Hand-to-Hand Model for Bioelectrical Impedance Analysis to Estimate Fat Free Mass in a Healthy Population

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
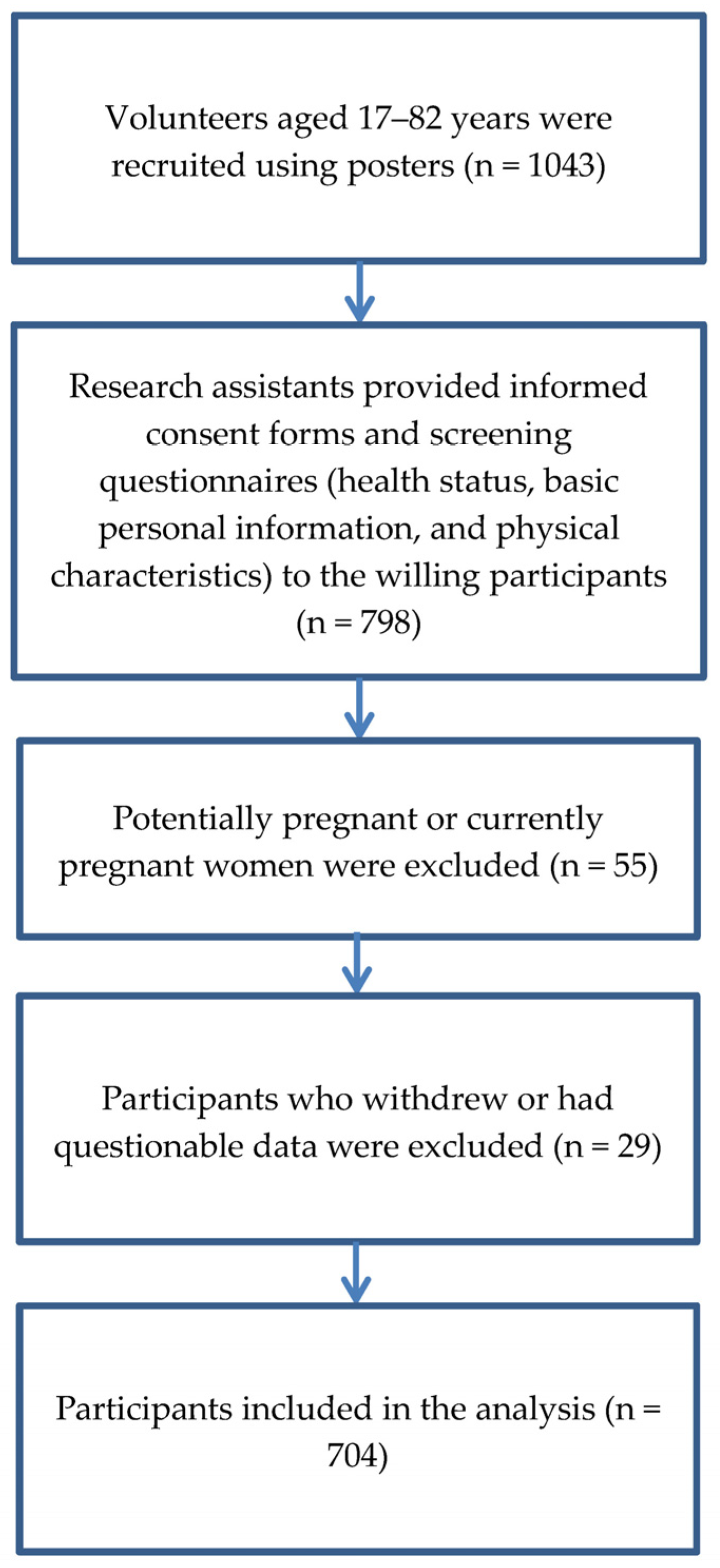
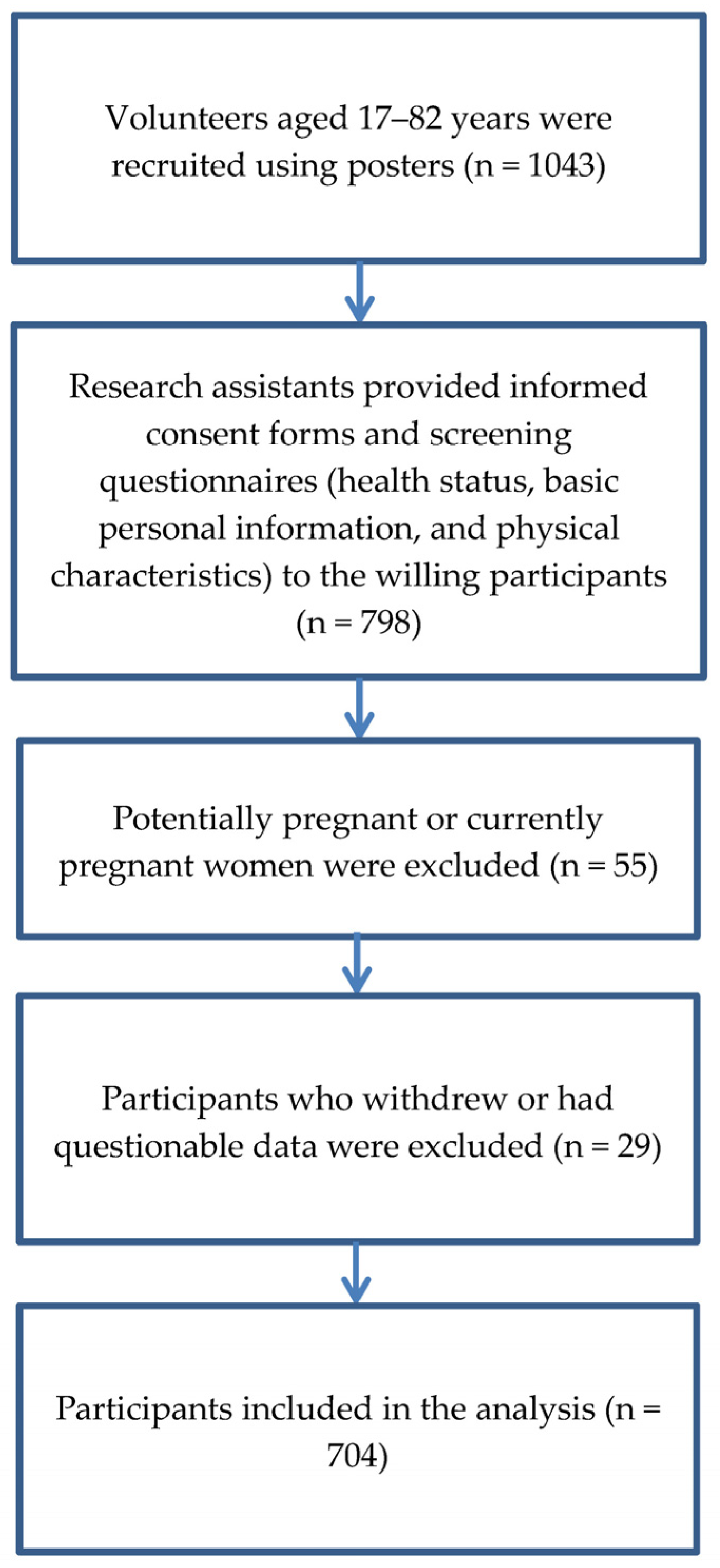
2.1. Participants
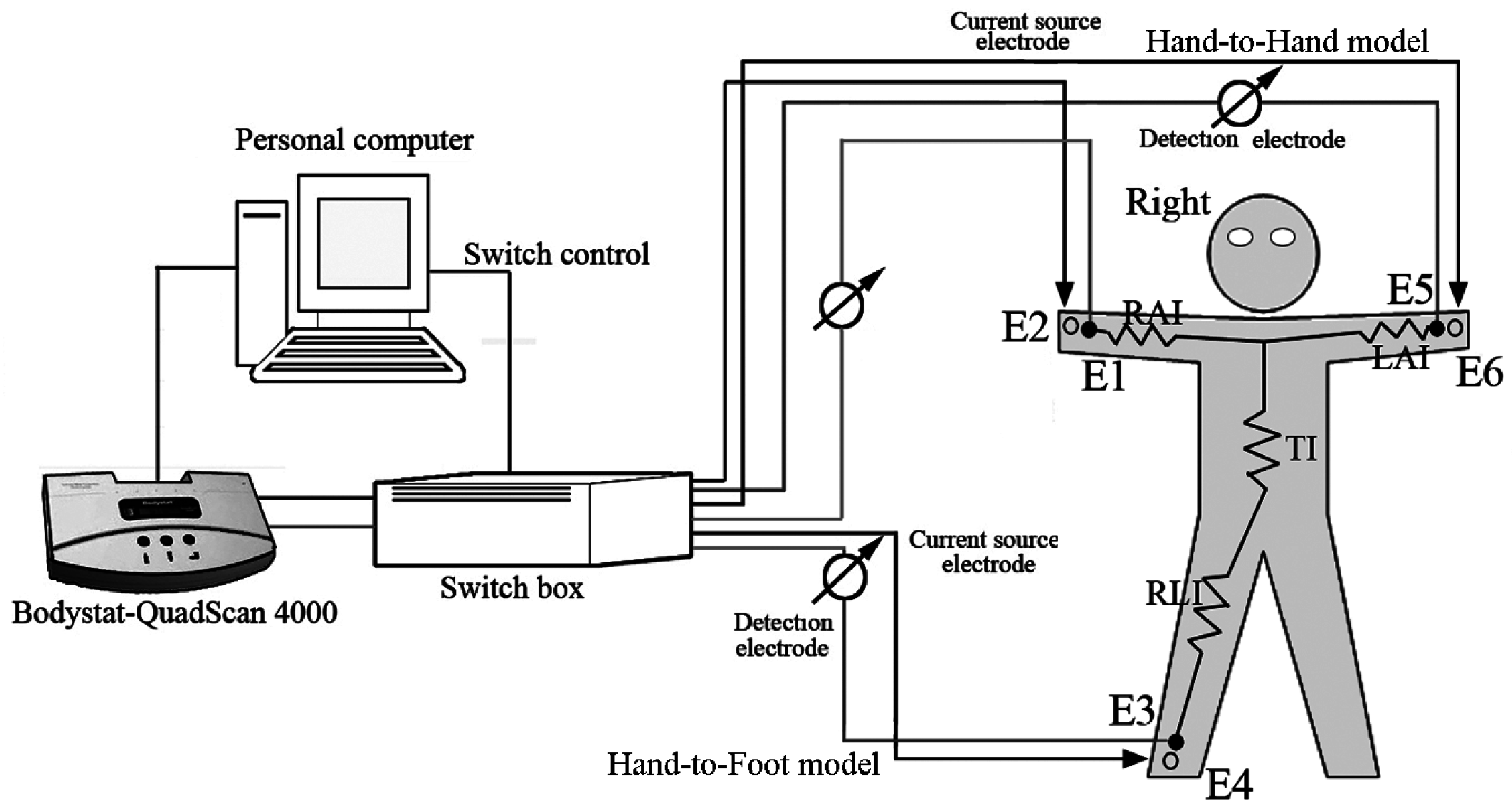
2.2. Impedance Measurements
2.3. Experimental Procedures
2.4. Statistical Analysis
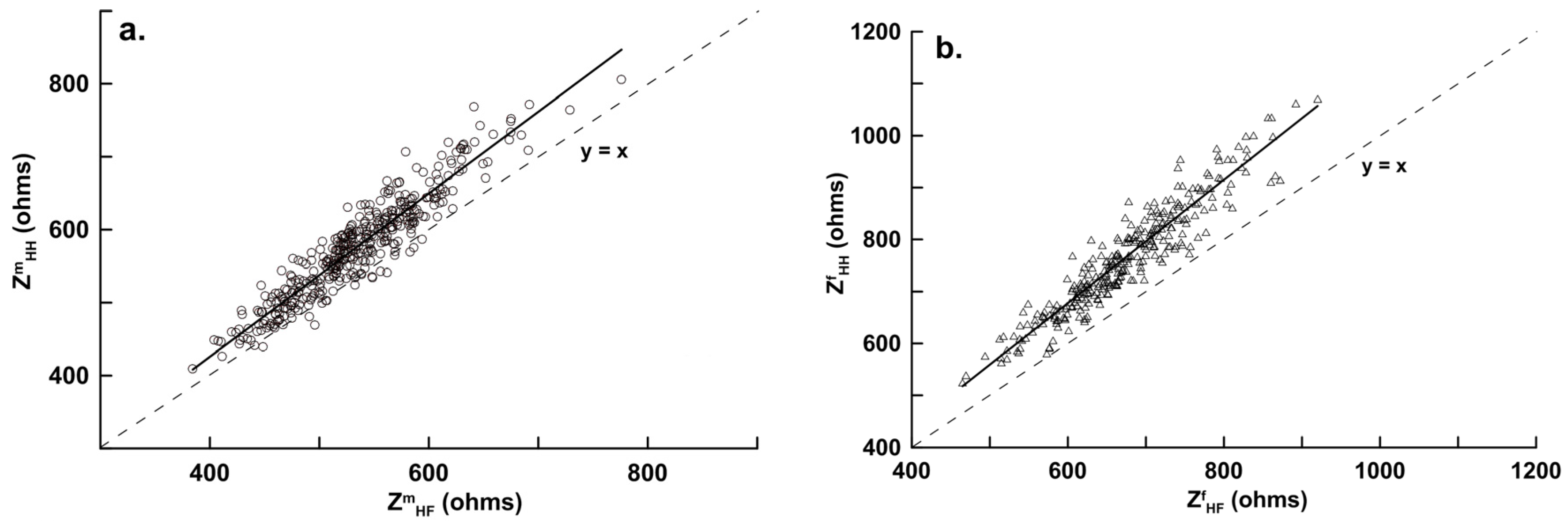
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Malik, S.; Wong, N.D.; Franklin, S.S.; Kamath, T.V.; L’Italien, G.J.; Pio, J.R.; Williams, G.R. Impact of the Metabolic Syndrome on Mortality from Coronary Heart Disease, Cardiovascular Disease, and All Causes in United States Adults. Circulation 2004, 110, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S. New approaches to body composition. Am. J. Clin. Nutr. 1982, 35, 1152–1158. [Google Scholar] [PubMed]
- Stewart, S.P.; Bramley, P.N.; Heighton, R.; Green, J.H.; Horsman, A.; Losowsky, M.S.; Smith, M.A. Estimation of body composition from bioelectrical impedance of body segments: Comparison with dual-energy X-ray absorptiometry. Br. J. Nutr. 1993, 69, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Methods for the assessment of human body composition: Traditional and new. Am. J. Clin. Nutr. 1987, 46, 537–556. [Google Scholar] [PubMed]
- Lukaski, H.C.; Siders, W.A. Validity and accuracy of regional bioelectrical impedance devices to determine whole-body fatness. Nutrition 2003, 19, 851–857. [Google Scholar] [CrossRef]
- Gartner, A.; Dioum, A.; Delpeuch, F.; Maire, B.; Schutz, Y. Use of hand-to-hand impedancemetry to predict body composition of African women as measured by air displacement plethysmography. Eur. J. Clin. Nutr. 2004, 58, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, P.; Deurenberg-Yap, M. Validation of skinfold thickness and hand-held impedance measurements for estimation of body fat percentage among Singaporean Chinese, Malay and Indian subjects. Asia Pac. J. Clin. Nutr. 2002, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bousbiat, S.; Jaffrin, M.Y.; Dongmo, E. Comparison of body fat-free masses calculated from hand-to-foot and foot-to-foot resistances with DXA measurements. Med. Biol. Eng. Comput. 2011, 49, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Lintsi, M.; Kaarma, H.; Kull, I. Comparison of hand-to-hand bioimpedance and anthropometry equations versus dual-energy X-ray absorptiometry for the assessment of body fat percentage in 17–18-year-old conscripts. Clin. Physiol. Funct. Imaging 2004, 24, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Esoc, R.M.; Olson, M.S.; Williford, H.N.; Lizana, S.N.; Russell, A.R. The accuracy of hand-to-hand bioelectrical impedance analysis in predicting body composition in college-age female athletes. J. Strength Cond. Res. 2011, 25, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Lazzer, S.; Boirie, Y.; Meyer, M.; Vermorel, M. Evaluation of two foot-to-foot bioelectrical impedance analysers to assess body composition in overweight and obese adolescents. Br. J. Nutr. 2003, 90, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Academic: New York, NY, USA, 1998. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Macias, N.; Alemán-Mateo, H.; Esparza-Romero, J.; Valencia, M.E. Body fat measurement by bioelectrical impedance and air displacement plethysmography: A cross-validation study design bioelectrical impedance equations in Mexican adults. Nutr. J. 2007, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Ludbrook, J. Statistical techniques for comparing measurers and methods of measurement: A critical review. Clin. Exp. Pharmacol. Physiol. 2002, 29, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Demura, S.; Yamaji, S.; Goshi, F.; Nagasawa, Y. The influence of posture change on measurements of relative body fat in the bioimpedance analysis method. J. Physiol. Anthropol. Appl. Hum. Sci. 2001, 20, 29–35. [Google Scholar] [CrossRef]
- Organ, L.W.; Bradham, G.B.; Gore, D.T.; Lozier, S.L. Segmental bioelectrical impedance analysis: Theory and application of a new technique. J. Appl. Physiol. 1994, 77, 98–112. [Google Scholar] [PubMed]
- Wang, J.; Deurenberg, P. The validity of predicted body composition in Chinese adults from anthropometry and bioelectrical impedance in comparison with densitometry. Br. J. Nutr. 1996, 76, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, P.; van der Kooy, K.; Leenen, R.; Weststrate, J.A.; Seidell, J.C. Sex and age specific prediction formulas for estimating body composition from bioelectrical impedance: A cross validation study. Int. J. Obes. 1991, 15, 17–25. [Google Scholar] [PubMed]
- Kyle, U.G.; Genton, L.; Karsegard, L.; Slosman, D.O.; Pichard, C. Single prediction equation for bioelectrical impedance analysis in adults aged 20–94 years. Nutrition 2001, 17, 248–253. [Google Scholar] [CrossRef]
- Houtkooper, L.B.; Lohman, T.G.; Going, S.B.; Howell, W. Why bioelectrical impedance analysis should be used for estimating adiposity. Am. J. Clin. Nutr. 1996, 64, S436–S448. [Google Scholar]
- Sun, S.S.; Chumlea, W.C.; Heymsfield, S.B.; Lukaski, H.C.; Schoeller, D.; Friedl, K.; Kuczmarski, R.J.; Flegal, K.M.; Johnson, C.L.; Hubbard, V.S. Development of bioelectrical impedance analysis prediction equations for body composition with the use of a multicomponent model for use in epidemiologic surveys. Am. J. Clin. Nutr. 2003, 77, 331–340. [Google Scholar] [PubMed]
- Xie, X.; Kolthoff, N.; Bärenholt, O.; Nielsen, S.P. Validation of a leg-to-leg bioimpedance analysis system in assessing body composition in postmenopausal women. Int. J. Obes. Metab. Disord. 1999, 23, 1079–1084. [Google Scholar] [CrossRef]
- Le Donne, M.; Metro, D.; Anoldo, R.; de Meo, L.; La Galia, T.; Muraca, U.; Cancellieri, F. Body composition estimated by bioimpedance analysis in Sicilian climacteric women. Minerva Ginecol. 2008, 60, 311–316. [Google Scholar] [PubMed]
- Nuñez, C.; Gallagher, D.; Visser, M.; Pi-Sunyer, F.X.; Wang, Z.; Heymsfield, S.B. Bioimpedance analysis: Evaluation of leg-to-leg system based on pressure contact footpad electrodes. Med. Sci. Sports Exerc. 1997, 29, 524–531. [Google Scholar] [PubMed]
- Kotler, D.P.; Burastero, S.; Wang, J.; Pierson, R.N., Jr. Prediction of body cell mass, fat-free mass, and total body water with bioelectrical impedance analysis: Effects of race, sex, and disease. Am. J. Clin. Nutr. 1996, 64 (Suppl. 3), 489s–497s. [Google Scholar] [PubMed]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [PubMed]
- Hannan, W.J.; Cowen, S.J.; Fearon, K.C.; Plester, C.E.; Falconer, J.S.; Richardson, R.A. Evaluation of multi-frequency bio-impedance analysis for the assessment of extracellular and total body water in surgical patients. Clin. Sci. 1994, 86, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.A.; Lobo, D.N.; Anderson, J.A.; Macdonald, I.A.; Perkins, A.C.; Neal, K.R.; Allison, S.P.; Rowlands, B.J. Body water compartment measurements: A comparison of bioelectrical impedance analysis with tritium and sodium bromide dilution techniques. Clin. Nutr. 2001, 20, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Dittmar, M.; Reber, H. New equation for estimating body cell mass from bio-impedance parallel models in healthy older Germans. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E1005–E1014. [Google Scholar] [PubMed]
- Maw, G.J.; Mackenzie, I.L.; Taylor, N.A. Redistribution of body fluids during postural manipulations. Acta Physiol. Scand. 1995, 155, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.C.; Crowley, J.; Freitas, I.F.; Luke, A. Validity of Hand-to-foot measurement of bioimpedance: Standing compared with lying position. Obesity 2006, 14, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Oshima, Y.; Shiag, T. Within-day variability of whole-body and segmental bioelectrical impedance in a standing position. Eur. J. Clin. Nutr. 2006, 60, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; de Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Lilienthal Heitmann, B.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Mazess, R.B.; Barden, H.S.; Bisek, J.P.; Hanson, J. Dual-energy X-ray absorptiometry for total-body and regional bone-mineral and soft-tissue composition. Am. J. Clin. Nutr. 1990, 51, 1106–1112. [Google Scholar] [PubMed]
- Williams, J.E.; Wells, J.C.K.; Wilson, C.M.; Haroun, D.; Lucas, A.; Fewtrell, M.S. Evaluation of Lunar Prodigy dual-energy X-ray absorptiometry for assessing body composition in healthy persons and patients by comparison with the criterion 4-component model. Am. J. Clin. Nutr. 2006, 83, 1047–1054. [Google Scholar] [PubMed]
- Lohman, T.G.; Harris, M.; Teixeira, P.J.; Weiss, L. Assessing body composition and changes in body composition: Another look at dual-energy X-ray absorptiometry. Ann. N. Y. Acad. Sci. 2000, 904, 45–54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Mean ± SD | Range | Mean ± SD | Range | p |
|---|---|---|---|---|---|
| Male (n = 403) | Female (n = 301) | ||||
| Age (years) | 33.1 ± 17.0 | 17.0–81.5 | 37.5 ± 16.1 | 17.1–77.6 | <0.01 |
| Height (cm) | 172.5 ± 7.5 | 151.5–200.0 | 159.6 ± 6.8 | 142.5–178.0 | <0.001 |
| Weight (kg) | 74.0 ± 13.1 | 42.0–133.8 | 60.0 ± 12.2 | 38.0–108.3 | <0.001 |
| BMI (kg/m2) | 24.8 ± 3.7 | 16.8–41.8 | 23.6 ± 4.5 | 15.8–42.7 | <0.05 |
| DXA | |||||
| FFMDXA (kg) | 58.5 ± 8.1 | 35.6–92.9 | 39.9 ± 5.5 | 28.4–58.7 | <0.001 |
| BF%DXA (%) | 20.9 ± 8.9 | 5.1–41.5 | 33.7 ± 9.5 | 10.4–56.6 | <0.001 |
| Bioimpedance | |||||
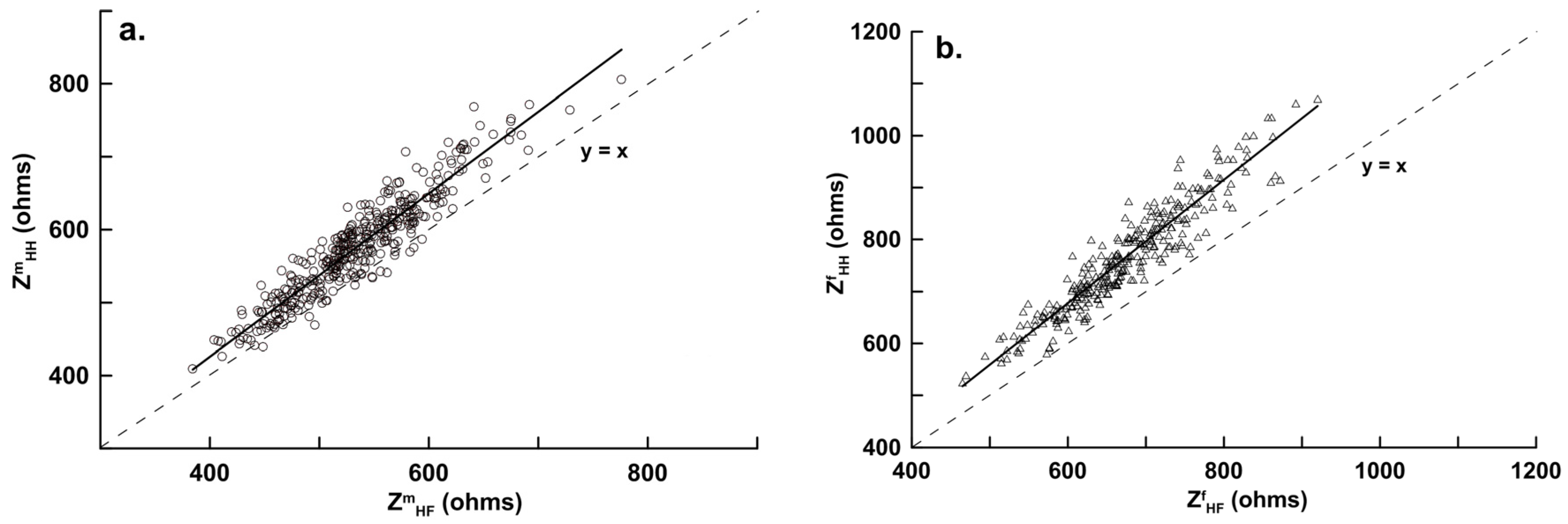
| Z5,HF (Ω) | 594.1 ± 60.3 | 423.3–834.3 | 763.4 ± 107.7 | 512.6–982.2 | <0.001 |
| Z5,HH (Ω) | 654.4 ± 76.4 | 450.3–852.0 | 860.9 ± 83.2 | 355.5–1103.4 | <0.001 |
| Z50,HF (Ω) | 533.4 ± 58.6 | 384.3–776.0 | 673.3 ± 80.8 | 465.0–920.0 | <0.001 |
| Z50,HH (Ω) | 576.3 ± 69.9 | 409.7–806.0 | 764.8 ± 101.7 | 525.0–1071.0 | <0.001 |
| Z100HF (Ω) | 482.7 ± 55.3 | 261.2–743.0 | 632.4 ± 95.1 | 434.1–888.3 | <0.001 |
| Z100,HH (Ω) | 532.9 ± 79.2 | 366.5–703.0 | 715.8 ± 95.2 | 394.3–943.4 | <0.001 |
| R50,HF (Ω) | 529.3 ± 58.2 | 380.2–774.0 | 669.2 ± 98.9 | 461.7–916.3 | <0.001 |
| R50,HH (Ω) | 562.1 ± 60.3 | 386.7–740.3 | 754.3 ± 99.5 | 452.3–1005.6 | <0.001 |
| X50,HF (Ω) | 64.3 ± 7.5 | 33.2–110.1 | 73.1 ± 8.9 | 42.5–114.5 | <0.001 |
| X50,HH (Ω) | 86.5 ± 8.9 | 49.4–131.8 | 103.2 ± 12.3 | 47.5–176.4 | <0.001 |
| PhA50,HF (deg) | 6.9 ± 0.8 | 4.1–9.2 | 6.2 ± 0.7 | 4.2–8.8 | <0.001 |
| PhA50,HH (deg) | 8.7 ± 1.1 | 6.0–10.8 | 7.8 ± 1.2 | 4.5–9.7 | <0.001 |
| BIA | |||||
| FFMHF (kg) | 58.5 ± 7.1 & | 39.0–86.6 | 39.9 ± 4.9 & | 29.1–56.2 | <0.001 |
| FFMHH (kg) | 58.5 ± 7.5 #,& | 37.9–89.3 | 39.9 ± 4.8 #,& | 28.9–54.6 | <0.001 |
| Modeling group | Male (n = 269) | Female (n = 201) | |||
| Age (years) | 32.6 ± 16.5 | 17.2–78.8 | 37.3 ± 16.2 | 17.1–74.8 | <0.01 |
| Height (cm) | 172.6 ± 7.4 | 153.0–200.0 | 159.7 ± 6.8 | 142.5–176.0 | <0.001 |
| Weight (kg) | 74.1 ± 13.9 | 42.0–133.8 | 59.9 ± 11.9 | 38.0–107.4 | <0.001 |
| BMI (kg/m2) | 24.8 ± 3.6 | 16.8–39.9 | 23.5 ± 4.5 | 15.8–37.8 | <0.05 |
| DXA | |||||
| FFMDXA (kg) | 58.7 ± 7.6 | 35.6–87.4 | 39.9 ± 5.2 | 28.4–58.7 | <0.001 |
| BF%DXA (%) | 20.9 ± 8.7 | 5.1–41.0 | 33.5 ± 9.4 | 13.5–56.6 | <0.001 |
| Bioimpedance | |||||
| Z50,HF (Ω) | 530.4 ± 59.0 | 384.3–776.0 | 674.7 ± 84.6 | 465.0–920.0 | <0.001 |
| Z50,HH (Ω) | 572.2 ± 69.7 | 409.7–806.0 | 766.1 ± 106.1 | 525.0–1071.0 | <0.001 |
| BIA | |||||
| FFMHF (kg) | 58.7 ± 7.0 & | 39.0–86.6 | 39.9 ± 4.8 & | 29.1–56.2 | <0.001 |
| FFMHH (kg) | 58.8 ± 7.4 #,& | 37.9–89.3 | 40.0 ± 4.8 #,& | 29.5–54.6 | <0.001 |
| Validation Group | Male (n = 134) | Female (n = 100) | |||
| Age (years) | 34.0 ± 18.0 | 15.3–81.5 | 38.0 ± 16.1 | 17.2–77.6 | <0.01 |
| Height (cm) | 172.5 ± 7.6 | 151.5–193.0 | 159.4 ± 6.8 | 143.0–178.0 | <0.001 |
| Weight (kg) | 73.9 ± 13.5 | 52.0–131.0 | 60.3 ± 12.8 | 42.0–108.3 | <0.001 |
| BMI (kg/m2) | 24.8 ± 3.8 | 18.7–41.8 | 23.7 ± 4.4 | 17.4–42.7 | <0.05 |
| DXA | |||||
| FFMDXA (kg) | 58.0 ± 7.7 | 42.0–86.6 | 40.0 ± 5.2 | 28.9–56.5 | <0.001 |
| BF%DXA (%) | 21.1 ± 9.4 | 5.1–41.0 | 34.2 ± 9.5 | 9.4–54.3 | <0.001 |
| Bioimpedance | |||||
| Z50,HF (Ω) | 539.2 ± 57.4 | 407.7–729.0 | 670.7 ± 73.1 | 517.3–856.5 | <0.001 |
| Z50,HH (Ω) | 584.4 ± 69.7 | 439.3–769.0 | 762.0 ± 92.8 | 583.0–1035.5 | <0.001 |
| BIA | |||||
| FFMHF (kg) | 57.9 ± 7.4 & | 40.5–82.8 | 39.8 ± 5.1 & | 29.0–54.5 | <0.001 |
| FFMHH (kg) | 57.8 ± 7.5 #,& | 40.0–83.7 | 39.8 ± 5.1 #,& | 28.6–54.1 | <0.001 |
| h2/Z | Age | Weight | Gender | Intercept | SEE (kg) | r2 | VIF | β |
|---|---|---|---|---|---|---|---|---|
| FFMHH, Total subjects (n = 704) | ||||||||
| 0.948 ± 0.011 * | - | - | - | 8.273 ± 0.500 * | 3.304 | 0.915 | 6.18 | 0.56 |
| 0.912 ± 0.009 * | −0.107 ± 0.006 * | - | - | 13.629 ± 0.524 * | 2.805 | 0.939 | 1.10 | −0.19 |
| 0.784 ± 0.013 * | −0.118 ± 0.006 * | 0.131 ± 0.101 * | - | 10.813 ± 0.527 * | 2.520 | 0.951 | 2.68 | 0.23 |
| 0.556 ± 0.017 * | −0.131 ± 0.005 * | 0.184 ± 0.009 * | 4.967 ± 0.293 * | 14.955 ± 0.507 * | 2.124 | 0.965 | 3.29 | 0.22 |
| FFMHF, Total subjects (n = 704) | ||||||||
| 0.962 ± 0.010 * | - | - | - | 3.562 ± 0.515 * | 3.092 | 0.926 | 6.46 | 0.58 |
| 0.927 ± 0.009 * | −0.096 ± 0.006 * | - | - | 8.626 ± 0.552 * | 2.670 | 0.945 | 1.36 | −0.18 |
| 0.813 ± 0.014 * | −0.122 ± 0.005 * | 3.233 ± 0.315 * | 12.585 ± 0.643 * | 2.491 | 0.952 | 3.18 | 0.22 | |
| 0.583 ± 0.017 * | −0.122 ± 0.005 * | 0.163 ± 0.009 * | 5.058 ± 0.281 * | 16.917 ± 0.800 * | 2.072 | 0.967 | 2.92 | 0.21 |
| FFMmHH, Male subjects (n = 269) | ||||||||
| 0.881 ± 0.026 * | - | - | - | 12.062 ± 1.389 * | 3.304 | 0.812 | 2.41 | 0.55 |
| 0.816 ± 0.024 * | −0.103 ± 0.011 * | - | - | 18.864 ± 1.413 * | 2.873 | 0.858 | 1.36 | −0.27 |
| 0.537 ± 0.026 * | −0.126 ± 0.009 * | 0.217 ± 0.015 * | - | 18.235 ± 1.066 * | 2.164 | 0.919 | 2.22 | 0.37 |
| FFMmHF, Male subjects (n = 269) | ||||||||
| 0.870 ± 0.026 * | - | - | - | 9.168 ± 1.465 * | 3.285 | 0.813 | 2.49 | 0.55 |
| 0.806 ± 0.023 * | −0.103 ± 0.011 * | - | - | 16.151 ± 1.482 * | 2.862 | 0.859 | 1.14 | −0.27 |
| 0.532 ± 0.027 * | −0.126 ± 0.009 * | 0.213 ± 0.016 * | - | 16.663 ± 1.144 * | 2.208 | 0.916 | 2.29 | 0.36 |
| FFMfHH, Female subjects (n = 201) | ||||||||
| 0.821 ± 0.044 * | - | - | - | 12.089 ± 1.495 * | 3.138 | 0.640 | 2.08 | 0.60 |
| 0.836 ± 0.030 * | −0.140 ± 0.019 * | - | - | 16.778 ± 1.082 * | 2.172 | 0.828 | 1.05 | −0.45 |
| 0.615 ± 0.038 * | −0.144 ± 0.008 * | 0.132 ± 0.016 * | - | 16.507 ± 0.939 * | 1.884 | 0.870 | 2.08 | 0.30 |
| FFMfHF, Female subjects (n = 201) | ||||||||
| 0.831 ± 0.036 * | - | - | - | 8.020 ± 1.389 * | 2.720 | 0.730 | 2.31 | 0.67 |
| 0.818 ± 0.025 * | −0.121 ± 0.008 * | - | - | 13.036 ± 1.024 * | 1.890 | 0.869 | 1.02 | −0.40 |
| 0.651 ± 0.035 * | −0.128 ± 0.008 * | 0.100 ± 0.016 * | - | 13.675 ± 0.940 * | 1.724 | 0.891 | 2.32 | 0.23 |
| Modeling Group | Male (n = 269) | |
|---|---|---|
| Measured FFMDXA | 58.7 ± 7.6 kg | |
| Validation Group | Male (n = 134) | |
| Measured FFMDXA | 58.0 ± 7.7 kg | |
| Prediction FFMmHH | 0.537 h2/ZmHH − 0.126 yr + 0.217 w + 18.235, (r2 = 0.919, SEE = 2.164 kg, n = 269) | (1a) |
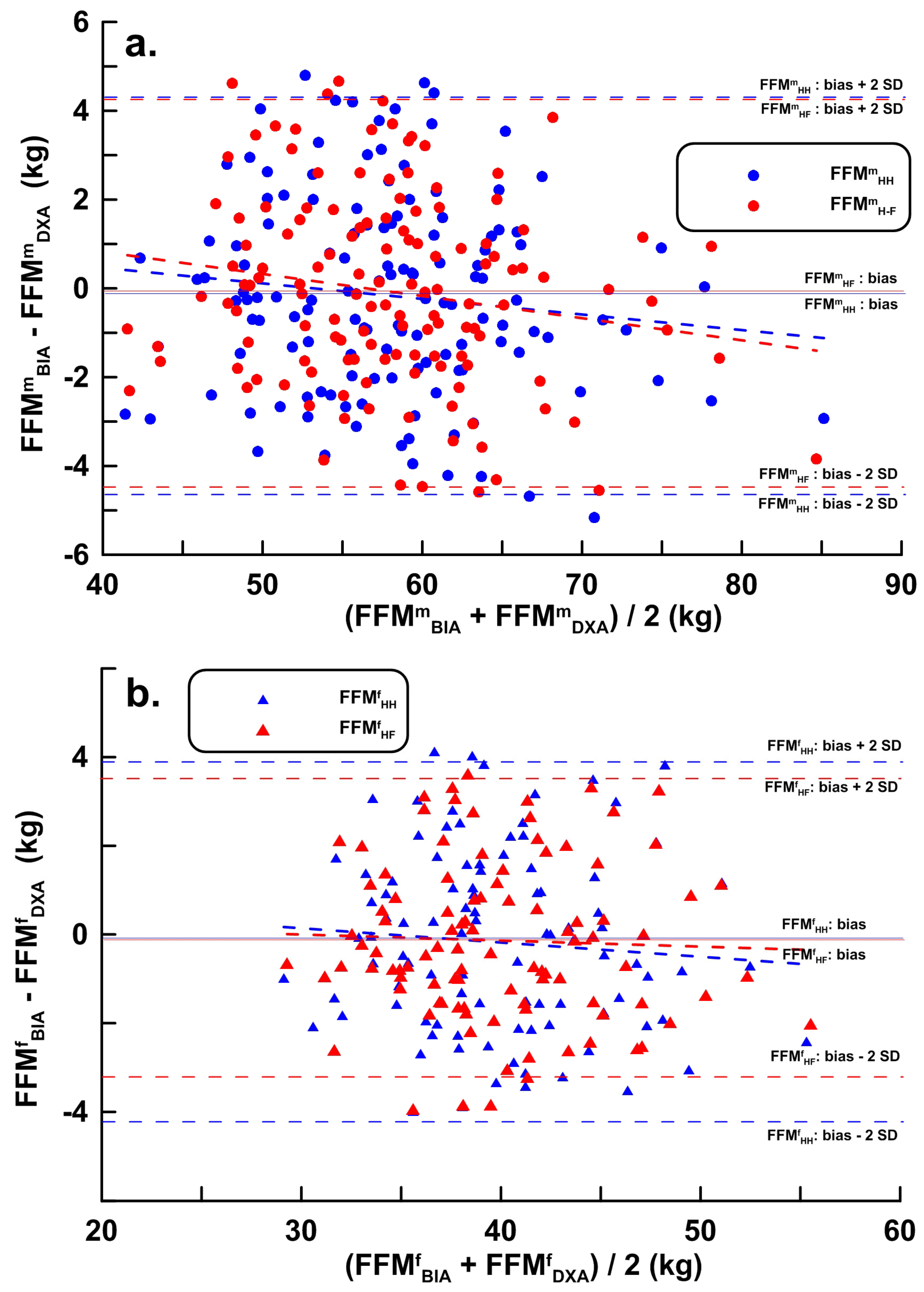
| Using Validation group FFMmHH | 57.8 ± 7.5 kg, r = 0.957, LOA = −4.616–4.289 kg, PE = 2.224 kg, bias = −0.164 kg | |
| Prediction FFMmHF | 0.532 h2/ZmHF − 0.126 yr + 0.213 w + 16.663, (r2 = 0.916, SEE = 2.208 kg, n = 269) | (1b) |
| Using Validation group FFMmHF | 57.9 ± 7.4 kg, r = 0.960, LOA = −4.395–4.255 kg, PE = 2.156 kg, bias = −0.070 kg | |
| Modeling Group | Female (n = 201) | |
| Measured FFMDXA | 39.9 ± 5.2 kg | |
| Validation Group | Female (n = 100) | |
| Measured FFMDXA | 40.0 ± 5.2 kg | |
| Prediction FFMfHH | 0.615 h2/ZmHH − 0.144 yr + 0.132 w + 16.507, (r2 = 0.870, SEE = 1.884 kg, n = 201) | (2a) |
| Using Validation group FFMfHH | 39.8 ± 5.1 kg, r = 0.921, LOA = −4.271–3.916 kg, PE = 2.044 kg, bias = −0.178 kg | |
| Prediction FFMfHF | 0.651 h2/ZmHH − 0.128 yr + 0.100 w + 13.675, (r2 = 0.891, SEE = 1.724 kg, n = 201) | (2b) |
| Using Validation group FFMfHF | 39.8 ± 5.1 kg, r = 0.939, LOA = −3.750–3.476 kg, PE = 1.803kg, bias = −0.137 kg | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, H.-K.; Chiang, L.-M.; Chen, Y.-Y.; Chuang, C.-L.; Chen, K.-T.; Dwyer, G.B.; Hsu, Y.-L.; Chen, C.-H.; Hsieh, K.-C. Hand-to-Hand Model for Bioelectrical Impedance Analysis to Estimate Fat Free Mass in a Healthy Population. Nutrients 2016, 8, 654. https://doi.org/10.3390/nu8100654
Lu H-K, Chiang L-M, Chen Y-Y, Chuang C-L, Chen K-T, Dwyer GB, Hsu Y-L, Chen C-H, Hsieh K-C. Hand-to-Hand Model for Bioelectrical Impedance Analysis to Estimate Fat Free Mass in a Healthy Population. Nutrients. 2016; 8(10):654. https://doi.org/10.3390/nu8100654
Chicago/Turabian StyleLu, Hsueh-Kuan, Li-Ming Chiang, Yu-Yawn Chen, Chih-Lin Chuang, Kuen-Tsann Chen, Gregory B. Dwyer, Ying-Lin Hsu, Chun-Hao Chen, and Kuen-Chang Hsieh. 2016. "Hand-to-Hand Model for Bioelectrical Impedance Analysis to Estimate Fat Free Mass in a Healthy Population" Nutrients 8, no. 10: 654. https://doi.org/10.3390/nu8100654
APA StyleLu, H.-K., Chiang, L.-M., Chen, Y.-Y., Chuang, C.-L., Chen, K.-T., Dwyer, G. B., Hsu, Y.-L., Chen, C.-H., & Hsieh, K.-C. (2016). Hand-to-Hand Model for Bioelectrical Impedance Analysis to Estimate Fat Free Mass in a Healthy Population. Nutrients, 8(10), 654. https://doi.org/10.3390/nu8100654