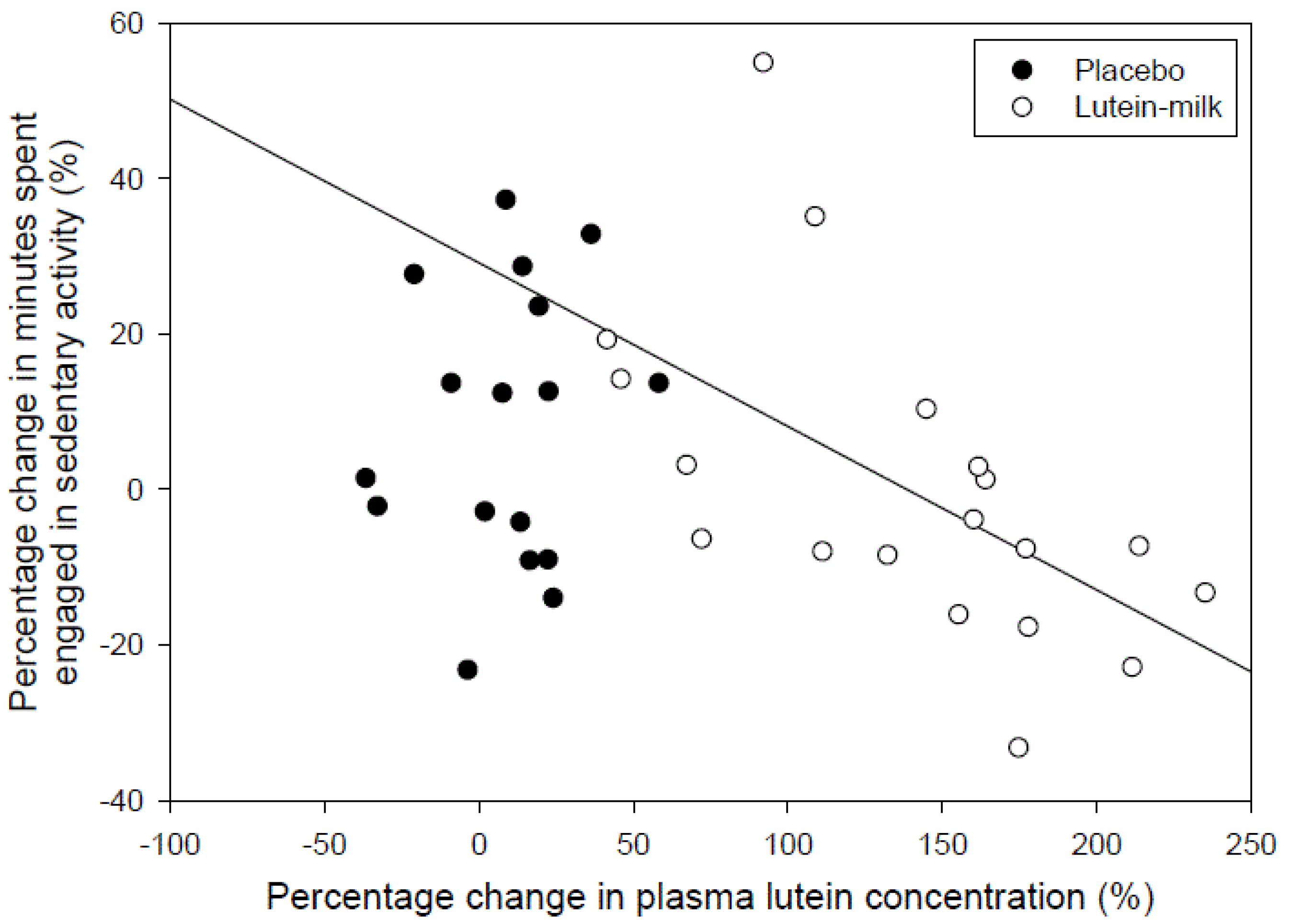
Increases in Plasma Lutein through Supplementation Are Correlated with Increases in Physical Activity and Reductions in Sedentary Time in Older Adults


 ,
,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Protocol

2.3. Physical Activity Program
2.4. Outcome Assessments
2.5. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Lutein | Placebo |
|---|---|---|
| Age (years) | 67.7 ± 7.7 | 67.4 ± 5.5 |
| BMI (kg/m2) | 24.9 ± 2.5 | 25.8 ± 2.6 |
| Weight (kg) ** | 70.3 ± 12.5 | 73.1 ± 10.6 |
| Plasma lutein (μg/dL) | 10.3 ± 2.5 | 10.1 ± 3.6 |
| Plasma zeaxanthin (μg/dL) | 4.3 ± 0.7 | 4.5 ± 0.7 |
| Plasma lutein + zeaxanthin (μg/dL) | 14.6 ± 2.9 | 14.6 ± 4.1 |
| Cholesterol (mmol/L) | 5.0 ± 0.8 | 4.8 ± 0.9 |
| Accelerometer counts per day | 235,292 ± 82,693 | 273,760 ± 85,018 |
| Sedentary time (min/day) | 235 ± 61 | 219 ± 46 |
| Light physical activity (min/day) | 301 ± 88 | 341 ± 76 |
| Moderate to vigorous physical activity (min/day) | 22 ± 14 | 24 ± 18 |
| Steps per day | 7685 ± 2234 | 7632 ± 2092 |
| Exercise self-efficacy | 1204 ± 345 | 1073 ± 425 |
| Outcome | Lutein | Placebo |
|---|---|---|
| Weight (kg) | 0.04 ± 1.12 | 0.02 ± 0.66 |
| Plasma lutein (μg/dL) ** | 13.9 ± 5.7 | 0.09 ± 2.5 |
| Plasma zeaxanthin (μg/dL) * | 0.58 ± 0.50 | 0.09 ± 0.88 |
| Plasma lutein + zeaxanthin (μg/dL) ** | 14.5 ± 5.9 | 0.2 ± 2.7 |
| Counts per day | 49,995 ± 77,384 | 8528 ± 75,691 |
| Sedentary time (min/day) | −3.4 ± 41.6 | 17.7 ± 42.8 |
| Light physical activity (min/day) | 19.0 ± 46.9 | −14.2 ± 70.8 |
| Moderate to vigorous physical activity (min/day) | 8.6 ± 15.2 | 7.1 ± 17.2 |
| Steps per day | 1652 ± 1602 | 948 ± 2054 |
| Exercise self-efficacy | 43 ± 160 | 87 ± 230 |

4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Prince, R.L.; Smith, M.; Dick, I.M.; Price, R.I.; Webb, P.G.; Henderson, N.K.; Harris, M.M. Prevention of postmenopausal osteoporosis. A comparative study of exercise, calcium supplementation, and hormone-replacement therapy. N. Engl. J. Med. 1991, 325, 1189–1195. [Google Scholar] [CrossRef]
- Hunter, D.J.; Eckstein, F. Exercise and osteoarthritis. J. Anat. 2009, 214, 197–207. [Google Scholar] [CrossRef]
- Evans, W.J.; Campbell, W.W. Sarcopenia and age-related changes in body composition and functional capacity. J. Nutr. 1993, 123, 465–468. [Google Scholar]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics (ABS). Physical Activity in Australia: A Snapshot, 2007-08; ABS: Canberra, Australia, 2011. [Google Scholar]
- Gruber, M.; Chappell, R.; Millen, A.; LaRowe, T.; Moeller, S.M.; Iannaccone, A.; Kritchevsky, S.B.; Mares, J. Correlates of Serum Lutein + Zeaxanthin: Findings from the Third National Health and Nutrition Examination Survey. J. Nutr. 2004, 134, 2387–2394. [Google Scholar]
- Rock, C.L.; Thornquist, M.D.; Neuhouser, M.L.; Kristal, A.R.; Neumark-Sztainer, D.; Cooper, D.A.; Patterson, R.E.; Cheskin, L.J. Diet and Lifestyle Correlates of Lutein in the Blood and Diet. J. Nutr. 2002, 132, 525S–530S. [Google Scholar]
- Altman, D.G.; Bland, J.M. Treatment allocation by minimisation. BMJ 2005, 330, 843. [Google Scholar] [CrossRef]
- Department of Health and Ageing. National Physical Activity Guidelines for Adults; Commonwealth of Australia: Canberra, Australia, 2005. [Google Scholar]
- Bandura, A. Guide for Constructing Self-Efficacy Scales. In Self-Efficacy Beliefs of Adolescents; Pajares, F., Urdan, T., Eds.; Information Age Publishing: Charlotte, UC, USA, 2006; pp. 307–337. [Google Scholar]
- Tudor-Locke, C.; Camhi, S.M.; Troiano, R.P. A catalog of rules, variables, and definitions applied to accelerometer data in the National Health and Nutrition Examination Survey, 2003–2006. Prev. Chronic. Dis. 2012, 9, E113. [Google Scholar]
- Jensen, S.K.; Johannsen, A.K.; Hermansen, J.E. Quantitative secretion and maximal secretion capacity of retinol, beta-carotene and alpha-tocopherol into cows’ milk. J. Dairy Res. 1999, 66, 511–522. [Google Scholar] [CrossRef]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J.H. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef]
- Koster, A.; Caserotti, P.; Patel, K.V.; Matthews, C.E.; Berrigan, D.; Van Domelen, D.R.; Brychta, R.J.; Chen, K.Y.; Harris, T.B. Association of Sedentary Time with Mortality Independent of Moderate to Vigorous Physical Activity. PLoS One 2012, 7, e37696. [Google Scholar] [CrossRef]
- Wang, L.; Gaziano, J.M.; Norkus, E.P.; Buring, J.E.; Sesso, H.D. Associations of plasma carotenoids with risk factors and biomarkers related to cardiovascular disease in middle-aged and older women. Am. J. Clin. Nutr. 2008, 88, 747–754. [Google Scholar]
- Kabat, G.C.; Kim, M.Y.; Sarto, G.E.; Shikany, J.M.; Rohan, T.E. Repeated measurements of serum carotenoid, retinol and tocopherol levels in relation to colorectal cancer risk in the Women’s Health Initiative. Eur. J. Clin. Nutr. 2012, 66, 549–554. [Google Scholar] [CrossRef]
- George, S.M.; Thompson, F.E.; Midthune, D.; Subar, A.F.; Berrigan, D.; Schatzkin, A.; Potischman, N. Strength of the relationships between three self-reported dietary intake instruments and serum carotenoids: The Observing Energy and Protein Nutrition (OPEN) Study. Public Health Nutr. 2012, 15, 1000–1007. [Google Scholar] [CrossRef]
- Zou, Z.; Xu, X.; Huang, Y.; Xiao, X.; Ma, L.; Sun, T.; Dong, P.; Wang, X.; Lin, X. High serum level of lutein may be protective against early atherosclerosis: The Beijing atherosclerosis study. Atherosclerosis 2011, 219, 789–793. [Google Scholar] [CrossRef]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Cook, D.G. What factors are associated with physical activity in older people, assessed objectively by accelerometry? Br. J. Sports Med. 2009, 43, 442–450. [Google Scholar] [CrossRef]
- Zaripheh, S.; Erdman, J.W., Jr. Factors that influence the bioavailablity of xanthophylls. J. Nutr. 2002, 132, 531S–534S. [Google Scholar]
- Roodenburg, A.J.; Leenen, R.; van het Hof, K.H.; Weststrate, J.A.; Tijburg, L.B. Amount of fat in the diet affects bioavailability of lutein esters but not of alpha-carotene, beta-carotene, and vitamin E in humans. Am. J. Clin. Nutr. 2000, 71, 1187–1193. [Google Scholar]
- Johnson, E.; Vishwanathan, R.; Scott, T.; Schlach, W.; Wittwer, J.; Hausman, D.; Davey, A.; Johnson, M.; Green, R.; Gearing, M.; et al. Serum carotenoids as a biomarker for carotenoid concentrations in the brain. FASEB J. 2011, 25, 344–342. [Google Scholar]
- Johnson, E.J.; McDonald, K.; Caldarella, S.M.; Chung, H.Y.; Troen, A.M.; Snodderly, D.M. Cognitive findings of an exploratory trial of docosahexaenoic acid and lutein supplementation in older women. Nutr. Neurosci. 2008, 11, 75–83. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Thomson, R.L.; Coates, A.M.; Howe, P.R.C.; Bryan, J.; Matsumoto, M.; Buckley, J.D. Increases in Plasma Lutein through Supplementation Are Correlated with Increases in Physical Activity and Reductions in Sedentary Time in Older Adults. Nutrients 2014, 6, 974-984. https://doi.org/10.3390/nu6030974
Thomson RL, Coates AM, Howe PRC, Bryan J, Matsumoto M, Buckley JD. Increases in Plasma Lutein through Supplementation Are Correlated with Increases in Physical Activity and Reductions in Sedentary Time in Older Adults. Nutrients. 2014; 6(3):974-984. https://doi.org/10.3390/nu6030974
Chicago/Turabian StyleThomson, Rebecca L., Alison M. Coates, Peter R. C. Howe, Janet Bryan, Megumi Matsumoto, and Jonathan D. Buckley. 2014. "Increases in Plasma Lutein through Supplementation Are Correlated with Increases in Physical Activity and Reductions in Sedentary Time in Older Adults" Nutrients 6, no. 3: 974-984. https://doi.org/10.3390/nu6030974
APA StyleThomson, R. L., Coates, A. M., Howe, P. R. C., Bryan, J., Matsumoto, M., & Buckley, J. D. (2014). Increases in Plasma Lutein through Supplementation Are Correlated with Increases in Physical Activity and Reductions in Sedentary Time in Older Adults. Nutrients, 6(3), 974-984. https://doi.org/10.3390/nu6030974