Consumption of the Soluble Dietary Fibre Complex PolyGlycopleX® Reduces Glycaemia and Increases Satiety of a Standard Meal Postprandially

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Health Benefits of Dietary Fibre
1.2. Satiety and Soluble Fibre
1.3. Glycaemia and Soluble Fibre
1.4. PGX and Wheat Dextrin
2. Experimental Section
2.1. Subjects
2.2. Study Design
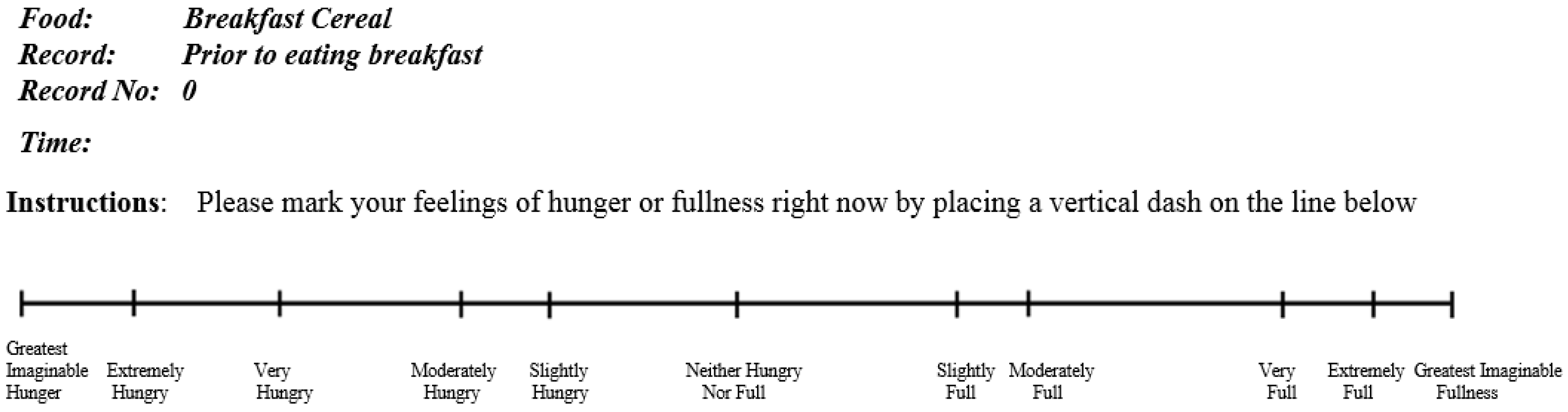
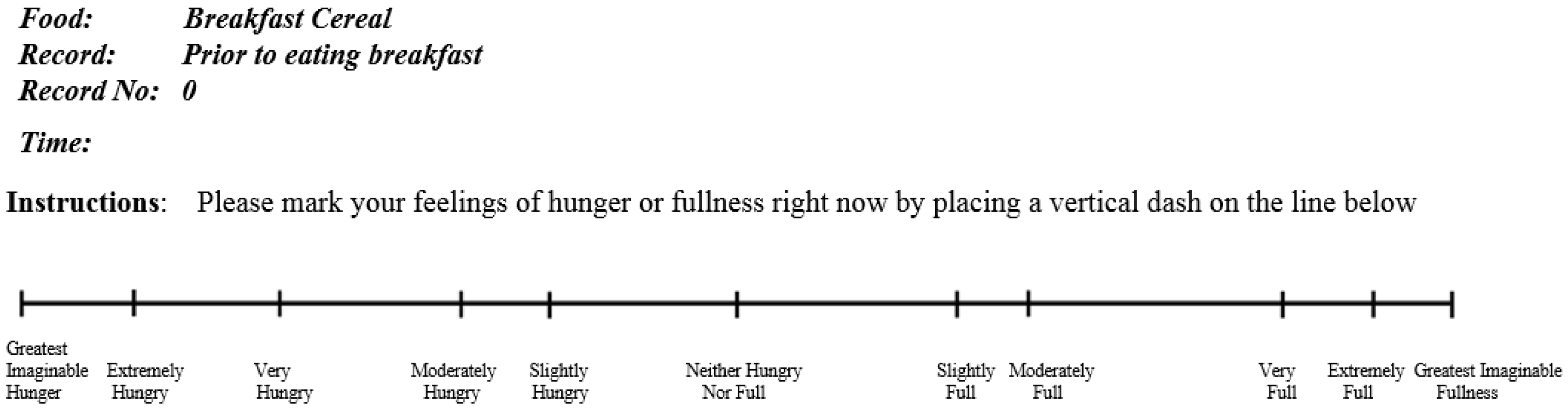
2.3. Satiety Measurement
2.4. Capillary Blood Glucose Measurement
2.5. Viscosity of PGX
2.6. Statistical Analysis
3. Results
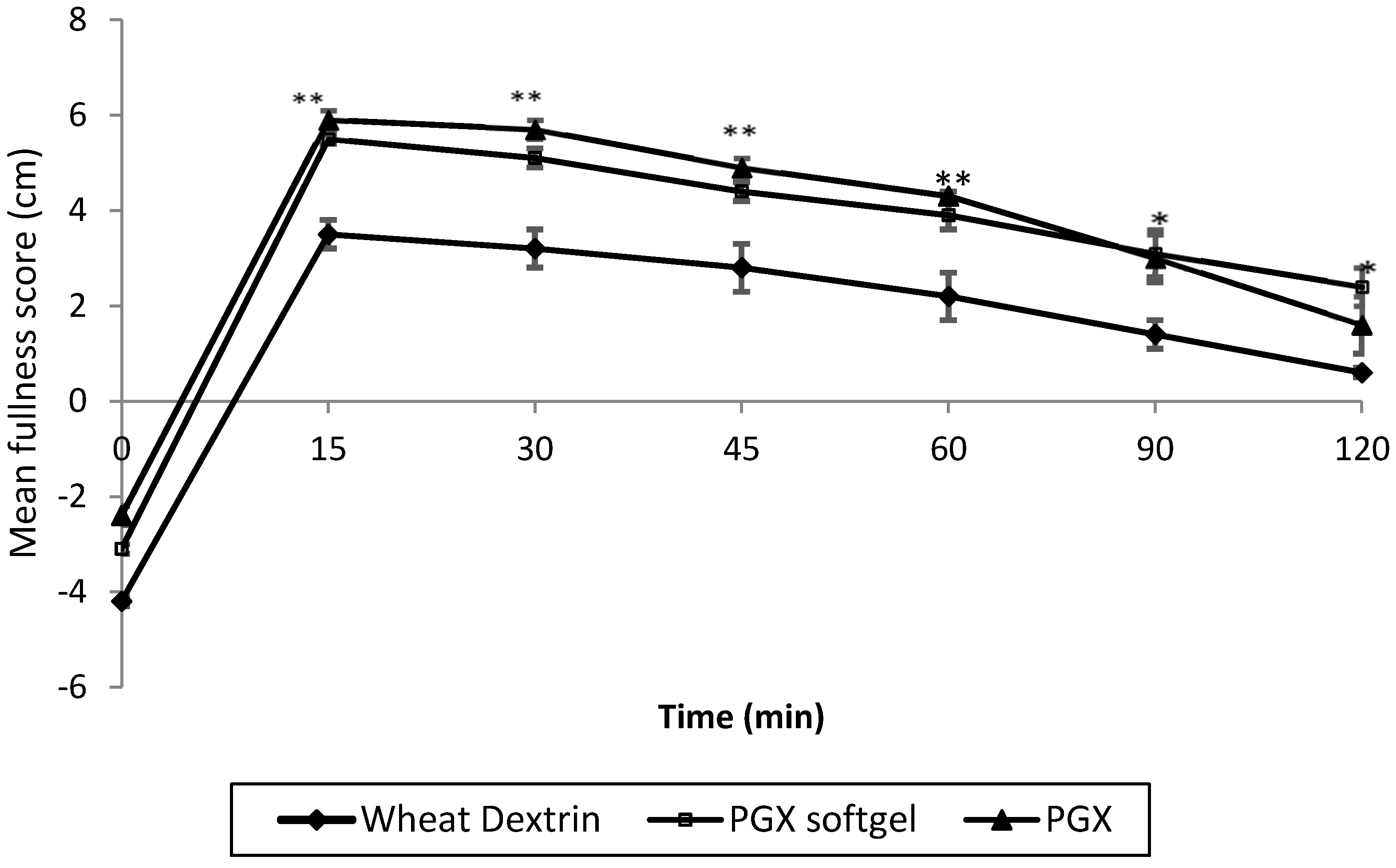
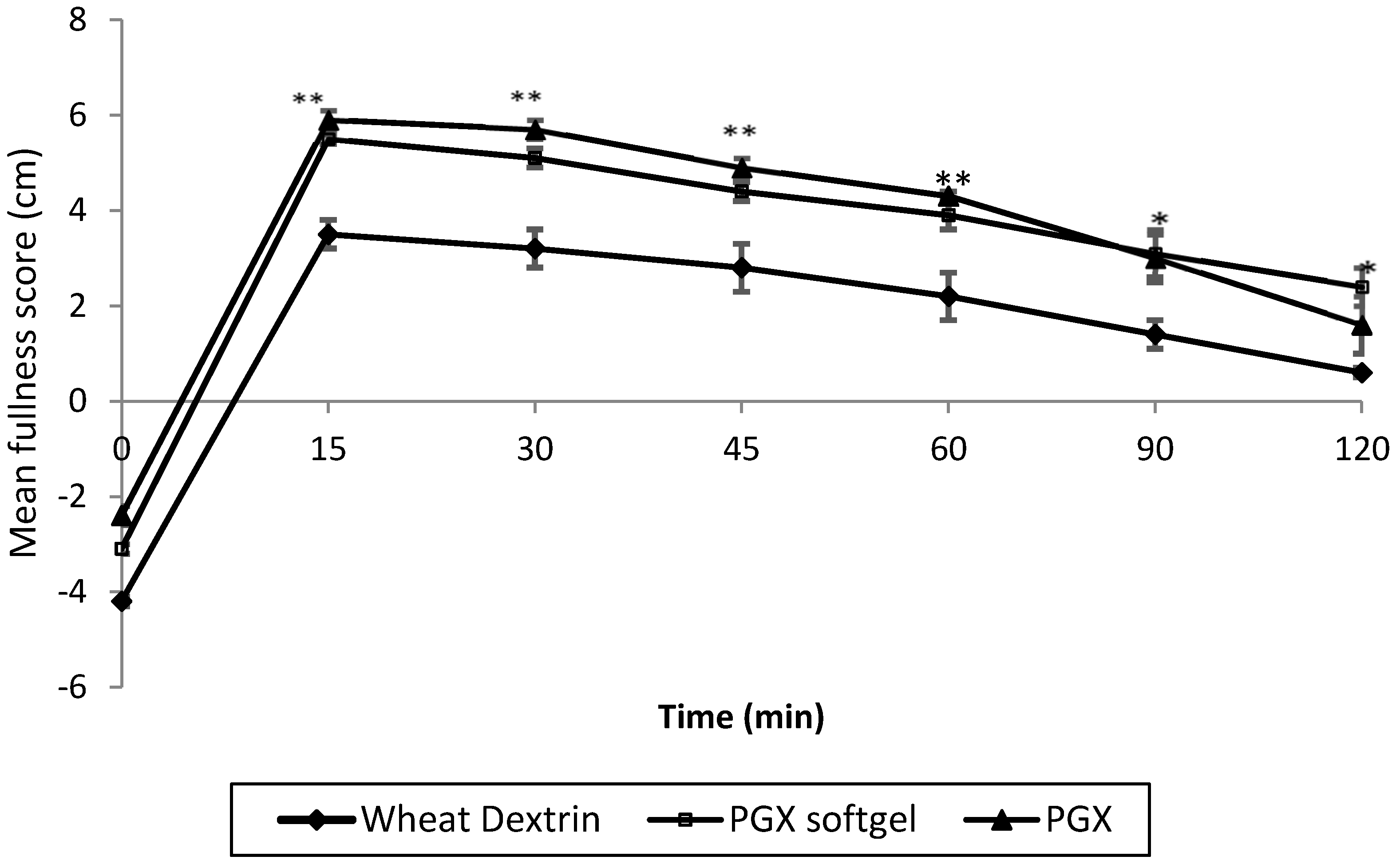
3.1. Satiety
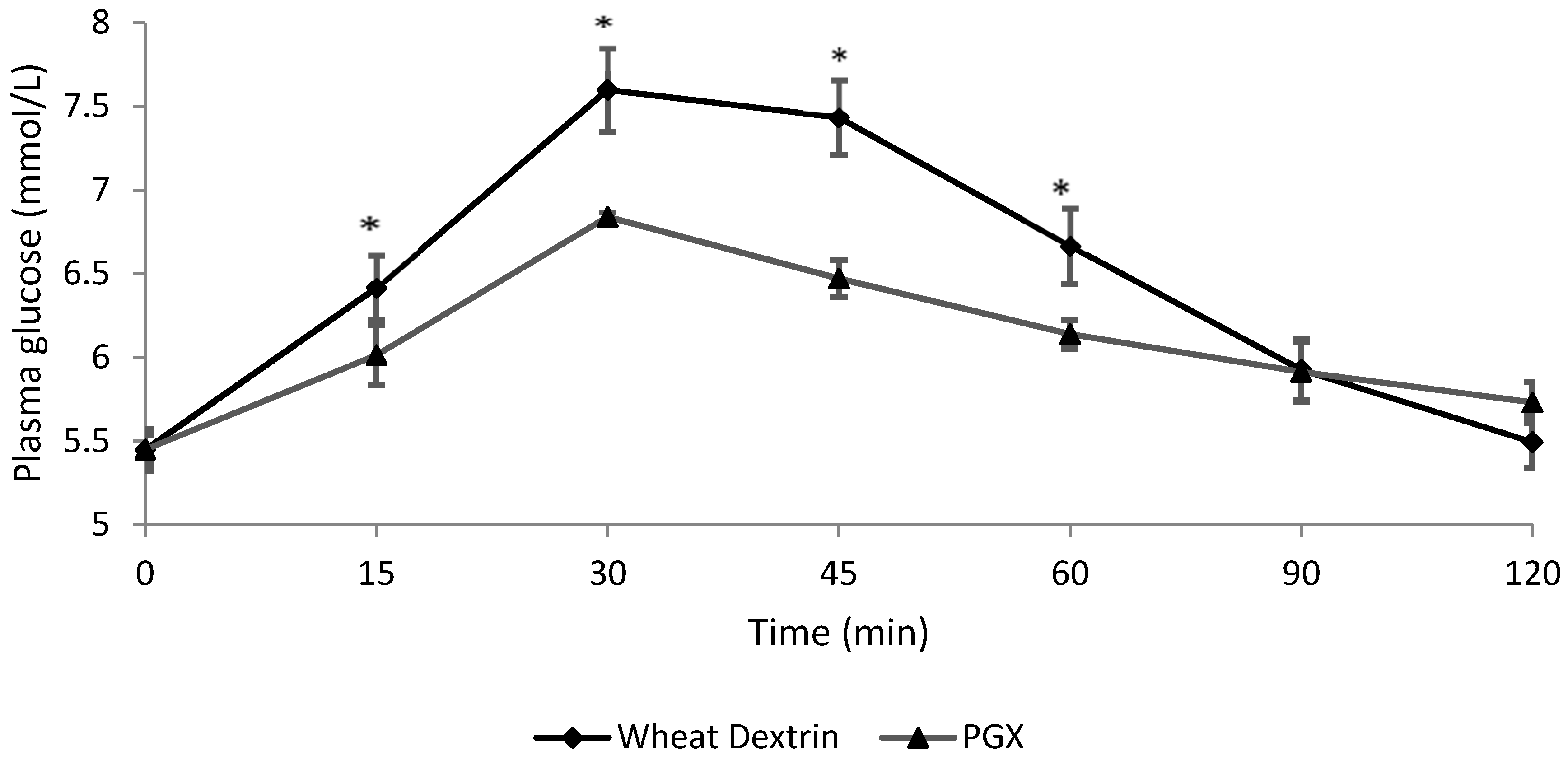
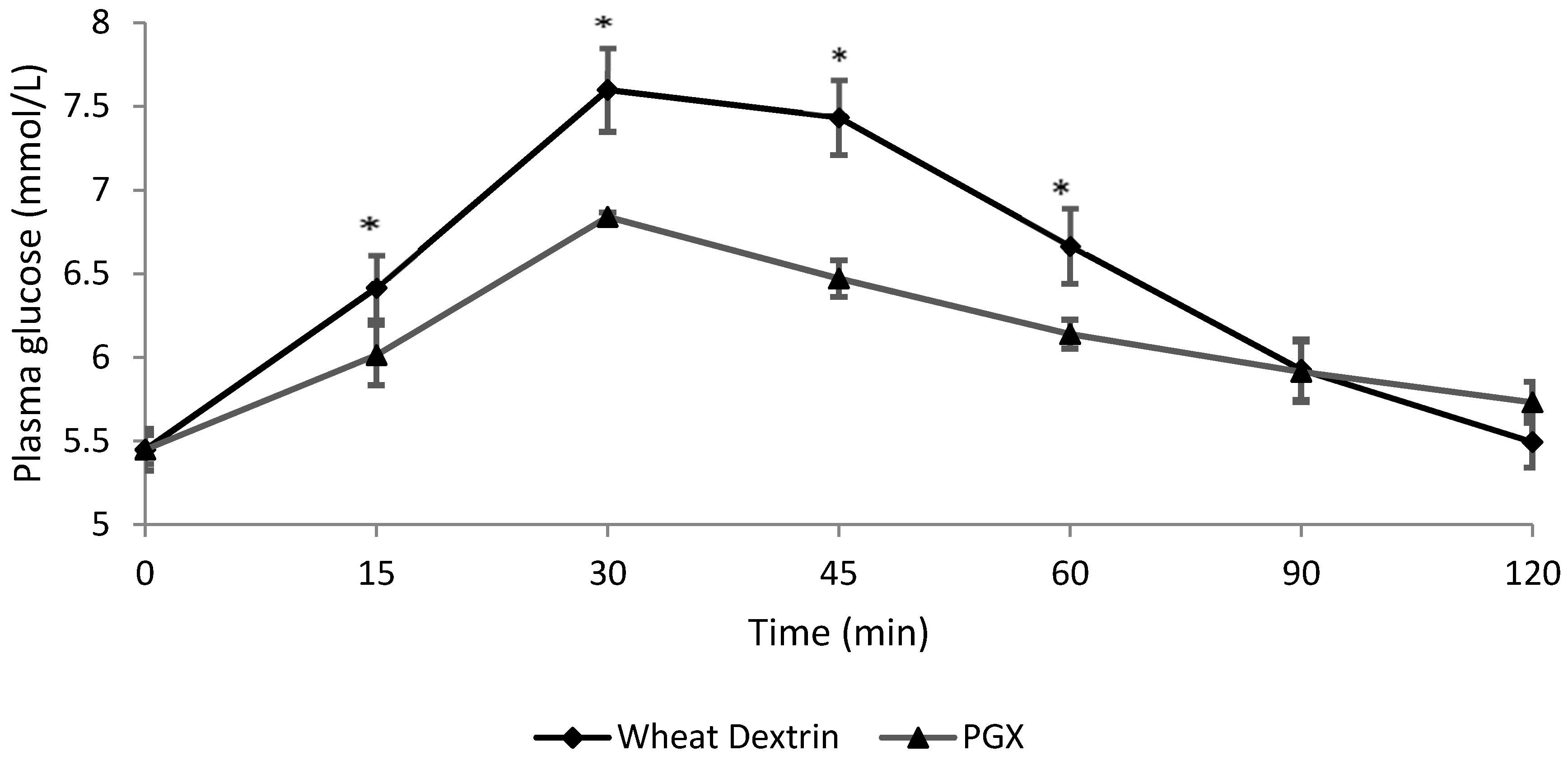
3.2. Blood Glucose
3.3. Viscosity
4. Discussion
4.1. Postprandial Satiety
4.2. Postprandial Glycaemia
4.3. Trained Panel Results
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Burkitt, D.P. The development of the fibre hypothesis. In Dietary Fibre; Birch, G.G., Parker, K.J., Eds.; Applied Science Publishers: London, UK, 1983; pp. 21–27. [Google Scholar]
- Mann, J.I.; Cummings, J.H. Possible implications for health of the different definitions of dietary fibre. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Chutkan, R.; Fahey, G.; Wright, W.L.; McRorie, J. Viscous versus non-viscous soluble fiber supplements: Mechanisms and evidence for fiber-specific health benefits. J. Am. Acad. Nurse Pract. 2012, 24, 476–487. [Google Scholar] [CrossRef] [PubMed]
- Howarth, N.C.; Saltzman, E.; Roberts, S.B. Dietary fiber and weight regulation. Nutr. Rev. 2001, 59, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, M.M.; Miller, M.J.; Freund, G.G. The health benefits of dietary fiber: Beyond the usual suspects of type 2 diabetes mellitus, cardiovascular disease and colon cancer. Metabolism 2012, 61, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L.; Savarino, V.; Paredes-Diaz, A.; Fotopoulos, G. A review of the role of soluble fiber in health with specific reference to wheat dextrin. J. Intern. Med. Res. 2009, 37, 1–17. [Google Scholar] [CrossRef]
- Brownlee, I.A. The physiological roles of dietary fibre. Food Hydrocoll. 2011, 25, 238–250. [Google Scholar] [CrossRef]
- Clark, M.J.; Slavin, J.L. The effect of fiber on satiety and food intake: A systematic review. J. Am. Coll. Nutr. 2013, 32, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.; Green, H. Dietary fibre and satiety. Nutr. Bull. 2007, 32, 32–42. [Google Scholar] [CrossRef]
- Mattes, R.D.; Rothacker, D. Beverage viscosity is inversely related to postprandial hunger in humans. Physiol. Behav. 2001, 74, 551–557. [Google Scholar] [CrossRef]
- Marciani, L.; Gowland, P.A.; Spiller, R.C.; Manoj, P.; Moore, R.J.; Young, P.; Fillery-Travis, A.J. Effect of meal viscosity and nutrients on satiety, intragastric dilution, and emptying assessed by MRI. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 280, 1227–1233. [Google Scholar]
- Hoad, C.L.; Rayment, P.; Spiller, R.C.; Marciani, L.; de Celis Alonso, B.; Traynor, C.; Mela, D.J.; Peters, H.F.P.; Gowland, P.A. In vivo imaging of intragastric gelation and its effect on satiety in humans. J. Nutr. 2004, 134, 2293–2300. [Google Scholar] [PubMed]
- Ludwig, D.S. Dietary glycaemic index and obesity. J. Nutr. 2000, 130, 280S–283S. [Google Scholar] [PubMed]
- Lafond, D.W.; Greaves, K.A.; Maki, K.C.; Leidy, H.J.; Romsos, D.R. Effects of two dietary fibers as part of ready-to-eat cereal (RTEC) breakfasts on perceived appetite and gut hormones in overweight women. Nutrients 2015, 7, 1245–1266. [Google Scholar] [CrossRef] [PubMed]
- Solah, V.A.; Kerr, D.; Meng, X.; Adikara, A.; Binns, C.; Zhu, K.; Devine, A.; Prince, R. Differences in satiety effects of alginate and whey protein-based foods. Appetite 2010, 54, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Guérin-Deremaux, L.; Pochat, M.; Reifer, C.; Wils, D.; Cho, S.; Miller, L.E. The soluble fiber NUTRIOSE induces a dose-dependent beneficial impact on satiety over time in humans. Nutr. Res. 2011, 31, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.L.; Kacinik, V.; Lyon, M.R.; Wolever, T. Effect of adding the novel fiber, PGX, to commonly consumed foods on glycaemic response, glycaemic index and GRIP: A simple and effective strategy for reducing postprandial blood glucose levels—A randomised, controlled trial. Nutr. J. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Kendall, C.W.; Esfahani, A.; Jenkins, D.J. The link between dietary fibre and human health. Food Hydrocoll. 2010, 24, 42–48. [Google Scholar] [CrossRef]
- Smith, I.H.; Lawson, C.J.; Harding, S.E.; Gahler, R.J.; Lyon, M.R.; Wood, S. Viscosity development during aqueous dispersion and dissolution: A comparison of PGX® with other dietary supplements and individual polysaccharides. Food Hydrocoll. 2014, 38, 152–162. [Google Scholar] [CrossRef]
- Brand-Miller, J.C.; Atkinson, F.S.; Gahler, R.J.; Kacinik, V.; Lyon, M.R.; Wood, S. Effects of PGX, a novel functional fibre, on acute and delayed postprandial glycaemia. Eur. J. Clin. Nutr. 2010, 64, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.C.; Atkinson, F.S.; Gahler, R.J.; Kacinik, V.; Lyon, M.R.; Wood, S. Effects of added PGX®, a novel functional fibre, on the glycaemic index of starchy foods. Br. J. Nutr. 2012, 108, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, S.S.; Wang, Y.; Anderson, C.; Gary, T.L. Have Americans increased their fruit and vegetable intake? The trends between 1988 and 2002. Am. J. Prev. Med. 2007, 32, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Rebello, C.J.; Liu, A.G.; Greenway, F.L.; Dhurandhar, N.V. Dietary strategies to increase satiety. Adv. Food Nutr. Res. 2013, 69, 105–182. [Google Scholar] [PubMed]
- Vuksan, V.; Panahi, S.; Lyon, M.; Rogovik, A.L.; Jenkins, A.L.; Leiter, L.A. Viscosity of fibre preloads affects food intake in adolescents. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Solah, V.; Brand-Miller, J.; Atkinson, F.; Gahler, R.; Kacinik, V.; Lyon, M.; Wood, S. Dose-response effect of a novel functional fibre, PolyGlycopleX, PGX, on satiety. Appetite 2014, 77, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Vermorel, M.; Coudray, C.; Wils, D.; Sinaud, S.; Tressol, J.C.; Montaurier, C.; Brandolini, M.; Vernet, J.; Bouteloup-Demange, C.; Rayssiguier, Y. Energy value of a low-digestible carbohydrate, NUTRIOSE® FB, and its impact on magnesium, calcium and zinc apparent absorption and retention in healthy young men. Eur. J. Nutr. 2004, 43, 322–349. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.; Hospattankar, A.; Deng, P.; Swanson, K.; Slavin, J. Prebiotic effects and fermentation kinetics of wheat dextrin and partially hydrolyzed guar gum in an in vitro batch fermentation system. Foods 2015, 4, 349–358. [Google Scholar] [CrossRef]
- Guerin-Deremaux, L.; Li, S.; Pochat, M.; Wils, D.; Mubasher, M.; Reifer, C.; Miller, L.E. Effects of NUTRIOSE® dietary fiber supplementation on body weight, body composition, energy intake, and hunger in overweight men. Int. J. Food Sci. Nutr. 2011, 62, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Solah, V.A.; Meng, X.; Wood, S.; Gahler, R.J.; Kerr, D.A.; James, A.P.; Pal, S.; Fenton, H.K.; Johnson, S.K. Effect of training on the reliability of satiety evaluation and use of trained panellists to determine the satiety effect of dietary fibre: A randomised controlled trial. PLoS ONE 2015, 10, e012. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Yong, M.K.; Solah, V.A.; Johnson, S.K.; Meng, X.; Kerr, D.A.; James, A.P.; Fenton, H.F.; Gahler, R.J.; Wood, S. Effects of a viscous-fibre supplemented evening meal and the following un-supplemented breakfast on post-prandial satiety responses in healthy women. Physiol. Behav. 2016, 154, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Mattes, R.D.; Hollis, J.; Hayes, D.; Stunkard, A.J. Appetite: Measurement and manipulation misgivings. J. Am. Diet. Assoc. 2005, 105, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Hlebowicz, J. Postprandial blood glucose response in relation to gastric emptying and satiety in healthy subjects. Appetite 2009, 53, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Ellis, P.; Morris, E. Importance of the rate of hydration of pharmaceutical preparations of guar gum: A new in vitro monitoring method. Diabetic Med. 1994, 8, 378–391. [Google Scholar] [CrossRef]
- Borreani, J.; Llorca, E.; Larrea, V.; Hernando, I. Adding neutral or anionic hydrocolloids to dairy proteins under in vitro gastric digestion conditions. Food Hydrocoll. 2016, 57, 169–177. [Google Scholar] [CrossRef]
- Batterham, R.L.; Rosenthal, J.M.; Zelaya, F.O.; Barker, G.J.; Withers, D.J.; Williams, S.C. PYY modulation of cortical and hypothalamic brain areas predicts feeding behaviour in humans. Nature 2007, 450, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Neary, M.T.; Batterham, R.L. Peptide YY: Food for thought. Physiol. Behav. 2009, 97, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Reimer, R.A.; Pelletier, X.; Carabin, I.G.; Lyon, M.; Gahler, R.; Parnell, J.A.; Woods, S. Increased plasma PYY levels following supplementation with functional fiber PolyGlycopleX in healthy adults. Eur. J. Clin. Nutr. 2010, 64, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Rolls, E.T. Understanding the mechanisms of food intake and obesity. Obes. Rev. 2007, 8, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Carabin, I.G.; Lyon, M.R.; Wood, S.; Pelletier, X.; Donazzolo, Y.; Burdock, G.A. Supplementation of the diet with the functional fiber PolyGlycoplex® is well tolerated by healthy subjects in a clinical trial. Nutr. J. 2009, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Hanefeld, M.; Leiter, L.; Monnier, L.; Moses, A.; Owens, D.; Tajima, N.; Tuomilehto, J. Postprandial glucose regulation and diabetic complications. Arch. Intern. Med. 2004, 164, 2090–2095. [Google Scholar] [CrossRef] [PubMed]
- Poppitt, S.D.; Van Drunen, J.D.; McGill, A.T.; Mulvey, T.B.; Leahy, F.E. Supplementation of a high-carbohydrate breakfast with barley β-glucan improves postprandial glycaemic response for meals but not beverages. Asia Pac. J. Clin. Nutr. 2007, 16, 16–24. [Google Scholar] [PubMed]
- Panahi, S.; Ezatagha, A.; Temelli, F.; Vasanthan, T.; Vuksan, V. β-glucan from two sources of oat concentrates affect postprandial glycemia in relation to the level of viscosity. J. Am. Coll. Nut. 2007, 26, 639–644. [Google Scholar] [CrossRef]
- Bookstein, L.; Gidding, S.S.; Donovan, M.; Smith, F.A. Day-to-day variability of serum cholesterol, triglyceride, and high-density lipoprotein cholesterol levels. Arch. Intern. Med. 1990, 150, 1653–1657. [Google Scholar] [CrossRef] [PubMed]
- Klop, B.; Cohn, J.S.; van Oostrom, A.J.; van Wijk, J.P.; Birnie, E.; Cabezas, M.C. Daytime triglyceride variability in men and women with different levels of triglyceridemia. Clin. Chim. Acta. 2011, 412, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Horner, K.M.; Byrne, N.M.; King, N.A. Reproducibility of subjective appetite ratings and ad libitum test meal energy intake in overweight and obese males. Appetite 2014, 81, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Grunwald, G.K.; Johnson, S.L.; Bessesen, D.H. Effects of short-term overfeeding on hunger, satiety, and energy intake in thin and reduced-obese individuals. Appetite 2004, 43, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Dye, L.; Blundell, J.E. Menstrual cycle and appetite control: Implications for weight regulation. Hum. Reprod. 1997, 12, 1142–1151. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Special K Original a | Cornflakes b | Full Cream Milk c | Drinking Water | Total Meal | |
|---|---|---|---|---|---|
| Mass of Serve (g) | 22.5 | 22.5 | 175 | 500 | 720 |
| Protein (g/serve) | 4.4 | 1.7 | 5.6 | 0 | 117 |
| Fat (g/serve) | 0.2 | 0.6 | 6.3 | 0 | 7.1 |
| Available Carbohydrates (g/serve) | 15 | 18.1 | 8.3 | 0 | 41.4 |
| Total Dietary Fibre (g/serve) | 2.6 | 1.2 | 0 | 0 | 3.8 |
| Energy (kJ) | 350 | 347 | 508 | 0 | 1205 |
| Satiety (Score (cm) Time (min)) | ||
| AUC mean (SD) | Difference from wheat dextrin Coefficient (95% CI), p value * | |
| Wheat dextrin | 215 (261) | |
| PGX softgel | 477 (121) | 262 (138, 387), p < 0.001 |
| PGX (granules) | 454 (242) | 240 (183, 296), p < 0.001 |
| Glucose (mmol/L·min) | ||
| AUC mean (SD) | Difference (PGX-wheat dextrin) Coefficient (95% CI), p value * | |
| Wheat dextrin | 713 (67) | |
| PGX (granules) | 674 (56) | −40 (−59, −21), p < 0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solah, V.A.; O’Mara-Wallace, B.; Meng, X.; Gahler, R.J.; Kerr, D.A.; James, A.P.; Fenton, H.K.; Johnson, S.K.; Wood, S. Consumption of the Soluble Dietary Fibre Complex PolyGlycopleX® Reduces Glycaemia and Increases Satiety of a Standard Meal Postprandially. Nutrients 2016, 8, 268. https://doi.org/10.3390/nu8050268
Solah VA, O’Mara-Wallace B, Meng X, Gahler RJ, Kerr DA, James AP, Fenton HK, Johnson SK, Wood S. Consumption of the Soluble Dietary Fibre Complex PolyGlycopleX® Reduces Glycaemia and Increases Satiety of a Standard Meal Postprandially. Nutrients. 2016; 8(5):268. https://doi.org/10.3390/nu8050268
Chicago/Turabian StyleSolah, Vicky A., Babette O’Mara-Wallace, Xingqiong Meng, Roland J. Gahler, Deborah A. Kerr, Anthony P. James, Haelee K. Fenton, Stuart K. Johnson, and Simon Wood. 2016. "Consumption of the Soluble Dietary Fibre Complex PolyGlycopleX® Reduces Glycaemia and Increases Satiety of a Standard Meal Postprandially" Nutrients 8, no. 5: 268. https://doi.org/10.3390/nu8050268
APA StyleSolah, V. A., O’Mara-Wallace, B., Meng, X., Gahler, R. J., Kerr, D. A., James, A. P., Fenton, H. K., Johnson, S. K., & Wood, S. (2016). Consumption of the Soluble Dietary Fibre Complex PolyGlycopleX® Reduces Glycaemia and Increases Satiety of a Standard Meal Postprandially. Nutrients, 8(5), 268. https://doi.org/10.3390/nu8050268