Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
3.1. 24 h Urine Samples
3.2. Blood Indices
3.3. Total Water Intake
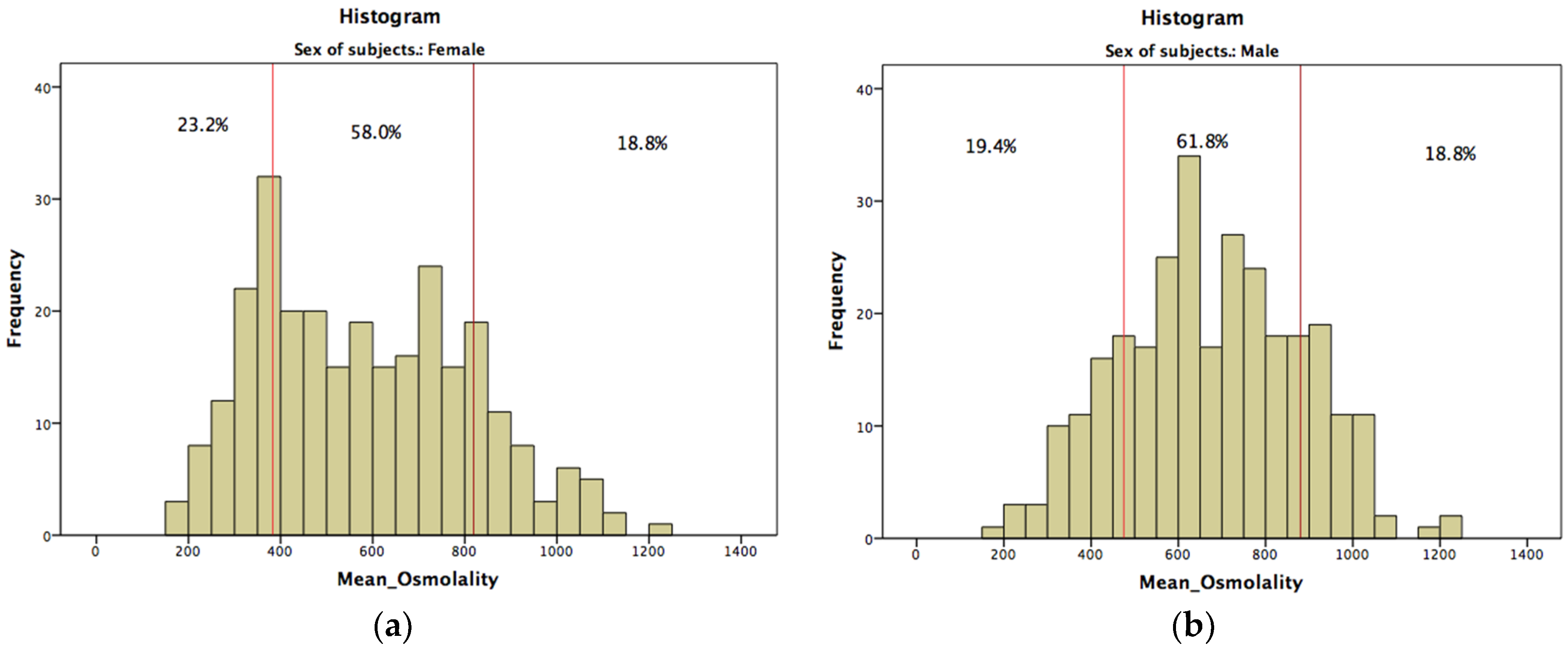
3.4. Classification of Subjects
3.5. Linear Regression Model
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- EFSA. Scientific opinion on the substantiation of health claims related to water and maintenance of normal physical and cognitive functions (id 1102, 1209, 1294, 1331), maintenance of normal thermoregulation (id 1208) and “basic requirement of all living things” (id 1207) pursuant to article 13(1) of regulation (ec) no 1924/2006. EFSA J. 2011, 9, 2075–2091. [Google Scholar]
- Tack, I. Effects of water consumption on kidney function and excretion. Nutr. Today 2010, 45, S37–S40. [Google Scholar] [CrossRef]
- Perrier, E.; Vergne, S.; Klein, A.; Poupin, M.; Rondeau, P.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I. Hydration biomarkers in free-living adults with different levels of habitual fluid consumption. Br. J. Nutr. 2013, 109, 1678–1687. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459–1507. [Google Scholar]
- Medicine, I.O. Panel on Dietary Reference Intakes for Electrolytes and Water: Dietary Reference Intakes for Water, Potassium, Sodium, Chloride and Sulfate; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Popkin, B.M.; D'Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Perrier, E.; Demazieres, A.; Girard, N.; Pross, N.; Osbild, D.; Metzger, D.; Guelinckx, I.; Klein, A. Circadian variation and responsiveness of hydration biomarkers to changes in daily water intake. Eur. J. Appl. Physiol. 2013, 113, 2143–2151. [Google Scholar] [CrossRef] [PubMed]
- Lemaire, J.B.; Wallace, J.E.; Dinsmore, K.; Lewin, A.M.; Ghali, W.A.; Roberts, D. Physician nutrition and cognition during work hours: Effect of a nutrition based intervention. BMC Health Serv. Res. 2010, 10, 241. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, F.; Houchins, J.A.; Mattes, R.D. Relationships between human thirst, hunger, drinking, and feeding. Physiol. Behav. 2008, 94, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Malisova, O.; Bountziouka, V.; Panagiotakos, D.B.; Zampelas, A.; Kapsokefalou, M. The water balance questionnaire: Design, reliability and validity of a questionnaire to evaluate water balance in the general population. Int. J. Food Sci. Nutr. 2012, 63, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.D.; Thornton, S.N.; Lee, J.K.; Laursen, P.B. Are we being drowned in hydration advice? Thirsty for more? Extreme Physiol. Med. 2014, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Perrier, E.; Rondeau, P.; Poupin, M.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Schatzkin, A.; Kipnis, V.; Carroll, R.J.; Midthune, D.; Subar, A.F.; Bingham, S.; Schoeller, D.A.; Troiano, R.P.; Freedman, L.S. A comparison of a food frequency questionnaire with a 24-h recall for use in an epidemiological cohort study: Results from the biomarker-based observing protein and energy nutrition (OPEN) study. Int. J. Epidemiol. 2003, 32, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Sawka, M.N. Biological variation and diagnostic accuracy of dehydration assessment markers. Am. J. Clin. Nutr. 2010, 92, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Fraser, C.G.; Kenefick, R.W.; Ely, B.R.; Sawka, M.N. Reference change values for monitoring dehydration. Clin. Chem. Lab. Med. 2011, 49, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Johnson, E.C.; Munoz, C.X.; Swokla, B.; Le Bellego, L.; Jimenez, L.; Casa, D.J.; Maresh, C.M. Hydration biomarkers and dietary fluid consumption of women. J. Acad. Nutr. Diet. 2012, 112, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Pumerantz, A.C.; Fiala, K.A.; Roti, M.W.; Kavouras, S.A.; Casa, D.J.; Maresh, C.M. Human hydration indices: Acute and longitudinal reference values. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 145–153. [Google Scholar] [PubMed]
- Armstrong, L.E. Assessing hydration status: The elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef] [PubMed]
- Kavouras, S.A. Assessing hydration status. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Vergne, S. Methodological aspects of fluid intake records and surveys. Nutr. Today 2012, 47, S7–S10. [Google Scholar] [CrossRef]
- Ix, J.H.; Wassel, C.L.; Stevens, L.A.; Beck, G.J.; Froissart, M.; Navis, G.; Rodby, R.; Torres, V.E.; Zhang, Y.L.; Greene, T.; et al. Equations to estimate creatinine excretion rate: The CKD epidemiology collaboration. Clin. J. Am. Soc. Nephrol. 2011, 6, 184–191. [Google Scholar] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [PubMed]
- Manz, F.; Wentz, A. 24-h hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57, S10–S18. [Google Scholar] [CrossRef] [PubMed]
- Beards, A.; Bryman, A.; Keil, T.; Goode, J.; Haslam, C.; Lanchashire, E. Women, men and food: The significance of gender for nutritional attitudes and choices. Br. Food J. 2002, 104, 470–491. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choices: The contribution of health beliefs and dieting Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef]
- Manz, F.; Johner, S.A.; Wentz, A.; Boeing, H.; Remer, T. Water balance throughout the adult life span in a german population. Br. J. Nutr. 2012, 107, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Intersalt cooperative research group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar]
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The beverage intake questionnaire: Determining initial validity and reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Zhang, Q.; Liu, A.; Zuo, J.; Zhang, W.; Zou, S.; Li, X.; Lu, L.; Pan, H.; Hu, X. Fluid intake of adults in four Chinese cities. Nutr. Rev. 2012, 70, S105–S110. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.; Shirreffs, S.M. Beverage consumption habits “24/7” among british adults: Association with total water intake and energy intake. Nutr. J. 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Pego, C.; Guelinckx, I.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Total fluid intake and its determinants: Cross-sectional surveys among adults in 13 countries worldwide. Eur. J. Nutr. 2015, 54, 35–43. [Google Scholar] [PubMed]
- Wolfram, G. New reference values for nutrient intake in germany, austria and switzerland (dach-reference values). Forum Nutr. 2003, 56, 95–97. [Google Scholar] [PubMed]
- Malisova, O.; Bountziouka, V.; Panagiotakos, D.; Zampelas, A.; Kapsokefalou, M. Evaluation of seasonality on total water intake, water loss and water balance in the general population in greece. J. Hum. Nutr. Diet. 2013, 26, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Panagiotakos, D.B.; Pitsavos, C.; Polychronopoulos, E.; Stefanadis, C. Implication of socio-economic status on the prevalence of overweight and obesity in greek adults: The attica study. Health Policy 2005, 74, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Gnardellis, C.; Lagiou, A.; Benetou, V.; Naska, A.; Trichopoulos, D. Physical activity and total energy intake selectively predict the waist-to-hip ratio in men but not in women. Am. J. Clin. Nutr. 2011, 74, 574–578. [Google Scholar]

{kind=link}
| Sodium (mEq/Day) | Potassium (mEq/Day) | Creatinine (mg/Day) | Urine Osmolality (mOsmol/kg·Η2Ο) | Urine Volume (L) | USG | Color | ||
|---|---|---|---|---|---|---|---|---|
| Winter | Male | 178.4 ± 51.5 | 76.0 ± 20.1 | 1738.4 ± 523.0 | 652 ± 211 | 1.66 ± 0.62 | 1.018 ± 0.005 | 4.4 ± 1.4 |
| Female | 162.9 ± 56.7 | 68.8 ± 21.8 | 1335.6 ± 404.1 | 571 ± 197 | 1.70 ± 0.72 | 1.016 ± 0.005 | 4.1 ± 1.3 | |
| Total | 171.4 ± 54.4 | 72.7 ± 21.2 | 1555.2 ± 512.8 | 615 ± 209 | 1.68 ± 0.66 | 1.017 ± 0.005 | 4.2 ± 1.4 | |
| Summer | Male | 181.9 ± 50.1 | 76.2 ± 25.7 | 1820.6 ± 451.6 | 698 ± 192 | 1.61 ± 0.70 | 1.018 ± 0.005 | 4.6 ± 1.2 |
| Female | 145.6 ± 53.1 | 68.5 ± 28.3 | 1290.0 ± 474.4 | 596 ± 251 | 1.63 ± 0.77 | 1.015 ± 0.006 | 3.9 ± 1.6 | |
| Total | 162.8 ±54.7 | 72.2 ± 27.3 | 1543.7 ± 533.6 | 645 ± 230 | 1.62 ± 0.73 | 1.017 ± 0.006 | 4.2 ± 1.5 | |
| P1 | 0.021 | 0.005 | <0.001 | 0.001 | 0.586 | 0.003 | 0.069 | |
| P2 | <0.001 | 0.016 | <0.001 | <0.001 | 0.789 | <0.001 | <0.001 | |
| P3 | 0.065 | 0.789 | 0.795 | 0.111 | 0.370 | 0.679 | 0.983 | |
| Winter & Summer | Total Male | 180.1 ± 50.8 | 76.1± 22.9 | 1779.1 ± 489.9 | 675 ± 203 | 1.63 ± 0.66 | 1.018 ± 0.005 | 4.5 ± 1.3 |
| Total Female | 153.2 ± 55.3 | 68.6 ± 25.6 | 1310 ± 444.7 | 585 ± 229 | 1.66 ± 0.74 | 1.015 ± 0.006 | 4.0 ± 1.5 | |
| Total Sample | 166.9 ± 54.7 | 72.4 ± 24.6 | 1549.1 ± 523.4 | 631 ± 221 | 1.65 ± 0.70 | 1.017 ± 0.005 | 4.2 ± 1.4 | |
| P4 | <0.001 | <0.001 | <0.001 | <0.001 | 0.619 | <0.001 | <0.001 | |
| Country | German | 162.2 ± 50.3 *,# | 77.9 ± 24.1 # | 1454.0 ± 401.0 * | 492 ± 170 *,# | 2.13 ± 0.76 *,# | 1.014 ± 0.005 *,# | 4.4 ± 1.3 # |
| Spain | 192.8 ± 51.7 + | 74.0 ± 27.8 + | 1807.9 ± 621.2 + | 753 ± 180+ | 1.40 ± 0.49 | 1.019 ± 0.004 + | 4.4 ± 1.5 + | |
| Greece | 143.8 ± 51.0 | 64.4 ± 18.7 | 1377.9 ± 415.3 | 658 ± 224 | 1.36 ± 0.50 | 1.017 ± 0.006 | 4.0 ±1.5 | |
| P5 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.008 |
| Hb (g/dL) | Htc (%) | Glucose (mmol/L) | Serum Osmolality (mOsmol/kg Η2Ο) | Sodium (mEq/L) | Potassium (mEq/L) | ||
|---|---|---|---|---|---|---|---|
| Winter | Male | 15.3 ± 1.5 | 45 ± 3 | 4.67 ± 0.46 | 297 ± 10 | 143.0 ± 4.9 | 4.4 ± 0.4 |
| Female | 14.1 ± 1.6 | 42 ± 4 | 4.73 ± 0.52 | 294 ± 10 | 141.6 ± 3.9 | 4.4 ± 0.4 | |
| Total | 14.7 ± 1.7 | 43 ± 4 | 4.70 ± 0.49 | 296 ± 10 | 142.4 ± 4.5 | 4.4 ± 0.4 | |
| Summer | Male | 15.5 ± 1.5 | 45 ± 3 | 5.02 ± 1.09 | 293 ± 7 | 143.3 ± 5.1 | 4.5 ± 0.5 |
| Female | 14.0 ± 1.6 | 41 ± 4 | 4.88 ± 1.59 | 291 ± 8 | 144.7 ± 11.3 | 4.6 ± 0.6 | |
| Total | 14.7 ± 1.7 | 43 ± 4 | 4.94 ± 1.37 | 292 ± 8 | 144.0 ± 8.9 | 4.6 ± 0.6 | |
| P1 | <0.001 | <0.001 | 0.339 | 0.015 | 0.020 | 0.580 | |
| P2 | <0.001 | <0.001 | 0.388 | 0.081 | 0.166 | 0.064 | |
| P3 | 0.824 | 0.397 | 0.005 | <0.001 | 0.005 | <0.001 | |
| Winter & Summer | Total Male | 15.4 ± 1.5 | 45 ± 3 | 4.84 ± 0.85 | 295 ± 9 | 143.1 ± 5.0 | 4.5 ± 0.5 |
| Total Female | 14.0 ± 1.6 | 42 ± 4 | 4.81± 1.24 | 292 ± 9 | 143.3 ± 8.9 | 4.5 ± 0.5 | |
| Total Sample | 14.7 ± 1.7 | 43 ± 4 | 4.83 ± 1.06 | 294 ± 9 | 143.2 ± 7.2 | 4.5 ± 0.5 | |
| P4 | <0.001 | <0.001 | 0.724 | 0.001 | 0.717 | 0.159 | |
| Country | German | 14.3 ± 1.3 * | 43 ± 3 *,# | 4.52 ± 1.43 *,# | 298 ± 11*# | 141.0 ± 1.7 # | 4.5 ± 0.4 # |
| Spain | 15.2 ± 1.3+ | 46 ± 3 + | 4.96 ± 0.39 | 289 ± 8 + | 141.2 ± 2.6 + | 4.4 ± 0.5 + | |
| Greece | 14.6 ± 2.3 | 41 ± 4 | 5.07 ± 0.97 | 294 ± 6 | 148.5 ± 11.4 | 4.6 ± 0.6 | |
| P5 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Total Water Intake (L/Day) | Water from Beverages (L/Day) | Water from Foods (L/Day) | Total Energy Intake (kcal/Day) | Energy from Beverages (kcal/Day) | ||
|---|---|---|---|---|---|---|
| Winter | Male | 2.77 ± 1.10 | 2.12 ± 1.09 | 0.67 ± 0.31 | 2248 ± 659 | 302 ± 203 |
| Female | 2.49 ± 0.80 | 1.89 ± 0.71 | 0.61 ± 0.25 | 1913 ± 477 | 258 ± 143 | |
| Total | 2.64 ± 0.98 | 2.01 ± 0.94 | 0.64 ± 0.29 | 2093 ± 605 | 282 ± 179 | |
| Summer | Male | 3.09 ± 1.07 | 2.41 ± 0.93 | 0.69 ± 0.29 | 2413 ± 706 | 338 ± 233 |
| Female | 2.61 ± 0.91 | 1.97 ± 0.75 | 0.64 ± 0.29 | 1989 ± 580 | 254 ± 141 | |
| Total | 2.84 ± 1.02 | 2.18 ± 0.87 | 0.68 ± 0.29 | 2192 ± 676 | 294 ± 195 | |
| P1 | 0.014 | 0.034 | 0.075 | <0.001 | 0.038 | |
| P2 | <0.001 | <0.001 | 0.152 | <0.001 | 0.001 | |
| P3 | 0.019 | 0.027 | 0.339 | 0.068 | 0.430 | |
| Winter & Summer | Total Male | 2.93 ± 1.10 | 2.27 ± 1.02 | 0.68 ± 0.30 | 2329 ± 686 | 320 ± 219 |
| Total Female | 2.55 ± 0.86 | 1.93 ± 0.73 | 0.63 ± 0.27 | 1955 ± 537 | 256 ± 142 | |
| Total Sample | 2.75 ± 1.01 | 2.10 ± 0.91 | 0.66 ± 0.29 | 2148 ± 644 | 288 ± 188 | |
| P4 | <0.001 | <0.001 | 0.027 | <0.001 | <0.001 | |
| Country | German | 3.29 ± 0.98 *,# | 2.49 ± 0.87 *,# | 0.81 ± 0.27 *,# | 2412 ± 609 *,# | 358 ± 240 *,# |
| Spain | 2.55 ± 0.98 | 1.96 ± 0.95 | 0.61 ± 0.29 + | 2214 ± 633 + | 296 ± 145 + | |
| Greece | 2.35 ± 0.77 | 1.82 ± 0.74 | 0.54 ± 0.23 | 1777 ± 512 | 203 ± 113 | |
| P5 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Categories of Hydration Status According to Urine Osmolality (mOsm/kg H20) | ||||
|---|---|---|---|---|
| Hyperhydrated | Euhydrated | Dehydrated | p | |
| (<383) | (383 to 810) | (>810) | ||
| Females, % (n) | 23.2 (64) | 58.0 (160) | 18.8 (52) | |
| Total water intake (L/day) | 3.36 ± 1.02 | 2.42 ± 0.61 | 2.02 ± 0.65 | <0.001 |
| Water from beverages (L/day) | 2.60 ± 0.91 | 1.81 ± 0.49 | 1.53 ± 0.57 | <0.001 |
| 24 h urine volume (L) | 2.51 ± 0.73 | 1.54 ± 0.52 | 1.00 ± 0.25 | <0.001 |
| 24 h urine specific gravity | 1.009 ± 0.002 | 1.016 ± 0.004 | 1.023 ± 0.003 | <0.001 |
| 24 h urine color | 3.0 ± 1.2 | 3.9 ± 1.2 | 5.5 ± 1.2 | <0.001 |
| 24 h urine Na (mEq/day) | 129.4 ± 37.1 | 158.7 ± 59.1 | 166.3 ± 54.2 | <0.001 |
| 24 h urine K (mEq/day) | 73.9 ± 36.5 | 67.6 ± 21.6 | 65.4 ± 20.1 | 0.153 |
| 24 h urine creatinine (mg/day) | 1137.6 ± 249.1 | 1362.5 ± 494.0 | 1363.6 ± 429.6 | 0.002 |
| (<475) | (475 to 880) | (>880) | ||
| Males, % (n) | 19.4 (55) | 61.8 (181) | 18.8 (54) | |
| Total water intake (L/day) | 3.59 ± 1.04 | 2.8 ± 0.99 | 2.64 ± 1.25 | <0.001 |
| Water from beverages (L/day) | 2.83 ± 1.00 | 2.15 ± 0.86 | 2.08 ± 1.31 | <0.001 |
| 24 h urine volume (L) | 2.45 ± 0.69 | 1.56 ± 0.46 | 1.00 ±0.24 | <0.001 |
| 24 h urine specific gravity | 1.011 ± 0.002 | 1.018 ± 0.003 | 1.025 ± 0.02 | <0.001 |
| 24 h urine color | 3.6 ± 1.4 | 4.3 ± 1.1 | 5.9 ± 1.0 | <0.001 |
| 24 h urine Na (mEq/day) | 156.4 ± 50.0 | 187.7 ± 46.4 | 180.1 ± 59.5 | <0.001 |
| 24 h urine K (mEq/day) | 76.9 ± 19.9 | 77.7 ± 24.4 | 69.8 ± 20.2 | 0.091 |
| 24 h urine creatinine (mg/day) | 1517.7 ± 399.02 | 1862.9 ± 483.3 | 1771.2 ± 522.1 | <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malisova, O.; Athanasatou, A.; Pepa, A.; Husemann, M.; Domnik, K.; Braun, H.; Mora-Rodriguez, R.; Ortega, J.F.; Fernandez-Elias, V.E.; Kapsokefalou, M. Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS). Nutrients 2016, 8, 204. https://doi.org/10.3390/nu8040204
Malisova O, Athanasatou A, Pepa A, Husemann M, Domnik K, Braun H, Mora-Rodriguez R, Ortega JF, Fernandez-Elias VE, Kapsokefalou M. Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS). Nutrients. 2016; 8(4):204. https://doi.org/10.3390/nu8040204
Chicago/Turabian StyleMalisova, Olga, Adelais Athanasatou, Alex Pepa, Marlien Husemann, Kirsten Domnik, Hans Braun, Ricardo Mora-Rodriguez, Juan F. Ortega, Valentin E. Fernandez-Elias, and Maria Kapsokefalou. 2016. "Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS)" Nutrients 8, no. 4: 204. https://doi.org/10.3390/nu8040204
APA StyleMalisova, O., Athanasatou, A., Pepa, A., Husemann, M., Domnik, K., Braun, H., Mora-Rodriguez, R., Ortega, J. F., Fernandez-Elias, V. E., & Kapsokefalou, M. (2016). Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS). Nutrients, 8(4), 204. https://doi.org/10.3390/nu8040204