Effects of Walnut Consumption on Mood in Young Adults—A Randomized Controlled Trial


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Dietary Intervention
2.4. Mood Testing
2.5. Statistical Analysis
3. Results
3.1. Description of the Study Population
3.2. POMS Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Grosso, G.; Estruch, R. Nut consumption and age-related disease. Maturitas 2016, 84, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Yang, J.; Marventano, S.; Micek, A.; Galvano, F.; Kales, S.N. Nut consumption on all-cause, cardiovascular, and cancer mortality risk: A systematic review and meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2015, 101, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Wang, Z.; Zhu, J.; Murad, A.L.; Prokop, L.J.; Murad, M.H. Nut consumption and risk of cancer and type 2 diabetes: A systematic review and meta-analysis. Nutr. Rev. 2015, 73, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Mozaffarian, D. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Mejia, S.B.; Kendall, C.W.; Viguiliouk, E.; Augustin, L.S.; Ha, V.; Cozma, A.I.; Mirrahimi, A.; Maroleanu, A.; Chiavaroli, L.; Leiter, L.A.; et al. Effect of tree nuts on metabolic syndrome criteria: A systematic review and meta-analysis of randomized controlled trials. BMJ Open 2014, 4, e004660. [Google Scholar] [CrossRef] [PubMed]
- Sabate, J.; Oda, K.; Ros, E. Nut consumption and blood lipid levels: A pooled analysis of 25 intervention trials. Arch. Intern. Med. 2010, 170, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Ros, E. Health benefits of nut consumption. Nutrients 2010, 2, 652–682. [Google Scholar] [CrossRef] [PubMed]
- Ownby, R.L. Neuroinflammation and cognitive aging. Curr. Psychiatry Rep. 2010, 12, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinilla, F. Brain foods: The effects of nutrients on brain function. Nat. Rev. Neurosci. 2008, 9, 568–578. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture: Nutrient Database. Available online: http://ndb.nal.usda.gov/ndb (accessed on 22 September 2016).
- Reiter, R.J.; Manchester, L.C.; Tan, D.X. Melatonin in walnuts: Influence on levels of melatonin and total antioxidant capacity of blood. Nutrition 2005, 21, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.A.; Oliveira, I.; Sousa, A.; Ferreira, I.C.; Bento, A.; Estevinho, L. Bioactive properties and chemical composition of six walnut (Juglans regia L.) cultivars. Food Chem. Toxicol. 2008, 46, 2103–2111. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, S.C. Dietary ω-3 fatty acid supplementation for optimizing neuronal structure and function. Mol. Nutr. Food Res. 2010, 54, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Poulose, S.M.; Miller, M.G.; Shukitt-Hale, B. Role of walnuts in maintaining brain health with age. J. Nutr. 2014, 144 (Suppl. 4), 561S–566S. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.A.; Howe, P.R.; Buckley, J.D.; Bryan, J.; Coates, A.M. Nut consumption for vascular health and cognitive function. Nutr. Res. Rev. 2014, 27, 131–158. [Google Scholar] [CrossRef] [PubMed]
- Pribis, P.; Bailey, R.N.; Russell, A.A.; Kilsby, M.A.; Hernandez, M.; Craig, W.J.; Grajales, T.; Shavlik, D.J.; Sabate, J. Effects of walnut consumption on cognitive performance in young adults. Br. J. Nutr. 2012, 107, 1393–1401. [Google Scholar] [CrossRef] [PubMed]
- McNair, D.M.; Heuchert, J.W.P. Profiles of Mood States—Technical Update; Multi-Health Systems, Inc.: Toronto, ON, Canada, 2005. [Google Scholar]
- Nyenhuis, D.L.; Yamamoto, C.; Luchetta, T.; Terrien, A.; Parmentier, A. Adult and geriatric normative data and validation of the profile of mood states. J. Clin. Psychol. 1999, 55, 79–86. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power for the Behavioral Sciences, 2nd ed.; Hillsdale & Lawrence Erlbaum: Hillsdale, NJ, USA, 1998. [Google Scholar]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Covas, M.I.; Arós, F.; Romaguera, D.; Gómez-Gracia, E.; Lapetra, J.; et al. Mediterranean dietary pattern and depression: The PREDIMED randomized trial. BMC. Med. 2013, 11, 208. [Google Scholar] [CrossRef] [PubMed]
- Pribis, P.; Shukitt-Hale, B. Cognition: The new frontier for nuts and berries. Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 347S–352S. [Google Scholar] [CrossRef] [PubMed]
- Newens, K.J.; Thompson, A.K.; Jackson, K.G.; Wright, J.; Williams, C.M. Acute effects of elevated NEFA on vascular function: A comparison of SFA and MUFA. Br. J. Nutr. 2011, 105, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Galvano, F.; Marventano, S.; Malaguarnera, M.; Bucolo, C.; Drago, F.; Caraci, F. Omega-3 fatty acids and depression: Scientific evidence and biological mechanisms. Oxid. Med. Cell. Longev. 2014, 2014, 313570. [Google Scholar] [CrossRef] [PubMed]
- Giles, G.E.; Mahoney, C.R.; Kanarek, R.B. Omega-3 fatty acids influence mood in healthy and depressed individuals. Nutr. Rev. 2013, 71, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Appleton, K.M.; Rogers, P.J.; Ness, A.R. Updated systematic review and meta-analysis of effects of n-3 long-chain polyunsaturated fatty acids on depressed mood. Am. J. Clin. Nutr. 2010, 91, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Bakewell, L.; Burdge, G.C.; Calder, P.C. Polyunsaturated fatty acid concentrations in young men and women consuming their habitual diets. Br. J. Nutr. 2006, 96, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Decsi, T.; Kennedy, K. Sex-specific differences in essential fatty acid metabolism. Am. J. Clin. Nutr. 2011, 94 (Suppl. 6), 1914S–1919S. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Mamplekou, E.; Pitsavos, C.; Kalogeropoulos, N.; Kastorini, C.M.; Papageorgiou, C.; Papadimitriou, G.N.; Stefanadis, C. Fatty acids intake and depressive symptomatology in a Greek sample: An epidemiological analysis. J. Am. Coll. Nutr. 2010, 29, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Astorg, P.; Couthouis, A.; Bertrais, S.; Arnault, N.; Meneton, P.; Guesnet, P.; Alessandri, J.M.; Galan, P.; Hercberg, S. Association of fish and long-chain n-3 polyunsaturated fatty acid intakes with the occurrence of depressive episodes in middle-aged French men and women. Prostaglandins Leukot. Essent. Fatty Acids 2008, 78, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Fontani, G.; Corradeschi, F.; Felici, A.; Alfatti, F.; Bugarini, R.; Fiaschi, A.I.; Cerretani, D.; Montorfano, G.; Rizzo, A.M.; Berra, B. Blood profiles, body fat and mood state in healthy subjects on different diets supplemented with Omega-3 polyunsaturated fatty acids. Eur. J. Clin. Investig. 2005, 35, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Antypa, N.; Van der Does, A.J.W.; Smelt, A.H.M.; Rogers, R.D. Omega-3 fatty acids (fish-oil) and depression-related cognition in healthy volunteers. J. Psychopharmacol. 2009, 23, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Young, W.M. Effect of plant sources of Omega-3 PUFA on mood status in healthy subjects: A cross over feeding trial. FASEB J. 2016, 30 (Suppl. 1), 130–138. [Google Scholar]
- Singh, U.; Devaraj, S.; Jialal, I. Vitamin E, oxidative stress and, inflammation. Annu. Rev. Nutr. 2005, 25, 151–174. [Google Scholar] [CrossRef] [PubMed]
- Collie, A.; Morley, G. Do polyphenols affect human cognitive function? Curr. Top. Neutraceutical Res. 2007, 5, 148–148. [Google Scholar]
- Korkmaz, A.; Reiter, R.J.; Tan, D.X.; Manchester, L.C. Melatonin; from pineal gland to healthy foods. Spatula DD 2011, 1, 33–36. [Google Scholar] [CrossRef]
- Leibenluft, E.; Albert, P.S.; Rosenthal, N.E.; Wehr, T.A. Relationship between sleep and mood in patients with rapid-cycling bipolar disorder. Psychiatry Res. 1996, 63, 161–168. [Google Scholar] [CrossRef]
- Benton, D.; Donohoe, R.T. The effects of nutrients on mood. Public Health. Nutr. 1999, 2, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R. What comes first: The food or the nutrient? Executive summary of a symposium. J. Nutr. 2014, 144 (Suppl. 4), 543S–546S. [Google Scholar] [CrossRef] [PubMed]
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Riffenburgh, R.H. Statistics in Medicine, 3th ed.; Academic Press: San Diego, CA, USA, 2012; pp. 267–268. [Google Scholar]

{kind=link}
| Nutrients in 14 Halves (28 g) | |
|---|---|
| Minerals (mg) | |
| Calcium | 28 |
| Magnesium | 45 |
| Potassium | 125 |
| Vitamins (μg) | |
| Thiamin | 97 |
| Vitamin B6 | 152 |
| Folate | 28 |
| Lutein | 3 |
| α-tocopherol | 200 |
| β-tocopherol | 40 |
| γ-tocopherol | 5910 |
| δ-tocopherol | 540 |
| Lipids (g) | |
| ALA; 18:3n-3 | 2.6 |
| LA; 18: 2n-6 | 10.8 |
| Phenols (mg GAE) | |
| Total phenols | 436 |
| Other (ng) | |
| Melatonin | 98 |
| Per 100 g | Walnuts | Placebo |
|---|---|---|
| Energy (kJ/kcal) | 1612/385 | 1202/287 |
| Carbohydrate (g) | 40.9 | 48.9 |
| Protein (g) | 7.0 | 5.2 |
| Fat (g) | 21.5 | 7.9 |
| Saturated Fatty Acids (g) | 2.5 | 1.5 |
| Monounsaturated Fatty Acids (g) | 3.8 | 1.9 |
| Polyunsaturated Fatty Acids (g) | 14.1 | 4.0 |
| α—Linolenic acid (18:3n-3) (g) | 2.5 | 0.2 |
| Linoleic acid (18:2n-6) (g) | 12.2 | 4.0 |
| Group | Walnut–Placebo (n = 32) | Placebo–Walnut (n = 32) | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (years) | 20.6 | 2.0 | 20.7 | 2.1 | 0.872 * |
| BMI (kg/m2) | 22.6 | 3.3 | 23.2 | 3.5 | 0.471 * |
| n | % | n | % | ||
| Ethnicity (n, %) | 0.255 † | ||||
| Caucasian | 18 | 56.3 | 11 | 35.5 | |
| African American | 5 | 15.6 | 7 | 22.6 | |
| Other | 9 | 28.1 | 13 | 41.9 | |
| Class standing (n, %) | 0.977 † | ||||
| Freshman | 8 | 25.0 | 7 | 22.6 | |
| Sophomore | 7 | 21.9 | 9 | 29.0 | |
| Junior | 8 | 25.0 | 7 | 22.6 | |
| Senior | 6 | 18.8 | 5 | 16.1 | |
| Graduate | 3 | 9.4 | 3 | 9.7 | |
| Treatment Means | Treatment Effect | |||
|---|---|---|---|---|
| Walnuts | Placebo | Walnuts–Placebo | ||
| Domains/TMD | Mean (95% CI) | Mean (95% CI) | % Change (95% CI) | p-Value |
| Tension-Anxiety | 11.2 (9.3–13.2) | 11.9 (9.9–13.8) | −5.2 (−20.8–10.4) | 0.507 |
| Depression-Dejection | 9.7 (6.7–12.7) | 12.1 (9.1–15.2) | −20.0 (−44.2–4.2) | 0.103 |
| Anger-Hostility | 6.5 (4.7–8.3) | 7.5 (5.7–9.3) | −13.3 (−36.8–10.2) | 0.261 |
| Vigor-Activity | 13.8 (12.2–15.4) | 13.1 (11.5–14.7) | 5.3 (−7.5–18.0) | 0.408 |
| Fatigue-Inertia | 10.2 (8.7–11.7) | 10.1 (8.6–11.6) | 1.1 (−14.3–16.6) | 0.882 |
| Confusion-Bewilderment | 9.5 (8.2–10.8) | 9.5 (8.2–10.8) | 0.0 (−12.6–12.1) | 0.969 |
| Total Mood Disturbance | 33.5 (24.7–42.3) | 37.9 (29.1–46.6) | −11.6 (−32.4–9.2) | 0.267 |
| Treatment Means | Treatment Effect | |||
|---|---|---|---|---|
| Walnuts | Placebo | Walnuts–Placebo | ||
| Domains/TMD | Mean (95% CI) | Mean (95% CI) | % Change (95% CI) | p-Value |
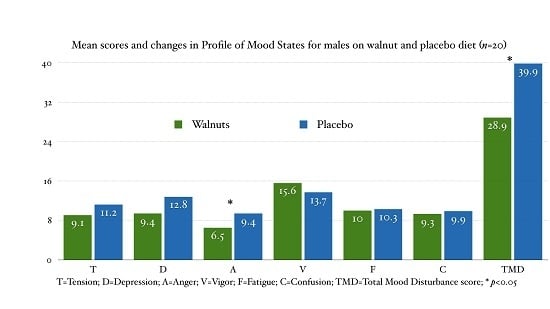
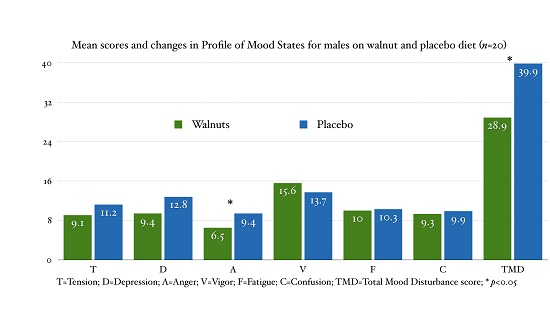
| Tension-Anxiety | 9.1 (6.2–12.0) | 11.2 (8.35–14.0) | −18.6 (−42.4–5.2) | 0.117 |
| Depression-Dejection | 9.4 (4.5–14.4) | 12.9 (8.01–17.7) | −26.5 (−61.9–8.9) | 0.132 |
| Anger-Hostility | 6.5 (3.4–9.6) | 9.4 (6.4–12.5) | −31.2 (−54.9–−7.4) | 0.013 |
| Vigor-Activity | 15.6 (12.9–18.2) | 13.8 (11.18–16.3) | 13.4 (−4.7–31.5) | 0.136 |
| Fatigue-Inertia | 10.0 (7.3–12.8) | 10.3 (7.57–13.1) | −2.8 (−21.2–15.6) | 0.750 |
| Confusion-Bewilderment | 9.3 (6.9–11.7) | 9.9 (7.6–12.3) | −6.4 (−23.0–10.3) | 0.432 |
| Total Mood Disturbance | 28.9 (13.3–44.7) | 39.9 (24.4–55.6) | −27.5 (−54.0–−1.00) | 0.043 |
| Treatment Means | Treatment Effect | |||
|---|---|---|---|---|
| Walnuts | Placebo | Walnuts–Placebo | ||
| Domains/TMD | Mean (95% CI) | Mean (95% CI) | % Change (95% CI) | p-Value |
| Tension-Anxiety | 12.6 (9.9–15.2) | 12.1 (9.5–14.8) | 3.6 (−18.3–25.6) | 0.735 |
| Depression-Dejection | 9.7 (5.7–13.8) | 11.3 (7.1–15.4) | −13.6 (−49.8–22.6) | 0.444 |
| Anger-Hostility | 6.4 (4.0–8.7) | 6.0 (3.6–8.4) | 6.5 (−36.7–49.7) | 0.758 |
| Vigor-Activity | 12.6 (10.5–14.7) | 12.6 (10.4–14.7) | 0.3 (−18.5–19.1) | 0.974 |
| Fatigue-Inertia | 10.1 (8.3–12.0) | 9.9 (8.0–11.8) | 2.2 (−21.7–26.0) | 0.853 |
| Confusion-Bewilderment | 9.6 (8.0–11.2) | 9.1 (7.5–10.8) | 5.1 (−13.9–24.0) | 0.587 |
| Total Mood Disturbance | 35.7 (24.8–46.6) | 35.6 (24.5–46.6) | 0.4 (−32.3–33.0) | 0.982 |
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pribis, P. Effects of Walnut Consumption on Mood in Young Adults—A Randomized Controlled Trial. Nutrients 2016, 8, 668. https://doi.org/10.3390/nu8110668
Pribis P. Effects of Walnut Consumption on Mood in Young Adults—A Randomized Controlled Trial. Nutrients. 2016; 8(11):668. https://doi.org/10.3390/nu8110668
Chicago/Turabian StylePribis, Peter. 2016. "Effects of Walnut Consumption on Mood in Young Adults—A Randomized Controlled Trial" Nutrients 8, no. 11: 668. https://doi.org/10.3390/nu8110668
APA StylePribis, P. (2016). Effects of Walnut Consumption on Mood in Young Adults—A Randomized Controlled Trial. Nutrients, 8(11), 668. https://doi.org/10.3390/nu8110668