Sodium Reduction in Processed Foods in Brazil: Analysis of Food Categories and Voluntary Targets from 2011 to 2017

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Product Selection Criteria
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Proportion of Products Meeting the PAHO Regional Targets
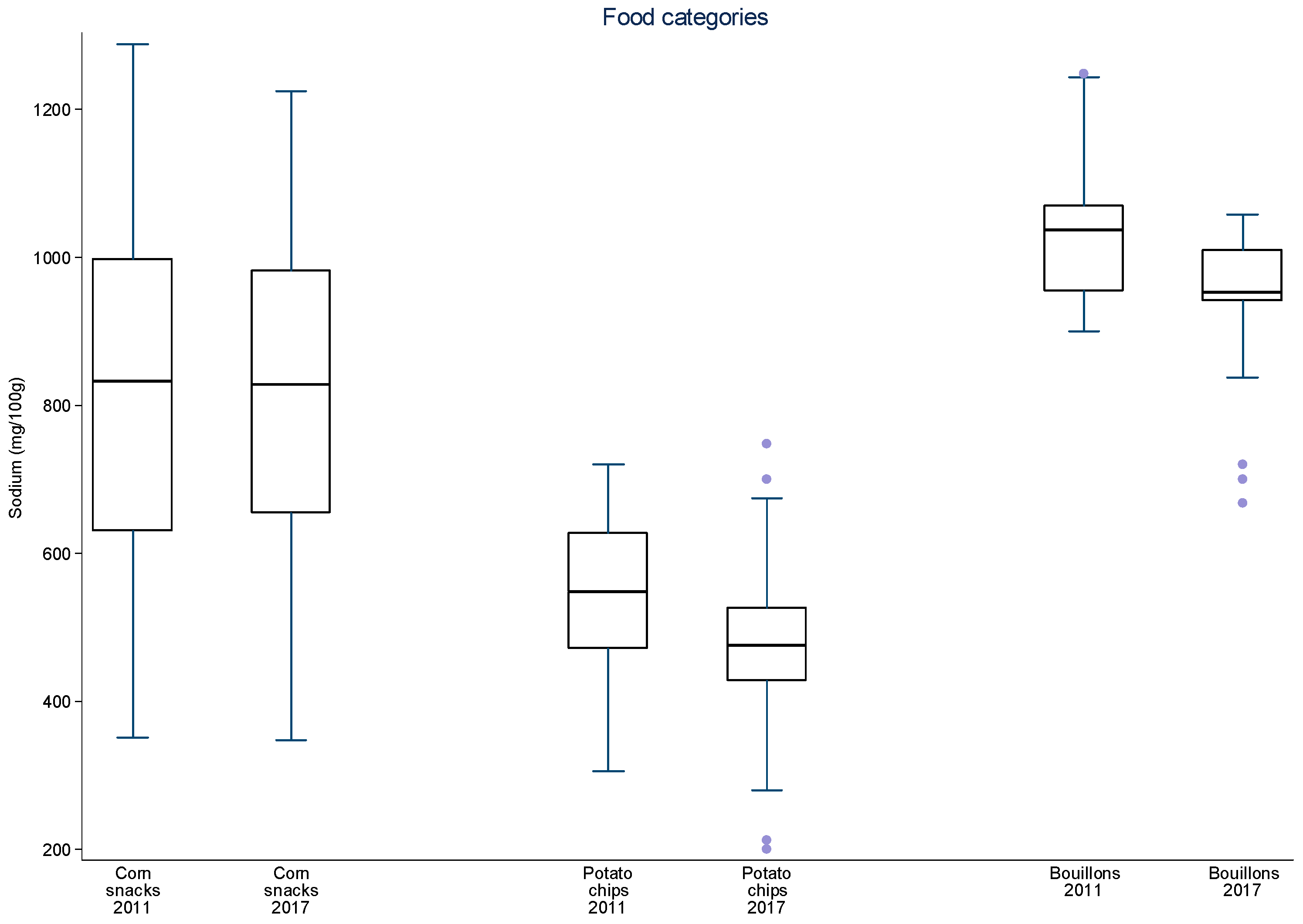
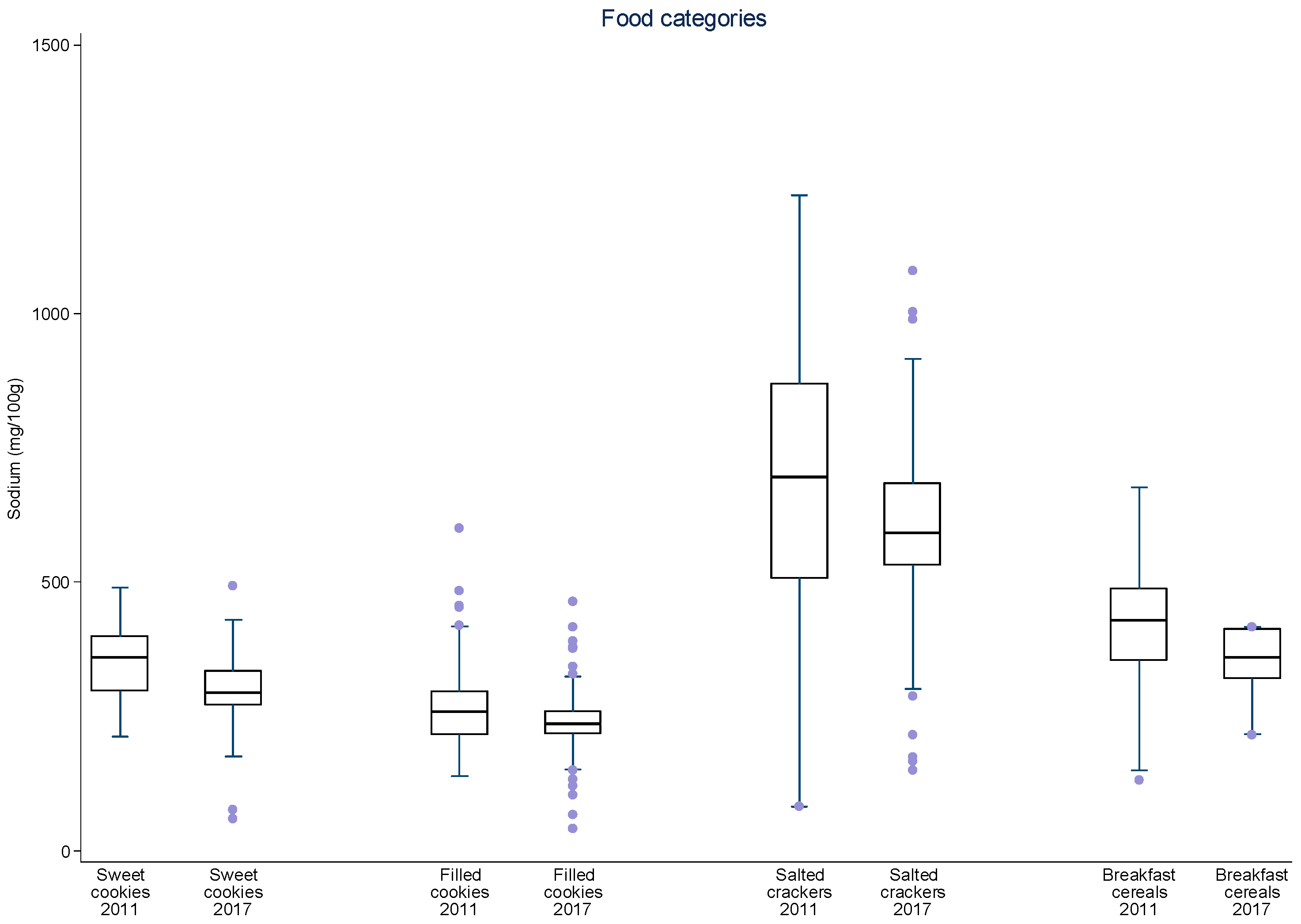
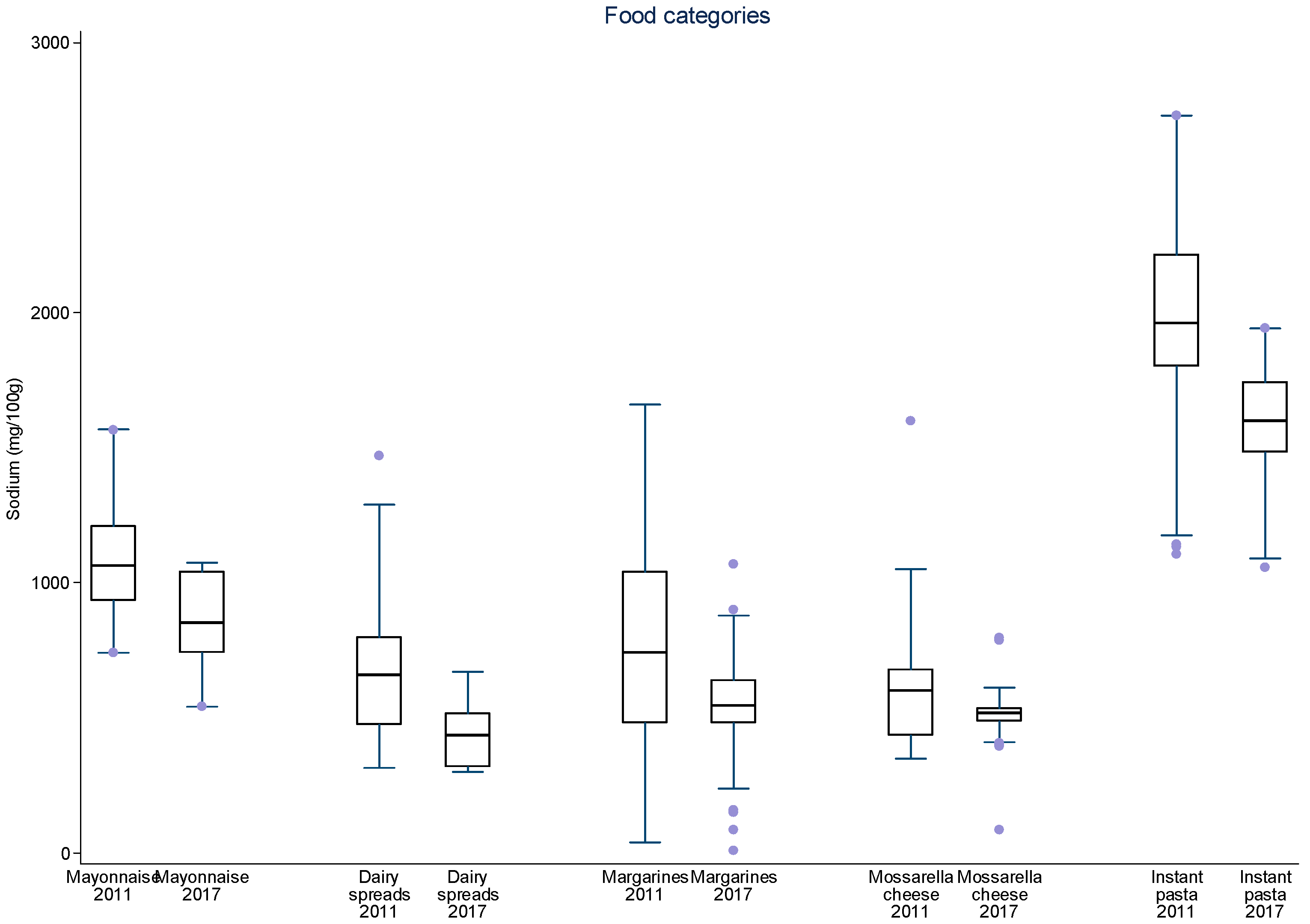
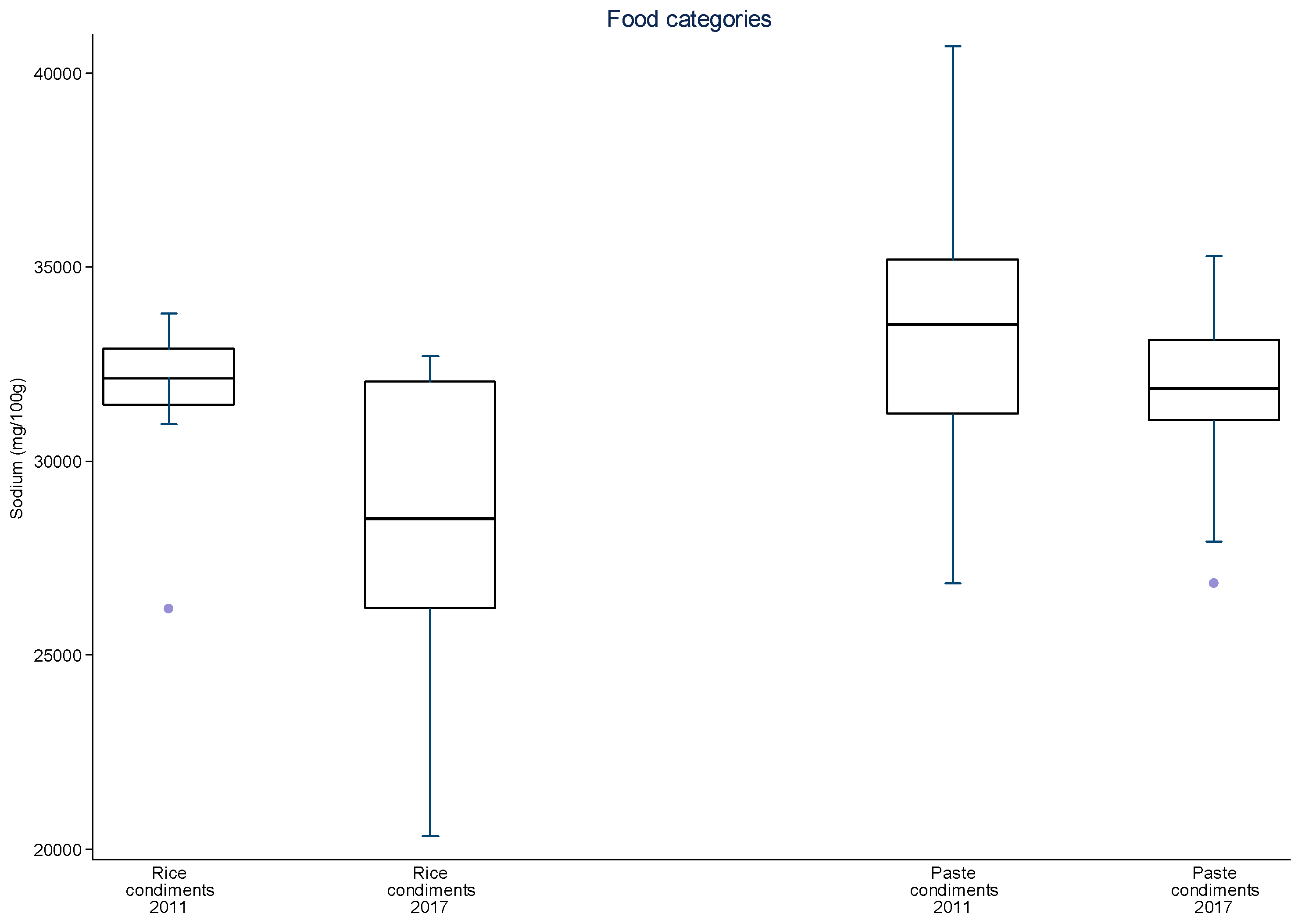
3.2. Analysis of Mean and Median Sodium Content for Each Food Category over Time
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt Intakes around the World: Implications for Public Health. Int. J. Epidemiol. 2009, 38, 791–813. Available online: https://academic.oup.com/ije/article-lookup/doi/10.1093/ije/dyp139 (accessed on 30 June 2017). [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; WHO: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854eng.pdf?ua=1 (accessed on 30 June 2017).
- Pan American Health Organization. Salt Smart Americas: A Guide for Country—Level Action; PAHO: Washington, DC, USA, 2013; Available online: http://www.paho.org/hq/index.php?option=com_docman&task=docdownload&gid=21554&Itemid=270&lang=en (accessed on 30 June 2017).
- World Health Organization. Scaling Up Action against Noncommunicable Diseases: How Much Will It Cost? WHO: Geneva, Switzerland, 2011; Available online: http://whqlibdoc.who.int/publications/2011/9789241502313eng.pdf?ua=1 (accessed on 30 June 2017).
- Webb, M.; Fahimi, S.; Saman, S.; Gitanjali, M.; Khatibzadeh, S.; Micha, R.; Powles, J. Cost Effectiveness of Government Supported Policy Strategy to Decrease Sodium Intake: Global Analysis across 183 Nations. BMJ 2017, 356. Available online: http://www.bmj.com/content/356/bmj.i6699.full.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Ribeiro, L.; Duncan, B.; Brant, L.; Lotufo, P.; Mill, G.; Barreto, S. Cardiovascular Health in Brazil—Trends and Perspectives. Circulation 2016, 133, 422–433. Available online: http://circ.ahajournals.org/content/133/4/422 (accessed on 30 June 2017).
- Ministério da Saúde. Saúde Brasil 2014. 2015. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2014_analise_situacao.pdf (accessed on 30 June 2017).
- Vigitel Brazil 2016: Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey: Estimates of Sociodemographic Frequency and Distribution of Risk and Protective Factors for Chronic Diseases in the Capitals of the 26 Brazilian States and the Federal District in 2016. 2017. Available online: http://portalsaude.saude.gov.br/images/pdf/2017/junho/07/vigitel_2016_jun17.pdf (accessed on 30 June 2017).
- Ministério da Saúde. Plano de Ações Estratégicas Para o Enfrentamento Das Doenças Crônicas Não Transmissíveis (DCNT) no Brasil. 2011–2022. 2011. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf (accessed on 30 June 2017).
- Louzada, M.L.C.; Martins, A.P.B.; Canella, D.S.; Baraldi, L.G.; Levy, R.B.; Claro, R.M.; Moubarac, J.C.; Cannon, G.; Monteiro, C.A. Alimentos Ultraprocessados e Perfil Nutricional da Dieta no Brasil. Rev. Saúde Pública 2015, 49. Available online: http://www.scielo.br/pdf/rsp/v49/0034-8910-rsp-S0034-89102015049006132.pdf (accessed on 30 June 2017).
- Sarno, F.; Claro, R.M.; Levy, R.B.; Bandoni, D.H.; Monteiro, C.A. Estimated Sodium Intake for the Brazilian Population, 2008–2009. Rev. Saude Publica 2013, 47, 571–578. Available online: http://www.scielo.br/pdf/rsp/v47n3/en_0034-8910-rsp-47-03-0571.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Martins, C.; De Sousa, A.; Veiros, M.; González-Chica, D.; Proença, R. Sodium Content and Labelling of Processed and Ultra-Processed Food Products Marketed in Brazil. Public Health Nutr. 2015, 18, 1206–1214. Available online: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/5B78C17E59B2227DE7870981139A15DC/S1368980014001736a.pdf/sodium_content_and_labelling_of_processed_and_ultraprocessed_food_products_marketed_in_brazil.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Rodrigues, V.M.; Rayner, M.; Fernandes, A.C.; de Oliveira, R.C.; Proença, R.P.C.; Fiates, G.M.R. Comparison of the Nutritional Content of Products, with and without Nutrient Claims, Targeted at Children in Brazil. Br. J. Nutr. 2016, 115, 2047–2056. Available online: http://nuppre.ufsc.br/files/2014/04/2016-Rodrigues-et-al.-Comparison-of-the-nutritional-content-of-products-with-and-without-nutrient-claims.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatistica. Pesquisa de Orçamentos Familiares 2008–2009—Análise do Consumo Alimentar Pessoal. 2011. Available online: http://biblioteca.ibge.gov.br/visualizacao/livros/liv50063.pdf (accessed on 30 June 2017).
- Oliveira, M.M.; Malta, D.C.; Santos, M.A.S.; Oliveira, T.P.; Nilson, E.A.F.; Claro, R.M. Self-Reported High Salt Intake in Adults: Data from the National Health Survey, Brazil, 2013. Epidemiol. Serv. Saúde 2015, 24, 249–256. Available online: http://www.scielo.br/pdf/ress/v24n2/en_2237-9622-ress-24-02-00249.pdf (accessed on 30 June 2017).
- Hyseni, L.; Elliot-Green, A.; Lloyd-Williams, F.; Kypridemos, C.; O’Flaherty, M.; McGill, R.; Orton, L.; Bromley, H.; Cappuccio, F.P. Systematic Review of Dietary Salt Reduction Policies: Evidence for An Effectiveness Hierarchy? PLoS ONE 2017, 12. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5436672/pdf/pone.0177535.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Hope, S.F.; Webster, J.; Trieu, K.; Pillay, A.; Ieremia, M.; Bell, C.; Moodie, M. A systematic review of economic evaluations of population-based sodium reduction interventions. PLoS ONE 2017, 12. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5371286/pdf/pone.0173600.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Webster, J.; Trieu, K.; Dunford, E.; Hawkes, C. Target Salt 2025: A Global Overview of National Programs to Encourage the Food Industry to Reduce Salt in Foods. Nutrients 2014, 6, 3274–3287. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4145308/pdf/nutrients-06-03274.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Campbell, N.; Legowski, B.; Legetic, B.; Ferrante, D.; Nilson, E.; Campbell, C.; L’Abbé, M. Targets and Timelines for Reducing Salt in Processed Food in the Americas. J. Clin. Hypertens. 2014, 16, 619–623. Available online: http://onlinelibrary.wiley.com/doi/10.1111/jch.12379/full (accessed on 30 June 2017). [CrossRef] [PubMed]
- Wyness, L.A.; Butriss, J.L.; Stanner, S.A. Reducing the Population’s Sodium Intake: The UK Food Standards Agency’s Salt Reduction Programme. Public Health Nutr. 2011, 15, 254–261. Available online: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/9289C9978849B50578E974F1F6BEA01E/S1368980011000966a.pdf/reducing-the-population-s-sodium-intake-the-uk-food-standards-agency-s-salt-reduction-programme.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Trevena, H.; Neal, B.; Dunford, E.; Wu, J.H. An Evaluation of the Effects of the Australian Food and Health Dialogue Targets on the Sodium Content of Bread, Breakfast Cereals and Processed Meats. Nutrients 2014, 6, 3802–3817. Available online: https://www.mdpi.com/resolver?pii=nu6093802 (accessed on 30 June 2017). [CrossRef] [PubMed]
- Zganiacz, F.; Wills, R.B.H.; Mukhopadhyay, S.P.; Arcot, J.; Greenfield, H. Changes in the Sodium Content of Australian Processed Foods between 1980 and 2013 Using Analytical Data. Nutrients 2017, 9. Available online: https://www.mdpi.com/resolver?pii=nu9050501 (accessed on 30 June 2017). [CrossRef] [PubMed]
- Allemandi, L.; Tiscornia, M.V.; Ponce, M.; Castrouovo, L.; Dunford, E. Sodium content in processed foods in Argentina: Compliance with the national law. Cardiovasc. Diagn. Ther. 2015, 5, 197–206. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4451319/pdf/cdt-05-03-197.pdf (accessed on 30 June 2017). [PubMed]
- Peters, S.; Dunford, E.; Ware, L.; Harris, T.; Walker, A.; Wicks, M.; Van Zyl, T.; Swanepoel, B.; Charlton, K.; Woodward, M.; et al. The Sodium Content of Processed Foods in South Africa during the Introduction of Mandatory Sodium Limits. Nutrients 2017, 9. Available online: https://www.mdpi.com/2072-6643/9/4/404/pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Nilson, E.A.F. The Strides to Reduce Salt Intake in Brazil: Have We Done Enough? Cardiovasc. Diagn. Ther. 2015, 5, 243–247. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4451315/pdf/cdt-05-03-243.pdf (accessed on 30 June 2017). [PubMed]
- Brasil. Dietary Guidelines for the Brazilian Population. 2014. Available online: http://189.28.128.100/dab/docs/portaldab/publicacoes/guia_alimentar_populacao_ingles.pdf (accessed on 30 June 2017).
- Nilson, E.A.F.; Jaime, P.C.; Resende, D.O. Iniciativas Desenvolvidas no Brasil Para a Redução do Teor de Sódio em Alimentos Processados. Rev. Panam. Salud Pública 2012, 32, 287–292. Available online: http://www.scielosp.org/pdf/rpsp/v32n4/en_07.pdf (accessed on 30 June 2017). [CrossRef] [PubMed][Green Version]
- Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008–2009—Aquisição Domiciliar Per Capita. Brasil, 2010. Available online: http://biblioteca.ibge.gov.br/visualizacao/livros/liv47307.pdf (accessed on 30 June 2017).
- Campbell, N.; Legowski, B.; Legetic, B.; Nilson, E.; L’Abbé, M. Inaugural Maximum Values for Sodium in Processed Food Products in the Americas. J. Clin. Hypertens. 2015, 17, 611–613. Available online: http://onlinelibrary.wiley.com/doi/10.1111/jch.12553/full (accessed on 30 June 2017). [CrossRef] [PubMed]
- Brasil. Ministério da Saúde. Termo de Compromisso com a Finalidade de Estabelecer Metas Nacionais Para a Redução do Teor de Sódio em Alimentos Processados no Brasil. Brasília, 2011. Available online: http://189.28.128.100/dab/docs/portaldab/documentos/termo_abia_abip_abima_abitrigo_2011.pdf (accessed on 30 June 2017).
- Brasil. Ministério da Saúde. Termo de Compromisso com a Finalidade de Estabelecer Metas Nacionais Para a Redução do Teor de Sódio em Alimentos Processados no Brasil. Brasília, 2011. Available online: http://189.28.128.100/dab/docs/portaldab/documentos/termo_5_dez_2011.pdf (accessed on 30 June 2017).
- Brasil. Ministério da Saúde. Termo de Compromisso com a Finalidade de Estabelecer Metas Nacionais Para a Redução do Teor de Sódio em Alimentos Processados no Brasil. Brasília, 2012. Available online: http://189.28.128.100/dab/docs/portaldab/documentos/termo_6_ago_2012.pdf (accessed on 30 June 2017).
- Brasil. Ministério da Saúde. Termo de Compromisso com a Finalidade de Estabelecer Metas Nacionais Para a Redução do Teor de Sódio em Alimentos Processados no Brasil. Brasília, 2013. Available online: http://189.28.128.100/dab/docs/portaldab/documentos/termo_nov_2013.pdf (accessed on 30 June 2017).
- De Moura Souza, A.; Nalin de Souza, B.; Bezerra, I.N.; Sichieri, R. The Impact of the Reduction of Sodium Content in Processed Foods in Salt Intake in Brazil. Cad. Saúde Pública 2016, 32, 1–7. Available online: http://www.scielo.br/pdf/csp/v32n2/en_0102-311x-csp-0102-311x00064615.pdf (accessed on 30 June 2017).
- Nilson, E.A.F.; Spaniol, A.M.; Gonçalves, V.S.S. A Redução do Consumo de Sódio no Brasil. Cad Saúde Pública 2016, 32. Available online: http://www.scielosp.org/pdf/csp/v32n11/1678-4464-csp-32-11-e00102016.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Combet, E.; Vlassopoulos, A.; Mölenberg, F.; Gressier, M.; Privet, L.; Wratten, C.; Sharif, S.; Vieux, F.; Lehmann, U.; Masset, G. Testing the Capacity of a Multi-Nutrient Profiling System to Guide Food and Beverage Reformulation: Results from Five National Food Composition Databases. Nutrients 2017, 9. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5409745/pdf/nutrients-09-00406.pdf (accessed on 30 June 2017). [CrossRef] [PubMed]
- Konfino, J.; Mekonnen, T.A.; Coxson, P.G.; Ferrante, D.; Bibbins-Domingo. Projected Impact of a Sodium Consumption Reduction Initiative in Argentina: An Analysis from the CVD Policy Model—Argentina. PLoS ONE 2013, 8. Available online: http://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0073824&type=printable (accessed on 30 June 2017). [CrossRef] [PubMed]
- Collins, M.; Mason, H.; O’Flaherty, M.; Guzman-Castillo, M.; Critchley, J.; Capewell, S. An Economic Evaluation of Salt Reduction Policies to Reduce Coronary Disease in England: A Policy Modeling Study. Value Health 2014, 17, 517–524. Available online: http://www.valueinhealthjournal.com/article/S1098-301501828-2/pdf (accessed on 30 June 2017). [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Categories and Subcategories | Regional Target | % Products That Have Met the Regional Targets (2017) | Lower Target | % Products That Have Met the Lower Regional Targets (2017) | |
|---|---|---|---|---|---|
| Americas | Brazil | mg/100 g | % | mg/100 g | % |
| Breads | Sliced bread (n = 82) | 600 | 100.0 | 400 | 59.8 |
| Buns (n = 11) | 100.0 | 81.8 | |||
| Cakes | Aerated cake mixes (n = 135) | 400 | 90.4 | 205 | 25.9 |
| Creamy cake mixes (n = 24) | 91.7 | 45.8 | |||
| Cakes without filling (n = 68) | 100.0 | 36.8 | |||
| Cakes with filling (n = 48) | 100.0 | 54.2 | |||
| Shelf-stable pasta and noodles (dry, uncooked) | Instant pasta (n = 87) | 1921 | 98.9 | 1333 | 10.3 |
| Snacks | Corn snacks (n = 39) | 900 | 53.8 | 530 | 10.2 |
| Potato chips (n = 29) | 100.0 | 75.9 | |||
| Mayonnaise | Mayonnaise (n = 28) | 1050 | 85.7 | 670 | 17.9 |
| Butter/dairy spread | Dairy spread (n = 45) | 800 | 100.0 | 500 | 73.3 |
| Margarines (n = 46) | 95.7 | 28.3 | |||
| Cheese * | Mozzarella cheese (n = 28) | 559 | 89.3 | 512 b | 50.0 |
| Condiments | Rice condiments (n = 5) | 33,100 | 100.0 | 9100 | 0.0 |
| Bouillon cubes and powders (n = 35) ** | 1025 | 97.1 | 900 | 11.4 | |
| Paste condiments * (n = 14) | 37,901 | 100.0 | 33,134 | 78.6 | |
| Cookies and sweet biscuits | Sweet biscuits (n = 52) | 485 | 99.8 | 265 | 21.2 |
| Filled cookies (n = 185) | 100.0 | 86.5 | |||
| Savory biscuits and crackers | Salted crackers (n = 84) | 1340 | 100.0 | 700 | 91.7 |
| Breakfast cereals | Breakfast cereals (n = 15) | 630 | 100.0 | 500 | 100.0 |
| Food Categories | n | Sodium 2011 (mg/100 g) | n | Sodium 2013–2014 (mg/100 g) | n | Sodium 2017 (mg/100 g) | p * | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Min–Max) | Mean ± SD | Median (Min–Max) | Mean ± SD | Median (Min–Max) | |||||
| Sliced bread | 117 | 426.5 ± 107.1 a,b | 432.0 (118.0−796.0) | 87 | 380.3 ± 122.1 a | 380.0 (126.0−870.0) | 82 | 365.0±87.6 b | 380.0 (134.0−536.0) | <0.001 |
| Buns | 9 | 436.1 ± 121.4 | 462.0 (260.0−570.0) | 8 | 388.5 ± 74.4 | 415.0 (270.0−462.0) | 11 | 374.4 ± 59.4 | 372.0 (270.0−512.0) | 0.359 |
| Aerated cake mixes | 125 | 372.3 ± 173.4 a,b | 314.0 (166.7−1111.5) | 201 | 309.6 ± 69.2 a,c | 327.0 (117.0−474.0) | 135 | 291.6 ± 92.6 b,c | 293 (119.6−724.3) | <0.001 |
| Creamy cake mixes | 24 | 270.7 ± 75.6 a | 280.0 (135.1−412.0) | 33 | 250.5 ± 44.6 | 251.0 (69.0−333.0) | 24 | 229.6 ± 82.1 a | 226.2 (40.7−422.9) | 0.047 |
| Cakes without filling | 64 | 335.7 ± 66.7 a,b | 355.0 (188.3−462.9) | 69 | 281.0 ± 85.9 a,c | 300.0 (117.0−398.3) | 68 | 241.1 ± 74.9 b,c | 250.0 (101.7−355.0) | <0.001 |
| Cakes with filling | 41 | 249.9 ± 51.4 a,b | 240.0 (107.0−330.0) | 68 | 212.3 ± 47.0 a,c | 224.0 (108.3−330.0) | 48 | 185.8 ± 55.0 b,c | 200.0 (80.0−255.0) | <0.001 |
| Instant pastas | 90 | 1960.0 ± 384.5 a,b | 1993.5 (1104.9−2729.1) | 97 | 1662.3 ± 265.7 a | 1670.0 (1057.5−2548.6) | 87 | 1598.6 ± 189.6 b | 1607.1 (1057.5−2548.6) | <0.001 |
| Corn snacks | 25 | 831.9 ± 226.1 | 840.0 (351.0−1288.0) | 39 | 753.9 ± 140.1 | 756.0 (352.0−1032.0) | 40 | 827.4 ± 242.8 | 884.0 (348.0−1224.0) | 0.067 |
| Potato chips | 22 | 547.6 ± 123.6 | 598.0 (305.0−720.0) | 28 | 513.3 ± 130.7 | 516.0 (276.0−700.0) | 30 | 475.4 ± 137.9 | 507.3 (200.0−748.0) | 0.237 |
| Mayonnaise | 31 | 1063.3 ± 198.2 a,b | 1058.3 (741.7−1566.7) | 41 | 891.3 ± 157.9 a | 925.0 (400.0−1075.0) | 29 | 852.7 ± 194.9 b | 933.3 (541.7−1075.0) | <0.001 |
| Dairy spreads | 80 | 659.5 ± 248.4 a,b | 596.7 (314.0−1470.0) | 80 | 524.4 ± 188.2 a,c | 468.3 (300.0−1100.0) | 45 | 434.5 ± 110.3 b,c | 410.0 (300.0−670.0) | <0.001 |
| Margarines | 94 | 739.9 ± 363.6 a | 730.0 (40.0−1660.0) | 84 | 689.8 ± 351.4 b | 710.0 (0.0−1660.0) | 46 | 544.3 ± 207.3 a,b | 600.0 (10.0−1070.0) | <0.001 |
| Mozzarella cheese | 26 | 600.2 ± 363.6 a | 540.0 (350.0−160.0) | 51 | 461.2 ± 132.2 a | 486.7 (87.0−786.7) | 28 | 517.2 ± 131.5 | 526.7 (86.7−796.7.0) | 0.039 |
| Rice condiments | 5 | 31,425.1 ± 3009.7 | 32,120.0 (26.186.0−33,800.0) | 4 | 29,530.0 ± 6140.7 | 32,370.0 (20,340.0−33,040.0) | 5 | 28,505.1 ± 5237.6 | 31,260.0 (20,340.0−32,700.0) | 0.325 |
| Bouillon cubes and powders | 41 | 1035.9 ± 94.4 a | 1015.0 (900.0−1247.0) | 26 | 985.2 ± 105.8 b | 1019.0 (705.0−1183.0) | 35 | 952.1 ± 88.2 a,b | 967.0 (668.0−1057.0) | 0.003 |
| Paste condiments | 14 | 33,494.5 ± 4054.4 | 33,450.0 (26,840.0−40,700.0) | 14 | 32,900.0 ± 3173.6 | 33,850.0 (26,840.0−37,280.0) | 14 | 31,845.7 ± 2615.9 | 32,220.0 (26,840.0−35,280.0) | 0.303 |
| Sweet biscuits | 17 | 359.2 ± 81.3 a,b | 386.7 (213.3−490.0) | 45 | 318.2 ± 50.3 a | 317.0 (236.7−416.0) | 52 | 293.9 ± 72.4 b | 306.7 (60.0−493.3) | 0.019 |
| Filled cookies | 176 | 259.5 ± 66.0 a,b | 251.7 (140.0−600.0) | 198 | 242.6 ± 48.9 a | 243.0 (127.0−390.0) | 185 | 235.5 ± 57.3 b | 240.0 (41.7−463.3) | 0.006 |
| Salted crackers | 39 | 695.8 ± 260.8 b | 686.7 (83.3−1220.0) | 94 | 660.4 ± 147.1 c | 633.0 (350.0−923.0) | 84 | 590.9 ± 163.4 b,c | 626.7 (150.0−1080.0) | 0.031 |
| Breakfast cereals | 27 | 428.9 ± 141.8 | 430.0 (132.0−676.7) | 21 | 406.7 ± 129.9 | 392.5 (195.0−679.3) | 15 | 359.2 ± 69.5 | 390.0 (216.7−416.7) | 0.209 |
| Food Categories | % Reduction in Mean Sodium | ||
|---|---|---|---|
| 2011−2013/14 | 2013/14−2017 | 2011−2017 | |
| Loaf bread | 10.8 * | 3.9 | 14.3 * |
| Buns | 11.0 | 3.6 | 14.2 |
| Aerated cake mixes | 16.9 * | 5.8 * | 21.8 * |
| Creamy cake mixes | 7.4 | 8.4 | 15.2 * |
| Cakes without filling | 16.1 * | 14.2 * | 28.0 * |
| Cakes with filling | 14.8 * | 12.7 * | 25.7 * |
| Instant pastas | 15.2 * | 3.8 | 18.5 * |
| Corn snacks | 9.4 | −9.8 | 0.5 |
| Potato chips | 6.2 | 7.4 | 13.2 |
| Mayonnaise | 16.2 * | 4.4 | 19.8 * |
| Dairy spreads | 20.5 * | 17.1 * | 34.1 * |
| Margarines | 6.8 | 21.0 * | 26.4 * |
| Mozzarella cheese | 23.2 * | −12.1 | 13.8 |
| Rice condiments | 6.0 | 3.5 | 9.3 |
| Bouillon cubes and powders | 4.8 | 3.3 * | 8.0 * |
| Paste condiments | 1.8 | 3.2 | 4.9 |
| Sweet biscuits | 11.4 * | 7.9 | 18.4 * |
| Filled cookies | 6.6 * | 2.9 | 9.3 * |
| Salted crackers | 5.0 | 10.4 * | 15.0 * |
| Breakfast cereals | 5.4 | 11.6 | 16.3 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilson, E.A.F.; Spaniol, A.M.; Gonçalves, V.S.S.; Moura, I.; Silva, S.A.; L’Abbé, M.; Jaime, P.C. Sodium Reduction in Processed Foods in Brazil: Analysis of Food Categories and Voluntary Targets from 2011 to 2017. Nutrients 2017, 9, 742. https://doi.org/10.3390/nu9070742
Nilson EAF, Spaniol AM, Gonçalves VSS, Moura I, Silva SA, L’Abbé M, Jaime PC. Sodium Reduction in Processed Foods in Brazil: Analysis of Food Categories and Voluntary Targets from 2011 to 2017. Nutrients. 2017; 9(7):742. https://doi.org/10.3390/nu9070742
Chicago/Turabian StyleNilson, Eduardo A. F., Ana M. Spaniol, Vivian S. S. Gonçalves, Iracema Moura, Sara A. Silva, Mary L’Abbé, and Patricia C. Jaime. 2017. "Sodium Reduction in Processed Foods in Brazil: Analysis of Food Categories and Voluntary Targets from 2011 to 2017" Nutrients 9, no. 7: 742. https://doi.org/10.3390/nu9070742
APA StyleNilson, E. A. F., Spaniol, A. M., Gonçalves, V. S. S., Moura, I., Silva, S. A., L’Abbé, M., & Jaime, P. C. (2017). Sodium Reduction in Processed Foods in Brazil: Analysis of Food Categories and Voluntary Targets from 2011 to 2017. Nutrients, 9(7), 742. https://doi.org/10.3390/nu9070742