Association between Breastfeeding and Endometrial Cancer Risk: Evidence from a Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
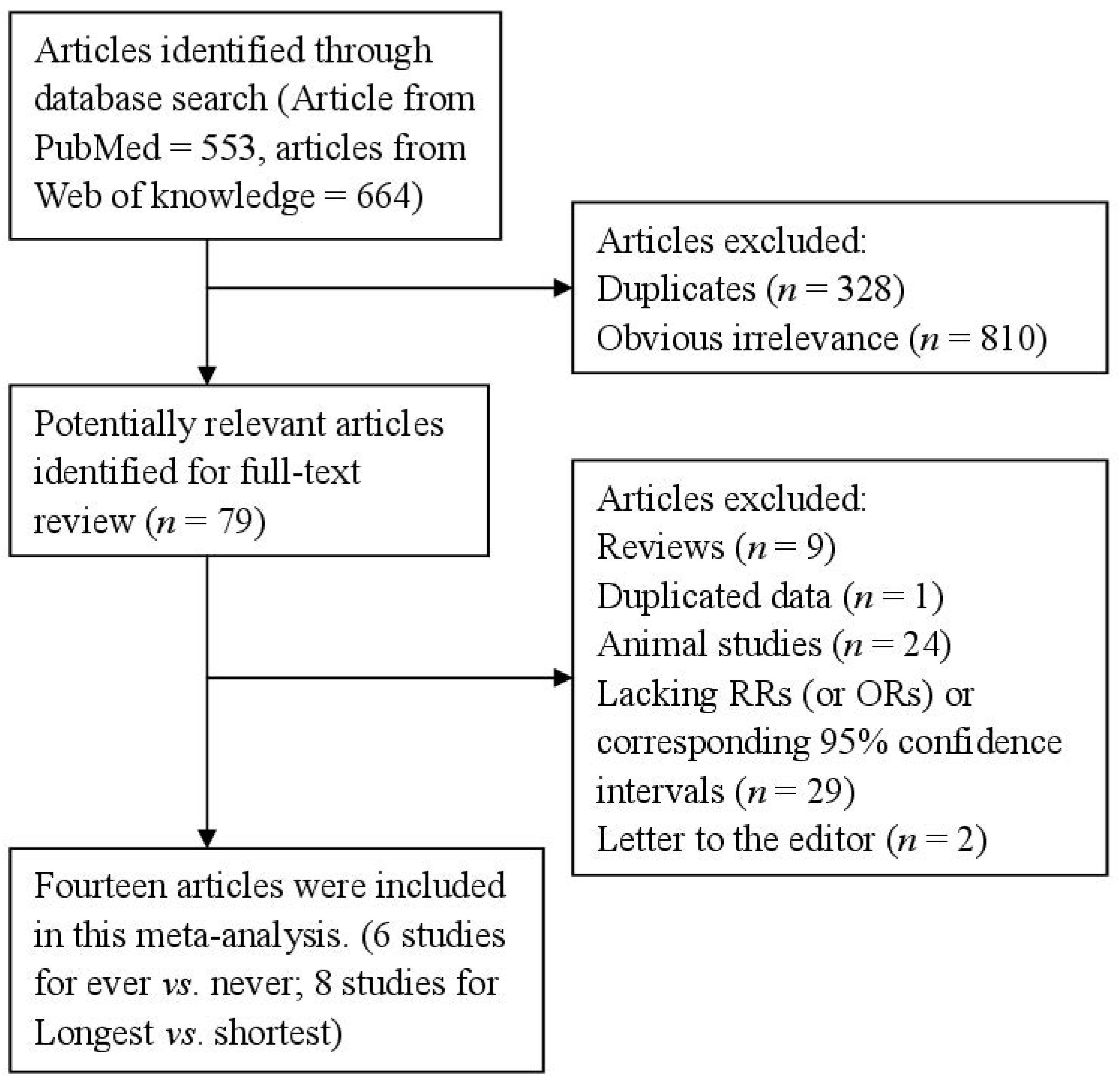
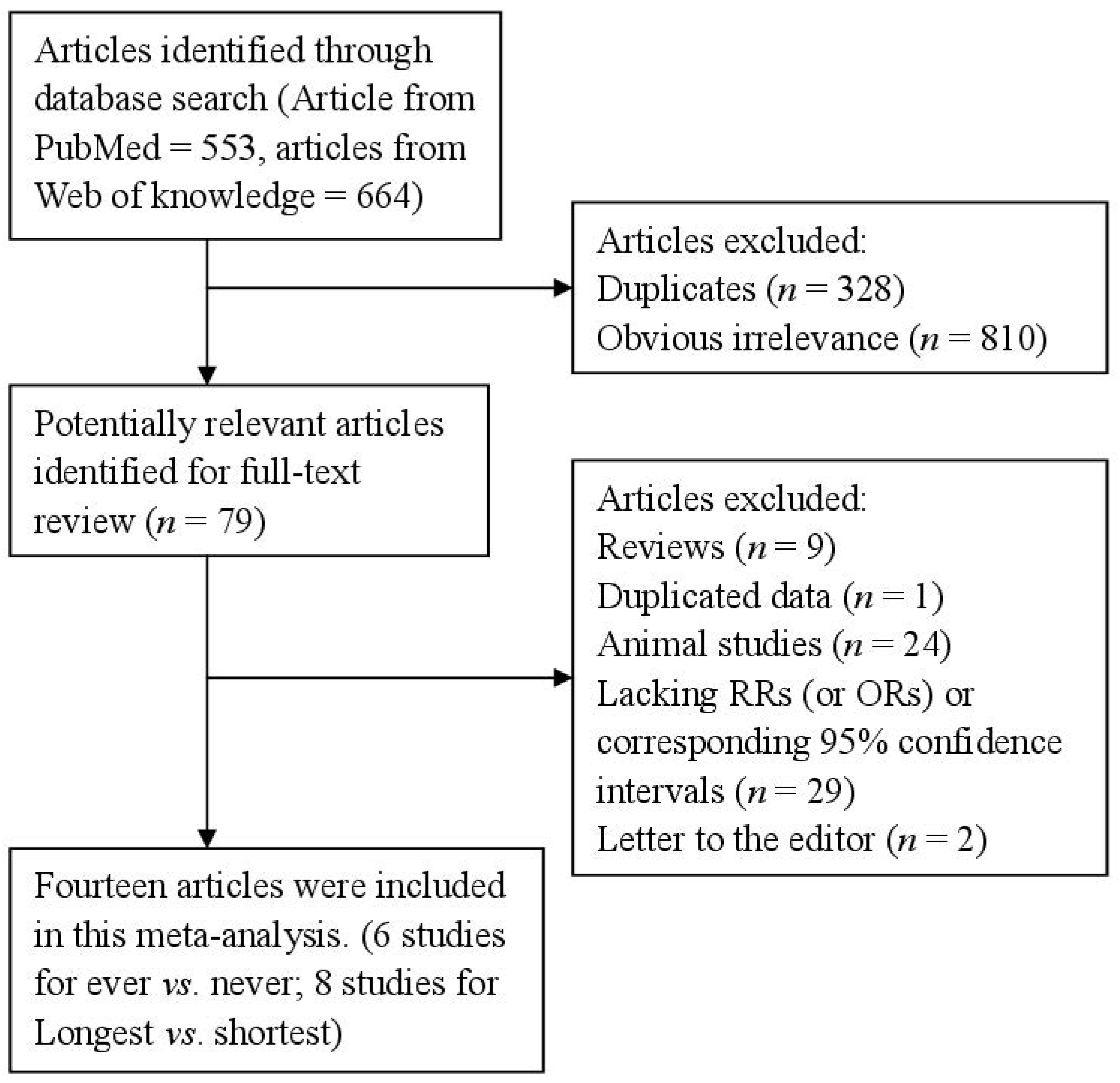
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Study Design | Cases, Age | Category | RR (95% CI) | Adjustment or Matched for |
|---|---|---|---|---|---|---|
| Brinton et al., 1992, [20] | United States | Retrospective | 405, 20–74 | Ever vs. never | 1.01 (0.60–1.60) | Adjusted for age at interview, years of education, recent weight, oral contraceptive use, and menopausal estrogen use. |
| Brinton et al., 2007, [21] | Polish | Retrospective | 551, 20–74 | ≥24 months vs. never | 0.72 (0.40–1.20) | Adjusted for age, study, site, years of education, age at menarche, number of full-term births, ever use of oral contraceptives, ever use of oral hormones, ever smoking, recent body mass index. |
| Dossus et al., 2009, [22] | Denmark, France, Germany, Greece, Italy, The Netherlands, Norway, Spain, Sweden and United Kingdom | Prospective | 1017, 30–80 | >18 months vs. ≤1 months | 0.77 (0.54–1.11) | Adjusted for age and center stratified and adjusted for BMI, physical activity, alcohol, diabetes, smoking status and education. |
| Elwood et al., 1977, [23] | United States | Retrospective | 410, 55–59 | Ever vs. never | 1.0 (0.7–1.5) | Na. |
| Herrinton et al., 2001, [24] | United States | Retrospective | 280, 20–54 | Ever vs. never | 0.95 (0.65–1.40) | Adjusted for history of oral contraceptive use and educational attainment. |
| Hirose et al., 1999, [25] | Japan | Retrospective | 133, 30–80 | >12 months vs. 1–5 months | 1.48 (0.63–3.49) | Adjusted for age and body mass index. |
| Newcomb et al., 2000, [26] | United States | Retrospective | 586, 40–79 | >24 months vs. never | 0.84 (0.52–1.40) | Adjusted for age, smoking status, education, body mass, postmenopausal hormone therapy, and parity. |
| Okamura et al., 2006, [27] | Japan | Retrospective | 155, 20–80 | Ever vs. never | 0.37 (0.17–0.82) | Adjusted for age, BMI, oral contraceptive use. |
| Rosenblatt et al., 1995, [28] | Australia, Israel, Chile, China, Philippines, and Thailand | Retrospective | 136, 20–75 | >72 months vs. never | 0.23 (0.08–0.68) | Adjusted for number of pregnancies and age at menarche. |
| Salazar-Martinez et al., 1999, [29] | Mexico | Retrospective | 85, 20–75 | >25 months vs. never | 0.33 (0.17–0.65) | Adjusted by age, hormonal use, number of pregnancies, smoking, diabetes mellitus, hypertension, physical activity, menopausal status, and body build index. |
| Sugawara et al., 2013, [30] | Japan | Prospective | 32, 40–79 | Ever vs. never | 0.31 (0.12–0.81) | Adjusted for age, BMI, family history of cancer, education, job status, smoking status, alcohol consumption, time spent walking, total calorie intake, menopausal status, age at menarche, age at first delivery, number of deliveries, history of oral contraceptive drug use, and history of hormone replacement therapy. |
| Wernli et al., 2006, [31] | China | Prospective | 206, 30–80 | >36 months vs. ≤1 months | 0.62 (0.35–1.09) | Adjusted for age at baseline and number of live births. |
| Xue et al., 2008, [32] | United States | Prospective | 708, 30–55 | >9 months vs. never | 0.99 (0.77–1.29) | Adjusted for age, premature birth, birth order, birth weight, family history of endometrial cancer, age at menarche, oral contraceptive use, parity, age at first birth, age at last birth, physical activity, cigarette smoking, tamoxifen use, menopausal status, age at menopause, postmenopausal hormone use, BMI, BMI at age 18 years, and somatotype at ages 5 and 10 years. |
| Zucchetto et al., 2009, [33] | Italy | Retrospective | 454, 18–79 | Ever vs. never | 1.33 (0.95–1.85) | Adjusted for period of interview, body mass index, age at menarche, age at menopause, parity, and oral contraceptive use, when appropriate. |
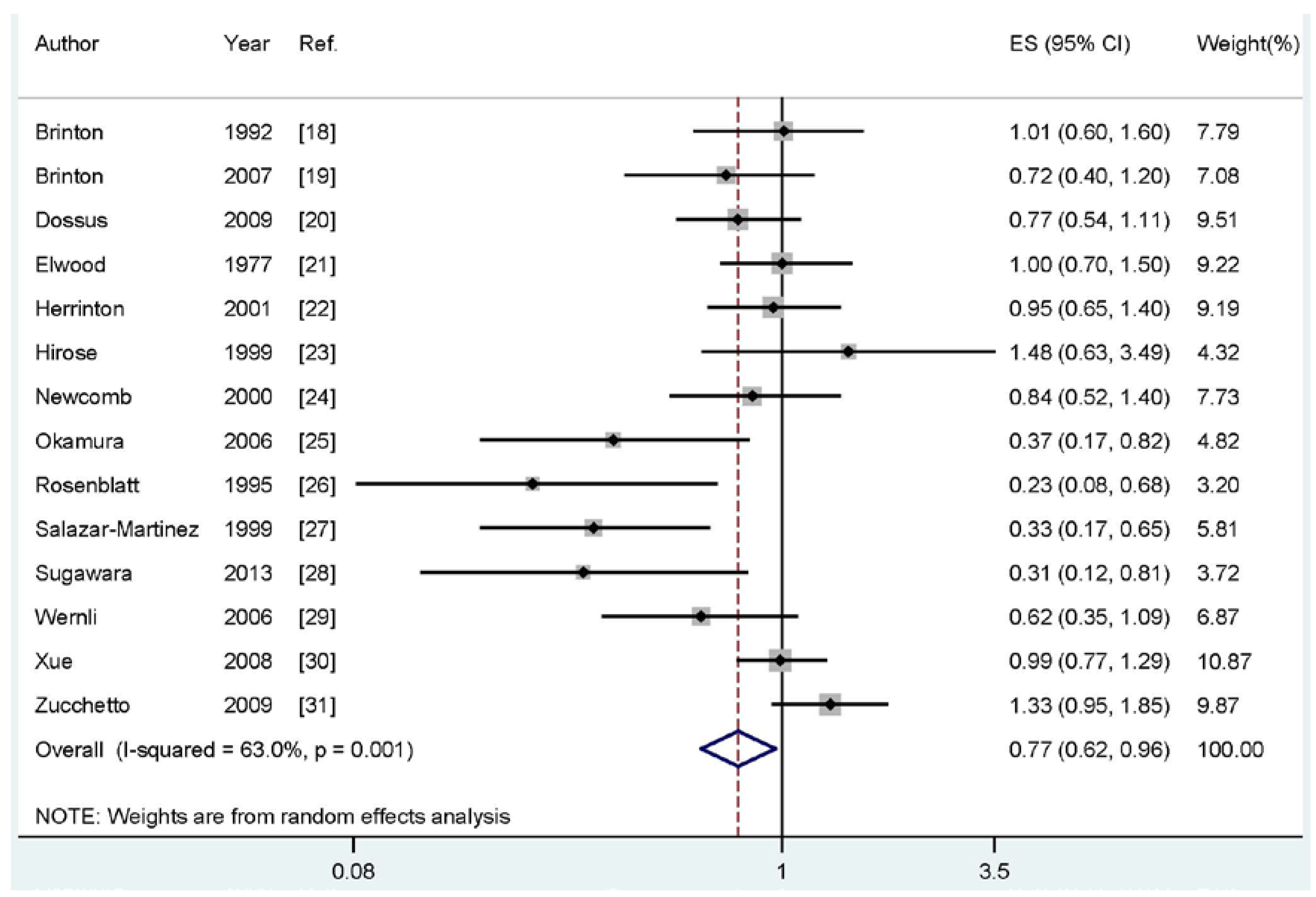
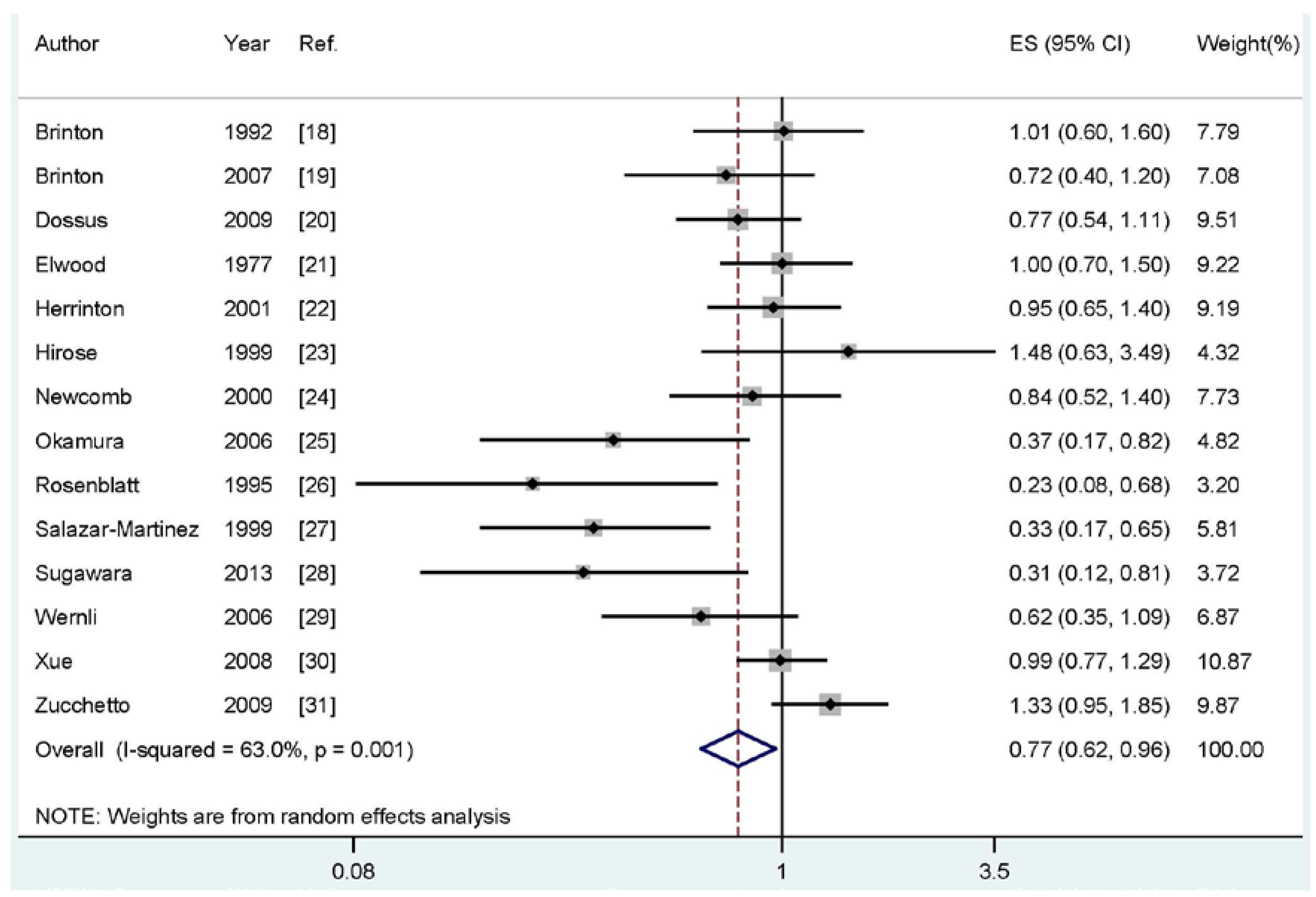
3.2. Breastfeeding and Endometrial Cancer
3.3. Ever vs. Never Breastfeeding and Risk of Endometrial Cancer
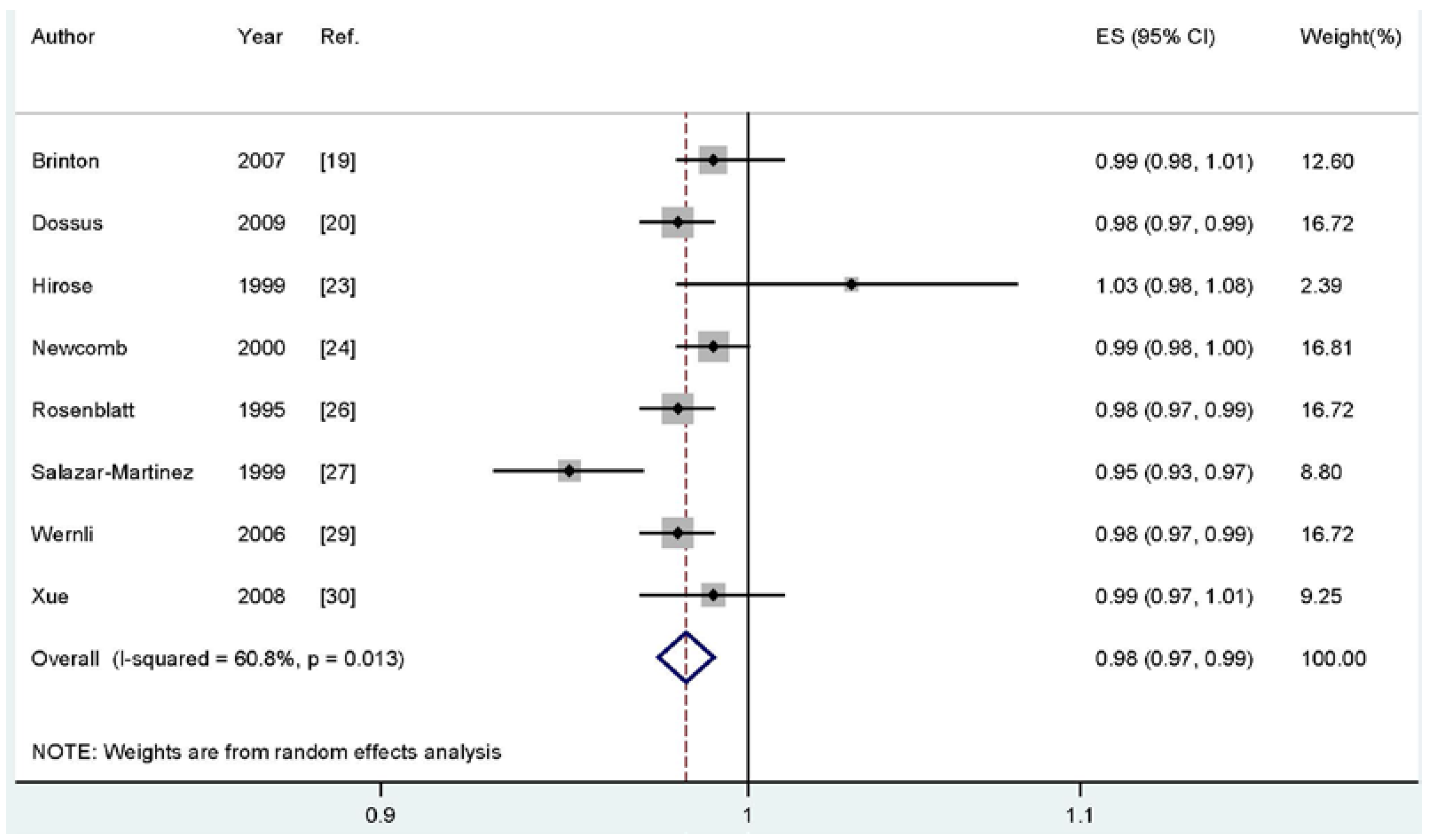
3.4. Longest Compared with Shortest Total Durations of Breastfeeding
3.5. Meta-Regression and Subgroups Analysis
| Sub-Groups | Cases | Studies | RR (95%CI) | I2 (%) | Pheterogeneity |
|---|---|---|---|---|---|
| All studies | 5158 | 14 | 0.77 (0.62–0.96) | 63.0 | 0.001 |
| Study Design | |||||
| Retrospective | 3195 | 10 | 0.78 (0.58–0.98) | 67.6 | 0.001 |
| Prospective | 1963 | 4 | 0.74 (0.52–1.04) | 57.5 | 0.070 |
| Study Type | |||||
| Ever vs. never | 1736 | 6 | 0.85 (0.61–1.20) | 66.1 | 0.011 |
| Longest vs. shortest | 3422 | 8 | 0.71 (0.53–0.95) | 60.3 | 0.014 |
| Geographic Locations | |||||
| North America | 2474 | 6 | 0.87 (0.79–0.95) | 48.8 | 0.082 |
| Europe | 2022 | 3 | 0.93 (0.62–1.40) | 67.5 | 0.046 |
| Asia | 526 | 4 | 0.58 (0.31–1.07) | 60.3 | 0.056 |
| Sources of Control | |||||
| Population-based | 1731 | 5 | 0.80 (0.57–1.11) | 57.9 | 0.050 |
| Hospital-based | 1464 | 5 | 0.74 (0.41–1.34) | 77.3 | 0.001 |
| Adjusted or Unadjusted Analyses | |||||
| Adjusted results | 4748 | 13 | 0.75 (0.59–0.95) | 65.3 | 0.001 |
| Unadjusted results | 2966 | 5 | 0.83 (0.70–0.99) | 15.2 | 0.318 |
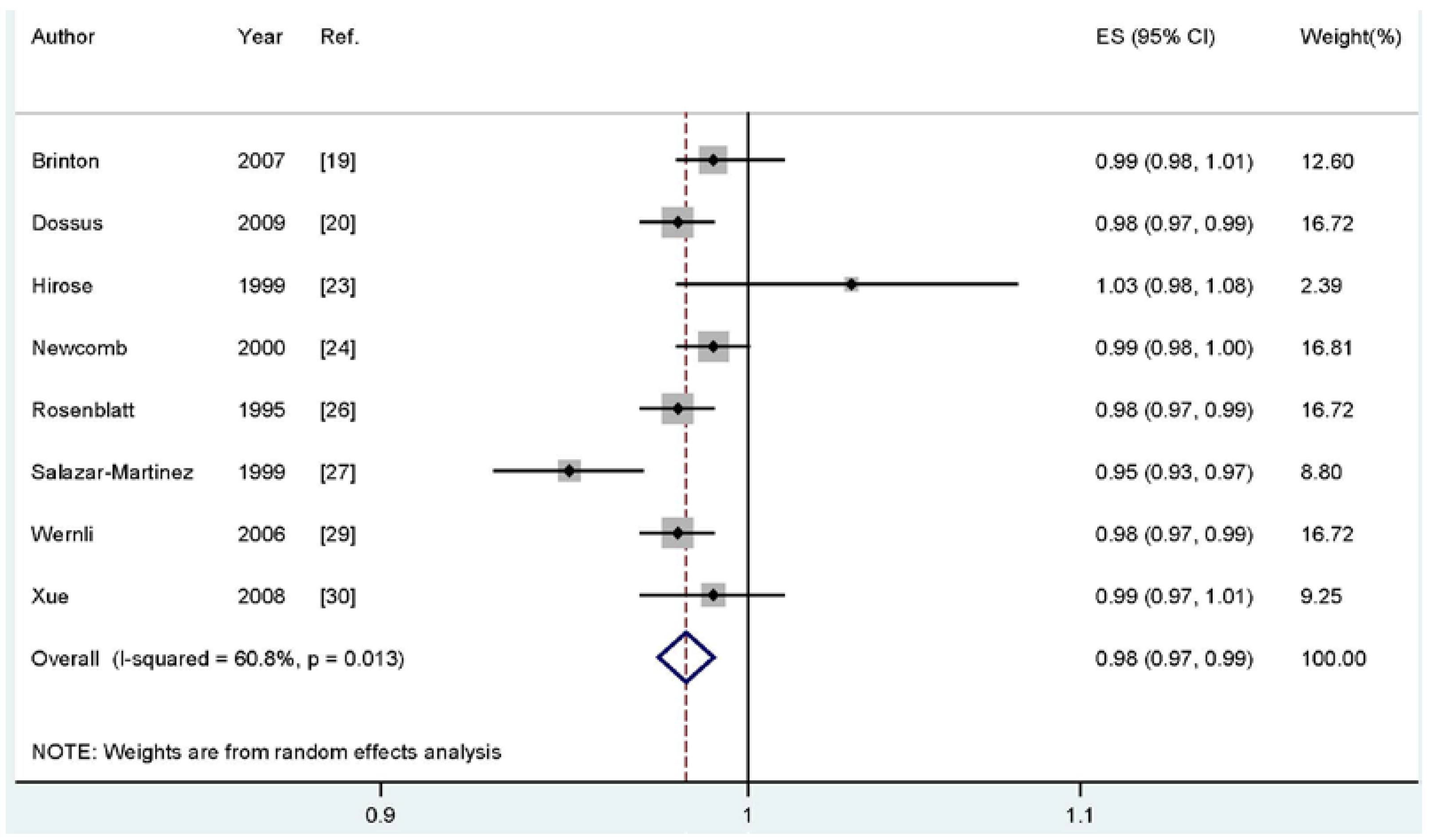
3.6. Dose-Response Analysis
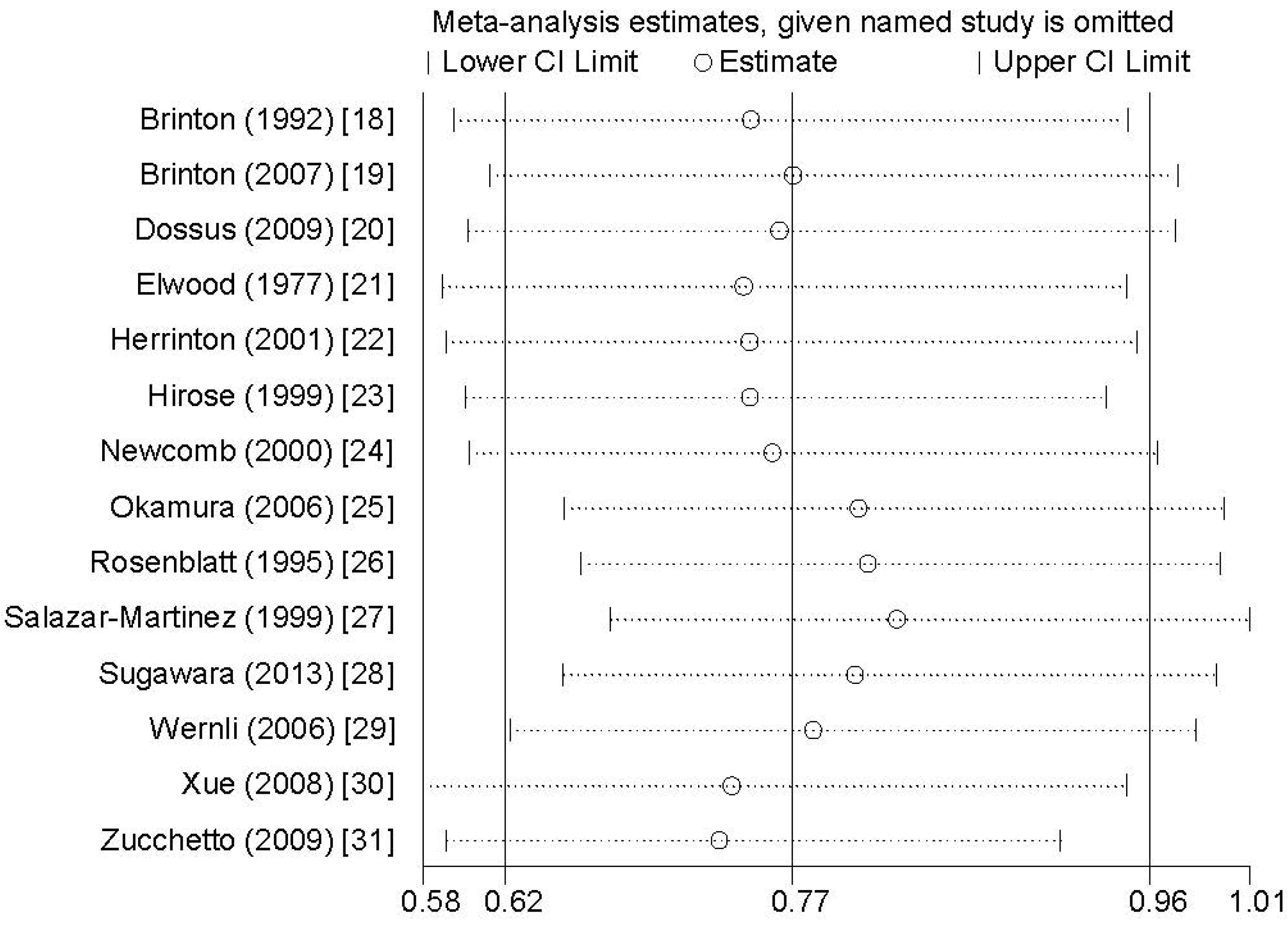
3.7. Sensitivity Analysis and Publication Bias

4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Pike, M.C. The dose-effect relationship between “unopposed” oestrogens and endometrial mitotic rate: Its central role in explaining and predicting endometrial cancer risk. Br. J. Cancer 1988, 57, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Siiteri, P.K. Steroid hormones and endometrial cancer. Cancer Res. 1978, 38, 4360–4366. [Google Scholar] [PubMed]
- Henderson, B.E.; Ross, R.K.; Pike, M.C.; Casagrande, J.T. Endogenous hormones as a major factor in human cancer. Cancer Res. 1982, 42, 3232–3239. [Google Scholar] [PubMed]
- Databases of PubMed. Available online: http://www.ncbi.nlm.nih.gov/pubmed (accessed on 1 April 2015).
- Web of Knowledge. Available online: http://apps.webofknowledge.com (accessed on 1 April 2015).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Wells, G. The Newcastle-Ottawa Scale (NOS) for assessingthe quality of nonrandomized studies in meta-analyses. Available online: http://wwwohrica/programs/clinicalepidemiology/oxfordasp (accessed on 25 November 2012).
- Rong, Y.; Chen, L.; Zhu, T.; Song, Y.; Yu, M.; Shan, Z.; Sands, A.; Hu, F.B.; Liu, L. Egg consumption and risk of coronary heart disease and stroke: Dose-response meta-analysis of prospective cohort studies. BMJ 2013, 346, e8539. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [PubMed]
- Orsini, N.; Bellocco, R. Generalized least squares for trend estimation of summarized dose-response data. Stata. J. 2006, 6, 40–57. [Google Scholar]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-analysis for linear and nonlinear dose-response relations: Examples, an evaluation of approximations, and software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Giovannucci, E.; Wolk, A. Folate and risk of breast cancer: A meta-analysis. J. Natl. Cancer Inst. 2007, 99, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Qin, S.; Wang, M.; Zhang, T.; Zhang, S. Association between cholesterol intake and pancreatic cancer risk: Evidence from a meta-analysis. Sci. Rep. 2015, 5, 8243. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Assessing the in fluence of a single study in the meta-analysis estimate. Stata. Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Brinton, L.A.; Berman, M.L.; Mortel, R.; Twiggs, L.B.; Barrett, R.J.; Wilbanks, G.D.; Lannom, L.; Hoover, R.N. Reproductive, menstrual, and medical risk factors for endometrial cancer: Results from a case-control study. Am. J. Obstet. Gynecol. 1992, 167, 1317–1325. [Google Scholar] [CrossRef]
- Brinton, L.A.; Sakoda, L.C.; Lissowska, J.; Sherman, M.E.; Chatterjee, N.; Peplonska, B.; Szeszenia-Dabrowska, N.; Zatonski, W.; Garcia-Closas, M. Reproductive risk factors for endometrial cancer among Polish women. Br. J. Cancer 2007, 96, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Dossus, L.; Allen, N.; Kaaks, R.; Bakken, K.; Lund, E.; Tjonneland, A.; Olsen, A.; Overvad, K.; Clavel-Chapelon, F.; Fournier, A.; et al. Reproductive risk factors and endometrial cancer: The European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2010, 127, 442–451. [Google Scholar] [PubMed]
- Elwood, J.M.; Cole, P.; Rothman, K.J.; Kaplan, S.D. Epidemiology of endometrial cancer. J. Natl. Cancer Inst. 1977, 59, 1055–1060. [Google Scholar] [PubMed]
- Herrinton, L.J.; Voigt, L.F.; Weiss, N.S.; Beresford, S.A.; Wingo, P.A. Risk factors for synchronous primary endometrial and ovarian cancers. Ann. Epidemiol. 2001, 11, 529–533. [Google Scholar] [CrossRef]
- Hirose, K.; Tajima, K.; Hamajima, N.; Kuroishi, T.; Kuzuya, K.; Miura, S.; Tokudome, S. Comparative case-referent study of risk factors among hormone-related female cancers in Japan. Jpn. J. Cancer Res. 1999, 90, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Newcomb, P.A.; Trentham-Dietz, A. Breast feeding practices in relation to endometrial cancer risk, USA. Cancer Causes Control. 2000, 11, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Okamura, C.; Tsubono, Y.; Ito, K.; Niikura, H.; Takano, T.; Nagase, S.; Yoshinaga, K.; Terada, Y.; Murakami, T.; Sato, S.; et al. Lactation and risk of endometrial cancer in Japan: A case-control study. Tohoku J. Exp. Med. 2006, 208, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, K.A.; Thomas, D.B.; WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Prolonged lactation and endometrial cancer. Int J. Epidemiol. 1995, 24, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Martinez, E.; Lazcano-Ponce, E.C.; Gonzalez Lira-Lira, G.; Escudero-De los Rios, P.; Salmeron-Castro, J.; Hernandez-Avila, M. Reproductive factors of ovarian and endometrial cancer risk in a high fertility population in Mexico. Cancer Res. 1999, 59, 3658–3662. [Google Scholar] [PubMed]
- Sugawara, Y.; Kakizaki, M.; Nagai, M.; Tomata, Y.; Hoshi, R.; Watanabe, I.; Nishino, Y.; Kuriyama, S.; Tsuji, I. Lactation pattern and the risk for hormone-related female cancer in Japan: The Ohsaki Cohort Study. Eur. J. Cancer Prev. 2013, 22, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Wernli, K.J.; Ray, R.M.; Gao, D.L.; De Roos, A.J.; Checkoway, H.; Thomas, D.B. Menstrual and reproductive factors in relation to risk of endometrial cancer in Chinese women. Cancer Causes Control. 2006, 17, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Xue, F.; Hilakivi-Clarke, L.A.; Maxwell, G.L.; Hankinson, S.E.; Michels, K.B. Infant feeding and the incidence of endometrial cancer. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1316–1321. [Google Scholar] [CrossRef] [PubMed]
- Zucchetto, A.; Serraino, D.; Polesel, J.; Negri, E.; De Paoli, A.; Dal Maso, L.; Montella, M.; La Vecchia, C.; Franceschi, S.; Talamini, R. Hormone-related factors and gynecological conditions in relation to endometrial cancer risk. Eur. J. Cancer Prev. 2009, 18, 316–321. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund; American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Globalperspective; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Munafo, M.R.; Flint, J. Meta-analysis of genetic association studies. Trends Genet. 2004, 20, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Wojcicki, J.M. Maternal prepregnancy body mass index and initiation and duration of breastfeeding: A review of the literature. J. Womens Health 2011, 20, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, J.; Li, Q.; Huang, W.; Lan, H.; Jiang, H. Association between breastfeeding and breast cancer risk: Evidence from a meta-analysis. Breastfeed. Med. 2015, 10, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Luan, N.N.; Wu, Q.J.; Gong, T.T.; Vogtmann, E.; Wang, Y.L.; Lin, B. Breastfeeding and ovarian cancer risk: A meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2013, 98, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Li, J.; Shi, Z. Association between Breastfeeding and Endometrial Cancer Risk: Evidence from a Systematic Review and Meta-Analysis. Nutrients 2015, 7, 5697-5711. https://doi.org/10.3390/nu7075248
Wang L, Li J, Shi Z. Association between Breastfeeding and Endometrial Cancer Risk: Evidence from a Systematic Review and Meta-Analysis. Nutrients. 2015; 7(7):5697-5711. https://doi.org/10.3390/nu7075248
Chicago/Turabian StyleWang, Lianlian, Jingxi Li, and Zhan Shi. 2015. "Association between Breastfeeding and Endometrial Cancer Risk: Evidence from a Systematic Review and Meta-Analysis" Nutrients 7, no. 7: 5697-5711. https://doi.org/10.3390/nu7075248
APA StyleWang, L., Li, J., & Shi, Z. (2015). Association between Breastfeeding and Endometrial Cancer Risk: Evidence from a Systematic Review and Meta-Analysis. Nutrients, 7(7), 5697-5711. https://doi.org/10.3390/nu7075248