Food Consumption and Nutrient Intake by Children Aged 10 to 48 Months Attending Day Care in The Netherlands

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Intake Assessment
2.3. Data Processing
2.4. Data Analysis
3. Results
3.1. Study Population
3.2. Nutrient Intake
- Energy: Mean daily intake, both for boys (5.5 MJ) and girls (5.3 MJ), was higher than the requirement established by the HCN (5 MJ for boys, 4.5 MJ for girls between 1 and 3 years old [16] and much higher than the intake considered adequate according to EFSA (3.3–4.9 MJ for boys, 3.0–4.6 MJ for girls [19]).
- Protein: Median usual intake (45 g, 14 energy percent) was approximately three times higher than the Adequate Intake of 5 energy percent [16] or the Population Reference Intake of 11–13 g [19]. Among the children below 1 year, 26% exceeded the TUIL of 15 energy percent for this age. If, among the children that used exclusively cow’s milk, liquid cow’s milk would be substituted by formula, median usual protein intake would decrease from 14.2 to 12.3 energy percent.
- Fat: Intake was relatively low (29 energy percent). The mean usual intake was within the recommended range (25–40 energy percent) according the HCN recommendation [16], although 11% of the population had an intake below 25 energy percent. The mean intake was lower than the more recent EFSA recommendation (35–40 energy percent for children under 4 years [19]). Less than 5% of the children achieved a usual fat intake of 35 energy percent. No children below the age of 1 year achieved a usual fat intake of 40 energy percent, as recommended by the HCN and EFSA.
- Dietary fiber: With a mean of 12.7 g or 2.3 g/MJ, the usual intake of the children of 1 year and older was below the intake considered as adequate by the HCN (2.8 g/MJ [17]) and not achieved by 92% of them. However, new reference intakes for young children established by EFSA are lower (10 g [19]). These were achieved by the large majority of the children.
- n-3 fatty acids from fish, i.e., eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA): the mean daily intake of DHA by children below 2 years and of EPA + DHA by children above 2 years was far below the intake considered adequate by the HCN or EFSA.
- Iron: The median usual iron intake of 6.0 mg was lower than the Adequate Intake of 8 mg/day [18] and also lower than the Population Reference Intake of 7 mg/day established by EFSA [22]. This implies that iron intake was possibly inadequate. Children receiving formula, most of them in combination with cow’s milk, had a median usual intake of 6.8 mg iron, whereas exclusive cow’s milk users had a median usual intake of 5.6 mg. If, in the latter group, liquid cow’s milk products would be replaced by formula, median usual iron intake would increase to 8.5 mg.
- Sodium: The percentage of children with a usual sodium intake of more than 1200 mg, i.e., the upper limit established by the NNC for young children above 1 year, increased with age from 47% to 81%, whereas the usual intake of all children below 1 year exceeded the upper limit of 400 mg [23].
- Zinc: The median usual intake of 5.9 mg was adequate. However, 17% of the children exceeded the TUIL of 7 mg/day.
- Retinol: 30% of the children exceeded the TUIL of 800 mg retinol. The percentage increased from 27% in the youngest age group to 33% in the oldest age group. Liverwurst spread, popular among young children, appeared to be responsible for the excess intake.
3.3. Food Consumption
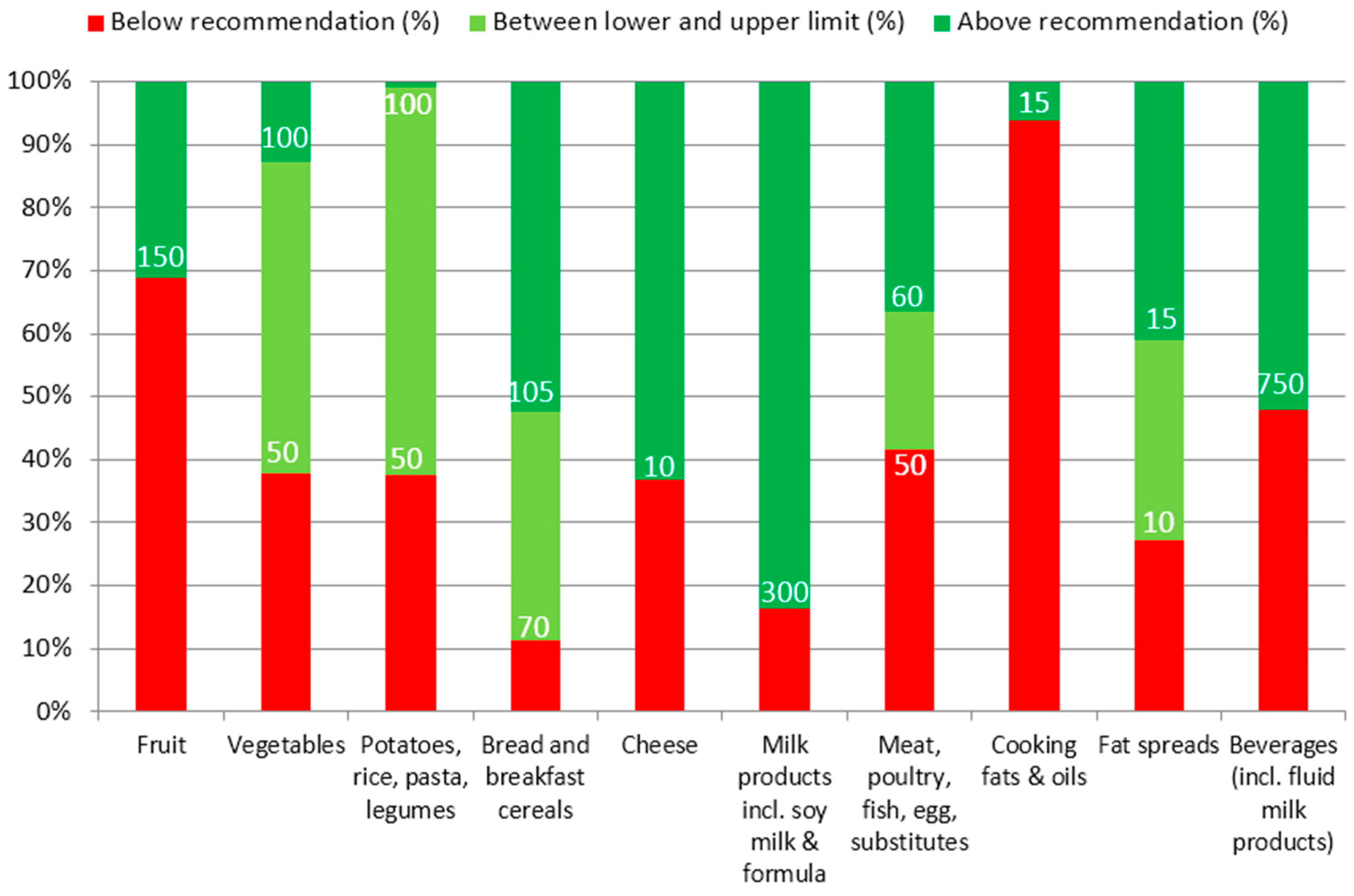
3.4. Consumption According to Food-Based Dietary Guidelines
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [PubMed]
- Florence, M.D.; Asbridge, M.; Veugelers, P.J. Diet quality and academic performance. J. Sch. Health 2008, 78, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Lanting, C.I.; de Vroome, E.M.; Elias, S.G.; van den Brandt, P.A.; van Leeuwen, F.E.; Kampman, E.; Kiemeney, L.A.; Peeters, P.H.; de Vries, E.; Bausch-Goldbohm, R.A. Contribution of lifestyle factors to cancer: Secondary analysis of Dutch data over 2010 and a projection for 2020. Ned. Tijdschr. Geneeskd. 2014, 159, A8085. [Google Scholar] [PubMed]
- Singer, M.R.; Moore, L.L.; Garrahie, E.J.; Ellison, R.C. The tracking of nutrient intake in young children: The Framingham children’s study. Am. J. Public Health 1995, 85, 1673–1677. [Google Scholar] [CrossRef] [PubMed]
- Statistics Netherlands. Minder Kinderen naar Kinderdagverblijven (Less Children in Day Care), 2014. Available online: http://www.cbs.nl/nl-NL/menu/themas/dossiers/jongeren/publicaties/artikelen/archief/2014/2014-4024-wm.htm (accessed on 20 May 2015).
- Gubbels, J.S.; Raaijmakers, L.G.M.; Gerards, S.M.P.L.; Kremers, S.P.J. Dietary intake by Dutch 1- to 3-year-old children at childcare and at home. Nutrients 2014, 6, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Gerards, S.M.; Kremers, S.P. Use of food practices by childcare staff and the association with dietary intake of children at childcare. Nutrients 2015, 7, 2161–2175. [Google Scholar] [CrossRef] [PubMed]
- WebArchitecten vof. FoodFigures. Available online: http://www.foodfigures.nl/ (accessed on 2 May 2015).
- SAS. Version 8.2; SAS Institute Inc.: Cary, NC, USA, 1999–2001. [Google Scholar]
- SAS. Version 9.3; SAS Institute Inc.: Cary, NC, USA, 1999–2001. [Google Scholar]
- Kistemaker, C.; Bouman, M. Voedselconsumptiepeiling Met SAS. de Ontwikkeling van een Geautomatiseerd Systeem voor de Verwerking van Voedingsenquetes. Deel 2: Beschrijving Functioneel en Systeem Ontwerp (Vertrouwelijk). Rapportnummer V98.799; TNO Voeding: Zeist, The Netherlands, 1999. [Google Scholar]
- NEVO-Online Versie 2013/4.0. Available online: http://nevo-online.rivm.nl/ (accessed on 20 May 2015).
- Dekkers, A.L.M.; Verkaik-Kloosterman, J.; Rossum, C.T.M.; Ocke, M.C. SPADE, a new statistical program to estimate habitual dietary intake from multiple food sources and dietary supplements. J. Nutr. 2014, 144, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific opinion on principles for deriving and applying dietary reference values. EFSA J. 2010, 8, 1458. [Google Scholar]
- Health Council of The Netherlands. Dietary Reference Intakes: Energy, Proteins, Fats and Digestible Carbohydrates; Health Council of The Netherlands: The Hague, The Netherlands, 2001. [Google Scholar]
- Health Council of The Netherlands. Guideline for Dietary Fibre Intake; Health Council of The Netherlands: The Hague, The Netherlands, 2006. [Google Scholar]
- Voedingscentrum (Netherlands Nutrition Centre). Aanbevelingen voor Vitamine, Mineralen en Spoorelementen: Factsheet (Recommendations for Vitamins, Minerals, and Trace Elements), 2014. Available online: http://www.voedingscentrum.nl/nl/pers/factsheets.aspx (accessed on 20 May 2015).
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar]
- Gezond eten met de Schijf van Vijf. Available online: http://www.voedingscentrum.nl/nl/schijf-van-vijf/schijf.aspx (accessed on 20 May 2015).
- Voedingscentrum (Netherlands Nutrition Centre). Richtlijnen Voedselkeuze, 1 Maart 2011, Update 12 April 2011 (Guidelines for Food Choice, 12 April 2011); Voedingscentrum: Den Haag, The Netherlands, 2011. [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on dietary reference values for iron. EFSA J. 2015, 13, 4254. [Google Scholar]
- Encyclopedie. Available online: http://www.voedingscentrum.nl/encyclopedie/zout.aspx (accessed on 20 May 2015).
- Ocké, M.C.; van Rossum, C.T.M.; Fransen, H.P.; Buurma, E.M.; de Boer, E.J.; Brants, H.A.M.; Niekerk, E.M.; van der Laan, J.D.; Drijvers, J.J.M.M.; Ghameshlou, Z. Dutch National Food Consumption Survey—Young Children 2005/2006; RIVM: Bilthoven, The Netherlands, 2008. [Google Scholar]
- Portegijs, W.; Cloïn, M.; Merens, A. Krimp in de Kinderopvang; Sociaal en Cultureel Planbureau: The Hague, The Netherlands, 2014. [Google Scholar]
- Lozoff, B.; Jimenez, E.; Smith, J.B. Double burden of iron deficiency in infancy and low socioeconomic status: A longitudinal analysis of cognitive test scores to age 19 years. Arch. Pediatr. Adolesc. Med. 2006, 160, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Qubty, W.; Renaud, D.L. Cognitive impairment associated with low ferritin responsive to iron supplementation. Pediatr. Neurol. 2014, 51, 831–833. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary reference intakes: Vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef]
- Uijterschout, L.; Vloemans, J.; Vos, R.; Teunisse, P.P.; Hudig, C.; Bubbers, S.; Verbruggen, S.; Veldhorst, M.; de Leeuw, T.; van Goudoever, J.B.; et al. Prevalence and risk factors of iron deficiency in healthy young children in the southwestern Netherlands. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Grote, V.; Closa-Monasterolo, R.; Escribano, J.; Langehendries, J.; Sain, E.; Giovannini, M.; Verduci, E.; Gruzfeld, S.; Socha, P.; et al. Lower protein content in infant formula reduces BMI and obesity risk at school age: Follow-up of a randomized trial. Am. J. Clin. Nutr. 2014, 99, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, A.; Börnhorst, C.; Barba, G.; Siani, A.; Huybrechts, I.; Tognon, G.; Eiben, G.; Moreno, L.A.; Fernández Alvira, J.M.; Loit, H.M.; et al. Associations between energy intake, daily food intake and energy density of foods and BMI z-score in 2–9-year-old european children. Eur. J. Nutr. 2014, 53, 673–681. [Google Scholar] [CrossRef] [PubMed]
- De Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N. Engl. J. Med. 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | Boy | 759 | 49.7 |
| Girl | 683 | 44.8 | |
| Missing | 84 | 5.5 | |
| Age | 10–11 months old | 31 | 2.0 |
| 1 year old | 411 | 26.9 | |
| 2 years old | 497 | 32.6 | |
| 3 years old | 410 | 26.9 | |
| Missing | 177 | 11.6 | |
| Zip-code based socioeconomic status of childcare centers | Low | 381 | 25.0 |
| Medium | 848 | 55.6 | |
| High | 218 | 14.3 | |
| Missing | 79 | 5.2 | |
| Number of days per week that the child attended childcare center | 2 days | 939 | 61.5 |
| 3 days | 348 | 22.8 | |
| 4 days | 68 | 4.5 | |
| 5 days | 16 | 1.1 | |
| Missing | 155 | 10.2 | |
| Hot meal at childcare center | Yes | 315 | 20.6 |
| No | 1189 | 77.9 | |
| Missing | 22 | 1.4 |
| Total Group (n = 1526) 1 | 10–11 Months (n = 31) | 1 Year (n = 411) | 2 Years (n = 497) | 3 Years (n = 410) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nutrient | Unit | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Energy | kJ | 5383 | 958 | 4241 | 795 | 4954 | 822 | 5424 | 872 | 5841 | 923 |
| Protein | g | 45 | 9 | 32 | 8 | 43 | 9 | 45 | 8 | 48 | 10 |
| en% | 14.1 | 2.2 | 12.6 | 2.2 | 14.6 | 2.4 | 13.9 | 2.0 | 13.9 | 2.1 | |
| Carbohydrates | g | 174 | 34 | 136 | 27 | 159 | 30 | 177 | 32 | 189 | 33 |
| en% | 54.4 | 5.1 | 54.2 | 5.9 | 54 | 5.3 | 54.8 | 5.0 | 54.5 | 4.8 | |
| Mono- and disaccharides | g | 100 | 25 | 79 | 18 | 91 | 24 | 102 | 24 | 108 | 26 |
| en% | 31.2 | 5.7 | 31.4 | 5.5 | 30.7 | 6.1 | 31.7 | 5.3 | 31.1 | 5.7 | |
| Polysaccharides | g | 75 | 16 | 58 | 15 | 69 | 14 | 75 | 15 | 81 | 16 |
| en% | 23.4 | 3.4 | 23.1 | 3.6 | 23.6 | 3.6 | 23.3 | 3.1 | 23.4 | 3.3 | |
| Fat | g | 42 | 11 | 34 | 10 | 38 | 10 | 42 | 10 | 45 | 11 |
| en% | 29.1 | 4.6 | 30.4 | 5.5 | 28.7 | 4.8 | 28.9 | 4.5 | 29.3 | 4.3 | |
| Saturated fatty acids | g | 14.8 | 3.8 | 12.6 | 4.7 | 13.5 | 3.4 | 14.8 | 3.7 | 16.1 | 3.8 |
| en% | 10.4 | 1.8 | 11.2 | 2.8 | 10.3 | 1.9 | 10.3 | 1.8 | 10.4 | 1.7 | |
| Monounsaturated fatty acids | g | 14.4 | 4.5 | 11.7 | 4.3 | 12.9 | 4.2 | 14.4 | 4.5 | 15.8 | 4.4 |
| en% | 10.0 | 2.3 | 10.4 | 3.0 | 9.8 | 2.4 | 9.9 | 2.3 | 10.2 | 2.2 | |
| Polyunsaturated fatty acids (PUFA) | g | 8.6 | 3.2 | 6.7 | 2.3 | 8.0 | 3.1 | 8.6 | 3.0 | 9.4 | 3.4 |
| en% | 6.0 | 1.8 | 5.9 | 1.5 | 6.1 | 1.9 | 5.9 | 1.7 | 6.0 | 1.7 | |
| n-3 PUFA | g | 1.0 | 0.4 | 0.9 | 0.3 | 1.0 | 0.3 | 1.0 | 0.4 | 1.1 | 0.4 |
| en% | 0.7 | 0.2 | 0.8 | 0.2 | 0.7 | 0.2 | 0.7 | 0.2 | 0.7 | 0.2 | |
| ALA (C18:3 (n-3) cis) | g | 1.0 | 0.3 | 0.8 | 0.3 | 0.9 | 0.3 | 1.0 | 0.3 | 1.0 | 0.4 |
| en% | 0.7 | 0.2 | 0.7 | 0.2 | 0.7 | 0.2 | 0.7 | 0.2 | 0.7 | 0.2 | |
| EPA (C20:5 (n-3) cis) | g | 0.01 | 0.03 | 0.02 | 0.03 | 0.02 | 0.03 | 0.01 | 0.02 | 0.01 | 0.03 |
| en% | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| DHA (C22:6 (n-3) cis) | g | 0.02 | 0.04 | 0.02 | 0.04 | 0.02 | 0.05 | 0.02 | 0.04 | 0.02 | 0.04 |
| en% | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| n-6 PUFA | g | 7.3 | 2.8 | 5.4 | 2.0 | 6.8 | 2.7 | 7.3 | 2.6 | 8.0 | 3.0 |
| en% | 5.1 | 1.6 | 4.8 | 1.4 | 5.1 | 1.7 | 5.0 | 1.5 | 5.1 | 1.5 | |
| Linoleic acid (C18:2 (n-6) cis) | g | 7.3 | 2.8 | 5.4 | 2.0 | 6.7 | 2.7 | 7.2 | 2.6 | 7.9 | 3.0 |
| en% | 5.0 | 1.6 | 4.8 | 1.4 | 5.1 | 1.7 | 5.0 | 1.5 | 5.1 | 1.5 | |
| Trans-unsaturated fatty acids | g | 0.4 | 0.2 | 0.3 | 0.2 | 0.4 | 0.2 | 0.4 | 0.2 | 0.5 | 0.2 |
| en% | 0.3 | 0.1 | 0.2 | 0.1 | 0.3 | 0.1 | 0.3 | 0.1 | 0.3 | 0.1 | |
| Cholesterol | mg | 76.1 | 38.0 | 45.9 | 45.9 | 69.2 | 37.2 | 77.4 | 38.6 | 84.4 | 38.2 |
| Dietary fiber | g | 12.6 | 2.7 | 12.4 | 2.6 | 12.4 | 2.7 | 12.5 | 2.6 | 13.1 | 2.7 |
| g/MJ | 2.4 | 0.4 | 3.0 | 0.5 | 2.5 | 0.5 | 2.3 | 0.4 | 2.3 | 0.4 | |
| Water | g | 1045 | 248 | 885 | 219 | 988 | 240 | 1047 | 231 | 1133 | 245 |
| Sodium | mg | 1273 | 359 | 790 | 266 | 1117 | 301 | 1317 | 340 | 1420 | 341 |
| Potassium | mg | 1923 | 405 | 1435 | 420 | 1864 | 391 | 1934 | 377 | 2010 | 402 |
| Phosphorus | mg | 943 | 199 | 715 | 190 | 907 | 189 | 941 | 186 | 997 | 206 |
| Magnesium | mg | 181 | 38 | 134 | 29 | 172 | 36 | 181 | 34 | 194 | 40 |
| Iron | mg | 6.3 | 2.0 | 8.4 | 2.5 | 6.5 | 2.4 | 6.0 | 1.7 | 6.1 | 1.7 |
| Calcium | mg | 735 | 186 | 684 | 200 | 734 | 177 | 720 | 177 | 745 | 202 |
| Copper | mg | 0.61 | 0.15 | 0.59 | 0.13 | 0.58 | 0.14 | 0.60 | 0.14 | 0.66 | 0.15 |
| Selenium | μg | 22 | 6 | 21 | 6 | 21 | 6 | 22 | 6 | 24 | 6 |
| Zinc | mg | 6.0 | 1.4 | 6.0 | 1.4 | 6.0 | 1.4 | 5.9 | 1.4 | 6.1 | 1.5 |
| Iodine | μg | 120 | 30 | 118 | 22 | 117 | 31 | 119 | 30 | 124 | 31 |
| Vitamin A (RAE) | μg | 846 | 568 | 753 | 448 | 746 | 483 | 834 | 568 | 902 | 626 |
| Retinol | μg | 731 | 560 | 648 | 434 | 636 | 479 | 712 | 558 | 787 | 618 |
| Thiamin (Vitamin B1) | mg | 0.58 | 0.17 | 0.60 | 0.20 | 0.58 | 0.17 | 0.57 | 0.17 | 0.57 | 0.17 |
| Riboflavin (Vitamin B2) | mg | 1.13 | 0.29 | 0.97 | 0.24 | 1.09 | 0.27 | 1.12 | 0.29 | 1.17 | 0.31 |
| Niacin | mg | 7.7 | 2.5 | 6.4 | 2.6 | 7.4 | 2.4 | 7.7 | 2.5 | 8.1 | 2.6 |
| Vitamin B6 | mg | 0.80 | 0.27 | 0.69 | 0.28 | 0.79 | 0.25 | 0.81 | 0.28 | 0.82 | 0.28 |
| Folate (DFE) | μg | 156 | 47 | 177 | 49 | 162 | 47 | 154 | 50 | 154 | 46 |
| Vitamin B12 | μg | 2.95 | 1.06 | 1.95 | 0.79 | 2.73 | 0.90 | 2.94 | 1.00 | 3.18 | 1.19 |
| Vitamin C | mg | 93 | 35 | 105 | 29 | 94 | 35 | 92 | 35 | 92 | 35 |
| Vitamin D | μg | 3.7 | 2.8 | 8.4 | 3.7 | 4.7 | 3.5 | 3.2 | 2.1 | 2.8 | 1.8 |
| Vitamin E | mg | 6.8 | 2.8 | 8.0 | 2.9 | 6.8 | 3.0 | 6.6 | 2.7 | 7.0 | 2.7 |
| Total Group (n = 1526) 1 | 10–11 Months (n = 31) | 1 Year (n = 411) | 2 Years (n = 497) | 3 Years (n = 410) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Food Group | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Potatoes | 29 | 27 | 25 | 25 | 31 | 28 | 28 | 27 | 28 | 26 |
| Vegetables | 58 | 39 | 48 | 45 | 60 | 41 | 58 | 39 | 61 | 38 |
| Fruit | 128 | 59 | 129 | 66 | 127 | 58 | 129 | 59 | 130 | 61 |
| Legumes | 1 | 7 | 1 | 4 | 2 | 9 | 1 | 6 | 1 | 6 |
| Bread | 100 | 35 | 57 | 29 | 86 | 33 | 103 | 33 | 114 | 33 |
| Cereals (including rice and pasta) | 29 | 29 | 21 | 26 | 30 | 30 | 28 | 28 | 30 | 28 |
| Cakes and biscuits | 13 | 12 | 6 | 8 | 11 | 10 | 14 | 12 | 16 | 13 |
| Nuts, seeds, savory snacks | 1 | 5 | 0 | 0 | 1 | 3 | 1 | 5 | 2 | 6 |
| Milk and milk products | 358 | 158 | 176 | 217 | 333 | 162 | 363 | 143 | 383 | 147 |
| Follow-on and young children’s formula | 63 | 135 | 411 | 226 | 111 | 162 | 35 | 87 | 15 | 61 |
| Cheese | 14 | 11 | 14 | 10 | 15 | 11 | 14 | 11 | 15 | 12 |
| Eggs | 3 | 8 | 1 | 4 | 2 | 7 | 3 | 8 | 3 | 8 |
| Fish | 5 | 12 | 2 | 7 | 5 | 12 | 5 | 12 | 6 | 13 |
| Meat, meat products, poultry | 44 | 25 | 24 | 23 | 40 | 24 | 44 | 22 | 49 | 26 |
| Soy and vegetarian products | 8 | 49 | 0 | 2 | 8 | 54 | 8 | 47 | 10 | 55 |
| Savory spreads | 4 | 6 | 0 | 0 | 3 | 6 | 4 | 6 | 4 | 7 |
| Mixed dishes | 20 | 45 | 52 | 78 | 28 | 53 | 15 | 39 | 14 | 35 |
| Soups | 10 | 33 | 0 | 1 | 6 | 23 | 12 | 37 | 13 | 39 |
| Sugar, confectionary, sweet spreads | 18 | 13 | 6 | 7 | 13 | 10 | 20 | 12 | 23 | 14 |
| Fat spreads, oils, savory sauces | 24 | 11 | 11 | 8 | 20 | 10 | 24 | 11 | 27 | 12 |
| Non-alcoholic beverages (excluding milk products) | 427 | 222 | 182 | 145 | 367 | 204 | 446 | 209 | 508 | 220 |
| Mean | Energy | Protein | MDS | PS | Fat | SFA | PUFA | Water | Dietary Fiber | Sodium | Vitamin C | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Basic Foods | g/day | % | % | % | % | % | % | % | % | % | % | % |
| Fruit | 123 | 6 | 2 | 13 | 3 | 1 | 1 | 2 | 10 | 16 | 0 | 42 |
| Vegetables | 58 | 1 | 2 | 1 | 1 | 1 | 0 | 1 | 5 | 10 | 1 | 11 |
| Potatoes, rice, pasta, legumes | 23 | 2 | 1 | 0 | 5 | 0 | 0 | 1 | 2 | 4 | 0 | 2 |
| Potatoes, rice, pasta, legumes (exception) | 30 | 3 | 3 | 0 | 10 | 2 | 1 | 2 | 2 | 3 | 0 | 1 |
| Bread and breakfast cereals | 98 | 19 | 22 | 3 | 54 | 4 | 3 | 7 | 3 | 42 | 34 | 2 |
| Cheese | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 |
| Cheese (exception) | 13 | 3 | 5 | 0 | 0 | 8 | 13 | 1 | 1 | 0 | 10 | 0 |
| Milk products including soy milk and formula | 333 | 13 | 23 | 16 | 1 | 13 | 21 | 4 | 26 | 4 | 10 | 11 |
| Milk products incl. soy milk (exception) | 90 | 6 | 7 | 9 | 2 | 5 | 8 | 2 | 7 | 2 | 4 | 1 |
| Meat, poultry, fish, egg, substitutes | 18 | 2 | 9 | 0 | 0 | 2 | 2 | 2 | 1 | 0 | 4 | 0 |
| Meat, poultry, fish, egg, substitutes (exception) | 35 | 8 | 15 | 0 | 2 | 18 | 18 | 12 | 2 | 1 | 13 | 6 |
| Fats, oils | 18 | 8 | 0 | 0 | 0 | 26 | 15 | 47 | 1 | 0 | 2 | 0 |
| Fats, oils (exception) | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 |
| Beverages, excluding milk products | 165 | 0 | 0 | 0 | 0 | 0 | 0 | 16 | 0 | 0 | 1 | |
| Beverages, excluding milk products (exception) | 267 | 12 | 1 | 39 | 0 | 0 | 0 | 0 | 22 | 3 | 4 | 21 |
| Mixed dishes | 12 | 1 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 2 | 1 | 0 |
| Mixed dishes (exception) | 7 | 1 | 1 | 0 | 2 | 1 | 2 | 1 | 0 | 1 | 2 | 0 |
| Non-Basic Foods | ||||||||||||
| Sugar, sweet spreads | 18 | 5 | 1 | 12 | 1 | 4 | 4 | 2 | 0 | 3 | 0 | 0 |
| Cakes and biscuits | 13 | 4 | 2 | 4 | 7 | 3 | 4 | 2 | 0 | 3 | 3 | 0 |
| Confectionary | 3 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
| Nuts, seeds, savory snacks | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 |
| Sauces | 5 | 1 | 0 | 0 | 0 | 2 | 1 | 4 | 0 | 0 | 2 | 0 |
| Savory spreads | 4 | 2 | 2 | 0 | 0 | 5 | 2 | 5 | 0 | 2 | 1 | 0 |
| Soups | 9 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 | 1 |
| Miscellaneous 2 | 14 | 3 | 2 | 1 | 8 | 1 | 1 | 1 | 1 | 4 | 4 | 0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldbohm, R.A.; Rubingh, C.M.; Lanting, C.I.; Joosten, K.F.M. Food Consumption and Nutrient Intake by Children Aged 10 to 48 Months Attending Day Care in The Netherlands. Nutrients 2016, 8, 428. https://doi.org/10.3390/nu8070428
Goldbohm RA, Rubingh CM, Lanting CI, Joosten KFM. Food Consumption and Nutrient Intake by Children Aged 10 to 48 Months Attending Day Care in The Netherlands. Nutrients. 2016; 8(7):428. https://doi.org/10.3390/nu8070428
Chicago/Turabian StyleGoldbohm, R. Alexandra, Carina M. Rubingh, Caren I. Lanting, and Koen F. M. Joosten. 2016. "Food Consumption and Nutrient Intake by Children Aged 10 to 48 Months Attending Day Care in The Netherlands" Nutrients 8, no. 7: 428. https://doi.org/10.3390/nu8070428
APA StyleGoldbohm, R. A., Rubingh, C. M., Lanting, C. I., & Joosten, K. F. M. (2016). Food Consumption and Nutrient Intake by Children Aged 10 to 48 Months Attending Day Care in The Netherlands. Nutrients, 8(7), 428. https://doi.org/10.3390/nu8070428