Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Explanatory Variable: Dietary Intake of Vitamin K
2.3. Dependent Variables: Neuropsychiatric Measures
2.4. Covariables
2.5. Statistical Analysis
3. Results


{kind=link}
| Total Cohort (n = 192) | Dietary Phylloquinone Intake * | p-Value | ||
|---|---|---|---|---|
| <207 µg/day (n = 64) | ≥207 µg/day (n = 128) | |||
| Demographical measures | ||||
| Age, years | 82.8 ± 7.1 | 83.7 ± 5.9 | 82.4 ± 7.7 | 0.227 |
| Female gender, n (%) | 120 (62.5) | 43 (67.2) | 77 (60.2) | 0.343 |
| Social problems, n (%) | 21 (10.9) | 10 (15.6) | 11 (8.6) | 0.141 |
| High education level †, n (%) | 152 (79.2) | 51 (79.7) | 101 (78.9) | 0.900 |
| Clinical measures | ||||
| Body mass index, kg/m2 | 26.2 ± 5.4 | 25.8 ± 4.9 | 26.4 ± 5.6 | 0.492 |
| CIRS-G score, /60 | 8.3 ± 4.0 | 9.0 ± 4.4 | 8.0 ± 3.8 | 0.118 |
| History of stroke, n (%) | 29 (15.2) | 10 (15.6) | 19 (15.0) | 0.904 |
| Use of vitamin K antagonists, n (%) | 31 (16.1) | 11 (17.2) | 20 (15.6) | 0.781 |
| Dietary intake of phylloquinone, µg/day | 319.9 ± 196.3 | 125.3 ± 52.1 | 417.1 ± 167.4 | <0.001 |
| Low dietary intake of fatty fish and eggs ‡, n (%) | 23 (12.2) | 9 (14.8) | 14 (10.9) | 0.453 |
| Neuropsychiatric measures | ||||
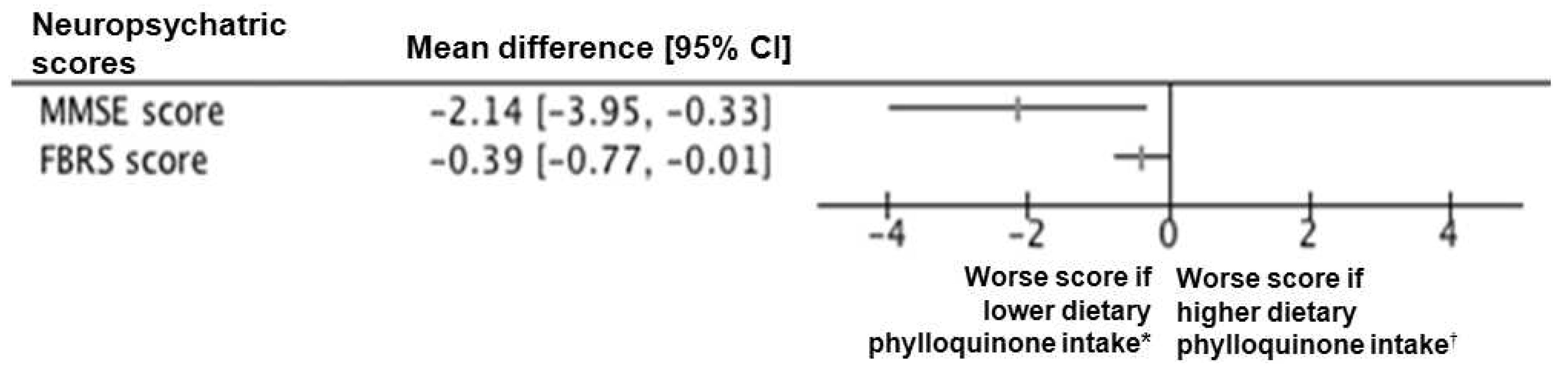
| MMSE score, /30 | 21.4 ± 5.9 | 19.9 ± 6.2 | 22.0 ± 5.7 | 0.024 |
| FBRS score, /4 | 1.6 ± 1.2 | 1.9 ± 1.3 | 1.5 ± 1.2 | 0.042 |
| Serum measures | ||||
| TSH concentration, mIU/L | 1.6 ± 1.8 | 1.5 ± 1.2 | 1.7 ± 2.0 | 0.440 |
| Vitamin B12 concentration, ng/L | 444.3 ± 266.2 | 478.5 ± 375.8 | 427.4 ± 190.6 | 0.228 |
| Albumin concentration, g/L | 34.9 ± 5.5 | 33.0 ± 5.7 | 35.9 ± 5.2 | 0.001 |
| Estimated glomerular filtration rate, mL/min | 53.7 ± 21.9 | 50.8 ± 18.2 | 55.1 ± 23.5 | 0.217 |
| Neuropsychiatric Measures | ||||||
|---|---|---|---|---|---|---|
| MMSE Score | FBRS Score | |||||
| β | (95% CI) | p-value | β | (95% CI) | p-value | |
| Log dietary phylloquinone intake | 1.66 | (0.36; 2.95) | 0.013 | −0.33 | (−0.63; −0.02) | 0.037 |
| Age | −0.22 | (−0.39; −0.06) | 0.009 | 0.02 | (−0.03; 0.06) | 0.450 |
| Female gender | −0.63 | (−2.46; 1.19) | 0.492 | −0.01 | (−0.47; 0.44) | 0.953 |
| Social problems | 2.75 | (−0.31; 5.82) | 0.078 | 0.10 | (−0.63; 0.83) | 0.792 |
| High education level † | 2.52 | (0.27; 4.77) | 0.029 | −0.11 | (−0.67; 0.45) | 0.691 |
| Body mass index | 0.02 | (−0.18; 0.23) | 0.842 | 0.02 | (−0.04; 0.07) | 0.561 |
| CIRS-G score | −0.14 | (−0.41; 0.13) | 0.312 | 0.03 | (−0.04; 0.09) | 0.441 |
| History of stroke | −1.56 | (−4.26; 1.13) | 0.253 | 0.38 | (−0.27; 1.02) | 0.248 |
| Use of vitamin K antagonists | −0.07 | (−2.69; 2.56) | 0.628 | −0.10 | (−0.75; 0.56) | 0.773 |
| Low dietary intake of fatty fish and eggs ‡ | −0.09 | (−2.83; 2.65) | 0.948 | 0.63 | (−0.06; 1.31) | 0.072 |
| TSH concentration | 0.76 | (0.02; 1.49) | 0.044 | 0.06 | (−0.13; 0.24) | 0.556 |
| Vitamin B12 concentration | −0.00 | (−0.01; 0.00) | 0.513 | 0.00 | (0.00; 0.00) | 0.281 |
| Albumin concentration | 0.24 | (0.04; 0.43) | 0.018 | 0.01 | (−0.04; 0.06) | 0.698 |
| Estimated glomerular filtration rate | −0.02 | (−0.07; 0.04) | 0.567 | −0.01 | (−0.02; 0.01) | 0.242 |
| Characteristics | 1. | 2. | 3. | 4. | 5. |
|---|---|---|---|---|---|
| 1. Log dietary phylloquinone intake | - | −0.14 | −0.24 ** | −0.09 | −0.03 |
| 2. Self-control disorders | - | 0.16 * | 0.29 *** | 0.32 *** | |
| 3. Physical neglect | - | 0.14 | 0.25 *** | ||
| 4. Mood disorders | - | 0.35 *** | |||
| 5. Lower general interest | - |
4. Discussion
5. Conclusions
Acknowledgments
Authors Contribution
Conflicts of Interest
References
- Suttie, J.W. Vitamin K in Health and Disease; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Ferland, G. Vitamin K, an emerging nutrient in brain function. Biofactors 2012, 38, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Ferland, G. Vitamin K and the nervous system: An overview of its actions. Adv. Nutr. 2012, 3, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.G.; Pauli, R.M.; Wilson, K.M. Maternal and fetal sequelae of anticoagulation during pregnancy. Am. J. Med. 1980, 68, 122–140. [Google Scholar] [CrossRef]
- Presse, N.; Belleville, S.; Gaudreau, P.; Greenwood, C.E.; Kergoat, M.J.; Morais, J.A.; Payette, H.; Shatenstein, B.; Ferland, G. Vitamin K status and cognitive function in healthy older adults. Neurobiol. Aging 2013, 34, 2777–2783. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Ferland, G.; Barberger-Gateau, P.; Brangier, A.; Rolland, Y.; Beauchet, O. Vitamin K antagonists and cognitive impairment: Results from a cross-sectional pilot study among geriatric patients. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Denis, S.; Duval, G.; Ferland, G.; Bartha, R.; Beauchet, O. Use of vitamin K antagonists and brain volumetry in seniors: Preliminary results from the GAIT study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, (in press). [Google Scholar]
- Sato, Y.; Honda, Y.; Hayashida, N.; Iwamoto, J.; Kanoko, T.; Satoh, K. Vitamin K deficiency and osteopenia in elderly women with Alzheimer’s disease. Arch. Phys. Med. Rehabil. 2005, 86, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Kergoat, M.J.; Reid, I. Poor nutrient intakes during 1-year follow-up with community-dwelling older adults with early stage Alzheimer dementia compared to cognitively intact matched controls. J. Am. Diet Assoc. 2007, 107, 2091–2099. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Honda, Y.; Hayashida, N.; Iwamoto, J.; Kanoko, T.; Satoh, K. Low vitamin K intakes in community-dwelling elders at an early stage of Alzheimer’s disease. J. Am. Diet Assoc. 2008, 108, 2095–2099. [Google Scholar]
- Allison, A.C. The possible role of vitamin K deficiency in the pathogenesis of Alzheimer’s disease and in augmenting brain damage associated with cardiovascular disease. Med. Hypotheses 2001, 57, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Presse, N.; Shatenstein, B.; Kergoat, M.J.; Ferland, G. Validation of a semi-quantitative food frequency questionnaire measuring dietary vitamin K intake in elderly people. J. Am. Diet Assoc. 2009, 109, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Lebert, F.; Pasquier, F.; Souliez, L.; Petit, H. Frontotemporal behavioral scale. Alzheimer Dis. Assoc. Disord. 1998, 12, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Hatano, S. Experience from a multicentre stroke register: A preliminary report. Bull World Health Organ. 1976, 54, 541–553. [Google Scholar] [PubMed]
- Chevallereau, G.; Gleyses, X.; Roussel, L.; Hamdan, S.; Beauchet, O.; Annweiler, C. Proposal and validation of a quick question to rate the influence of diet in geriatric epidemiological studies on vitamin D. Int. J. Vitam Nutr. Res. 2013, 83, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Ascherio, A.; Grodstein, F. Fruit and vegetable consumption and cognitive decline in aging women. Ann. Neurol. 2005, 57, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Wilson, R.S. Associations of vegetable and fruit consumption with age-related cognitive change. Neurology 2006, 67, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Clinical guideline on the identification, evaluation, and treatment of overweight and obesity in adults: The evidence report. 1998; National Heart, Lung, and Blood Institute (online). Available online: http://www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf (accessed on 6 August 2014).
- Yagami, T.; Ueda, K.; Asakura, K.; Okamura, N.; Sakaeda, T.; Sakaguchi, G.; Itoh, N.; Hashimoto, Y.; Nakano, T.; Fujimoto, M.; et al. Effect of Gas6 on secretory phospholipase A(2)-IIA-induced apoptosis in cortical neurons. Brain Res. 2003, 985, 142–149. [Google Scholar] [CrossRef]
- Liu, D.; Guo, H.; Griffin, J.H.; Fernandez, J.A.; Zlokovic, B.V. Protein S confers neuronal protection during ischemic/hypoxic injury in mice. Circulation 2003, 107, 1791–1796. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.; Wang, Y.; Guo, H.; Sagare, A.; Fernández, J.A.; Bell, R.D.; Barrett, T.M.; Griffin, J.H.; Freeman, R.S.; Zlokovic, B.V.; et al. Protein S protects neurons from excitotoxic injury by activating the TAM receptor Tyro3-phosphatidylinositol 3-kinase-Akt pathway through its sex hormone-binding globulin-like region. J. Neurosci. 2010, 30, 15521–15534. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.L.; Suttie, J.W. Dietary intake and adequacy of vitamin K. J. Nutr. 1998, 128, 785–788. [Google Scholar] [PubMed]
- Holmes, M.V.; Hunt, B.J.; Shearer, M.J. The role of dietary vitamin K in the management of oral vitamin K antagonists. Blood Rev. 2012, 26, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Spencer, R.J.; Wendell, C.R.; Giggey, P.P.; Katzel, L.I.; Lefkowitz, D.M.; Siegel, E.L.; Waldstein, S.R. Psychometric limitations of the mini-mental state examination among nondemented older adults: An evaluation of neurocognitive and magnetic resonance imaging correlates. Exp. Aging Res. 2013, 39, 382–397. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chouet, J.; Ferland, G.; Féart, C.; Rolland, Y.; Presse, N.; Boucher, K.; Barberger-Gateau, P.; Beauchet, O.; Annweiler, C. Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study. Nutrients 2015, 7, 6739-6750. https://doi.org/10.3390/nu7085306
Chouet J, Ferland G, Féart C, Rolland Y, Presse N, Boucher K, Barberger-Gateau P, Beauchet O, Annweiler C. Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study. Nutrients. 2015; 7(8):6739-6750. https://doi.org/10.3390/nu7085306
Chicago/Turabian StyleChouet, Justine, Guylaine Ferland, Catherine Féart, Yves Rolland, Nancy Presse, Kariane Boucher, Pascale Barberger-Gateau, Olivier Beauchet, and Cedric Annweiler. 2015. "Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study" Nutrients 7, no. 8: 6739-6750. https://doi.org/10.3390/nu7085306
APA StyleChouet, J., Ferland, G., Féart, C., Rolland, Y., Presse, N., Boucher, K., Barberger-Gateau, P., Beauchet, O., & Annweiler, C. (2015). Dietary Vitamin K Intake Is Associated with Cognition and Behaviour among Geriatric Patients: The CLIP Study. Nutrients, 7(8), 6739-6750. https://doi.org/10.3390/nu7085306