Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients

 ,
, 

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Renal Transplant Characteristics
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association of Plasma Vitamin C Concentration with Clinical Variables
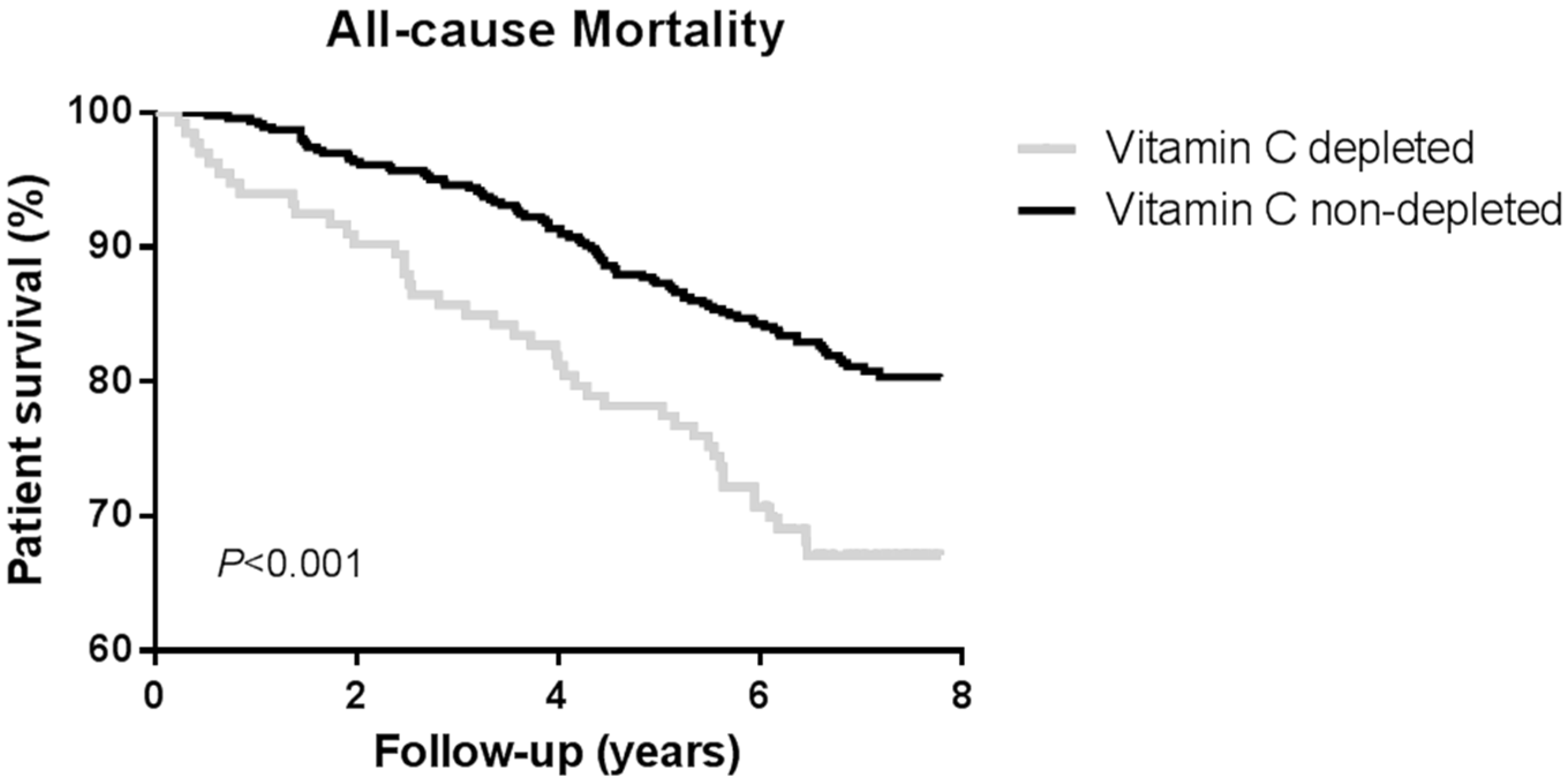
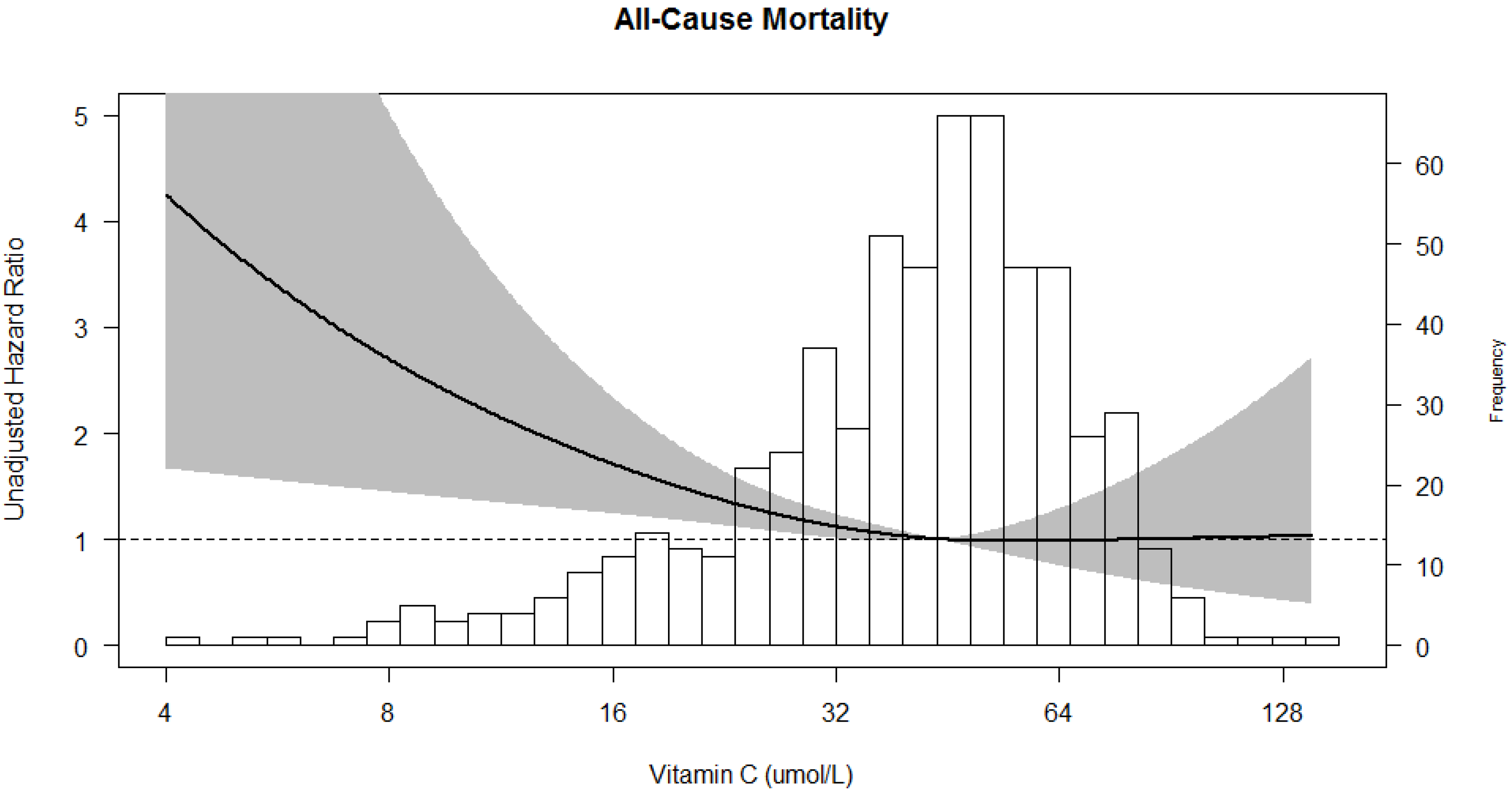
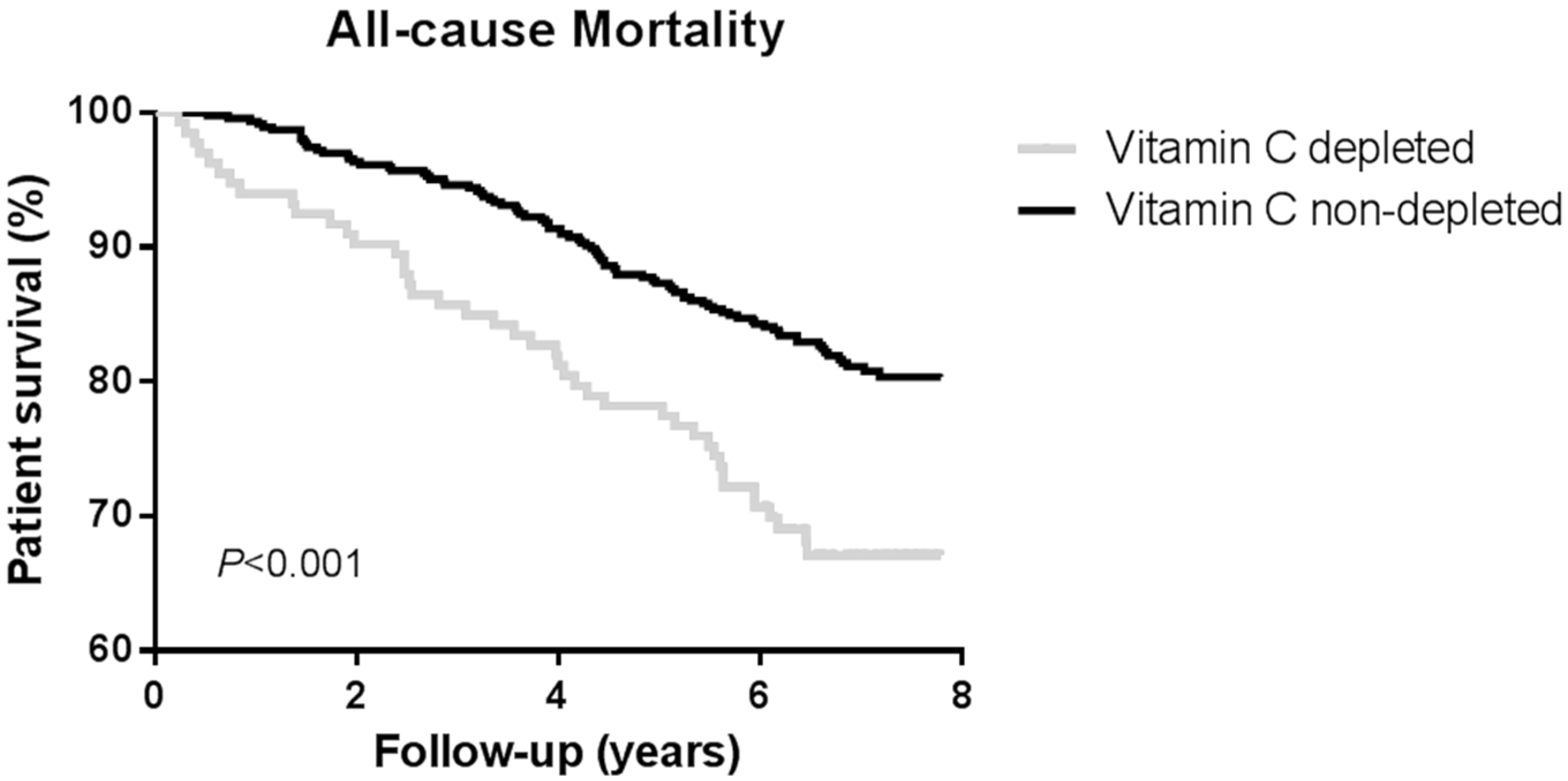
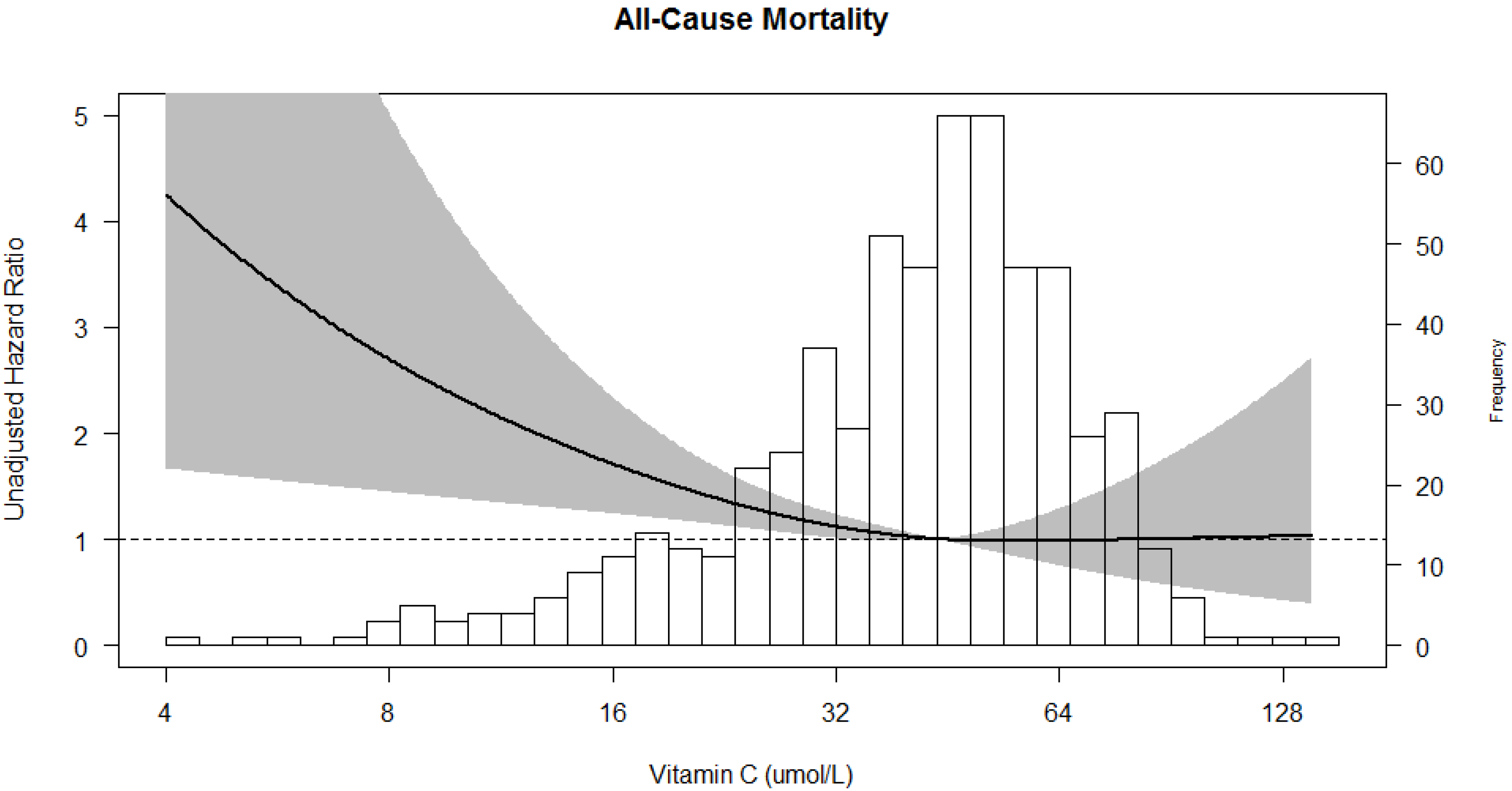
3.3. Prospective Analyses
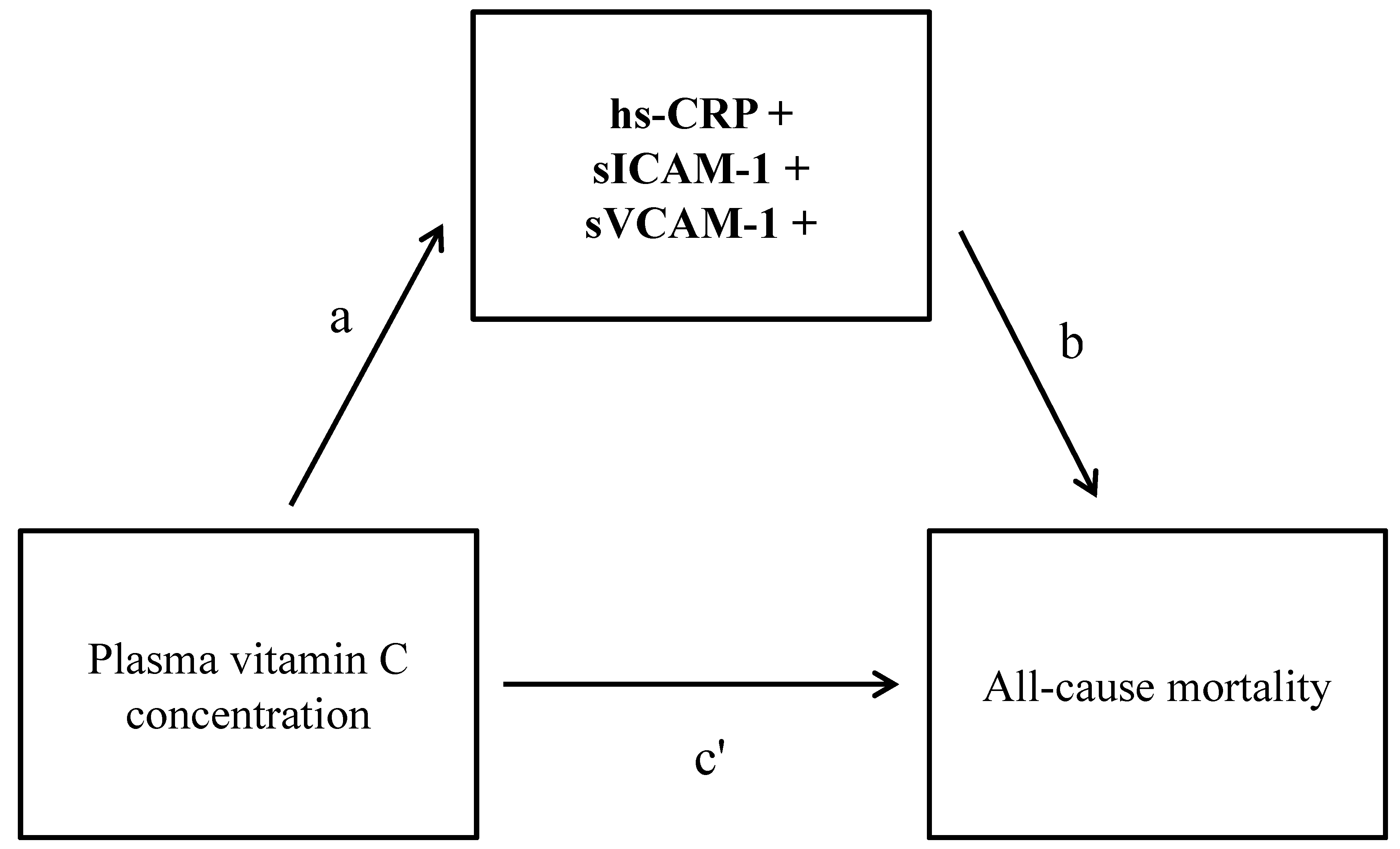
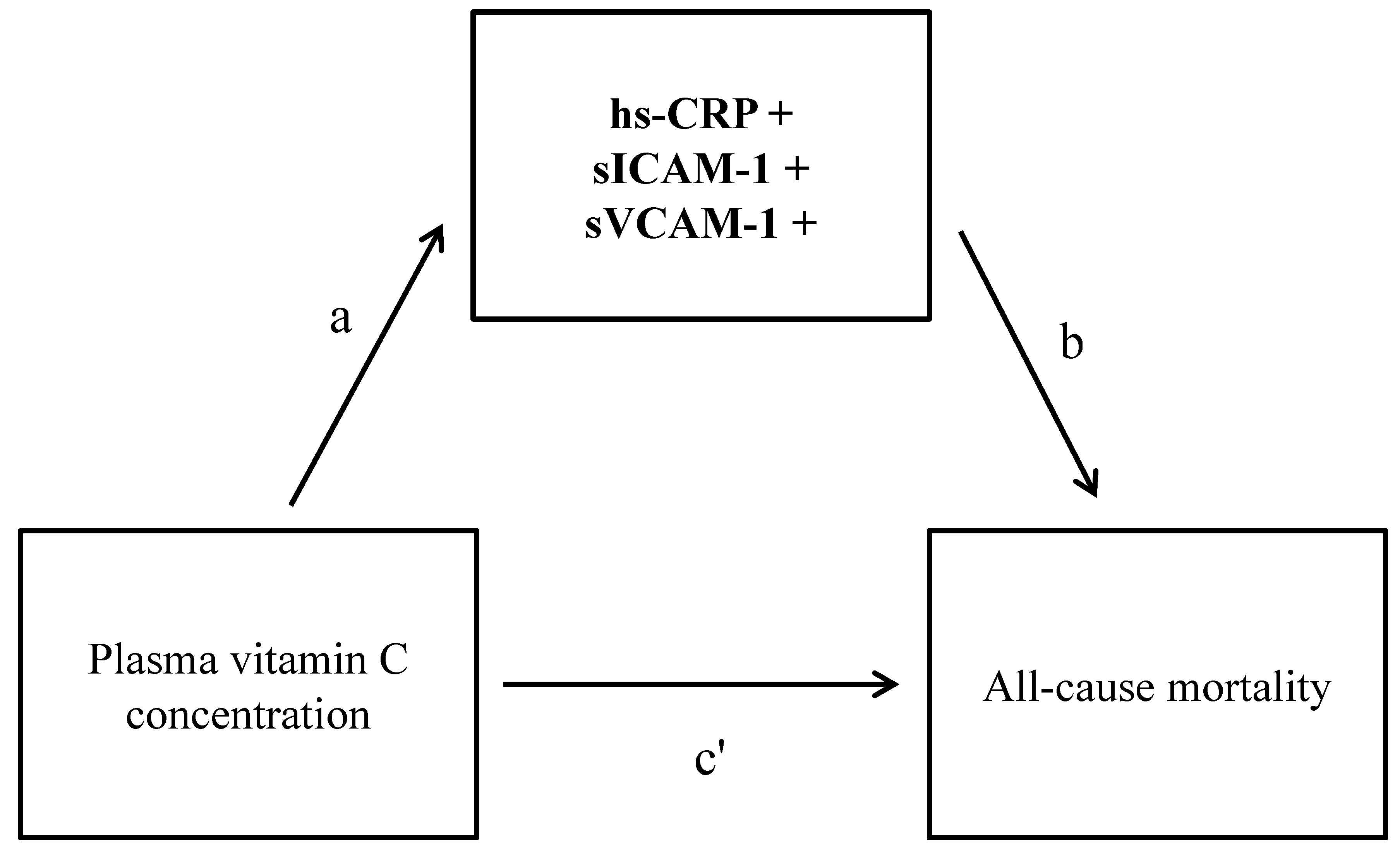
3.4. Mediation Analyses
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
References
- Schippers, H.; Kalff, M.W. Cost Comparison Haemodialysis and Renal Transplantation. HLA 1976, 7, 86–90. [Google Scholar] [CrossRef]
- Laupacis, A.; Keown, P.; Pus, N.; Krueger, H.; Ferguson, B.; Wong, C.; Muirhead, N. A Study of the Quality of Life and Cost-Utility of Renal Transplantation. Kidney Int. 1996, 50, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Jofre, R.; Lopez-Gomez, J.M.; Moreno, F.; Sanz-Guajardo, D.; Valderrabano, F. Changes in Quality of Life After Renal Transplantation. Am. J. Kidney Dis. 1998, 32, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in all Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, M.; Ichikawa, Y.; Yoshiya, K.; Isotani, S.; Higuchi, A.; Nagano, S.; Arakawa, S.; Hamami, G.; Matsumoto, O.; Kamidono, S. Assessment of Health-Related Quality of Life in Renal Transplant and Hemodialysis Patients using the SF-36 Health Survey. Urology 2000, 56, 201–206. [Google Scholar] [CrossRef]
- Oniscu, G.C.; Brown, H.; Forsythe, J.L. Impact of Cadaveric Renal Transplantation on Survival in Patients Listed for Transplantation. J. Am. Soc. Nephrol. 2005, 16, 1859–1865. [Google Scholar] [CrossRef] [PubMed]
- Chkhotua, A.; Pantsulaia, T.; Managadze, L. The Quality of Life Analysis in Renal Transplant Recipients and Dialysis Patients. Georgian Med. News 2011, 11, 10–17. [Google Scholar] [PubMed]
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared with Dialysis in Clinically Relevant Outcomes. Am. J. Transpl. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Oterdoom, L.H.; de Vries, A.P.; van Ree, R.M.; Gansevoort, R.T.; van Son, W.J.; van der Heide, J.J.H.; Navis, G.; de Jong, P.E.; Gans, R.O.; Bakker, S.J. N-Terminal Pro-B-Type Natriuretic Peptide and Mortality in Renal Transplant Recipients Versus the General Population. Transplantation 2009, 87, 1562–1570. [Google Scholar] [CrossRef] [PubMed]
- Kocak, H.; Ceken, K.; Yavuz, A.; Yucel, S.; Gurkan, A.; Erdogan, O.; Ersoy, F.; Yakupoglu, G.; Demirbas, A.; Tuncer, M. Effect of Renal Transplantation on Endothelial Function in Haemodialysis Patients. Nephrol. Dial. Transpl. 2006, 21, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, K.; Tonbul, H.Z.; Toker, A.; Gaipov, A.; Erdur, F.M.; Cicekler, H.; Anil, M.; Ozbek, O.; Selcuk, N.Y.; Yeksan, M. The Relationship between Oxidative Stress, Inflammation, and Atherosclerosis in Renal Transplant and End-Stage Renal Disease Patients. Ren. Fail. 2012, 34, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Ocak, N.; Dirican, M.; Ersoy, A.; Sarandol, E. Adiponectin, Leptin, Nitric Oxide, and C-Reactive Protein Levels in Kidney Transplant Recipients: Comparison with the Hemodialysis and Chronic Renal Failure. Ren. Fail. 2016, 38, 1639–1646. [Google Scholar] [CrossRef] [PubMed]
- Cañas, L.; Iglesias, E.; Pastor, M.C.; Barallat, J.; Juega, J.; Bancu, I.; Lauzurica, R. Inflammation and Oxidation: Do they Improve After Kidney Transplantation? Relationship with Mortality After Transplantation. Int. Urol. Nephrol. 2017, 49, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Lorenz, M.; Kramar, R.; Födinger, M.; Hörl, W.H.; Sunder-Plassmann, G. C-Reactive Protein and Body Mass Index Independently Predict Mortality in Kidney Transplant Recipients. Am. J. Transplant. 2004, 4, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- Abedini, S.; Holme, I.; Marz, W.; Weihrauch, G.; Fellstrom, B.; Jardine, A.; Cole, E.; Maes, B.; Neumayer, H.H.; Gronhagen-Riska, C.; et al. Inflammation in Renal Transplantation. Clin. J. Am. Soc. Nephrol. 2009, 4, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Langlois, M.; Duprez, D.; Delanghe, J.; De Buyzere, M.; Clement, D.L. Serum Vitamin C Concentration is Low in Peripheral Arterial Disease and is Associated with Inflammation and Severity of Atherosclerosis. Circulation 2001, 103, 1863–1868. [Google Scholar] [CrossRef] [PubMed]
- Korantzopoulos, P.; Kolettis, T.M.; Kountouris, E.; Dimitroula, V.; Karanikis, P.; Pappa, E.; Siogas, K.; Goudevenos, J.A. Oral Vitamin C Administration Reduces Early Recurrence Rates After Electrical Cardioversion of Persistent Atrial Fibrillation and Attenuates Associated Inflammation. Int. J. Cardiol. 2005, 102, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Mikirova, N.; Casciari, J.; Rogers, A.; Taylor, P. Effect of High-Dose Intravenous Vitamin C on Inflammation in Cancer Patients. J. Transl. Med. 2012, 10, 189. [Google Scholar] [CrossRef] [PubMed]
- Mikirova, N.; Casciari, J.; Riordan, N.; Hunninghake, R. Clinical Experience with Intravenous Administration of Ascorbic Acid: Achievable Levels in Blood for Different States of Inflammation and Disease in Cancer Patients. J. Transl. Med. 2013, 11, 191. [Google Scholar] [CrossRef] [PubMed]
- Enstrom, J.E.; Kanim, L.E.; Klein, M.A. Vitamin C Intake and Mortality among a Sample of the United States Population. Epidemiology 1992, 3, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.K.; Shekelle, R.; Selwyn, B.J.; Tangney, C.; Stamler, J. Dietary Vitamin C and Β-Carotene and Risk of Death in Middle-Aged Men the Western Electric Study. Am. J. Epidemiol. 1995, 142, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Sahyoun, N.R.; Jacques, P.F.; Russell, R.M. Carotenoids, Vitamins C and E, and Mortality in an Eiderly Population. Am. J. Epidemiol. 1996, 144, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Loria, C.M.; Klag, M.J.; Caulfield, L.E.; Whelton, P.K. Vitamin C Status and Mortality in US Adults. Am. J. Clin. Nutr. 2000, 72, 139–145. [Google Scholar] [PubMed]
- Khaw, K.; Bingham, S.; Welch, A.; Luben, R.; Wareham, N.; Oakes, S.; Day, N. Relation between Plasma Ascorbic Acid and Mortality in Men and Women in EPIC-Norfolk Prospective Study: A Prospective Population Study. Lancet 2001, 357, 657–663. [Google Scholar] [CrossRef]
- Irwin, M.I.; Hutchins, B.K. A Conspectus of Research on Vitamin C Requirements of Man. J. Nutr. 1976, 106, 821–879. [Google Scholar] [PubMed]
- Jacob, R.A.; Skala, J.H.; Omaye, S.T. Biochemical Indices of Human Vitamin C Status. Am. J. Clin. Nutr. 1987, 46, 818–826. [Google Scholar] [PubMed]
- Sauberlich, H.E.; Kretsch, M.J.; Taylor, P.C.; Johnson, H.L.; Skala, J.H. Ascorbic Acid and Erythorbic Acid Metabolism in Nonpregnant Women. Am. J. Clin. Nutr. 1989, 50, 1039–1049. [Google Scholar] [PubMed]
- Blanchard, J.; Conrad, K.A.; Watson, R.R.; Garry, P.J.; Crawley, J.D. Comparison of Plasma, Mononuclear and Polymorphonuclear Leucocyte Vitamin C Levels in Young and Elderly Women during Depletion and Supplementation. Eur. J. Clin. Nutr. 1989, 43, 97–106. [Google Scholar] [PubMed]
- Jacob, R.A. Assessment of Human Vitamin C status12. J. Nutr. 1990, 120, 1480–1485. [Google Scholar] [PubMed]
- Johnston, C.S.; Thompson, L.L. Vitamin C Status of an Outpatient Population. J. Am. Coll. Nutr. 1998, 17, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.S.; Solomon, R.E.; Corte, C. Vitamin C Depletion is Associated with Alterations in Blood Histamine and Plasma Free Carnitine in Adults. J. Am. Coll. Nutr. 1996, 15, 586–591. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, K.; Sanders, J.S.; Stegeman, C.; Smit, A.; Kallenberg, C.G.; Bijl, M. Accelerated Atherosclerosis in Patients with Wegener’s Granulomatosis. Ann. Rheum. Dis. 2005, 64, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Montoye, H.J.; Kemper, H.C.; Saris, W.H.; Washburn, R.A. Measuring Physical Activity and Energy Expenditure; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS Procedures for Estimating Indirect Effects in Simple Mediation Models. Behav. Res. Methods 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Zhang, K.; Li, Y.; Cheng, X.; Liu, L.; Bai, W.; Guo, W.; Wu, L.; Zuo, L. Cross-over study of influence of oral vitamin C supplementation on inflammatory status in maintenance hemodialysis patients. BMC Nephrol. 2013, 14, 252. [Google Scholar] [CrossRef] [PubMed]
- Attallah, N.; Osman-Malik, Y.; Frinak, S.; Besarab, A. Effect of intravenous ascorbic acid in hemodialysis patients with EPO-hyporesponsive anemia and hyperferritinemia. Am. J. Kidney Dis. 2006, 47, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Koenig, W.; Sund, M.; Frohlich, M.; Lowel, H.; Hutchinson, W.L.; Pepys, M.B. Refinement of the Association of Serum C-Reactive Protein Concentration and Coronary Heart Disease Risk by Correction for within-Subject Variation Over Time: The MONICA Augsburg Studies, 1984 and 1987. Am. J. Epidemiol. 2003, 158, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Danesh, J.; Wheeler, J.G.; Hirschfield, G.M.; Eda, S.; Eiriksdottir, G.; Rumley, A.; Lowe, G.D.; Pepys, M.B.; Gudnason, V. C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease. N. Engl. J. Med. 2004, 350, 1387–1397. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients | Vitamin C (Ln), µmol/L | |||
|---|---|---|---|---|---|
| Std. β | p Value | ||||
| No. of patients | 598 | - | - | ||
| Vitamin C, µmol/L | 44 (31–55) | - | - | ||
| Demographics | |||||
| Age, years | 51 ± 12 | −0.05 * | 0.23 * | ||
| Sex (male), n (%) | 328 (54) | −0.18 * | <0.001 * | ||
| Ethnicity (caucasian), n (%) | 577 (96) | −0.02 | 0.60 | ||
| Body Composition | |||||
| Body surface area, m2 | 1.87 ± 0.19 | −0.04 | 0.22 | ||
| Body mass index, kg/m2 | 26.0 ± 4.3 | −0.08 | 0.06 | ||
| Primary Renal Diseases | −0.02 | 0.61 | |||
| Primary glomerulonephritis, n (%) | 169 (28) | - | - | ||
| Glomerulonephritis due to vascular or autoimmune disease, n (%) | 36 (6) | - | - | ||
| Tubulointerstitial nephritis and pyelonephritis, n (%) | 92 (15) | - | - | ||
| Polycystic kidney disease, n (%) | 106 (18) | - | - | ||
| Dysplasia and hypoplasia, n (%) | 21 (4) | - | - | ||
| Renovascular disease, n (%) | 32 (5) | - | - | ||
| Diabetic nephropathy, n (%) | 22 (4) | - | - | ||
| Hereditary diseases and other, n (%) | 117 (20) | - | - | ||
| Tobacco Use | −0.08 | 0.06 | |||
| Never smoker, n (%) | 214 (35) | - | - | ||
| Ex-smoker, n (%) | 251 (42) | - | - | ||
| Current smoker, n (%) | 131 (21) | - | - | ||
| Blood Pressure | |||||
| Systolic blood pressure, mmHg | 153 ± 22 | −0.11 | 0.004 | ||
| Diastolic blood pressure, mmHg | 89 ± 9 | −0.11 | 0.01 | ||
| Use of ACE-inhibitor or aII-antagonist, n (%) | 201 (33) | 0.07 | 0.11 | ||
| Use of beta-blocker, n (%) | 368 (61) | −0.07 | 0.11 | ||
| Prior History of CV Disease | |||||
| History of MI, n (%) | 48 (8) | −0.01 | 0.75 | ||
| History of TIA/CVA, n (%) | 32 (5) | −0.04 | 0.36 | ||
| Transplantation | |||||
| Time since transplantation, years | 5.9 (2.6–11.4) | 0.20 | <0.001 | ||
| Dialysis vintage, months | −0.14 | 0.001 | |||
| 141 (24) | - | - | |||
| 1–5 years | 363 (61) | - | - | ||
| >5 years | 94 (16) | - | - | ||
| Deceased donor, n (%) | 515 (86) | 0.02 | 0.61 | ||
| Immunosuppressive Therapy | |||||
| Prednisolone, mg/day | 10.0 (7.5–10.0) | −0.11 | 0.008 | ||
| Use of calcineurin inhibitors | −0.09 | 0.02 | |||
| Cyclosporine, n (%) | 386 (65) | - | - | ||
| Tacrolimus, n (%) | 84 (14) | - | - | ||
| None, n (%) | 128 (21) | - | - | ||
| Use of antimetabolites | −0.06 | 0.19 | |||
| Azathioprine, n (%) | 194 (32) | - | - | ||
| Mycophenolic acid, n (%) | 247 (41) | - | - | ||
| None, (%) | 157 (26) | - | - | ||
| Use of m-TOR inhibitors, n (%) | 10 (2) | −0.10 | 0.02 | ||
| Induction therapy | −0.20 | <0.001 | |||
| Anti-thymocyte globulin, n (%) | 70 (12) | - | - | ||
| Muromonab-CD3 , n (%) | 26 (4) | - | - | ||
| Anti-CD25 monoclonal antibodies, n (%) | 10 (2) | - | - | ||
| None, n (%) | 492 (82) | - | - | ||
| Acute rejection treatment | −0.13 | 0.03 | |||
| High doses of steroids, n (%) | 186 (31) | - | - | ||
| Other rejection therapy, n (%) | 82 (14) | - | - | ||
| Cumulative dose of prednisolone, grams | 21.3 (11.3–37.9) | 0.21 | <0.001 | ||
| Ischemia Times | |||||
| Cold ischemia time, hours | 22 (15–27) | 0.01 | 0.75 | ||
| Total warm ischemia, minutes | 35 (30–45) | 0.02 | 0.72 | ||
| Renal Allograft Function | |||||
| eGFR, mL/min/1.73 m2 | 47 ± 15 | 0.11 | 0.009 | ||
| Urinary protein excretion, g/24 h | 0.2 (0.0–0.5) | −0.06 | 0.22 | ||
| Proteinuria (>0.5 g/24 h), n (%) | 166 (27) | −0.11 | 0.006 | ||
| Inflammation | |||||
| hs-CRP, mg/L | 2.0 (0.7–4.8) | −0.19 | <0.001 | ||
| sICAM-1, ng/L | 602 (514–720) | −0.17 | <0.001 | ||
| sVCAM-1, ng/L | 965 (772–1196) | −0.16 | <0.001 | ||
| Lipids | |||||
| Total colesterol, mmol/L | 5.6 ± 1.0 | 0.05 | 0.24 | ||
| HDL colesterol, mmol/L | 1.0 ± 0.3 | 0.11 | 0.004 | ||
| LDL cholesterol, mmol/L | 3.5 ± 0.9 | 0.07 | 0.09 | ||
| Triglycerides, mmol/L | 1.9 (1.4–2.6) | −0.13 | 0.001 | ||
| Use of statins, n (%) | 295 (49) | 0.06 | 0.13 | ||
| Oxidative Stress | |||||
| Gamma glutamate, U/L | 24 (18–39) | −0.10 | 0.02 | ||
| Alkaline phophatase, U/L | 72 (57–94) | −0.21 | <0.001 | ||
| Uric acid, mmol/L | 0.4 (0.3–0.5) | −0.08 | 0.05 | ||
| Glucose Homeostasis | |||||
| Insulin, µU/mL | 11 (7–16) | −0.08 | 0.04 | ||
| Glucose, mmol/L | 4.5 (4.1–5.0) | −0.07 | 0.06 | ||
| HbA1c, % | 6.5 ± 1.0 | −0.12 | 0.002 | ||
| Diabetes, n (%) | 105 (17) | −0.11 | 0.008 | ||
| Hematology | |||||
| Leukocyte count, x 109/L | 8.5 ± 2.4 | −0.03 | 0.42 | ||
| Hemoglobin, mmol/L | 8.5 ± 0.9 | 0.01 | 0.77 | ||
| Platelets count, x 109/L | 231 ± 69 | −0.02 | 0.56 | ||
| Vitamin C, Status | Vitamin C, Continuous | ||||||
|---|---|---|---|---|---|---|---|
| ≤28 µmol/L n = 133 | >28 µmol/L n = 465 | 2log, µmol/L n = 598 | |||||
| HR | 95% CI | p | Reference | HR | 95% CI | p | |
| Model 1 | 1.95 | 1.35–2.81 | <0.001 | 1.00 | 0.71 | 0.59–0.87 | 0.001 |
| Model 2 | 1.92 | 1.33–2.77 | 0.001 | 1.00 | 0.74 | 0.61–0.90 | 0.002 |
| Model 3 | 1.88 | 1.28–2.76 | 0.001 | 1.00 | 0.76 | 0.62–0.94 | 0.011 |
| Model 4 | 1.91 | 1.30–2.82 | 0.001 | 1.00 | 0.76 | 0.62–0.94 | 0.012 |
| Model 5 | 1.80 | 1.22–2.65 | 0.003 | 1.00 | 0.79 | 0.64–0.98 | 0.030 |
| Model 6 | 1.70 | 1.15–2.52 | 0.008 | 1.00 | 0.79 | 0.63–0.98 | 0.030 |
| Model 7 | 1.74 | 1.18–2.57 | 0.005 | 1.00 | 0.78 | 0.63–0.97 | 0.024 |
| Potential Mediator | Effect (Path) * | Multivariate Model ** | |
|---|---|---|---|
| Coefficient (95% CI) † | Proportion Mediated | ||
| hs-CRP | Indirect effect (ab path) | −0.016 (−0.036; −0.004) | 16% *** |
| Total effect (ab + c’ path) | −0.103 (−0.189; −0.010) | ||
| sICAM-1 | Indirect effect (ab path) | −0.018 (−0.043; −0.003) | 17% *** |
| Total effect (ab + c’ path) | −0.103 (−0.194; −0.016) | ||
| sVCAM-1 | Indirect effect (ab path) | −0.015 (−0.040; −0.003) | 15% *** |
| Total effect (ab + c’ path) | −0.103 (−0.200; −0.015) | ||
| Combined inflammation | Indirect effect (ab path) | −0.033 (−0.065; −0.012) | 32% *** |
| Total effect (ab + c’ path) | −0.103 (−0.191; −0.013) | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotomayor, C.G.; Eisenga, M.F.; Gomes Neto, A.W.; Ozyilmaz, A.; Gans, R.O.B.; Jong, W.H.A.d.; Zelle, D.M.; Berger, S.P.; Gaillard, C.A.J.M.; Navis, G.J.; et al. Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients. Nutrients 2017, 9, 568. https://doi.org/10.3390/nu9060568
Sotomayor CG, Eisenga MF, Gomes Neto AW, Ozyilmaz A, Gans ROB, Jong WHAd, Zelle DM, Berger SP, Gaillard CAJM, Navis GJ, et al. Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients. Nutrients. 2017; 9(6):568. https://doi.org/10.3390/nu9060568
Chicago/Turabian StyleSotomayor, Camilo G., Michele F. Eisenga, Antonio W. Gomes Neto, Akin Ozyilmaz, Rijk O.B. Gans, Wilhelmina H.A. de Jong, Dorien M. Zelle, Stefan P. Berger, Carlo A. J.M. Gaillard, Gerjan J. Navis, and et al. 2017. "Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients" Nutrients 9, no. 6: 568. https://doi.org/10.3390/nu9060568
APA StyleSotomayor, C. G., Eisenga, M. F., Gomes Neto, A. W., Ozyilmaz, A., Gans, R. O. B., Jong, W. H. A. d., Zelle, D. M., Berger, S. P., Gaillard, C. A. J. M., Navis, G. J., & Bakker, S. J. L. (2017). Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients. Nutrients, 9(6), 568. https://doi.org/10.3390/nu9060568