Improvements in Cycling but Not Handcycling 10 km Time Trial Performance in Habitual Caffeine Users

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Preliminary Trials
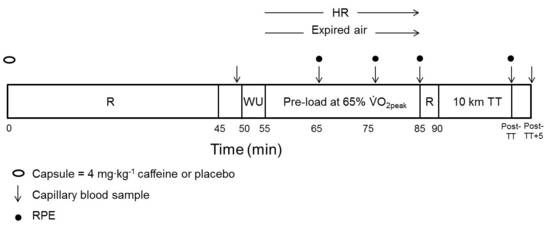
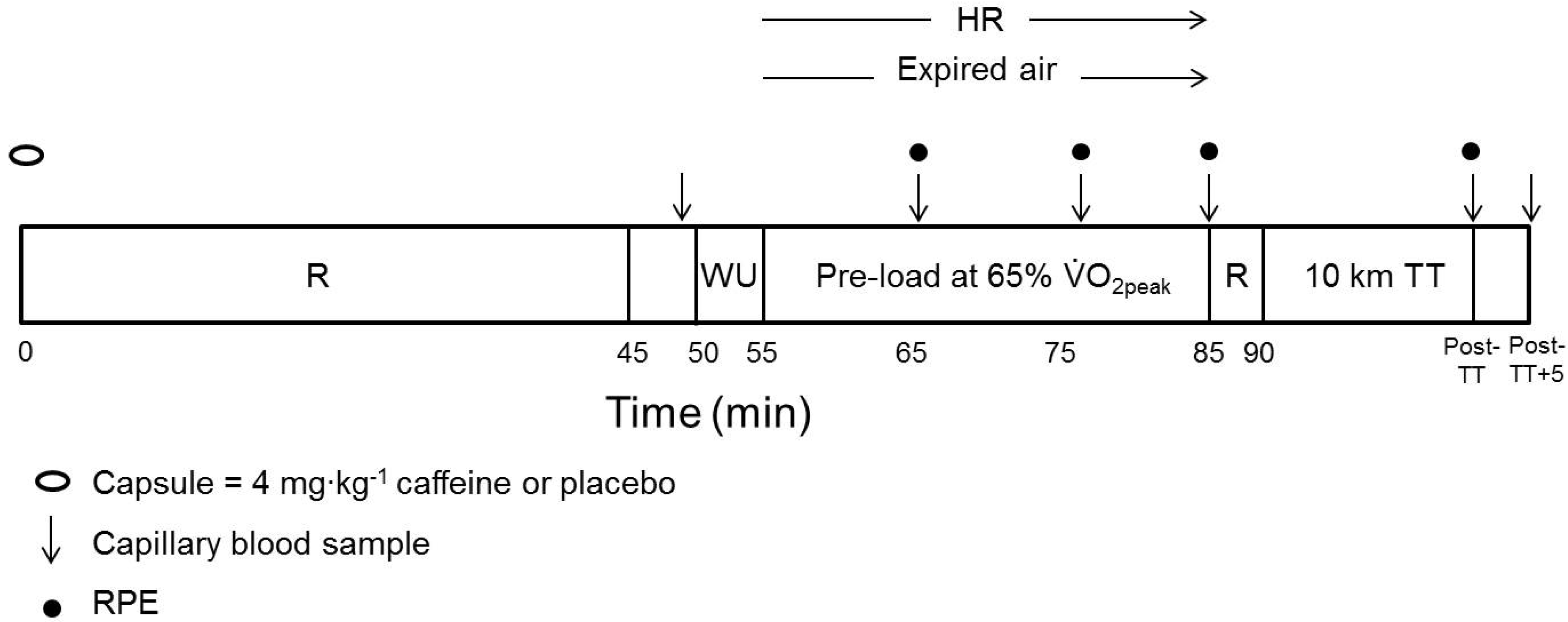
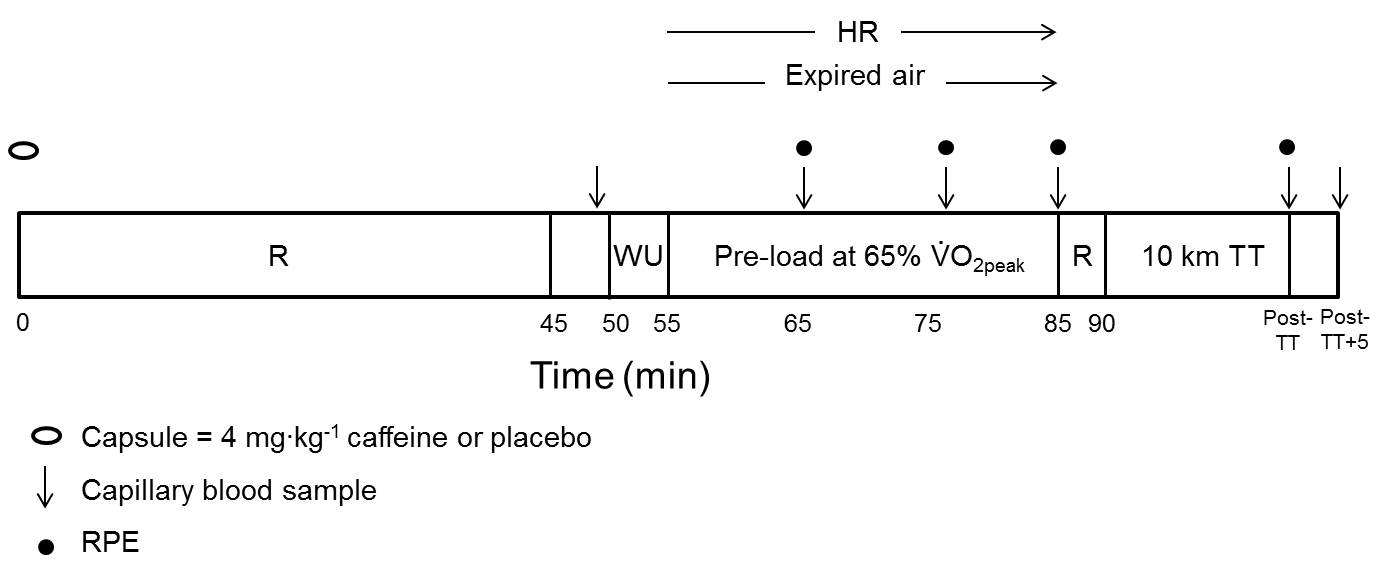
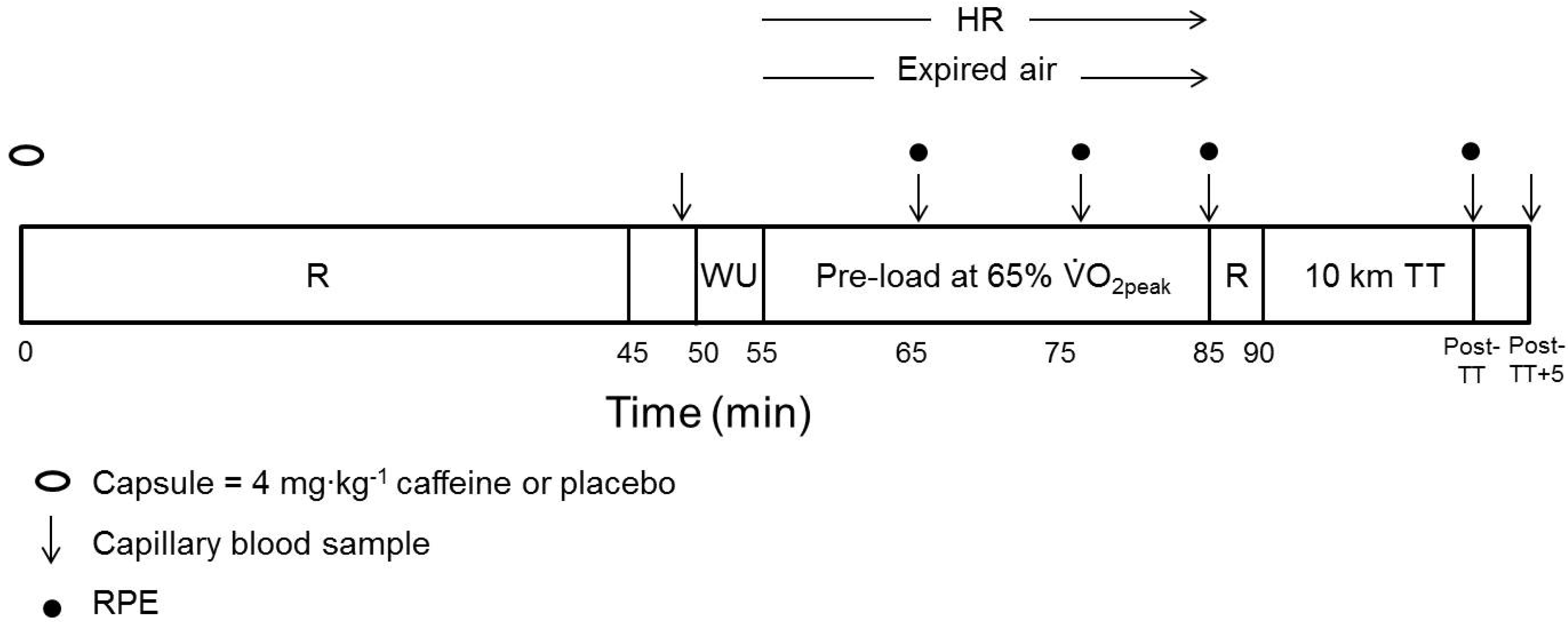
2.4. Experimental Trials
2.5 Statistical Analyses
3. Results
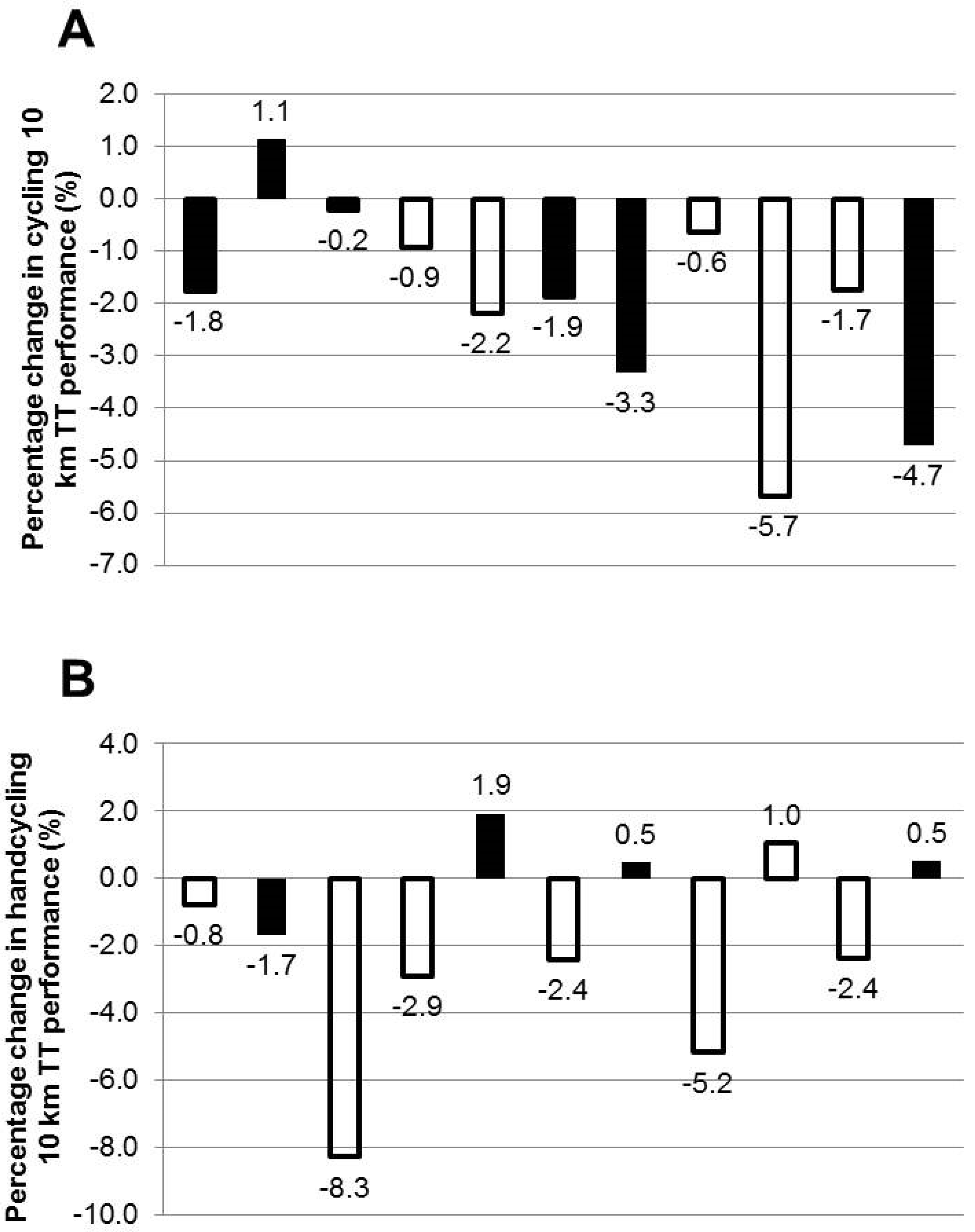
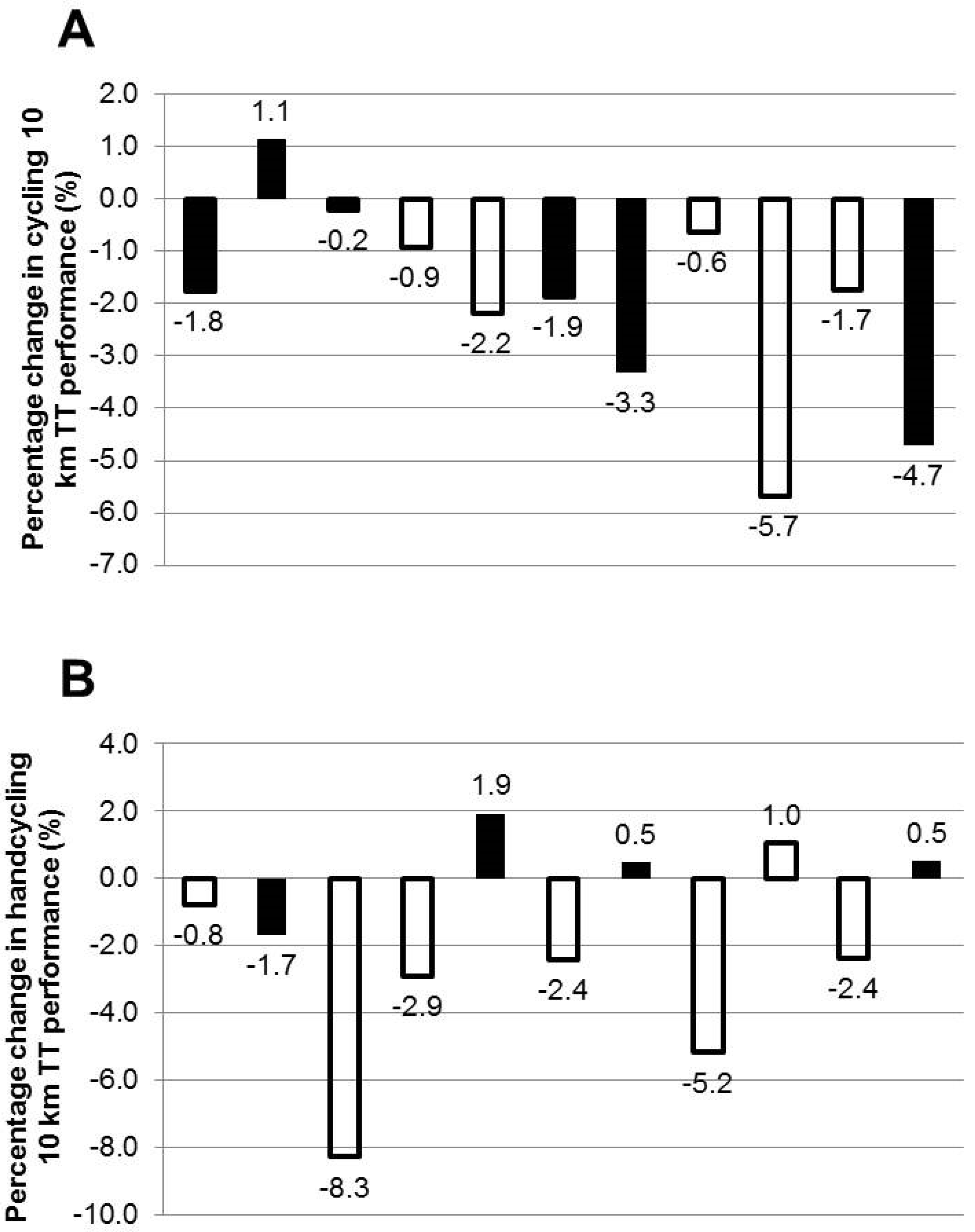
3.1. Performance Tests
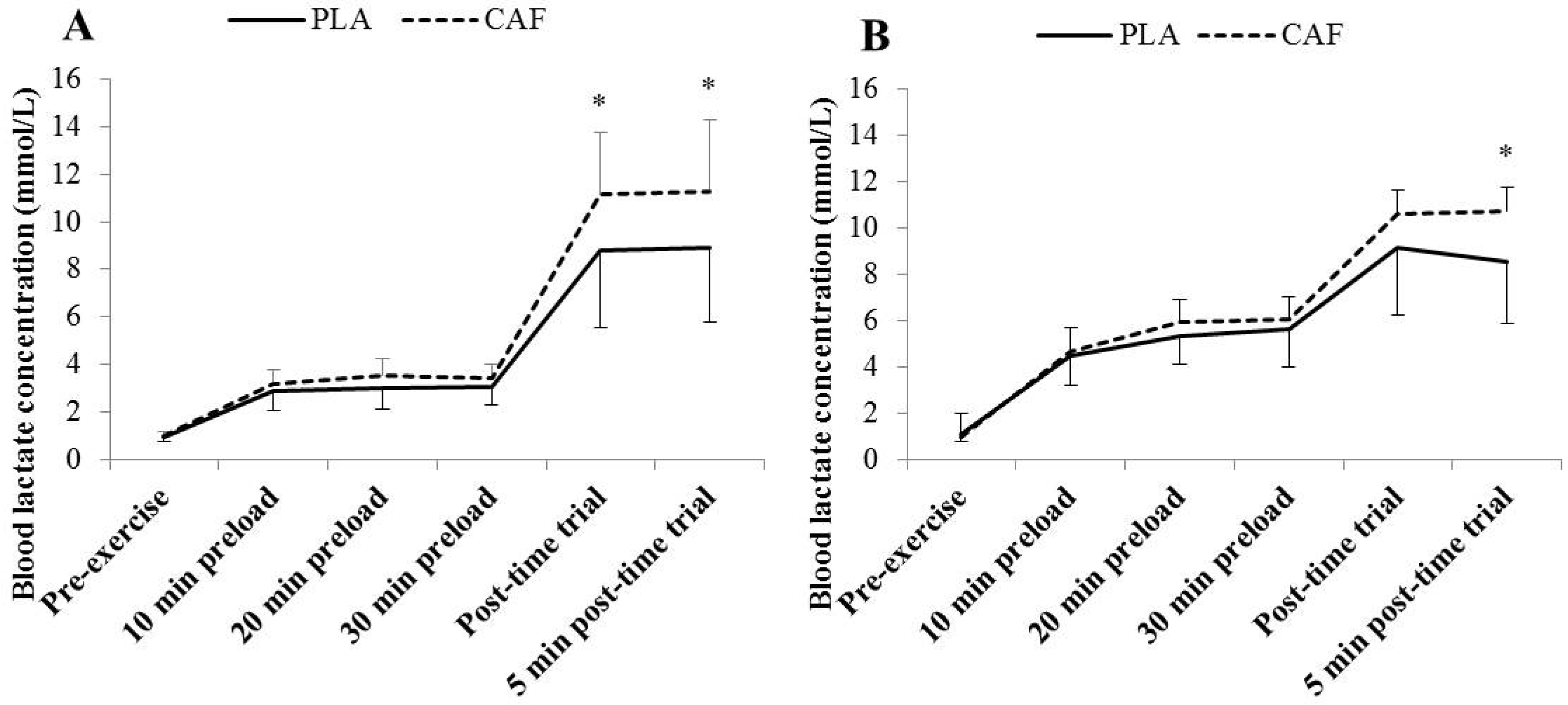
3.2. Blood Lactate Concentration
3.3. Subjective Feelings
4. Discussion
4.1. Preload
4.2. Time Trial Performance
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AB | Able-bodied |
| (Bla) | Blood lactate concentration |
| CAF | Caffeine |
| CNS | Central nervous system |
| HR | Heart rate |
| LBE | Lower-body exercise |
| PO | Power output |
| PLA | Placebo |
| RPE | Rating of perceived exertion |
| RPEC | Central rating of perceived exertion |
| RPEO | Overall rating of perceived exertion |
| RPEP | Peripheral rating of perceived exertion |
| SD | Standard deviation |
| TT | Time trial |
| UBE | Upper-body exercise |
| Oxygen uptake | |
| peak | Peak oxygen uptake |
References
- Astorino, T.A.; Cottrell, T.; Lozano, A.T.; Aburto-Pratt, K.; Duhon, J. Effect of caffeine on RPE and perceptions of pain, arousal, and pleasure/displeasure during a cycling time trial in endurance trained and active men. Physiol. Behav. 2012, 106, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Santos Rde, A.; Kiss, M.A.; Silva-Cavalcante, M.D.; Bertuzzi, R.; Bishop, D.J.; Lima-Silva, A.E. Caffeine alters anaerobic distribution and pacing during a 4000-m cycling time trial. PLoS ONE 2013, 8, e75399. [Google Scholar] [CrossRef] [PubMed]
- Braun, H.; Koehler, K.; Geyer, H.; Kleinert, J.; Mester, J.; Schänzer, W. Dietary supplement use among elite young German athletes. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 97–109. [Google Scholar] [PubMed]
- Erdman, K.A.; Fung, T.S.; Reimer, R.A. Influence of performance level on dietary supplementation in elite Canadian athletes. Med. Sci. Sports Exerc. 2006, 38, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Graham-Paulson, T.S.; Perret, C.; Smith, B.; Crosland, J.; Goosey-Tolfrey, V.L. Nutritional supplement habits of athletes with an impairment and their sources of information. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, D.R. Cardiovascular, respiratory, and metabolic responses to upper body exercise. Med. Sci. Sports Exerc. 1989, 21, 121–125. [Google Scholar] [CrossRef]
- Davis, J.M.; Zhao, Z.; Stock, H.S.; Mehl, K.A.; Buggy, J.; Hand, G.A. Central nervous system effects of caffeine and adenosine on fatigue. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 284, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Fredholm, B.B.; Bättig, K.; Holmen, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. J. Pharmacol. Exp. Ther. 1999, 51, 83–133. [Google Scholar]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on rating of perceived exertion during and after exercise: A meta-analysis. Scand. J. Med. Sci. Sports 2005, 15, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Smit, H.J.; Rogers, P.J. Effects of low doses of caffeine on cognitive performance, mood, and thirst in low, moderate and higher caffeine users. Psychopharmacology 2000, 152, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Cureton, K.J.; Warren, G.L.; Millard-Stafford, M.L.; Wingo, J.E.; Trilk, J.; Buyckx, M. Caffeinated sports drink: Ergogenic effects and possible mechanisms. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 35–55. [Google Scholar] [PubMed]
- Stadheim, H.K.; Kvamme, B.; Olsen, R. Caffeine increases performance in cross-country double-poling time trial exercise. Med. Sci. Sports Exerc. 2013, 45, 2175–2183. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; O’Connor, P.J.; Tubandt, L.; Puetz, T.; Ely, M.R. Effect of caffeine on leg muscle pain during cycling exercise among females. Med. Sci. Sports Exerc. 2006, 38, 598–604. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Motl, R.W.; Broglio, S.P.; Ely, M.R. Dose-dependent effect of caffeine on reducing leg muscle pain during cycling exercise is unrelated to systolic blood pressure. Pain 2004, 109, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Park, N.D.; Maresca, R.S.; Mckibans, K.I.; Millard-Stafford, M.L. Effect of caffeine ingestion on muscular strength and endurance: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef] [PubMed]
- Black, C.D.; Waddell, D.E.; Gonglach, A.R. Caffeine’s ergogenic effects on cycling: Neuromuscular and perceptual factors. Med. Sci. Sports Exerc. 2015, 47, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, M.; Juel, C.; Bro-Rasmussen, T.; Mygind, E.; Schibye, B.; Rasmussen, B.; Saltin, B. Limb skeletal muscle adaptation in athletes after training at altitude. J. Appl. Physiol. 1990, 68, 496–502. [Google Scholar] [PubMed]
- Mygind, E. Fibre characteritics and enzyme levels of arm and leg muscles in elite cross-country skiers. Scand. J. Med. Sci. Sports 1995, 5, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Cerretelli, P.; Pendergast, D.P.; Paganelli, W.C.; Rennie, D.W. Effects of specific muscle training on on-response and early blood lactate. J. Appl. Physiol. 1979, 47, 761–769. [Google Scholar]
- Gollnick, P.D.; Armstrong, R.B.; Saubert, C.W.; Piehl, K.; Saltin, B. Enzyme activity and fiber composition in skeletal muscle of untrained and trained men. J. App. Physiol. 1972, 33, 312–319. [Google Scholar]
- Aedma, M.; Timpmann, S.; Ööpik, V. Effect of caffeine on upper body anaerobic performance in wrestlers in simulated competition day conditions. Int. J. Sport. Nutr. Exerc. Metab. 2013, 23, 601–609. [Google Scholar] [PubMed]
- Drust, B.; Waterhouse, J.; Atkinson, G.; Edwards, B.; Reilly, T. Circadian rhythms in sports performance-an update. Chronobiol. Int. 2005, 22, 21–44. [Google Scholar] [CrossRef] [PubMed]
- Skinner, T.L.; Jenkins, D.G.; Coombes, J.S.; Taafe, D.R.; Leveritt, M.D. Dose response of caffeine on 2000-m rowing performance. Med. Sci. Sports Exerc. 2010, 42, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Spendiff, O.; Campbell, I.G. The effect of glucose ingestion on endurance upper-body exercise and performance. Int. J. Sports Med. 2002, 23, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Cottrell, T.; Lozano, A.T.; Aburto-Pratt, K.; Duhon, J. Increases in cycling performance in response to caffeine ingestion are repeatable. Nutr. Res. 2012, 32, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics Publishers: Champaign, IL, USA, 1998. [Google Scholar]
- McNaughton, L.R.; Lovell, R.J.; Siegler, J.; Midgley, A.W.; Moore, L.; Bentley, D.J. The effects of caffeine ingestion on time trial cycling performance. Int. J. Sports Physiol. Perf. 2008, 3, 157–163. [Google Scholar]
- Bell, D.G.; McLellan, T.M. Effect of repeated caffeine ingestion on repeated exhaustive exercise endurance. Med. Sci. Sports Exerc. 2003, 35, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Greer, F.; Friars, D.; Graham, T.E. Comparison of caffeine and theophylline ingestion: exercise metabolism and endurance. J. Appl. Physiol. 2000, 89, 1837–1844. [Google Scholar] [PubMed]
- Ganio, M.S.; Klau, J.F.; Casa, D.J.; Armstrong, L.E.; Maresh, C.M. Effect of caffeine on sport-specific endurance performance: a systematic review. J. Strength Cond. Res. 2009, 23, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Graham, T.E. Caffeine and exercise: Metabolism, endurance and performance. Sports Med. 2001, 31, 785–807. [Google Scholar] [CrossRef] [PubMed]
- Skinner, T.L.; Jenkins, D.G.; Leverett, M.D.; McGorm, A.; Bolam, K.A.; Coombes, J.S.; Taafe, D.R. Factors influencing serum caffeine concentrations following caffeine ingestion. J. Sci. Med. Sport 2014, 17, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Perret, C. Elite-adapted wheelchair sports performance: A systematic review. Disabil. Rehabil. 2015, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.P.; Wells, C.L.; Manore, M.M.; Philip, S.A.; Martin, N. Differences in epinephrine and substrate responses between arm and leg exercise. Med. Sci. Sports Exerc. 1990, 22, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Mitsumoto, H.; DeBoer, G.E.; Bunge, G.; Andrish, J.T.; Tetzlaff, J.E.; Cruse, P. Fiber-type specific caffeine sensitivities in normal human skinned muscle fibers. Anesthesiology 1990, 72, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Price, M.J.; Campbell, I.G. Determination of peak oxygen uptake during upper body exercise. Ergonomics 1997, 40, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.; Pandolf, K. Upper body exercise: physiology and training application for human presence in space. SAE Tech. Paper 1991. [Google Scholar] [CrossRef]
- Collomp, K.; Ahmaidi, S.; Chatard, J.C.; Audran, M.; Préfaut, C. Benefits of caffeine ingestion on sprint performance in trained and untrained swimmers. Eur. J. Appl. Physiol. 1992, 64, 377–380. [Google Scholar] [CrossRef]
- Sewell, D.A.; McGregor, R.A. Evaluation of a cycling time trial protocol in recreationally active humans. Eur. J. Appl. Physiol. 2008, 102, 615–621. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preload 10 min | Preload 20 min | Preload 30 min | Post-Time Trial | ||
|---|---|---|---|---|---|
| Overall RPE | C PLA | 13 (12, 13) | 13 (13, 14) † | 14 (13, 14) †,‡ | 19 (17, 20) †,‡,# |
| C CAF | 12 (11, 13) * | 13 (12, 14) †,* | 13 (12, 14) †,* | 19 (18, 20) †,‡,# | |
| HC PLA | 13 (12, 14) | 14 (12, 15) † | 14 (13, 16) †,‡ | 19 (18, 20) †,‡,# | |
| HC CAF | 12 (11, 13) * | 13 (12, 14) †,* | 14 (12, 15) † | 19 (18, 20) †,‡,# | |
| Central RPE | C PLA | 12 (11, 13) | 12 (11, 13) † | 13 (11, 14) †,‡ | 18 (17, 20) †,‡,# |
| C CAF | 12 (11, 13) | 13 (12, 14) † | 13 (12, 14)*,†,‡ | 19 (18, 20) †,‡,# | |
| HC PLA | 12 (11, 13) | 12 (11, 13) † | 13 (12, 14) †,‡ | 17 (16, 18) †,‡,# | |
| HC CAF | 11 (11, 12) | 13 (11, 13) † | 13 (11, 14) † | 17 (17, 19) †,‡,# | |
| Peripheral RPE | C PLA | 13 (12, 13) | 13 (13, 15) † | 14 (13, 16) †,‡ | 19 (18, 20) †,‡,# |
| C CAF | 13 (11, 13) | 13 (12, 14) *,† | 14 (13, 15) †,‡ | 19 (17, 20) †,‡,# | |
| HC PLA | 14 (13, 15) | 15 (13, 16) † | 15 (13, 16) †,‡ | 19 (19, 20) †,‡,# | |
| HC CAF | 13 (11, 14) | 14 (12, 15) | 15 (12, 16) *,† | 19 (18, 20) †,‡,# |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graham-Paulson, T.; Perret, C.; Goosey-Tolfrey, V. Improvements in Cycling but Not Handcycling 10 km Time Trial Performance in Habitual Caffeine Users. Nutrients 2016, 8, 393. https://doi.org/10.3390/nu8070393
Graham-Paulson T, Perret C, Goosey-Tolfrey V. Improvements in Cycling but Not Handcycling 10 km Time Trial Performance in Habitual Caffeine Users. Nutrients. 2016; 8(7):393. https://doi.org/10.3390/nu8070393
Chicago/Turabian StyleGraham-Paulson, Terri, Claudio Perret, and Victoria Goosey-Tolfrey. 2016. "Improvements in Cycling but Not Handcycling 10 km Time Trial Performance in Habitual Caffeine Users" Nutrients 8, no. 7: 393. https://doi.org/10.3390/nu8070393
APA StyleGraham-Paulson, T., Perret, C., & Goosey-Tolfrey, V. (2016). Improvements in Cycling but Not Handcycling 10 km Time Trial Performance in Habitual Caffeine Users. Nutrients, 8(7), 393. https://doi.org/10.3390/nu8070393