Krill Products: An Overview of Animal Studies

Abstract
:1. Introduction

{kind=link}
| Composition | KO (g/100 g Oil) | KP (g/100 g Powder or Extracted Fat) | KPC (g/100 g KPC or Extracted Fat) |
|---|---|---|---|
| Protein | - | 38 | 78 |
| Total lipids | 89 | 51 | 8 |
| Triglycerides | 34 | 45 * | - |
| Total PLs | 43 | 43 * | - |
| PC | 35 | 40 * | - |
| Total omega-3 | 25 | 20 * | 27 * |
| EPA | 13 | 10 * | 12 * |
| DHA | 7 | 5 * | 13 * |
| Total omega-6 | 2 | 2 * | 4 * |
| Saturated FA | 23 | 25 * | 37 * |
| Total MUFAs | 15 | 20 * | 21 * |
2. Documentation of Krill Oil Health Benefits in Animal Studies
| Classification of health benefits | Study | Animal model | Diets | Duration of Supplementation | Effect of KO/KPC and KP |
|---|---|---|---|---|---|
| Effect of KO | |||||
| Obesity | Zhu et al., 2008 [34] | SD rats (obesity model) n = 60 | Different doses: High fat with 16.7, 33.3, 99.9 or 199.8 g/L KO | 4 weeks | decreased levels of serum TAG, TC and LDL-C |
| reduced body weight | |||||
| Obesity | Batetta et al., 2009 [23] | Zucker rats (obesity model) n = 18 | Control diet with 0.5 g EPA+DHA/100 g diet (from either KO or FO) | 4 weeks | decreased levels of plasma LDL-C |
| increased levels of plasma TAG | |||||
| reduced TAG in liver and heart | |||||
| decreased AEA and 2-AG in VAT and AEA in liver and heart | |||||
| reduced TNFα secretion from macrophages (associated with lower levels of AA in membrane PLs) | |||||
| Obesity | Tandy et al., 2009 [30] | C57BL/6 mice (obesity model) n = 46 | Different doses: Normal diet or high fat diet with 1.25%, 2.5% or 5.0% KO | 8 weeks | reduced hepatic steatosis and plasma glucose and TC (not TAG) |
| increased adiponectin | |||||
| reduced hepatic TNFα expression and down-regulation of several hepatic genes involved in FA synthesis and catabolism | |||||
| Obesity | Di Marzo et al., 2010 [28] | Zucker rats (obesity model) n = 18 | Control diet with 0.5 g EPA+DHA/100 g diet (from either KO or FO) | 4 weeks | increased EPA and DHA levels in brain |
| decreased 2-AG levels in brain | |||||
| Obesity | Piscitelli et al., 2011 [29] | C57BL/6 mice (obesity model) n = 6–10 per group | Different doses: Normal diet or high fat diet with 1.25, 2.5 or 5% KO | 8 weeks | reduction of AEA and/or 2-AG levels in heart, kidneys, gastrocnemius muscle, inguinal and epididymal adipose tissue |
| Obesity | Ferramosca et al., 2012 [24] | SD rats n = 120 | Control, High fat control, High fat 2.5% KO | 12 weeks | decreased levels of hepatic TAG and cholesterol |
| reduced plasma TAG and glucose levels | |||||
| reduced hepatic FA synthesis | |||||
| increased hepatic FA oxidation | |||||
| increased mitochondrial respiration efficiency | |||||
| reduction in body weight | |||||
| Obesity | Tillander et al., 2014 [31] | C57BL/6J mice | High fat control (n = 9) High fat FO (5.8%) (n = 6) High fat KO (5.7%) (n = 6) | 6 weeks | decreased plasma levels of NEFA |
| down regulation of cholesterol and fatty acid synthesis (mRNA level) | |||||
| Obesity | Ivanova et al., 2014 [32] | New Zealand white rabbits n = 24 | Castrated control, Non-castrated control, Castrated KO (daily dose of 600 mg omega-3), Castrated FO (daily dose of 600 mg omega-3) | 2 months | decreased fasting glucose for both FO and KO |
| modified gene expression of key enzymes in β-oxidation, lipogenesis in liver and skeletal muscle | |||||
| Inflammation | Ierna et al., 2010 [27] | DBA/1 mice (arthritis model) n = 42 | Control diet with 0.44 g EPA+DHA/100 g diet from KO or 0.47 g EPA+DHA/100 g diet from FO). Induction of arthritis Day 25, boost Day 47 | 68 days | reduction in paw swelling |
| reduction in histopathology scores (joint section) | |||||
| Inflammation | Grimstad et al., 2012 [21] | Wistar rats (colitis model) n = 30 | Control, Control + DSS, Control + DSS + KO, Induction of colitis by DSS on Day 23 | 30 days | improved colon length |
| increased level of (PG)E3 and Pparg1 α expression | |||||
| Cardiovascular | Fosshaug et al., 2011 [25] | Wistar rats (myocardial infarction model) | Control n = 14 pre-treated (2 weeks) with KO n = 18 not pre-treated with KO n = 17 Induction of myocardial infarction by left coronary artery ligation | 7 weeks | Pre-treated KO group: - attenuated LV dilation - reduced heart and lung weights - reduced mRNA levels of LV stress and matrix remodeling markers |
| Not pre-treated KO group: - increased LV | |||||
| Brain | Gamoh et al., 2011 [35] | Wistar rats | Control (n = 15) High dose krill PL (420 mg EPA+DHA) (n = 14) Low dose krill PL (301 mg EPA+DHA) (n = 13) | 6 weeks | improved spatial-memory related learning ability |
| increased levels of EPA, DPA and DHA and decreased level of AA in the brain | |||||
| decreased levels of lipid peroxide and reactive oxygen species | |||||
| increased cell generation in dentate gyrus | |||||
| Brain | Wibrand et al., 2013 [22] | Wistar rats | Control (n = 12) Imipramine (n = 12) KO 1.25% (n = 14) KO 2.50% (n = 14) | 7 weeks | improved learning and memory processes |
| anti-depressant-like effects | |||||
| Liver | Ferramosca et al., 2012 [36] | Wistar rats n = 18 | Control, 2.5% KO, 2.5% FO | 6 weeks | decreased levels of plasma TAG and TC |
| inhibition of hepatic lipogenesis (reduced activity of CIC, ACC and FAS) | |||||
| Gene expression | Burri et al., 2011 [37] | CBA/J micen = 30 | Control diet with 1.5% KO or 1.1% FO | 3 months | down-regulation of: hepatic glucose pathways, lipid and cholesterol synthesis (FO up-regulated cholesterol synthesis pathway) |
| Kidney | Gigliotti et al., 2013 [33] | Female SD rats n = 60 | 12% corn oil (n = 10) 12% flaxseed (n = 10) 12% menhaden oil (n = 10) 12% KO (n = 10) 12% salmon oil (n = 10) 12% tuna oil (n = 10) | 8 weeks | increased kidney weight |
| increased calcium content of the kidneys | |||||
| increased urinary phosphorous excretion | |||||
| Safety | Robertson et al., 2014 [20] | Wistar rats n = 80 | Control, 1.7% KO, 3.3% KO, 5% KO | 13 weeks | NOAEL is 5% KO |
| Effect of KPC and KP | |||||
| Inflammation | Bjørndal et al., 2012 [38] | C57BL/6 mice constitutively expressing hTNFα gene (n = 20) | High fat control; High fat 3% KP | 6 weeks | decreased plasma and liver TAG levels |
| down-regulation of hepatic genes involved in lipogenesis | |||||
| reduction of TNFα in liver | |||||
| Kidney | Gigliotti et al., 2008 [40] | Female SD rats n = 30 | 10% KPC, 10% casein | 4 weeks | reduced kidney weight |
| reduced total mineral content of the kidneys | |||||
| no differences in kidney function | |||||
| Kidney, Bone | Gigliotti et al., 2011 [41] | Female SD rats n = 20 | 10% KPC, 10% casein | 4 weeks | reduced kidney injury (lower urinary NAG activity, reduced kidney mineralization, tendency for higher GRFs and lower proteinuria) and Ca deposition |
| no effect on bone mass or strength | |||||
| Gene expression | Bjørndal et al., 2013 [41] | CBA/J mice n = 20 | Low fat control Low fat 3% KP | 3 months | large number of pathways are modulated |
| down regulated pathways: β-oxidation, glucose metabolism and amino acid catabolism | |||||
| Safety | Bridges et al., 2010 [42] | Female SD rats n = 20 | 10% KPC, 10% casein | 4 weeks | increased DHA concentration in brain, and increased EPA and DHA concentration in fat pads and liver |
| decreased pro-inflammatory 2-series prostaglandin and thromboxan metabolites | |||||
| Safety | Berge et al., 2014 [43] | Wistar rats | Control, 9.67% KP | 13 weeks | NOAEL is 9.67% KP |
2.1. Different tissue FA Distribution When Carried in PL Versus TAG Ester Forms
2.2. Krill Oil—Endocannabinoid System
2.3. Krill Oil—Body and Tissue Weights
2.4. Krill Oil—Glucose Tolerance
2.5. Krill Oil—Chronic Inflammation, Rheumatoid Arthritis and Ulcerative Colitis
2.6. Krill Oil—Cardiovascular Risk Markers and Myocardial Infarction
2.7. Krill Oil— Cognitive Function/Depression
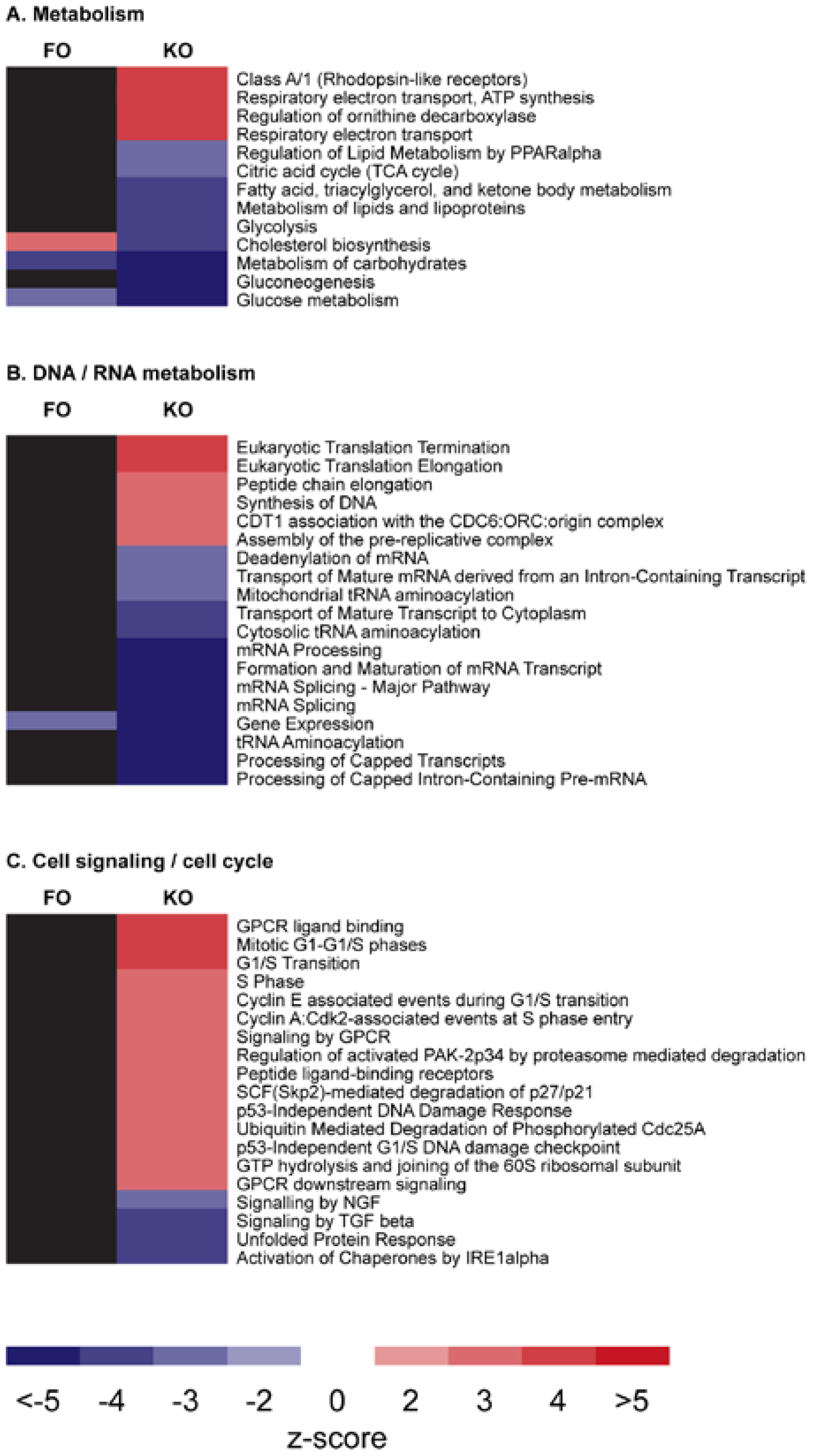
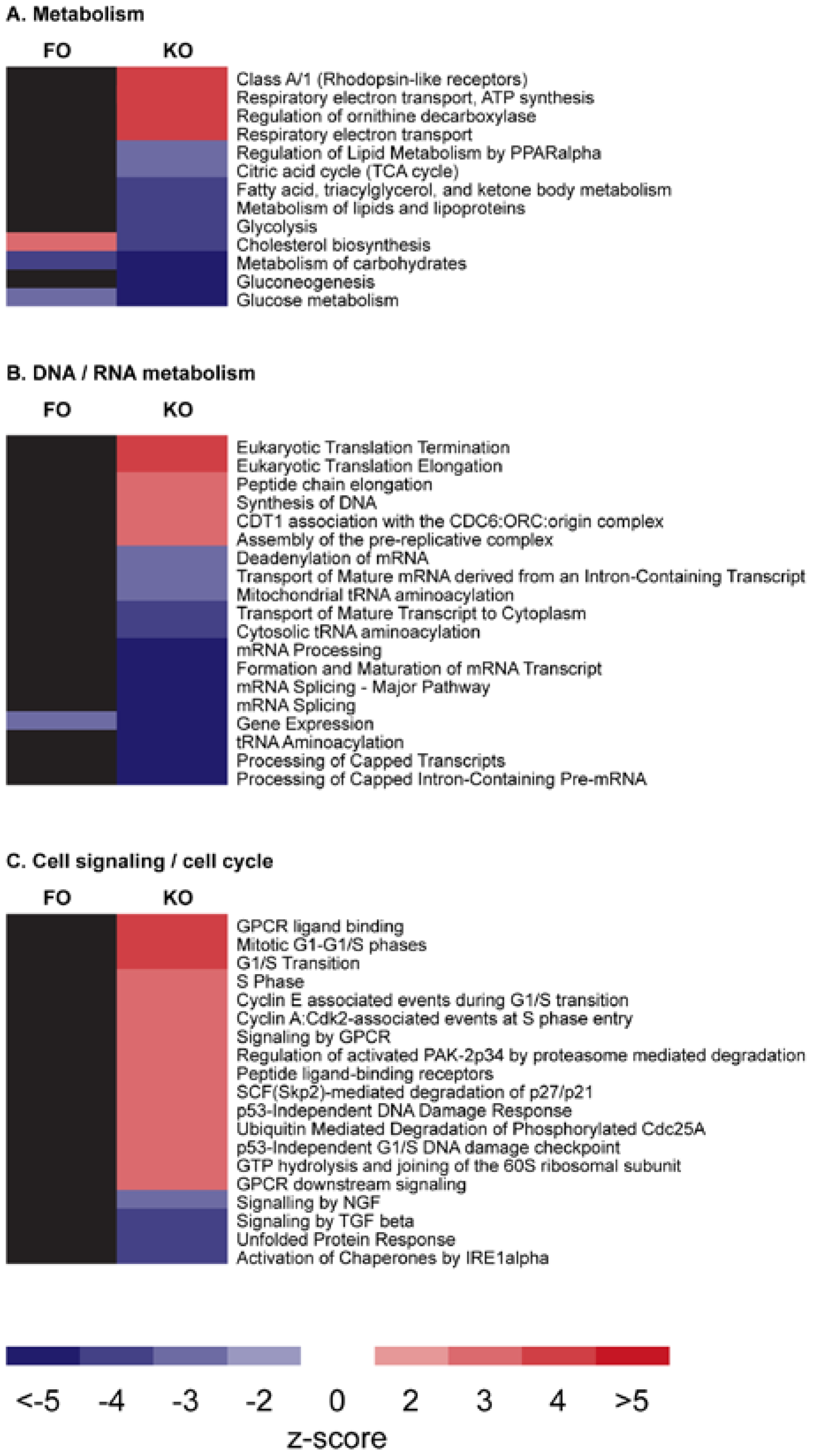
2.8. Krill Oil—Gene Expression
2.9. Krill Powder
| Metabolic Pathway | Krill Oil | Krill Powder | ||
|---|---|---|---|---|
| High-fat | Low-fat | High-fat | Low-fat | |
| Lipid synthesis | ↓ | ↓ | ↓ | - |
| Cholesterol metabolism | ↓ | ↓ | ↓ | - |
| β-oxidation | ↑ | ↓ | ↑ | ↓ |
| Mitochondrial respiration | ? | ↑ | ? | ↑ |
| Amino acid catabolism | ? | - | ? | ↓ |
| Glucose synthesis | ↓ | ↓ | ↓ | ↓ |
3. Discussion
4. Conclusions
Abbreviations
| AEA | N-arachidonoyl-ethanolamine |
| 2-AG | 2-arachidonoylglycerol |
| ALA | α-linolenic acid |
| ALSAT | aversive light stimulus avoidance test |
| ARA | arachidonic acid |
| CIC | mitochondrial citrate carrier |
| CNS | central nervous system |
| CVD | cardiovascular disease |
| DAI | disease activity index |
| DHA | docosahexaenoic acid |
| DSS | dextran sulfate sodium |
| EC | endocannabinoids |
| EPA | eicosapentaenoic acid |
| FA | fatty acid |
| FO | fish oil |
| HDL | high-density lipoprotein |
| IMIP | Imipramine |
| KO | krill oil |
| LDL | low-density lipoprotein |
| LPS | lipopolysaccharide |
| LV | left ventricular |
| lyso-PC | lysophosphatidylcholine |
| MI | myocardial infarction |
| NAFLD | non-alcoholic fatty liver disease |
| NHANES | national health and nutrition examination survey |
| NEFA | non-esterified fatty acid |
| NOAEL | no observed adverse effect level |
| n-3 PUFA | omega-3 polyunsaturated fatty acid |
| PC | phosphatidylcholine |
| PE | phosphatidylethanolamine |
| PL | phospholipid |
| PPARα | peroxisome proliferator-activated receptor alpha |
| RME | Reference Memory Error |
| TAG | triacylglyceride |
| TNFα | tumor necrosis factor-alpha |
| WME | Working Memory Error |
Acknowledgements
Conflicts of Interest
References
- Phleger, C.F.; Nelson, M.M.; Mooney, B.D.; Nichols, P.D. Interannual and between species comparison of the lipids, fatty acids and sterols of Antarctic krill from the US AMLR elephant island survey area. Comp. Biochem. Physiol. B Biochem. Mol. Biol. 2002, 131, 733–747. [Google Scholar] [CrossRef] [PubMed]
- Tou, J.C.; Jaczynski, J.; Chen, Y.C. Krill for human consumption: Nutritional value and potential health benefits. Nutr. Rev. 2007, 65, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Food and Nutrition Board, Institute of Medicine. Dietary reference intakes: For thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. National Academy of Sciences: Washington, DC, USA, 1998; pp. 390–422. [Google Scholar]
- Jensen, H.H.; Batres-Marquez, S.P.; Carriquiry, A.; Schalinske, K.L. Choline in the diets of the US population: Nhanes, 2003–2004. FASEB J. 2007, 21, LB46. [Google Scholar]
- Fischer, L.M.; da Costa, K.A.; Kwock, L.; Stewart, P.W.; Lu, T.S.; Stabler, S.P.; Allen, R.H.; Zeisel, S.H. Sex and menopausal status influence human dietary requirements for the nutrient choline. Am. J. Clin. Nutr. 2007, 85, 1275–1285. [Google Scholar] [PubMed]
- Graf, B.A.; Duchateau, G.S.; Patterson, A.B.; Mitchell, E.S.; van Bruggen, P.; Koek, J.H.; Melville, S.; Verkade, H.J. Age dependent incorporation of 14C-DHA into rat brain and body tissues after dosing various 14C-DHA-esters. Prostaglandins Leukot. Essent. Fat. Acids 2010, 83, 89–96. [Google Scholar] [CrossRef]
- Liu, L.; Bartke, N.; Van Daele, H.; Lawrence, P.; Qin, X.; Park, H.G.; Kothapalli, K.; Windust, A.; Bindels, J.; Wang, Z.; et al. Higher efficacy of dietary DHA provided as a phospholipid than as a triglyceride for brain DHA accretion in neonatal piglets. J. Lipid Res. 2014, 55, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Rossmeisl, M.; Jilkova, Z.M.; Kuda, O.; Jelenik, T.; Medrikova, D.; Stankova, B.; Kristinsson, B.; Haraldsson, G.G.; Svensen, H.; Stoknes, I.; et al. Metabolic effects of n-3 PUFA as phospholipids are superior to triglycerides in mice fed a high-fat diet: Possible role of endocannabinoids. PLoS ONE 2012, 7, e38834. [Google Scholar] [CrossRef] [PubMed]
- Wijendran, V.; Huang, M.C.; Diau, G.Y.; Boehm, G.; Nathanielsz, P.W.; Brenna, J.T. Efficacy of dietary arachidonic acid provided as triglyceride or phospholipid as substrates for brain arachidonic acid accretion in baboon neonates. Pediatr. Res. 2002, 51, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Singh, M. Essential fatty acids, DHA and human brain. Indian J. Pediatr. 2005, 72, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.N.; Ma, D.; Shui, G.; Wong, P.; Cazenave-Gassiot, A.; Zhang, X.; Wenk, M.R.; Goh, E.L.; Silver, D.L. Mfsd2a is a transporter for the essential omega-3 fatty acid docosahexaenoic acid. Nature 2014, 509, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre-Delaunay, D.; Pachiaudi, C.; Laville, M.; Pousin, J.; Armstrong, M.; Lagarde, M. Blood compartmental metabolism of docosahexaenoic acid (DHA) in humans after ingestion of a single dose of [(13)C]DHA in phosphatidylcholine. J. Lipid Res. 1999, 40, 1867–1874. [Google Scholar] [PubMed]
- Abedi, E.; Sahari, M.A. Long-chain polyunsaturated fatty acid sources and evaluation of their nutritional and functional properties. Food Sci. Nutr. 2014, 2, 443–463. [Google Scholar] [CrossRef] [PubMed]
- Arterburn, L.M.; Hall, E.B.; Oken, H. Distribution, interconversion, and dose response of n-3 fatty acids in humans. Am. J. Clin. Nutr. 2006, 83, 1467S–1476S. [Google Scholar] [PubMed]
- Wassall, S.R.; Stillwell, W. Polyunsaturated fatty acid-cholesterol interactions: Domain formation in membranes. Biochim. Biophys. Acta 2009, 1788, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Riediger, N.D.; Othman, R.A.; Suh, M.; Moghadasian, M.H. A systemic review of the roles of n-3 fatty acids in health and disease. J. Am. Diet. Assoc. 2009, 109, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Banni, S.; Di Marzo, V. Effect of dietary fat on endocannabinoids and related mediators: Consequences on energy homeostasis, inflammation and mood. Mol. Nutr. Food Res. 2010, 54, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochim. Biophys. Acta. 2015, 1851, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Cottin, S.C.; Sanders, T.A.; Hall, W.L. The differential effects of EPA and DHA on cardiovascular risk factors. Proc. Nutr. Soc. 2011, 70, 215–231. [Google Scholar] [CrossRef] [PubMed]
- Robertson, B.; Burri, L.; Berge, K. Genotoxicity test and subchronic toxicity study with superba krill oil in rats. Toxicol. Rep. 2014, 1, 764–776. [Google Scholar] [CrossRef]
- Grimstad, T.; Bjorndal, B.; Cacabelos, D.; Aasprong, O.G.; Janssen, E.A.; Omdal, R.; Svardal, A.; Hausken, T.; Bohov, P.; Portero-Otin, M.; et al. Dietary supplementation of krill oil attenuates inflammation and oxidative stress in experimental ulcerative colitis in rats. Scand. J. Gastroenterol. 2012, 47, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Wibrand, K.; Berge, K.; Messaoudi, M.; Duffaud, A.; Panja, D.; Bramham, C.R.; Burri, L. Enhanced cognitive function and antidepressant-like effects after krill oil supplementation in rats. Lipids Health Dis. 2013, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Batetta, B.; Griinari, M.; Carta, G.; Murru, E.; Ligresti, A.; Cordeddu, L.; Giordano, E.; Sanna, F.; Bisogno, T.; Uda, S.; et al. Endocannabinoids may mediate the ability of (n-3) fatty acids to reduce ectopic fat and inflammatory mediators in obese Zucker rats. J. Nutr. 2009, 139, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Ferramosca, A.; Conte, A.; Burri, L.; Berge, K.; de Nuccio, F.; Giudetti, A.M.; Zara, V. A krill oil supplemented diet suppresses hepatic steatosis in high-fat fed rats. PLoS ONE 2012, 7, e38797. [Google Scholar] [CrossRef] [PubMed]
- Fosshaug, L.E.; Berge, R.K.; Beitnes, J.O.; Berge, K.; Vik, H.; Aukrust, P.; Gullestad, L.; Vinge, L.E.; Oie, E. Krill oil attenuates left ventricular dilatation after myocardial infarction in rats. Lipids Health Dis. 2011, 10, 245. [Google Scholar] [CrossRef] [PubMed]
- Vigerust, N.F.; Bjorndal, B.; Bohov, P.; Brattelid, T.; Svardal, A.; Berge, R.K. Krill oil versus fish oil in modulation of inflammation and lipid metabolism in mice transgenic for TNF-alpha. Eur. J. Nutr. 2013, 52, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Ierna, M.; Kerr, A.; Scales, H.; Berge, K.; Griinari, M. Supplementation of diet with krill oil protects against experimental rheumatoid arthritis. BMC Musculoskelet. Disord. 2010, 11, 136. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V.; Griinari, M.; Carta, G.; Murru, E.; Ligresti, A.; Cordeddu, L.; Giordano, E.; Bisogno, T.; Collu, M.; Batetta, B.; et al. Dietary krill oil increases docosahexaenoic acid and reduces 2-arachidonoylglycerol but not n-acylethanolamine levels in the brain of obese Zucker rats. Int. Dairy J. 2010, 20, 231–235. [Google Scholar]
- Piscitelli, F.; Carta, G.; Bisogno, T.; Murru, E.; Cordeddu, L.; Berge, K.; Tandy, S.; Cohn, J.S.; Griinari, M.; Banni, S.; et al. Effect of dietary krill oil supplementation on the endocannabinoidome of metabolically relevant tissues from high-fat-fed mice. Nutr. Metab. (Lond.) 2011, 8, 51. [Google Scholar] [CrossRef]
- Tandy, S.; Chung, R.W.; Wat, E.; Kamili, A.; Berge, K.; Griinari, M.; Cohn, J.S. Dietary krill oil supplementation reduces hepatic steatosis, glycemia, and hypercholesterolemia in high-fat-fed mice. J. Agric. Food Chem. 2009, 57, 9339–9345. [Google Scholar] [CrossRef] [PubMed]
- Tillander, V.; Bjorndal, B.; Burri, L.; Bohov, P.; Skorve, J.; Berge, R.K.; Alexson, S.E. Fish oil and krill oil supplementations differentially regulate lipid catabolic and synthetic pathways in mice. Nutr. Metab. (Lond.) 2014, 11, 20. [Google Scholar] [CrossRef]
- Ivanova, Z.; Bjorndal, B.; Grigorova, N.; Roussenov, A.; Vachkova, E.; Berge, K.; Burri, L.; Berge, R.; Stanilova, S.; Milanova, A.; et al. Effect of fish and krill oil supplementation on glucose tolerance in rabbits with experimentally induced obesity. Eur. J. Nutr. 2014. [Google Scholar] [CrossRef]
- Gigliotti, J.C.; Benedito, V.A.; Livengood, R.; Oldaker, C.; Nanda, N.; Tou, J.C. Feeding different omega-3 polyunsaturated fatty acid sources influences renal fatty acid composition, inflammation, and occurrence of nephrocalcinosis in female sprague-dawley rats. Food Nutr. Sci. 2013, 4, 125–136. [Google Scholar] [CrossRef]
- Zhu, J.J.; Shi, J.H.; Qian, W.B.; Cai, Z.Z.; Li, D. Effects of krill oil on serum lipids of hyperlipidemic rats and human SW480 cells. Lipids Health Dis. 2008, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Gamoh, S. Krill-derived phospholipids rich in n-3 fatty acid improve spatial memory in adult rats. J. Agric. Sci. 2011, 3, 3–12. [Google Scholar]
- Ferramosca, A.; Conte, L.; Zara, V. A krill oil supplemented diet reduces the activities of the mitochondrial tricarboxylate carrier and of the cytosolic lipogenic enzymes in rats. J. Anim. Physiol. Anim. Nutr. 2012, 96, 295–306. [Google Scholar] [CrossRef]
- Burri, L.; Berge, K.; Wibrand, K.; Berge, R.K.; Barger, J.L. Differential effects of krill oil and fish oil on the hepatic transcriptome in mice. Front. Genet. 2011, 2, 45. [Google Scholar] [CrossRef] [PubMed]
- Bjørndal, B.; Vik, B.; Brattelid, T.; Vigerust, N.F.; Burri, L.; Bohov, P.; Nygard, O.; Skorve, J.; Berge, R.K. Krill powder increases liver lipid catabolism and reduces glucose mobilization in tumor necrosis factor-alpha transgenic mice fed a high-fat diet. Metabolism 2012, 61, 1461–1472. [Google Scholar] [CrossRef] [PubMed]
- Gigliotti, J.C.; Smith, A.L.; Jaczynski, J.; Tou, J.C. Determination of the nutritional value, protein quality and safety of krill protein concentrate isolated using an isoelectric solubilization/precipitation technique. Food Chem. 2008, 111, 209–214. [Google Scholar] [CrossRef]
- Gigliotti, J.C.; Smith, A.L.; Jaczynski, J.; Tou, J.C. Consumption of krill protein concentrate prevents early renal injury and nephrocalcinosis in female sprague-dawley rats. Urol. Res. 2011, 39, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Bjørndal, B.; Berge, K.; Barger, J.L.; Berge, R.K.; Burri, L. A krill powder-diet reduces fatty acid and amino acid catabolism while increasing mitochondrial oxidative phosphorylation, a study of the hepatic transcriptome in mice. J. Funct. Foods 2013, 6, 623–630. [Google Scholar] [CrossRef]
- Bridges, K.M.; Gigliotti, J.C.; Altman, S.; Jaczynski, J.; Tou, J.C. Determination of digestibility, tissue deposition, and metabolism of the omega-3 fatty acid content of krill protein concentrate in growing rats. J. Agric. Food Chem. 2010, 58, 2830–2837. [Google Scholar] [CrossRef] [PubMed]
- Berge, K.; Robertson, B.; Burri, L. Safety assessment of superba™ krill powder: Subchronic toxicity study in rats. Toxicol. Rep. 2014, 2, 144–151. [Google Scholar] [CrossRef]
- Maki, K.C.; Reeves, M.S.; Farmer, M.; Griinari, M.; Berge, K.; Vik, H.; Hubacher, R.; Rains, T.M. Krill oil supplementation increases plasma concentrations of eicosapentaenoic and docosahexaenoic acids in overweight and obese men and women. Nutr. Res. 2009, 29, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Ulven, S.M.; Kirkhus, B.; Lamglait, A.; Basu, S.; Elind, E.; Haider, T.; Berge, K.; Vik, H.; Pedersen, J.I. Metabolic effects of krill oil are essentially similar to those of fish oil but at lower dose of EPA and DHA, in healthy volunteers. Lipids 2011, 46, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Schuchardt, J.P.; Schneider, I.; Meyer, H.; Neubronner, J.; von Schacky, C.; Hahn, A. Incorporation of EPA and DHA into plasma phospholipids in response to different omega-3 fatty acid formulations—A comparative bioavailability study of fish oil vs. Krill oil. Lipids Health Dis. 2011, 10, 145. [Google Scholar] [CrossRef] [PubMed]
- Kovatchev, B.; Cox, D.; Hill, R.; Reeve, R.; Robeva, R.; Loboschefski, T. A psychophysiological marker of attention deficit/hyperactivity disorder (ADHD)—Defining the EEG consistency index. Appl. Psychophysiol. Biofeedback 2001, 26, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.A.; Lubar, J.F.; Zimmerman, A.W.; Miller, C.A.; Muenchen, R.A. Quantitative analysis of EEG in boys with attention-deficit-hyperactivity disorder: Controlled study with clinical implications. Pediatr. Neurol. 1992, 8, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Li, Y.; Watkins, B.A. Fat to treat fat: Emerging relationship between dietary PUFA, endocannabinoids, and obesity. Prostaglandins Other Lipid Mediat. 2013, 104–105, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Osei-Hyiaman, D.; DePetrillo, M.; Pacher, P.; Liu, J.; Radaeva, S.; Batkai, S.; Harvey-White, J.; Mackie, K.; Offertaler, L.; Wang, L.; et al. Endocannabinoid activation at hepatic CB1 receptors stimulates fatty acid synthesis and contributes to diet-induced obesity. J. Clin. Investig. 2005, 115, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.J.; Genelhu, V.; Di Marzo, V.; Francischetti, E.A. The endocannabinoid system—Back to the scene of cardiometabolic risk factors control? Horm. Metab. Res. 2014, 46, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; de Chiara, V.; Musella, A.; Sacchetti, L.; Cantarella, C.; Castelli, M.; Cavasinni, F.; Motta, C.; Studer, V.; Bernardi, G.; et al. Preservation of striatal cannabinoid cb1 receptor function correlates with the antianxiety effects of fatty acid amide hydrolase inhibition. Molecular pharmacology 2010, 78, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Fisman, E.Z.; Tenenbaum, A. Adiponectin: A manifold therapeutic target for metabolic syndrome, diabetes, and coronary disease? Cardiovasc. Diabetol. 2014, 13, 103. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, E.; Taddei, G.; Vetuschi, A.; Sferra, R.; Frieri, G.; Ricciardi, G.; Caprilli, R. Dextran sulfate sodium (DSS) colitis in rats: Clinical, structural, and ultrastructural aspects. Dig. Dis. Sci. 1999, 44, 1458–1475. [Google Scholar] [CrossRef] [PubMed]
- Legein, B.; Temmerman, L.; Biessen, E.A.; Lutgens, E. Inflammation and immune system interactions in atherosclerosis. Cell. Mol. Life Sci. 2013, 70, 3847–3869. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Lambadiari, V.; Dimitriadis, G.; Zampelas, A. Metabolic syndrome and cardiometabolic risk factors. Curr. Vasc. Pharmacol. 2013, 11, 858–879. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Jaczynski, J. Gelation of protein recovered from whole antarctic krill (euphausia superba) by isoelectric solubilization/precipitation as affected by functional additives. J. Agric. Food Chem. 2007, 55, 1814–1822. [Google Scholar] [CrossRef] [PubMed]
- Burri, L.; Thoresen, G.H.; Berge, R.K. The role of PPARalpha activation in liver and muscle. PPAR Res. 2010, 2010. [Google Scholar] [CrossRef]
- Vitic, J.; Stevanovic, J. Comparative studies of the serum lipoproteins and lipids in some domestic, laboratory and wild animals. Comp. Biochem. Physiol. B 1993, 106, 223–229. [Google Scholar] [PubMed]
- Amate, L.; Ramirez, M.; Gil, A. Positional analysis of triglycerides and phospholipids rich in long-chain polyunsaturated fatty acids. Lipids 1999, 34, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.S.; Wat, E.; Kamili, A.; Tandy, S. Dietary phospholipids, hepatic lipid metabolism and cardiovascular disease. Curr. Opin. Lipidol. 2008, 19, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Ferramosca, A.; Zara, V. Modulation of hepatic steatosis by dietary fatty acids. World J. Gastroenterol. 2014, 20, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- Hartweg, J.; Perera, R.; Montori, V.; Dinneen, S.; Neil, H.A.; Farmer, A. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2009, 1, CD003205. [Google Scholar]
- Hendrich, S. (n-3) fatty acids: Clinical trials in people with type 2 diabetes. Adv. Nutr. 2010, 1, 3–7. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Sublette, M.E.; Ellis, S.P.; Geant, A.L.; Mann, J.J. Meta-analysis of the effects of eicosapentaenoic acid (EPA) in clinical trials in depression. J. Clin. Psychiatry 2011, 72, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and physical frailty: Two sides of the same coin. Front. Aging Neurosci. 2014, 6, 192. [Google Scholar] [PubMed]
- Johannsen, D.L.; Ravussin, E. The role of mitochondria in health and disease. Curr. Opin. Pharmacol. 2009, 9, 780–786. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burri, L.; Johnsen, L. Krill Products: An Overview of Animal Studies. Nutrients 2015, 7, 3300-3321. https://doi.org/10.3390/nu7053300
Burri L, Johnsen L. Krill Products: An Overview of Animal Studies. Nutrients. 2015; 7(5):3300-3321. https://doi.org/10.3390/nu7053300
Chicago/Turabian StyleBurri, Lena, and Line Johnsen. 2015. "Krill Products: An Overview of Animal Studies" Nutrients 7, no. 5: 3300-3321. https://doi.org/10.3390/nu7053300
APA StyleBurri, L., & Johnsen, L. (2015). Krill Products: An Overview of Animal Studies. Nutrients, 7(5), 3300-3321. https://doi.org/10.3390/nu7053300