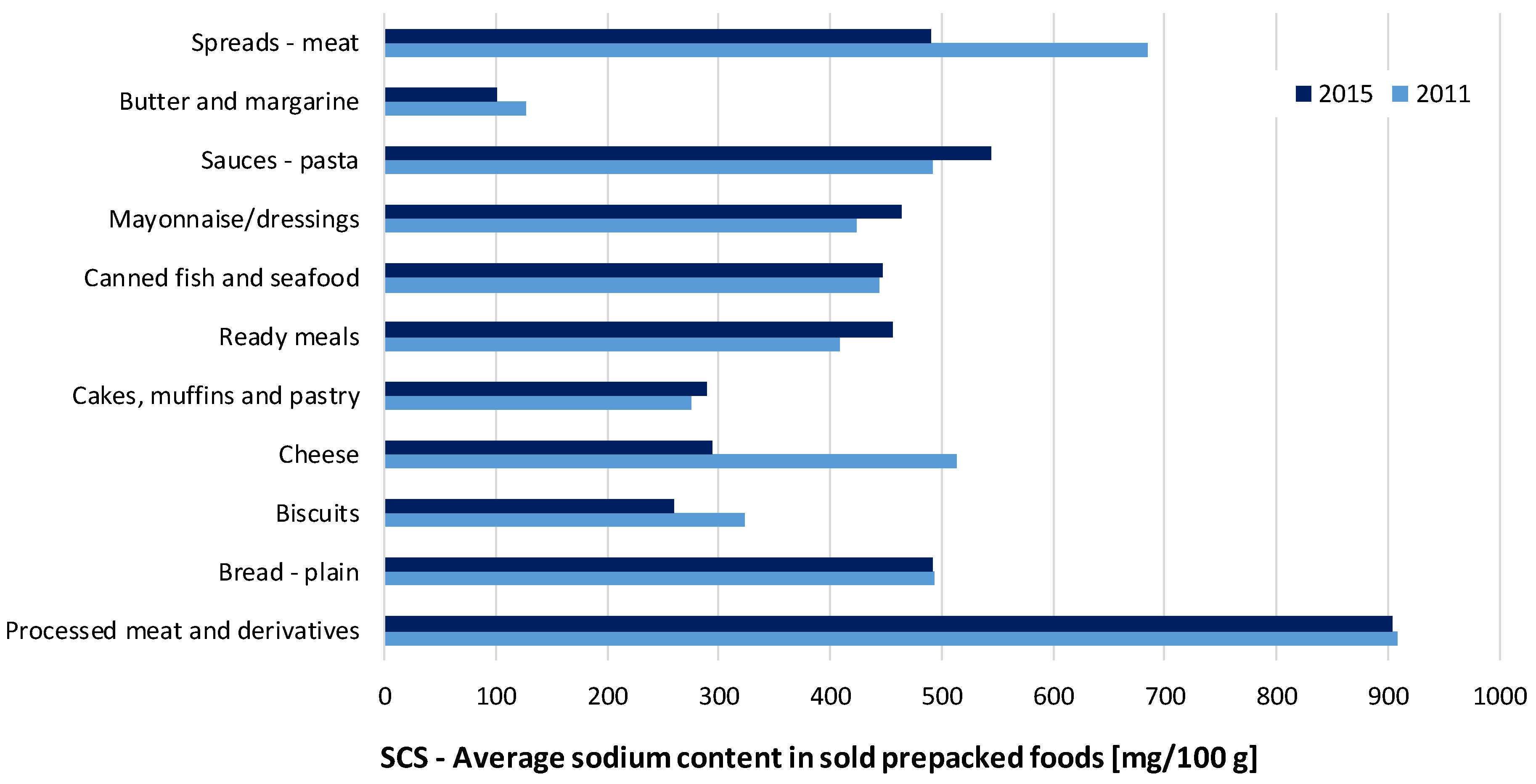
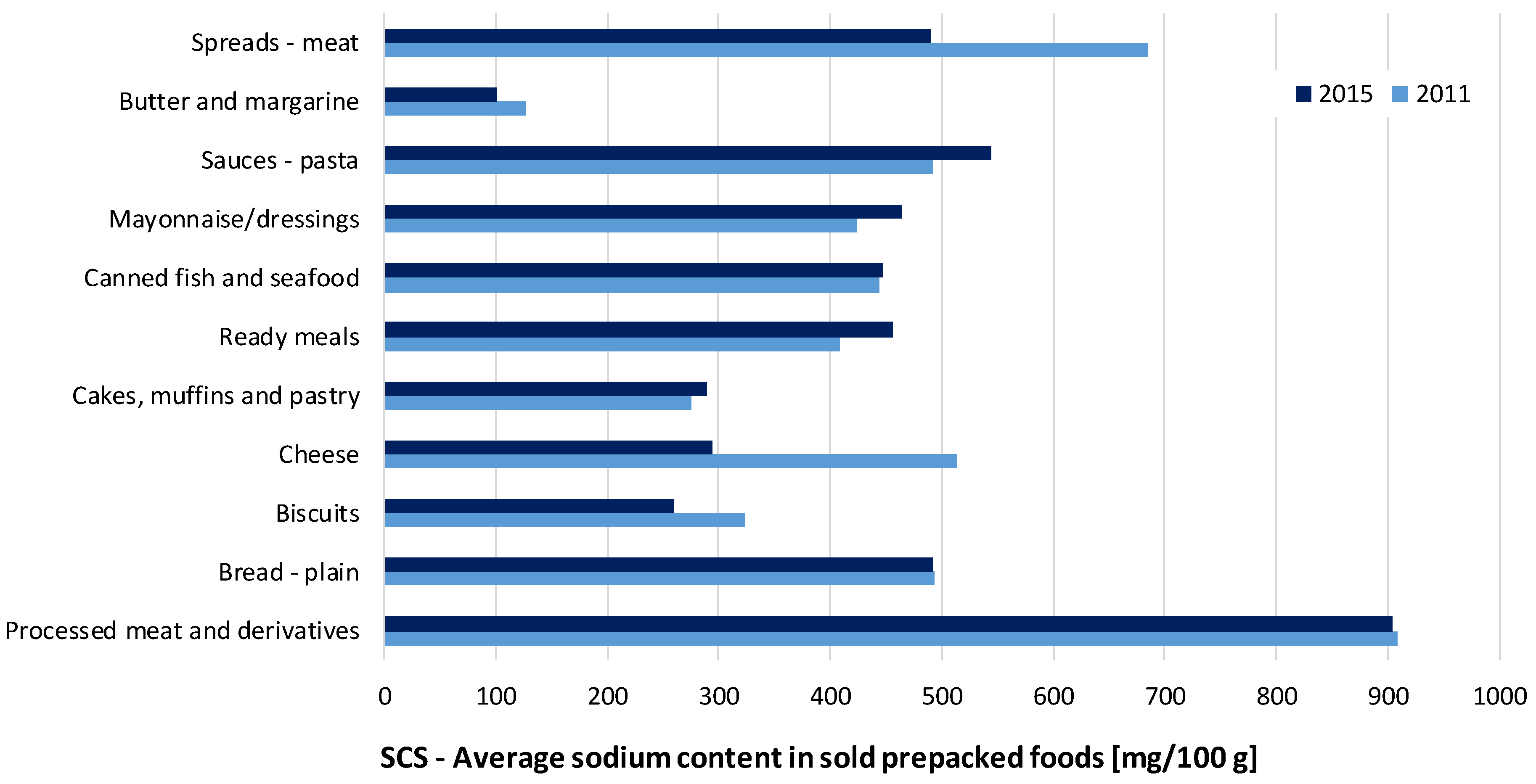
| - plain | 111 | 81% | 530 (499–562) | 492 | 93% | 8.1% | 155 | 30% | 488 (449–527) | 493 | 109% | 100% |
| Biscuits | 655 | 73% | 335 (305–364) | 259 | 78% | 6.6% | 485 | 45% | 353 (312–394) | 324 | 95% | 80% |
| Cakes, muffins and pastry | 285 | 71% | 268 (246–289) | 289 | 108% | 2.5% | 73 | 12% | 226 (169–283) | 275 | 119% | 105% |
| Noodles | 103 | 77% | 103 (61–145) | 27 | 27% | 0.1% | 67 | 31% | 94 (0–195) | 20 | 109% | 136% |
| Breakfast cereals | 212 | 94% | 215 (182–248) | 14 | 7% | 3.8% | ||||||
| Pasta | 296 | 88% | 128 (102–154) | 75 | 58% | 1.3% | ||||||
| - plain | 242 | 88% | 61 (40–81) | 55 | 91% | 0.9% | 281 | 53% | 15 (7–23) | 29 | 398% * | 193% |
| - filled | 54 | 87% | 431 (380–482) | 409 | 95% | 0.4% | ||||||
| Pizza | 21 | 71% | 539 (493–586) | 519 | 96% | 0.2% | 23 | 70% | 932 (649–1215) | 799 | 58% | 65% |
| Soups - concentrated | 150 | 78% | 425 (353–497) | 387 | 91% | 0.8% | ||||||
| Ready meals | 206 | 66% | 510 (469–551) | 457 | 90% | 2.2% | 152 | 34% | 480 (367–579) | 409 | 106% * | 112% |
| Cheese | 292 | 74% | 524 (480–567) | 294 | 56% | 5.1% | 381 | 13% | 626 (429–823) | 513 | 84% | 57% |
| Butter and margarine | 85 | 78% | 144 (101–187) | 101 | 71% | 1.0% | 74 | 62% | 168 (100–236) | 127 | 86% | 80% |
| Canned fish and seafood | 155 | 61% | 659 (478–840) | 447 | 68% | 2.2% | 180 | 12% | 443 (375–511) | 444 | 149% | 101% |
| Vegetables | 453 | 56% | 395 (335–455) | 319 | 81% | 9.4% | ||||||
| - canned | 330 | 60% | 484 (413–555) | 382 | 79% | 9.1% | ||||||
| Processed meat and derivatives | 362 | 47% | 984 (910–1058) | 904 | 92% | 13.1% | 363 | 15% | 1116 (952–1258) | 909 | 88% | 99% |
| Meat alternatives | 53 | 58% | 453 (318–589) | 220 | 48% | 0.1% | ||||||
| Crisps and snacks | 206 | 86% | 787 (742–833) | 804 | 102% | 6.3% | ||||||
| Sauces | 273 | 55% | 1131 (877–1386) | 720 | 64% | 3.0% | ||||||
| - pasta | 108 | 65% | 601 (528–673) | 545 | 91% | 1.1% | 135 | 21% | 386 (288–484) | 492 | 155% * | 111% |
| Mayonnaise/dressings | 48 | 92% | 580 (512–648) | 464 | 80% | 1.3% | 36 | 47% | 576 (481–671) | 424 | 101% | 109% |
| Spreads | 234 | 57% | 425 (359–490) | 192 | 45% | 1.0% | ||||||
| - meat | 131 | 45% | 509 (469–548) | 490 | 96% | 0.6% | 123 | 4% | 626 (573–679) | 686 | 81% | 71% |
| - vegetable | 48 | 71% | 653 (454–853) | 524 | 80% | 0.1% | 39 | 44% | 578 (408–748) | 459 | 113% | 114% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pravst, I.; Lavriša, Ž.; Kušar, A.; Miklavec, K.; Žmitek, K. Changes in Average Sodium Content of Prepacked Foods in Slovenia during 2011–2015. Nutrients 2017, 9, 952. https://doi.org/10.3390/nu9090952
Pravst I, Lavriša Ž, Kušar A, Miklavec K, Žmitek K. Changes in Average Sodium Content of Prepacked Foods in Slovenia during 2011–2015. Nutrients. 2017; 9(9):952. https://doi.org/10.3390/nu9090952
Chicago/Turabian StylePravst, Igor, Živa Lavriša, Anita Kušar, Krista Miklavec, and Katja Žmitek. 2017. "Changes in Average Sodium Content of Prepacked Foods in Slovenia during 2011–2015" Nutrients 9, no. 9: 952. https://doi.org/10.3390/nu9090952