Micronutrient Status among Pregnant Women in Zinder, Niger and Risk Factors Associated with Deficiency

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
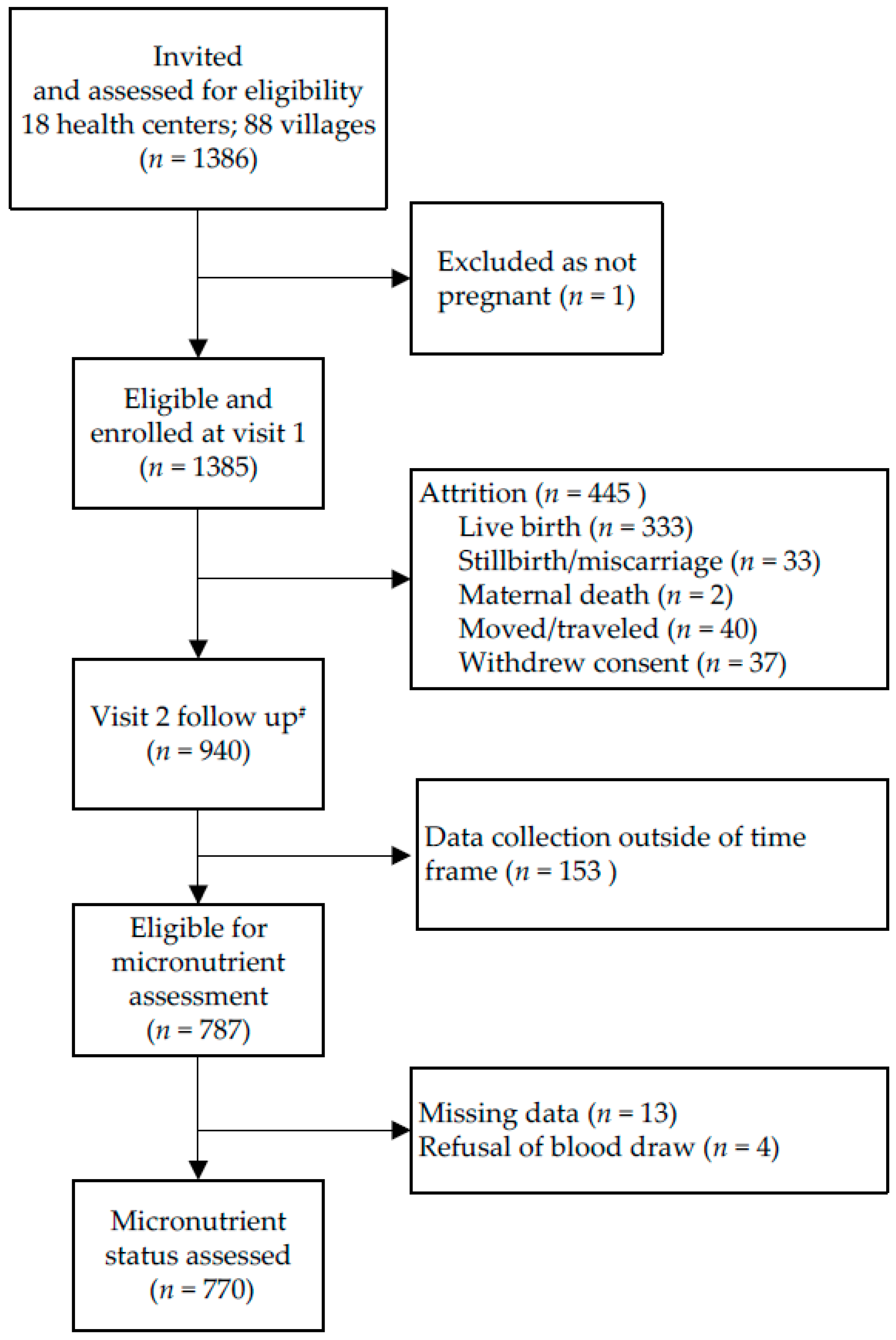
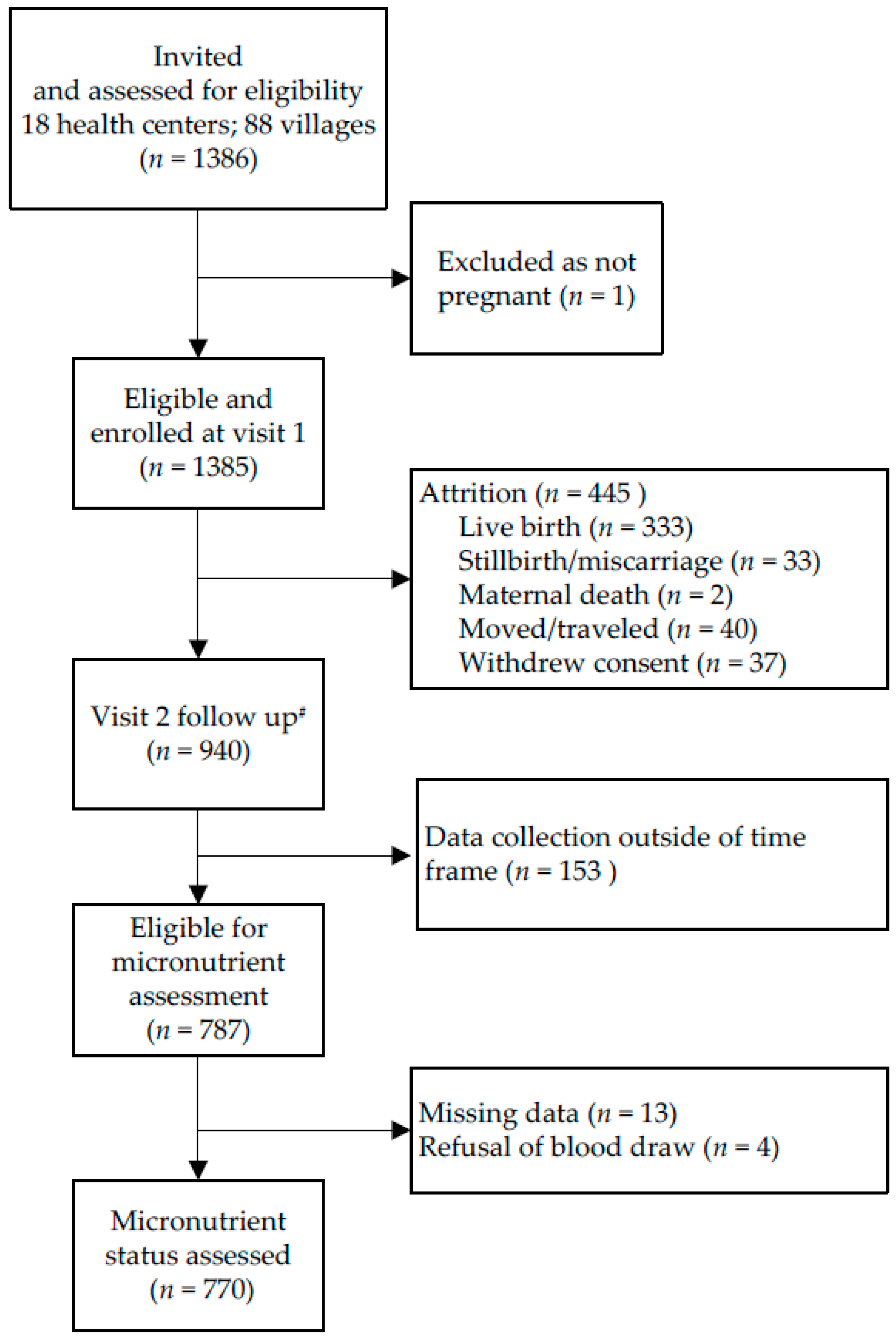
2.2. Study Participants
2.3. Ethical Considerations
2.4. Data Collection
2.5. Biochemical Assessments
2.6. Sample Size
2.7. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Associations with Hemoglobin, Ferritin, Soluble Transferrin Receptor and Zinc
3.3. Associations with Retinol Binding Protein, Vitamin B12 and Folate Status
3.4 Predictors of Multiple Micronutrient Deficiencies
3.5. Multivariable Models
4. Discussion
4.1. Associations between MN Deficiencies and Predictors
4.1.1. Trimester
4.1.2. Season
4.1.3. Demographic and SES Factors
4.1.4. Obstetric History
4.1.5. Knowledge Attitudes and Practices
4.1.6. Nutritional and Health Status
4.2. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AGP | α-1-acid glycoprotein |
| ANC | antenatal care |
| APP | acute phase proteins |
| CRP | C-reactive protein |
| CS | health post |
| CSI | integrated health center |
| DHS | demographic and health survey |
| ENA | essential nutrition actions |
| Hb | Hemoglobin |
| HFIAS | Household Food Insecurity Access Scale |
| HRP2 | histidine-rich protein II |
| IFA | iron and folic acid |
| KAP | knowledge, attitudes and practices |
| LMP | last menstrual period |
| MDD-W | minimum dietary diversity—women |
| MN | micronutrient |
| MMN | multiple micronutrient |
| MUAC | mid-upper arm circumference |
| pZn | plasma zinc |
| RBP | retinol binding protein |
| SES | socio-economic status |
| SFH | symphysis-fundal height |
| sTfR | soluble transferrin receptor |
| WHO | World Health Organization |
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Mori, R.; Ota, E.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2012, 2, CD000230. [Google Scholar]
- Burke, R.M.; Leon, J.S.; Suchdev, P.S. Identification, prevention and treatment of iron deficiency during the first 1000 days. Nutrients 2014, 6, 4093–4114. [Google Scholar] [CrossRef] [PubMed]
- Darnton-Hill, I.; Mkparu, U.C. Micronutrients in pregnancy in low- and middle-income countries. Nutrients 2015, 7, 1744–1768. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef]
- Pena-Rosas, J.P.; De-Regil, L.M.; Garcia-Casal, M.N.; Dowswell, T. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2015, 12, CD004736. [Google Scholar]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Ferguson, E.L.; Penrose, K.; Arimond, M. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. J. Nutr. 2010, 140, 2051S–2058S. [Google Scholar] [CrossRef] [PubMed]
- Institut National de la Statistique (INS); ICF International. Enquête Démographique et de Santé et à Indicateurs Multiples du Niger 2012; INS et ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- United Nations Development Programme. Human Development Reports. Human Development Indicators, Niger. 2016. Available online: http://hdr.undp.org/en/countries/profiles/NER (accessed on 16 November 2016).
- World Health Organization. The Global Prevalence of Anaemia in 2011; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Institut National de la Statistique, Ministère de l’Économie et des Finances; Macro International Inc. Niger: Enquête Démographique et de Santé et à Indicateurs Multiples 2006; Institut National de la Statistique, Ministère de l’Économie et des Finances: Niamey, Niger, 2007.
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Ministere de la Sante Publique; Module de Formation en Consultation Prenatale Recentree (CPNR). Manuel du Formateur; Ministry of Health: Niamey, Niger, 2008. [Google Scholar]
- Hampshire, R.D.; Aguayo, V.M.; Harouna, H.; Roley, J.A.; Tarini, A.; Baker, S.K. Delivery of nutrition services in health systems in sub-Saharan Africa: opportunities in Burkina Faso, Mozambique and Niger. Public Health Nutr. 2004, 7, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Designing Household Survey Samples: Practical Guidelines; Department of Economic and Social Affairs, Statistics Division; United Nations Publication: New York, NY, USA, 2008; Available online: http://www.un-ilibrary.org/economic-and-social-development/designing-household-survey-samples_f7348051-en (accessed on 16 November 2016).
- Cogill, B. Anthropometric Indicators Measurement Guide; Food and Nutrition Technical Assistance Project; Academy for Educational Development: Washington, DC, USA, 2003. [Google Scholar]
- King Edward Memorial Hospital. Clinical Guidelines: 1 Antepartum Care—1.6.3 Measuring Fundal Height with a Tape Measure. Available online: http://www.kemh.health.wa.gov.au/development/manuals/O%26G_guidelines/sectionb/1/b1.6.3.pdf (accessed on 12 April 2013).
- Ververs, M.T.; Antierens, A.; Sackl, A.; Staderini, N.; Captier, V. Which anthropometric indicators identify a pregnant woman as acutely malnourished and predict adverse birth outcomes in the humanitarian context? PLoS Curr. 2013, 5. [Google Scholar] [CrossRef] [PubMed]
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Begum, K.O.C.; Wessells, K.R.; Young, R.R.; Faye, M.T.; Wuehler, S.E.; Hess, S.Y. Prevalence of and factors associated with antenatal care seeking and adherence to recommended iron-folic acid supplementation among pregnant women in Zinder, Niger. Matern. Child Nutr. 2017, in press. [Google Scholar]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v.3); FHI 360/FANTA: Washington, DC, USA, 2007. [Google Scholar]
- Papageorghiou, A.T.; Ohuma, E.O.; Gravett, M.G.; Hirst, J.; da Silveira, M.F.; Lambert, A.; Carvalho, M.; Jaffer, Y.A.; Altman, D.G.; Altman, J.A.; et al. International standards for symphysis-fundal height based on serial measurements from the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project: prospective cohort study in eight countries. BMJ 2016, 355, i5662. [Google Scholar] [CrossRef] [PubMed]
- Hess, S.Y.; Ouedraogo, C.T. NiMaNu Project [Internet]. Open Science Framework. 2016. Available online: https://osf.io/4cenf. (accessed on 8 November 2016).
- International Zinc Nutrition Consultative Group (IZiNCG). Assessing Population Zinc Status with Serum Zinc Concentration. IZiNCG Technical Brief No. 2; University of California: Davis, CA, USA, 2012; Available online: http://www.izincg.org (accessed on 26 March 2014).
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lönnerdal, B.; Ruel, M.T.; Sandtröm, B.; Wasantwisut, E.; Hotz, C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar] [PubMed]
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined measurement of ferritin, soluble transferrin receptor, retinol binding protein, and C-reactive protein by an inexpensive, sensitive, and simple sandwich enzyme-linked immunosorbent assay technique. J. Nutr. 2004, 134, 3127–3132. [Google Scholar] [PubMed]
- Engle-Stone, R.; Nankap, M.; Ndjebayi, A.O.; Erhardt, J.G.; Brown, K.H. Plasma ferritin and soluble transferrin receptor concentrations and body iron stores identify similar risk factors for iron deficiency but result in different estimates of the national prevalence of iron deficiency and iron-deficiency anemia among women and children in Cameroon. J. Nutr. 2013, 143, 369–377. [Google Scholar] [PubMed]
- Suchdev, P.S.; Namaste, S.M.; Aaron, G.J.; Raiten, D.J.; Brown, K.H.; Flores-Ayala, R. Overview of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project. Adv. Nutr. 2016, 7, 349–356. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Serum Ferritin Concentrations for the Assessment of Iron Status and Iron Deficiency in Populations (WHO/NMH/NHD/MNM/11.2); Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Engle-Stone, R.; Haskell, M.J.; Ndjebayi, A.O.; Nankap, M.; Erhardt, J.G.; Gimou, M.M.; Brown, K.H. Plasma retinol-binding protein predicts plasma retinol concentration in both infected and uninfected Cameroonian women and children. J. Nutr. 2011, 141, 2233–2241. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, J.F.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.D.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development-Folate Review. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H.; Miller, J.W.; Rosenberg; Smith, D.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND): Vitamin B-12 Review. J. Nutr. 2017, in press. [Google Scholar]
- Ota, E.; Hori, H.; Mori, R.; Tobe-Gai, R.; Farrar, D. Antenatal dietary education and supplementation to increase energy and protein intake. Cochrane Database Syst. Rev. 2015, 9, CD000032. [Google Scholar]
- Girard, A.W.; Olude, O. Nutrition education and counselling provided during pregnancy: effects on maternal, neonatal and child health outcomes. Paediatr. Perinat Epidemiol. 2012, 26, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Mullany, L.C.; Hurley, K.M.; Katz, J.; Black, R.E. Nutrition and maternal, neonatal, and child health. Semin. Perinatol. 2015, 39, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Zagre, N.M.; Desplats, G.; Adou, P.; Mamadoultaibou, A.; Aguayo, V.M. Prenatal multiple micronutrient supplementation has greater impact on birthweight than supplementation with iron and folic acid: A cluster-randomized, double-blind, controlled programmatic study in rural Niger. Food Nutr. Bull. 2007, 28, 317–327. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Harding, K.B.; Roche, M.L. Preconceptional Nutrition Interventions for Adolescent Girls and Adult Women: Global Guidelines and Gaps in Evidence and Policy with Emphasis on Micronutrients. J. Nutr. 2016, 146, 1461S–1470S. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, S. Assessment and interpretation of micronutrient status during pregnancy. Proc. Nutr Soc. 2008, 67, 437–450. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Niger: Food Security and Safety Nets. Report No. 44072-NE. 18 February 2009. Available online: http://reliefweb.int/sites/reliefweb.int/files/resources/fullreport_154.pdf (accessed on 17 November 2016).
- Becquey, E.; Delpeuch, F.; Konate, A.M.; Delsol, H.; Lange, M.; Zoungrana, M.; Martin-Prevel, Y. Seasonality of the dietary dimension of household food security in urban Burkina Faso. Br. J. Nutr. 2012, 107, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Toe, L.C.; Bouckaert, K.P.; De Beuf, K.; Roberfroid, D.; Meda, N.; Thas, O.; Van Camp, J.; Kolsteren, P.W.; Huybregts, L.F. Seasonality modifies the effect of a lipid-based nutrient supplement for pregnant rural women on birth length. J. Nutr. 2015, 145, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Salas, P.; Moore, S.E.; Cole, D.; da Costa, K.A.; Cox, S.E.; Dyer, R.A.; Fulford, A.J.; Innis, S.M.; Waterland, R.A.; Zeisel, S.H.; et al. DNA methylation potential: dietary intake and blood concentrations of one-carbon metabolites and cofactors in rural African women. Am. J. Clin. Nutr. 2013, 97, 1217–1227. [Google Scholar] [CrossRef] [PubMed]
- Hartikainen, H.; Maleta, K.; Kulmala, T.; Ashorn, P. Seasonality of gestational weight gain and foetal growth in rural Malawi. East Afr. Med. J. 2005, 82, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Rayco-Solon, P.; Fulford, A.J.; Prentice, A.M. Differential effects of seasonality on preterm birth and intrauterine growth restriction in rural Africans. Am. J. Clin. Nutr. 2005, 81, 134–139. [Google Scholar] [PubMed]
- Bates, C.J.; Prentice, A.M.; Paul, A.A. Seasonal variations in vitamins A, C, riboflavin and folate intakes and status of pregnant and lactating women in a rural Gambian community: Some possible implications. Eur. J. Clin. Nutr. 1994, 48, 660–668. [Google Scholar] [PubMed]
- Rah, J.H.; Christian, P.; Shamim, A.A.; Arju, U.T.; Labrique, A.B.; Rashid, M. Pregnancy and lactation hinder growth and nutritional status of adolescent girls in rural Bangladesh. J. Nutr. 2008, 138, 1505–1511. [Google Scholar] [PubMed]
- Ganchimeg, T.; Ota, E.; Morisaki, N.; Laopaiboon, M.; Lumbiganon, P.; Zhang, J.; Yamdamsuren, B.; et al. Pregnancy and childbirth outcomes among adolescent mothers: A World Health Organization multicountry study. BJOG 2014, 121, 40–48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Early Pregnancy and Poor Reproductive Outcomes among Adolescents in Developing Countries: What the Evidence Says; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Bhutta, Z.A.; Lassi, Z.S.; Blanc, A.; Donnay, F. Linkages among reproductive health, maternal health, and perinatal outcomes. Semin. Perinatol. 2010, 34, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Conde-Agudelo, A.; Rosas-Bermudez, A.; Castano, F.; Norton, M.H. Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Stud. Fam. Plan. 2012, 43, 93–114. [Google Scholar] [CrossRef]
- Rutstein, S.O. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: Evidence from the demographic and health surveys. Int. J. Gynaecol. Obstet. 2005, 89, S7–S24. [Google Scholar] [CrossRef] [PubMed]
- Martin-Prével, Y.A.P.; Arimond, M.; Ballard, T.; Deitchler, M.; Dop, M.C.; Kennedy, G.; Lee, W.T.; Mousi, M. Moving Forward on Choosing a Standard Operational Indicator of Women’s Dietary Diversity; FAO: Rome, Italy, 2015. [Google Scholar]
- Guyon, A.B.; Quinn, V.J. Booklet on Key Essential Nutrition Actions Messages; Core Group: Washington, DC, USA, 2011. [Google Scholar]
- Antelman, G.; Msamanga, G.I.; Spiegelman, D.; Urassa, E.J.; Narh, R.; Hunter, D.J.; Fawzi, W.W. Nutritional factors and infectious disease contribute to anemia among pregnant women with human immunodeficiency virus in Tanzania. J. Nutr. 2000, 130, 1950–1957. [Google Scholar] [PubMed]
- Adam, I.; Khamis, A.H.; Elbashir, M.I. Prevalence and risk factors for anaemia in pregnant women of eastern Sudan. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Young, S.L.; Khalfan, S.S.; Farag, T.H.; Kavle, J.A.; Ali, S.M.; Hajji, H.; Rasmussen, K.M.; Pelto, G.H.; Tielsch, J.M.; Stoltzfus, R.J.; et al. Association of pica with anemia and gastrointestinal distress among pregnant women in Zanzibar, Tanzania. Am. J. Trop. Med. Hyg. 2010, 83, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Young, S.L. Pica in pregnancy: new ideas about an old condition. Annu. Rev. Nutr. 2010, 30, 403–422. [Google Scholar] [CrossRef] [PubMed]
- Miao, D.; Young, S.L.; Golden, C.D. A meta-analysis of pica and micronutrient status. Am. J. Hum. Biol. 2015, 27, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Wessells, K.R.; Hess, S.Y.; Ouedraogo, Z.P.; Rouamba, N.; Ouedraogo, J.B.; Brown, K.H. Asymptomatic malaria infection affects the interpretation of biomarkers of iron and vitamin A status, even after adjusting for systemic inflammation, but does not affect plasma zinc concentrations among young children in Burkina Faso. J. Nutr. 2014, 144, 2050–2058. [Google Scholar] [CrossRef] [PubMed]
- Radeva-Petrova, D.; Kayentao, K.; ter Kuile, F.O.; Sinclair, D.; Garner, P. Drugs for preventing malaria in pregnant women in endemic areas: Any drug regimen versus placebo or no treatment. Cochrane Database Syst. Rev. 2014, 10, CD000169. [Google Scholar]
- Eisele, T.P.; Larsen, D.; Steketee, R.W. Protective efficacy of interventions for preventing malaria mortality in children in Plasmodium falciparum endemic areas. Int. J. Epidemiol. 2010, 39, i88–i101. [Google Scholar] [CrossRef] [PubMed]
- Hess, S.Y.; Ouedraogo, C.T.; Young, R.R.; Bamba, I.F.; Stinca, S.; Zimmermann, M.B.; Wessells, K.R. Urinary iodine concentration identifies pregnant women as iodine deficient yet school-aged children as iodine sufficient in rural Niger. Public Health Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Abioye, A.I.; Aboud, S.; Premji, Z.; Etheredge, A.J.; Gunaratna, N.S.; Sudfeld, C.R.; Mongi, R.; Meloney, L.; Darling, A.M.; Noor, R.; et al. Iron Supplementation Affects Hematologic Biomarker Concentrations and Pregnancy Outcomes among Iron-Deficient Tanzanian Women. J. Nutr. 2016, 146, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Kearns, A.D.; Caglia, J.M.; Ten Hoope-Bender, P.; Langer, A. Antenatal and postnatal care: A review of innovative models for improving availability, accessibility, acceptability and quality of services in low-resource settings. BJOG 2016, 123, 540–548. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Value |
|---|---|
| Participants (n) | 787 2 |
| Current pregnancy, trimester | |
| First | 1 (0.1) |
| Second | 236 (30.3) |
| Third | 542 (69.6) |
| Season | |
| June–September (Lean, rainy season) | 277 (35.2) |
| October–February (Post-harvest, cool season) | 286 (36.4) |
| March–May (Hot season) | 223 (28.4) |
| Demographic and socio-economic characteristics | |
| Age (year) 3 | 26.5 (26.0, 26.9) |
| Adolescent | 106 (13.8) |
| Household food insecurity access scale (HFIAS) score | 5.4 (4.7, 6.1) |
| Marital status | |
| Monogamous | 532 (68.0) |
| Polygamous, first wife | 95 (12.2) |
| Polygamous, ≥2nd wife | 155 (19.8) |
| Ethnicity, maternal | |
| Hausa | 671 (85.3) |
| Tuareg | 83 (10.6) |
| Other (minority) | 33 (4.2) |
| Education, maternal | |
| None | 458 (58.2) |
| Koranic schooling | 171 (21.7) |
| Primary (1–6 years) | 112 (14.2) |
| Secondary (7–14 years) | 46 (5.8) |
| Obstetric history | |
| Primigravida | 88 (11.2) |
| Age at first pregnancy (year) | 16.9 (16.7, 17.0) |
| Attended ANC in last pregnancy | 641 (91.8) |
| Result of last pregnancy | |
| Miscarriage, stillbirth | 26 (3.7) |
| Live birth, child deceased | 69 (9.9) |
| Live birth, child living | 604 (86.4) |
| Knowledge, attitudes and practices | |
| Attended ANC in current pregnancy | 562 (71.4) |
| IFA coverage | 489 (62.9) |
| IFA adherence (consumed daily for past 7 days) | 328 (42.3) |
| Utilization of mosquito net | 626 (79.5) |
| Quantity of food consumed during pregnancy (compared to non-pregnant state) | |
| Increased | 153 (19.5) |
| Decreased | 406 (51.7) |
| No change | 227 (28.9) |
| Number of meals consumed during pregnancy (compared to non-pregnant state) | |
| Increased | 134 (17.1) |
| Decreased | 352 (45.0) |
| No change | 297 (37.9) |
| Adequate minimum dietary diversity—women (MDD-W) 4 | 147 (18.7) |
| Consumed vitamin A rich foods in past 24 h | 680 (86.5) |
| Consumed animal source foods in past 24 h | 295 (37.5) |
| Geophagy (consumed clay) during pregnancy | 71 (9.0) |
| Nutritional and health status | |
| Height (cm) | 158.5 (157.9, 158.9) |
| Mid-upper arm circumference (MUAC; cm) | 24.7 (24.4, 25.0) |
| Gestational weight gain (kg/week) | 0.24 (0.20, 0.28) |
| Nightblindness | 9 (2.1) |
| Variable | Unadjusted | Adjusted for CRP/AGP 2 |
|---|---|---|
| Participants (n) 3 | 770 | 770 |
| Hb concentration, g/dL 4 | 9.6 (9.5,9.8) | - |
| Anemia, Hb < 10.5 g/dL (2nd trimester) or 11.0 g/dL (1st, 3rd trimester) | 601 (79.0) | - |
| Mild anemia (Hb 10.0–10.4 or 10.9 g/dL) | 173 (22.7) | - |
| Moderate anemia (Hb 7.0–9.9 g/dL) | 402 (52.8) | - |
| Severe anemia (Hb < 7.0 g/dL) | 26 (3.4) | - |
| Ferritin, µg/L | 30.5 (28.5, 32.7) | 27.3 (25.8, 28.8) |
| Iron deficiency, ferritin < 15 µg/L | 137 (17.8) | 159 (20.7) |
| sTfR, mg/L | 7.8 (7.5, 8.1) | - |
| Iron deficiency, sTfR > 8.3 mg/L | 275 (35.7) | - |
| pZn, µg/dL | 51.7 (51.0, 52.4) | 52.3 (51.6, 53.0) |
| Zinc deficiency, pZn < 50 µg/dL 5 | 311 (43.4) | 292 (40.7) |
| RBP, µmol/L | 1.05 (1.03, 1.08) | 1.07 (1.05, 1.10) |
| RBP < 0.70 µmol/L | 68 (8.8) | 57 (7.4) |
| Inadequate or marginal status, RBP < 1.32 µmol/L | 622 (80.8) | 614 (79.7) |
| B12, pmol/L | 169.9 (165.1, 174.9) | - |
| Inadequate status, B12 < 148 pmol/L | 259 (34.8) | - |
| Marginal status, B12, 148–221 pmol/L | 324 (43.5) | - |
| Folate, nmol/L | 10.5 (10.1, 10.9) | - |
| Inadequate status, folate < 10 nmol/L | 328 (44.3) | - |
| Micronutrient deficiency anemia 6 | ||
| Iron deficiency anemia (Anemia + ferritin < 15 µg/L) | 124 (16.3) | 142 (18.7) |
| Iron deficiency anemia (Anemia + sTfR > 8.3 mg/L) | 250 (32.9) | - |
| B12 deficiency anemia (Anemia + B12 < 148 pmol/L) | 208 (28.3) | - |
| Folate-deficiency anemia (Anemia + and folate < 10 nmol/L) | 265 (36.4) | - |
| Multiple micronutrient (MNN) deficiency 7 | ||
| 0 | 25 (3.6) | 24 (3.5) |
| 1 | 131 (19.0) | 131 (19.0) |
| 2 | 212 (30.8) | 222 (32.3) |
| 3 | 173 (25.2) | 164 (23.8) |
| 4 | 114 (16.6) | 114 (16.6) |
| 5 | 33 (4.8) | 33 (4.8) |
| AGP, g/L | 0.39 (0.38,0.40) | - |
| AGP > 1 g/L | 23 (3.0) | - |
| CRP, mg/L | 2.2 (2.0, 2.4) | - |
| CRP > 5 mg/L | 189 (24.6) | - |
| Malaria antigenemia (elevated HRP2) 8 | 97 (12.6) | - |
| Variable | Hemoglobin (g/dL) | Ferritin, Adjusted for APP (µg/L) 2,3 | Soluble Transferrin Receptor (mg/L) 2 | Zinc, Adjusted for APP (µg/dL) 3 | ||||
|---|---|---|---|---|---|---|---|---|
| Mean (95% CI) | p | Geometric Mean (95% CI) | p | Geometric Mean (95% CI) | p | Mean (95% CI) | p | |
| Current pregnancy, trimester 4 | 0.64 | <0.01 | <0.01 | <0.01 | ||||
| First | NA | NA | NA | NA | ||||
| Second | 9.7 (9.5, 9.9) | 32.0 (29.2, 35.1) | 7.0 (6.6, 7.5) | 55.5 (54.3, 56.7) | ||||
| Third | 9.6 (9.5, 9.8) | 25.4 (23.8, 27.0) | 8.1 (7.8, 8.5) | 50.9 (50.1, 51.7) | ||||
| Season | <0.01 | 0.14 | 0.04 | 0.29 | ||||
| June–September (Lean, rainy season) | 9.5 (9.1, 9.9) | 0.01 | 24.0 (20.1, 28.8) | 0.15 | 8.1 (7.2, 9.2) | 0.04 | 54.0 (51.7, 56.2) | 0.71 |
| October–February (Post-harvest, cool season) | 9.1 (8.6, 9.5) | <0.01 | 25.5 (20.5, 31.6) | 0.05 | 8.8 (7.7, 10.2) | <0.01 | 50.9 (48.2, 53.7) | 0.37 |
| March–May (Hot season) | 10.5 (10.0, 11.1) | REF | 34.4 (26.7, 44.3) | REF | 6.3 (5.3, 7.5) | REF | 51.9 (48.7, 55.1) | REF |
| Demographic and socio-economic characteristics | ||||||||
| Adolescent | <0.01 | <0.01 | 0.50 | 0.64 | ||||
| Yes | 9.2 (8.9, 9.5) | 32.1 (28.0, 36.8) | 8.0 (7.3, 8.7) | 52.7 (51.0, 54.4) | ||||
| No | 9.7 (9.6, 9.8) | 26.5 (25.0, 28.1) | 7.7 (7.4, 8.1) | 52.3 (51.6, 53.0) | ||||
| Marital status | 0.25 | 0.95 | 0.02 | 0.79 | ||||
| Monogamous | 9.7 (9.5, 9.8) | REF | 27.1 (25.4, 28.8) | REF | 7.8 (7.4, 8.1) | REF | 52.3 (51.5, 53.1) | REF |
| Polygamous, first wife | 9.6 (9.3, 9.9) | 0.55 | 27.7 (24.0, 32.0) | 0.76 | 7.0 (6.4, 7.7) | 0.04 | 52.0 (50.2, 53.8) | 0.78 |
| Polygamous, ≥2nd wife | 9.5 (9.2, 9.7) | 0.10 | 27.1 (24.2, 30.3) | 0.99 | 8.2 (7.7, 8.9) | 0.13 | 52.7 (51.3, 54.2) | 0.57 |
| Ethnicity, matrnal | 0.17 | 0.05 | 0.05 | 0.25 | ||||
| Hausa | 9.7 (9.5, 9.8) | REF | 28.0 (26.5, 29.6) | REF | 7.6 (7.3, 8.0) | REF | 52.5 (51.8, 53.2) | REF |
| Tuareg | 9.5 (9.1, 9.8) | 0.36 | 23.1 (19.6, 27.2) | 0.03 | 8.4 (7.6, 9.4) | 0.09 | 50.6 (48.5, 52.7) | 0.10 |
| Other (minority) | 9.2 (8.7, 9.7) | 0.09 | 23.8 (18.6, 30.5) | 0.21 | 8.9 (7.6, 10.4) | 0.05 | 52.4 (49.4, 55.5) | 0.95 |
| Education, maternal | 0.91 | 0.19 | <0.01 | 0.20 | ||||
| None | 9.6 (9.5, 9.8) | REF | 26.8 (25.0, 28.7) | REF | 8.0 (7.6, 8.4) | REF | 51.9 (51.0, 52.8) | REF |
| Koranic schooling | 9.6 (9.4, 9.9) | 0.87 | 26.6 (23.9, 29.6) | 0.90 | 7.9 (7.4, 8.5) | 0.76 | 52.6 (51.2, 54.0) | 0.36 |
| Primary (1–6 years) | 9.5 (9.3, 9.8) | 0.52 | 31.1 (27.2, 35.6) | 0.05 | 6.9 (6.3, 7.5) | <0.01 | 53.9 (52.1, 55.6) | 0.04 |
| Secondary (7–14 years) | 9.6 (9.2, 10.0) | 0.87 | 25.7 (20.9, 31.5) | 0.70 | 7.4 (6.5, 8.4) | 0.26 | 51.8 (49.2, 54.4) | 0.97 |
| Obstetric history | ||||||||
| Primigravida | 0.01 | <0.01 | 0.56 | 0.72 | ||||
| Yes | 9.3 (9.0, 9.6) | 34.9 (30.1, 40.4) | 8.0 (7.2, 8.8) | 52.6 (50.8, 54.5) | ||||
| No | 9.7 (9.5, 9.8) | 26.4 (25.1, 27.9) | 7.7 (7.4, 8.1) | 52.3 (51.5, 53.0) | ||||
| Attended ANC in last pregnancy | 0.63 | 0.35 | 0.01 | 0.11 | ||||
| Yes | 9.7 (9.5, 9.8) | 26.6 (25.1, 28.1) | 7.6 (7.3, 7.9) | 52.4 (51.7, 53.2) | ||||
| No | 9.8 (9.4 , 10.1) | 24.2 (20.1, 29.1) | 9.1 (8.0, 10.2) | 50.5 (48.2, 52.8) | ||||
| Result of last pregnancy, n (%) | <0.01 | <0.01 | <0.01 | 0.12 | ||||
| Miscarriage, stillbirth | 9.5 (8.9, 10.0) | 0.32 | 20.3 (15.4, 26.7) | <0.01 | 9.3 (7.8, 11.1) | <0.01 | 54.1 (50.6, 57.7) | 0.24 |
| Live birth, child deceased | 9.0 (8.7, 9.4) | <0.01 | 21.2 (17.9, 25.0) | 0.04 | 9.1 (8.2, 10.1) | 0.02 | 54.0 (51.9, 56.2) | 0.07 |
| Live birth, child living | 9.7 (9.6, 9.9) | REF | 27.3 (25.8, 28.9) | REF | 7.5 (7.3, 7.9) | REF | 52.0 (51.2, 52.7) | REF |
| Knowledge, attitudes and practices | ||||||||
| Attended ANC in current pregnancy | 0.88 | 0.15 | 0.31 | 0.19 | ||||
| Yes | 9.6 (9.5, 9.8) | 27.9 (26.3, 29.7) | 7.7 (7.3, 8.0) | 52.0 (51.2, 52.8) | ||||
| No | 9.6 (9.4, 9.9) | 25.6 (23.1, 28.3) | 8.0 (7.5, 8.5) | 53.0 (51.7, 54.3) | ||||
| IFA supplement coverage | 0.45 | 0.27 | 0.02 | 0.54 | ||||
| Yes | 9.6 (9.4, 9.8) | 27.8 (26.0, 29.8) | 7.5 (7.2, 7.9) | 52.1 (51.3, 53.0) | ||||
| No | 9.7 (9.5, 9.8) | 26.0 (23.8, 28.5) | 8.2 (7.7, 8.7) | 52.6 (51.5, 53.8) | ||||
| IFA supplement adherence | 0.82 | 0.44 | <0.01 | 0.45 | ||||
| Yes | 9.6 (9.4, 9.8) | 27.8 (25.6, 30.2) | 7.4 (7.0, 7.8) | 52.0 (51.0, 53.0) | ||||
| No | 9.6 (9.5, 9.8) | 26.6 (24.8, 28.6) | 8.1 (7.7, 8.5) | 52.5 (51.6, 53.4) | ||||
| Utilization of mosquito net | 0.02 | 0.46 | 0.29 | 0.52 | ||||
| Yes | 9.7 (9.6, 9.8) | 26.9 (25.4, 28.6) | 7.7 (7.4, 8.0) | 52.2 (51.4, 53.0) | ||||
| No | 9.4 (9.1, 9.6) | 28.3 (25.2, 31.8) | 8.0 (7.5, 8.7) | 52.7 (51.3, 54.2) | ||||
| Quantity of food consumed during pregnancy | 0.99 | 0.05 | 0.42 | 0.29 | ||||
| Increased | 9.6 (9.4, 9.9) | 0.92 | 27.1 (24.2, 30.4) | 0.23 | 7.6 (7.0, 8.1) | 0.22 | 52.7 (51.3, 54.1) | 0.20 |
| Decreased | 9.6 (9.5, 9.8) | 0.94 | 28.7 (26.7, 30.8) | 0.02 | 7.7 (7.3, 8.1) | 0.30 | 52.6 (51.7, 53.5) | 0.14 |
| No change | 9.6 (9.4, 9.8) | REF | 24.7 (22.4, 27.3) | REF | 8.0 (7.5, 8.6) | REF | 51.5 (50.2, 52.7) | REF |
| Number of meals consumed during pregnancy | 0.37 | 0.30 | 0.08 | 0.13 | ||||
| Increased | 9.8 (9.5, 10.0) | 0.20 | 27.3 (24.2, 30.9) | 0.49 | 7.3 (6.7, 7.9) | 0.02 | 53.1 (51.6, 54.6) | 0.09 |
| Decreased | 9.6 (9.4, 9.8) | 0.97 | 28.4 (26.3, 30.7) | 0.12 | 7.7 (7.3, 8.1) | 0.21 | 52.7 (51.8, 53.7) | 0.08 |
| No change | 9.6 (9.4, 9.8) | REF | 26.0 (23.8, 28.3) | REF | 8.1 (7.6, 8.5) | REF | 51.5 (50.4, 52.6) | REF |
| Adequate minimum dietary diversity—women (MDD-W) | 0.46 | 0.70 | <0.01 | 0.62 | ||||
| Yes | 9.5 (9.3, 9.8) | 27.8 (24.7, 31.3) | 7.1 (6.6, 7.7) | 52.6 (51.1, 54.2) | ||||
| No | 9.6 (9.5, 9.8) | 27.1 (25.6, 28.7) | 7.9 (7.6, 8.2) | 52.2 (51.5, 53.0) | ||||
| Consumed vitamin A rich foods in past 24 h | 0.17 | 0.59 | 0.23 | 0.92 | ||||
| Yes | 9.6 (9.5, 9.7) | 27.1 (25.6, 28.6) | 7.8 (7.5, 8.2) | 52.3 (51.6, 53.0) | ||||
| No | 9.8 (9.5, 10.1) | 28.2 (24.6, 32.4) | 7.4 (6.8, 8.1) | 52.4 (50.6, 54.1) | ||||
| Consumed animal source foods in past 24 h | 0.49 | 0.30 | 0.29 | 0.93 | ||||
| Yes | 9.7 (9.5, 9.9) | 26.3 (24.1, 28.6) | 7.6 (7.2, 8.0) | 52.3 (51.3, 53.4) | ||||
| No | 9.6 (9.4, 9.8) | 27.8 (26.0, 29.7) | 7.9 (7.5, 8.2) | 52.3 (51.4, 53.1) | ||||
| Geophagy (consumed clay) | <0.01 | <0.01 | <0.01 | 0.02 | ||||
| Yes | 9.1 (8.7, 9.4) | 17.2 (14.6, 20.4) | 10.4 (9.3, 11.6) | 50.0 (47.9, 52.1) | ||||
| No | 9.7 (9.5, 9.8) | 28.5 (27.0, 30.1) | 7.5 (7.2, 7.9) | 52.6 (51.8, 53.3) | ||||
| Nutritional and health status | ||||||||
| Malaria antigenemia (elevated HRP2) | <0.01 | <0.01 | 0.59 | 0.23 | ||||
| Yes | 9.0 (8.7, 9.3) | 33.8 (29.3, 39.0) | 8.0 (7.2, 8.7) | 51.3 (49.5, 53.1) | ||||
| No | 9.7 (9.6, 9.9) | 26.5 (25.1, 27.9) | 7.7 (7.4, 8.1) | 52.5 (51.7, 53.2) | ||||
| Variable | Hemoglobin | Ferritin, Adjusted for APP 2,3 | Soluble Transferrin Receptor 2 | Zinc, Adjusted for APP 3 | ||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| Demographic and socio-economic characteristics 4 | ||||||||
| Age (year) | 0.026 (0.0098, 0.041) | <0.01 | −0.0056 (−0.014, 0.0025) | 0.18 | −0.00074 (−0.0057, 0.0043) | 0.77 | −0.0088 (−0.11, 0.094) | 0.87 |
| Age at first pregnancy (year) | −0.0063 (−0.055, 0.043) | 0.80 | 0.010 (−0.014, 0.036) | 0.40 | 0.0082 (−0.0070, 0.024) | 0.29 | 0.25 (−0.056, 0.55) | 0.11 |
| HFIAS score | −0.0069 (−0.027, 0.013) | 0.49 | 0.0039 (−0.0058, 0.014) | 0.43 | 0.0036 (−0.0026, 0.0098) | 0.25 | 0.058 (−0.064, 0.18) | 0.35 |
| Housing quality index | 0.60 (−0.047, 1.2) | 0.07 | 0.19 (−0.13, 0.63) | 0.27 | −0.20 (−0.35, −0.027) | 0.03 | 4.50 (0.55, 8.46) | 0.03 |
| Household ownership index | 0.099 (−0.0010, 0.20) | 0.05 | 0.0020 (−0.046, 0.053) | 0.94 | −0.039 (−0.068, −0.0085) | 0.01 | 0.52 (−0.10, 1.15) | 0.10 |
| Nutritional and health status 3 | ||||||||
| Mid-upper arm circumference (cm) | 0.099 (0.060, 0.14) | <0.01 | −0.012 (−0.031, 0.0071) | 0.21 | −0.011 (−0.023, 0.0015) | 0.08 | 0.28 (0.045, 0.52) | 0.02 |
| Gestational weight gain (kg/week) | 0.22 (0.0033, 0.43) | 0.047 | −0.13 (−0.22, −0.027) | 0.01 | −0.062 (−0.13, 0.0036) | 0.06 | −0.52 (−1.9, 0.83) | 0.45 |
| Variable | RBP, Adjusted for APP (µmol/L) 2 | Vitamin B12 (pmol/L) 3 | Folate (nmol/L) 3 | |||
|---|---|---|---|---|---|---|
| Mean (95% CI) | p | Geometric Mean (95% CI) | p | Geometric Mean (95% CI) | p | |
| Current pregnancy, trimester 4 | 0.23 | 0.01 | 0.01 | |||
| First | NA | NA | NA | |||
| Second | 1.10 (1.05, 1.14) | 183.7 (175.4, 192.3) | 11.4 (10.8, 12.0) | |||
| Third | 1.07 (1.04, 1.10) | 163.6 (158.5, 168.9) | 10.1 (9.7, 10.6) | |||
| Season | 0.81 | 0.66 | 0.07 | |||
| June–September (Lean, rainy season) | 1.09 (1.01, 1.18) | 0.53 | 170.2 (155.3, 186.5) | 0.63 | 11.3 (10.2, 12.6) | 0.89 |
| October–February (Post-harvest, cool season) | 1.09 (0.99, 1.19) | 0.60 | 162.1 (145.8, 180.3) | 0.37 | 9.2 (8.2, 10.4) | 0.09 |
| March– May (Hot season) | 1.04 (0.92, 1.16) | REF | 177.9 (156.8, 201.8) | REF | 11.2 (9.7, 12.8) | REF |
| Demographic and socio-economic characteristics | ||||||
| Adolescent | 0.08 | 0.20 | 0.89 | |||
| Yes | 1.13 (1.07, 1.19) | 163.1 (152.5, 174.4) | 10.6 (9.8, 11.3) | |||
| No | 1.07 (1.04, 1.10) | 170.7 (165.6, 175.9) | 10.5 (10.1, 10.9) | |||
| Marital status | 0.02 | 0.09 | 0.48 | |||
| Monogamous | 1.09 (1.06, 1.12) | REF | 170.8 (165.5, 176.3) | REF | 10.6 (10.1, 11.0) | REF |
| Polygamous, first wife | 1.00 (0.93, 1.06) | 0.01 | 158.1 (147.5, 169.4) | 0.04 | 10.1 (9.4, 10.9) | 0.26 |
| Polygamous, ≥2nd wife | 1.08 (1.03, 1.13) | 0.61 | 172.8 (163.4, 182.8) | 0.71 | 10.4 (9.7, 11.0) | 0.51 |
| Ethnicity, maternal | 0.83 | 0.89 | 0.59 | |||
| Hausa | 1.08 (1.05, 1.11) | REF | 169.3 (164.4, 174.3) | REF | 10.5 (10.1, 11.0) | REF |
| Taureg | 1.06 (0.98, 1.13) | 0.56 | 169.3 (156.0, 183.6) | 0.99 | 10.1 (9.3, 11.1) | 0.40 |
| Other (minority) | 1.07 (0.96, 1.18) | 0.83 | 174.3 (154.8, 196.3) | 0.63 | 10.8 (9.6, 12.2) | 0.62 |
| Education, maternal | 0.08 | 0.41 | 0.27 | |||
| None | 1.08 (1.05, 1.12) | REF | 166.5 (160.9, 172.3) | REF | 10.5 (10.1, 11.0) | REF |
| Koranic schooling | 1.11 (1.06, 1.16) | 0.29 | 173.1 (164.1, 182.6) | 0.21 | 10.8 (10.2, 11.4) | 0.46 |
| Primary (1–6 years) | 1.02 (0.96, 1.08) | 0.07 | 173.3 (162.4, 184.9) | 0.27 | 10.0 (9.3, 10.7) | 0.13 |
| Secondary (7–14 years) | 1.03 (0.94, 1.12) | 0.25 | 176.8 (160.3, 195.0) | 0.25 | 10.2 (9.2, 11.2) | 0.48 |
| Obstetric history | ||||||
| Primigravida | 0.74 | 0.34 | 0.52 | |||
| Yes | 1.07 (1.00, 1.13) | 164.0 (152.3, 176.5) | 10.3 (9.5, 11.1) | |||
| No | 1.08 (1.05, 1.11) | 170.2 (165.3, 175.1) | 10.5 (10.1, 10.9) | |||
| Attended ANC in last pregnancy | 0.32 | 0.25 | 0.82 | |||
| Yes | 1.07 (1.05, 1.10) | 169.0 (164.0, 174.2) | 10.5 (10.1, 11.0) | |||
| No | 1.12 (1.03, 1.20) | 178.8 (163.2, 195.9) | 10.4 (9.5, 11.4) | |||
| Result of last pregnancy, n (%) | 0.31 | 0.28 | 0.17 | |||
| Miscarriage, stillbirth | 1.14 (1.02, 1.26) | 0.26 | 189.3 (165.2,217.1) | 0.11 | 11.2 (9.9, 12.8) | 0.35 |
| Live birth, child deceased | 1.11 (1.04, 1.19) | 0.26 | 169.7 (156.4, 184.3) | 0.94 | 9.9 (9.1, 10.8) | 0.12 |
| Live birth, child living | 1.07 (1.04, 1.10) | REF | 169.2 (164.1, 174.4) | REF | 10.6 (10.2, 11.0) | REF |
| Knowledge, attitudes and practices | ||||||
| Attended ANC in current pregnancy | 0.96 | 0.57 | 0.37 | |||
| Yes | 1.08 (1.05, 1.11) | 168.6 (163.3, 174.2) | 10.4 (10.0, 10.9) | |||
| No | 1.08 (1.03, 1.12) | 171.5 (163.1, 180.4) | 10.7 (10.1, 11.3) | |||
| IFA coverage | 0.76 | 0.05 | 0.98 | |||
| Yes | 1.08 (1.05, 1.11) | 165.9 (160.2, 171.8) | 10.5 (10.0, 11.0) | |||
| No | 1.07 (1.03, 1.11) | 175.7 (167.8, 183.9) | 10.5 (10.0, 11.1) | |||
| IFA adherence | 0.54 | 0.17 | 0.97 | |||
| Yes | 1.07 (1.03, 1.11) | 165.8 (159.2, 172.8) | 10.5 (10.0, 11.0) | |||
| No | 1.08 (1.05, 1.12) | 172.2 (166.1, 178.5) | 10.5 (10.0, 11.0) | |||
| Utilization of mosquito net | 0.59 | 0.26 | 0.76 | |||
| Yes | 1.08 (1.05, 1.11) | 170.8 (165.6, 176.1) | 10.5 (10.1, 11.0) | |||
| No | 1.06 (1.01, 1.12) | 164.7 (155.6, 174.4) | 10.4 (9.8, 11.1) | |||
| Quantity of food consumed during pregnancy | 0.89 | 0.20 | 0.18 | |||
| Increased | 1.09 (1.04, 1.14) | 0.73 | 163.5 (154.6, 173.0) | 0.07 | 11.0 (10.3, 11.7) | 0.19 |
| Decreased | 1.07 (1.04, 1.11) | 0.91 | 168.9 (162.9, 175.2) | 0.27 | 10.3 (9.9, 10.8) | 0.73 |
| No change | 1.08 (1.03, 1.12) | REF | 174.7 (166.3, 183.5) | REF | 10.5 (9.9, 11.0) | REF |
| Number of meals consumed during pregnancy | 0.05 | 0.20 | 0.59 | |||
| Increased | 1.11 (1.06, 1.17) | 0.03 | 164.3 (154.7, 174.4) | 0.11 | 10.7 (10.1, 11.4) | 0.63 |
| Decreased | 1.09 (1.06, 1.13) | 0.04 | 167.2 (160.8, 173.8) | 0.15 | 10.4 (9.9, 10.9) | 0.56 |
| No change | 1.04 (1.00, 1.08) | REF | 174.1 (166.7, 181.8) | REF | 10.5 (10.0, 11.1) | REF |
| Adequate minimum dietary diversity—women (MDD-W) | 0.27 | 0.38 | 0.62 | |||
| Yes | 1.05 (1.00, 1.11) | 173.5 (163.7, 183.9) | 10.4 (9.7, 11.0) | |||
| No | 1.08 (1.05, 1.11) | 168.6 (163.6, 173.6) | 10.5 (10.1, 11.0) | |||
| Consumed vitamin A rich foods in past 24 h | 0.52 | 0.19 | 0.54 | |||
| Yes | 1.08 (1.05, 1.11) | 168.4 (163.5, 173.3) | 10.5 (10.1, 11.0) | |||
| No | 1.06 (1.00, 1.12) | 176.7 (165.1, 189.1) | 10.3 (9.6, 11.1) | |||
| Consumed animal source foods in past 24 h | 0.91 | 0.01 | 0.32 | |||
| Yes | 1.08 (1.04, 1.12) | 177.1 (169.7, 184.8) | 10.3 (9.8, 10.9) | |||
| No | 1.08 (1.04, 1.11) | 165.4 (160.0, 170.9) | 10.6 (10.1, 11.1) | |||
| Consumed clay | 0.10 | 0.01 | 0.64 | |||
| Yes | 1.02 (0.94, 1.09) | 153.1 (140.7, 166.6) | 10.3 (9.5, 11.2) | |||
| No | 1.08 (1.05, 1.11) | 171.2 (166.3, 176.1) | 10.5 (10.1, 10.9) | |||
| Nutritional and health status | ||||||
| Malaria antigenemia (elevated HRP2) | 0.01 | 0.77 | 0.64 | |||
| Yes | 1.00 (0.93, 1.06) | 167.9 (156.4, 180.2) | 10.3 (9.6, 11.1) | |||
| No | 1.09 (1.06, 1.12) | 169.7 (164.9, 174.7) | 10.5 (10.1, 10.9) | |||
| Variable | RBP, Adjusted for APP 2 | Vitamin B12 3 | Folate 3 | |||
|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| Demographic and socio-economic characteristics 4 | ||||||
| Age (year) | −0.0017 (−0.0052, 0.0019) | 0.36 | 0.00035 (−0.0036, 0.0043) | 0.86 | 0.0030 (−0.00075, 0.0020) | 0.12 |
| Age at first pregnancy (year) | −0.0059 (−0.017, 0.0048) | 0.28 | 0.014 (0.0022, 0.026) | 0.02 | −0.0050 (−0.016, 0.0064) | 0.39 |
| HFIAS score | 0.0049 (0.00065, 0.0092) | 0.02 | −0.0043 (−0.0090, 0.00035) | 0.07 | −0.0028 (−0.0075, 0.0020) | 0.25 |
| Housing quality index | 0.045 (−0.096, 0.19) | 0.53 | 0.28 (0.10, 0.49) | 0.01 | 0.0025 (−0.14, 0.17) | 0.98 |
| Household ownership index | 0.0096 (−0.012, 0.032) | 0.39 | 0.020 (−0.0047, 0.044) | 0.11 | −0.0076 (−0.031, 0.016) | 0.53 |
| Nutritional and health status 3 | ||||||
| Mid-upper arm circumference (cm) | 0.012 (0.0032, 0.020) | 0.01 | −0.0051 (−0.014, 0.0043) | 0.29 | 0.012 (0.0023, 0.021) | 0.01 |
| Gestational weight gain (kg/week) | −0.039 (−0.086, 0.0084) | 0.11 | −0.036 (−0.085, 0.015) | 0.16 | 0.028 (−0.023, 0.081) | 0.29 |
| Malaria Antigenemia (HRP2 Elevated) | No Malaria Antigenemia (HRP2 Non-Elevated) | p for Interaction | |||
|---|---|---|---|---|---|
| Primigravida | Multigravida | Primigravida | Multigravida | ||
| Participants 2, n | 31 | 66 | 56 | 616 | |
| Hemoglobin (g/dL) 3 | 8.5 (8.0, 9.0) a | 9.3 (8.9, 9.6) b | 9.7 (9.3, 10.1) b,c | 9.7 (9.6, 9.9) c | 0.028 |
| Ferritin, adjusted for APP (µg/L) 4 | 45.4 (35.6, 58.0) a | 29.4 (24.8, 34.9) b | 30.3 (25.2, 36.3) b | 26.2 (24.8, 27.6) b | 0.104 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wessells, K.R.; Ouédraogo, C.T.; Young, R.R.; Faye, M.T.; Brito, A.; Hess, S.Y. Micronutrient Status among Pregnant Women in Zinder, Niger and Risk Factors Associated with Deficiency. Nutrients 2017, 9, 430. https://doi.org/10.3390/nu9050430
Wessells KR, Ouédraogo CT, Young RR, Faye MT, Brito A, Hess SY. Micronutrient Status among Pregnant Women in Zinder, Niger and Risk Factors Associated with Deficiency. Nutrients. 2017; 9(5):430. https://doi.org/10.3390/nu9050430
Chicago/Turabian StyleWessells, K. Ryan, Césaire T. Ouédraogo, Rebecca R. Young, M. Thierno Faye, Alex Brito, and Sonja Y. Hess. 2017. "Micronutrient Status among Pregnant Women in Zinder, Niger and Risk Factors Associated with Deficiency" Nutrients 9, no. 5: 430. https://doi.org/10.3390/nu9050430
APA StyleWessells, K. R., Ouédraogo, C. T., Young, R. R., Faye, M. T., Brito, A., & Hess, S. Y. (2017). Micronutrient Status among Pregnant Women in Zinder, Niger and Risk Factors Associated with Deficiency. Nutrients, 9(5), 430. https://doi.org/10.3390/nu9050430