Dietary Factors and Type 2 Diabetes in the Middle East: What Is the Evidence for an Association?––A Systematic Review


Abstract
:1. Introduction
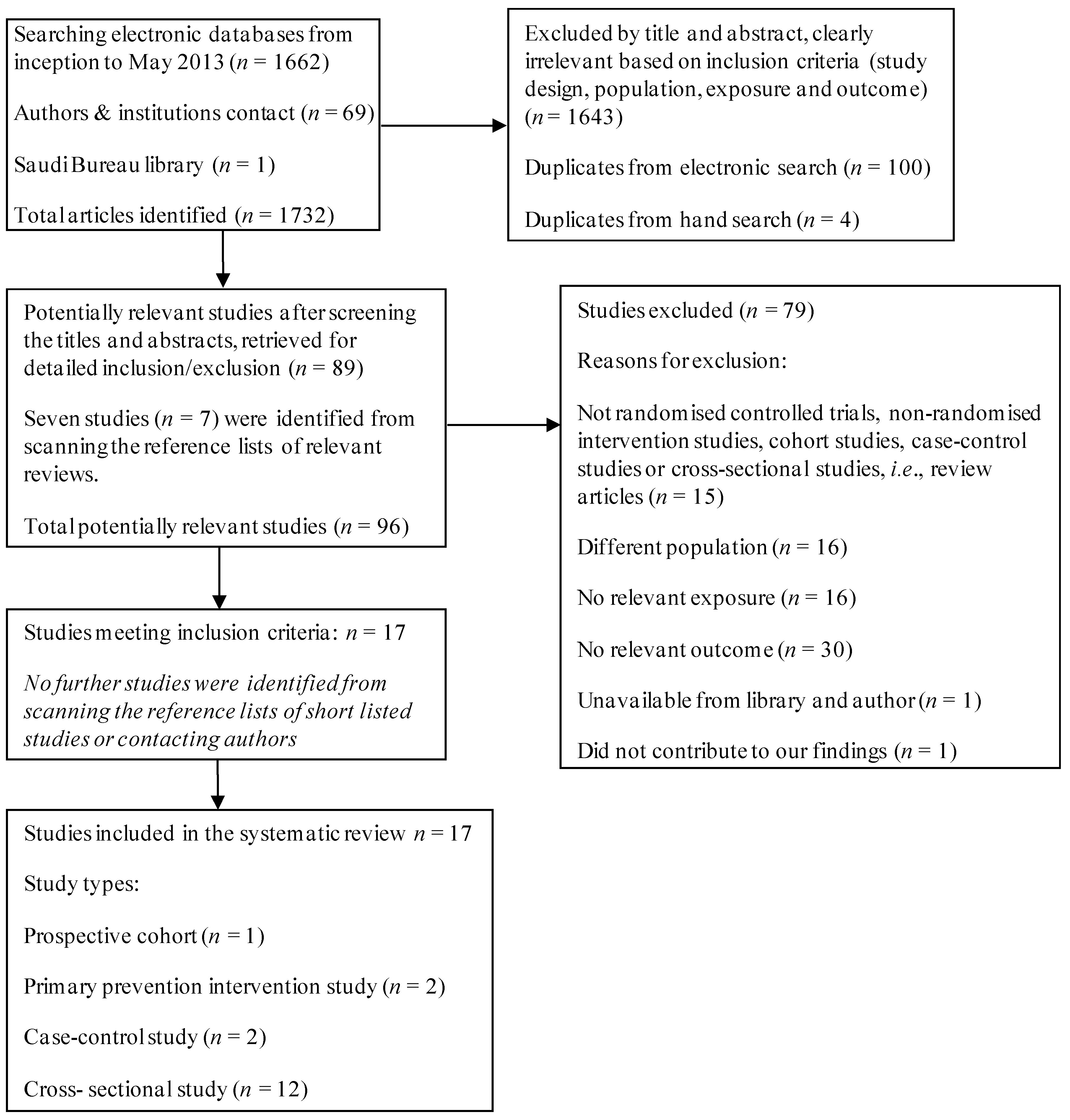
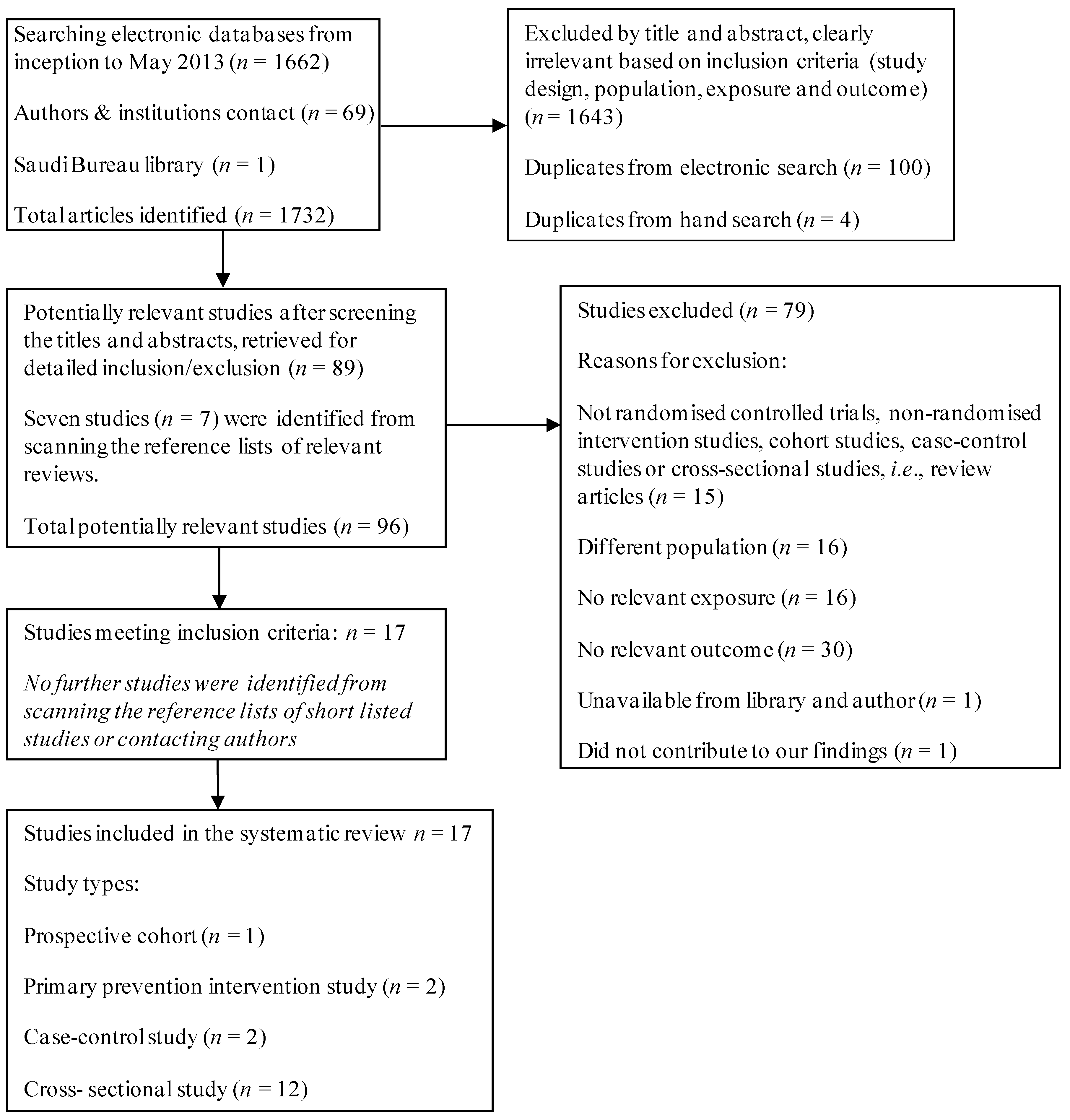
2. Materials and Methods
3. Results

{kind=link}
| Author | Study design | Country/study population | Sample size | Sex (%) | Age (years) | DietaryAssessment method | Dietary factor | Results |
|---|---|---|---|---|---|---|---|---|
| Energy and nutrients | ||||||||
| Kahn et al., 1971 [34] | Prospective cohort. Follow-up: 2 years | Israeli civil-services employees | 8369 | M: 100 | >40 | Short dietary questionnaire | Total calories (kcal/day), total carbohydrate (g/day), animal protein (g/day), saturated fatty acid (g/day), and sugar calories (kcal/day). | There was no association between dietary variables assessed and T2DM incidence. |
| Foods | ||||||||
| Midhet et al., 2010 [35] | Case-control | Saudi Arabian PHCC’s attendees | 498 | M: 48.6 F: 51.4 | 30–70 | Food preference questions and 24-h DR | Food items consumed regularly, Kabsa (rice/chicken with rice), dates, fish, vegetables, bakery items, potato chips and/or French fries, snacks and hummus, full fat dairy products, coffee and/or tea with sugar, juices and soft drinks. | Routine consumption of Kabsa (OR 5.5, CI: 2.3–13.5), bakery items (OR 2.4, CI: 1.3–4.6), French fries (OR 2.2, CI: 1.2–3.9) and fish (OR 2.5, CI: 1.3–4.7) were associated with an increased risk of T2DM. Vegetables showed a protective effect (OR 0.4, CI: 0.2–0.7). |
| Ezmaillzadeh et al., 2005 [36] | Cross-sectional | Iranian residents | 827 | M: 43.2 F: 56.8 | 18–74 | Validated 168-items FFQ (Willet format) | Whole-grain foods (e.g., dark breads, barley bread, popcorn, whole-grain breakfast cereal, wheat germ and bulgur). Refined grain foods (e.g., white breads, iceberg bread, noodle, pasta, rice, toasted bread, milled barley, sweet bread, white flour, starch and biscuits). | The highest quartile of whole-grain consumption was associated with a reduced risk of T2DM (OR 0.88, CI: 0.8, 0.94) as compared to the reference category (p < 0.05). There was no significant increase in the risk of diabetes with refined-grain consumption (highest category OR 1.14, CI: 0.87–2.52) |
| Esmillzadeh et al., 2011 [37] | Cross-sectional | Iranian teachers | 486 | F: 100 | ≥40 | Validated 168-items FFQ (Willet format) | Vegetable oil which included partially hydrogenated vegetable oil (PHVO) and non-hydrogenated vegetable oil (NHVO) (e.g., soyabean oil, olive oil, sunflower oil, maize oil, rapeseed oil). | No significant association was found between PHVO (p = 0.31) or NHVO (p = 0.19) and diabetes. However, diabetes prevalence increased across PHVO quintiles, and decreased across NHVO quintiles. |
| Khosravi-Boroujeni et al., 2012 [38] | Cross-sectional | Iranian residents | 4774 | M: 76 F: 24 | >19 | Validated 49-items FFQ | Potato consumption. | There was a positive association (p < 0.001) between potato intake and risk of diabetes (OR 1.38, CI: 1.41–1.67). |
| Beverages | ||||||||
| Golozar et al., 2011 [39] | Cross-sectional | Iranian residents | 50,039 | M: 42.4 F: 57.6 | ≥30 | Validated 158-items FFQ | Green and black tea consumption (mL/day). | Heavy green tea consumption (≥600 mL/day) was positively associated with T2DM (prevalence ratio (PR) 1.24, CI: 1.05–1.47) |
| Energy density | ||||||||
| Esmillzadeh et al., 2012 [40] | Cross-sectional | Iranian teachers | 486 | F: 100 | ≥40 | Validated 168-items FFQ (Willet format) | Dietary energy density (DED) from food (kcal/g) 1. | No significant association between the highest quartile of DEDFood (prevalence ration (PR): 1.06, CI: 0.42–2.73) and diabetes. |
| Kalter-Leibovici et al., 2012 [41] | Cross-sectional | Israel (Jewish and Arab residents) | 1092 | M: 49.6 F: 50.4 | ≥25 | 240-items FFQ | DEDFood + Beverages (kcal/g) 2 | Arabs with diabetes were more likely to be in the highest quartiles of DED (29.5% vs. 35.4%). The risk of diabetes was significantly higher in highest quartiles of DED (adjusted hazards ratio: 1.67, CI: 1.08–2.61) in comparison to lower quartiles (adjusted hazards ratio: 1.53, CI: 0.98–2.39). |
| Author | Study design | Country/study population | Sample size | Sex (%) | Age (years) | Dietary | Dietary factor | Results |
|---|---|---|---|---|---|---|---|---|
| Assessment method | ||||||||
| A priori Dietary Patterns | ||||||||
| Bilenko et al., 2005 [42] | Cross-sectional | Israeli residents | 1159 | M: 44.9 F: 55.1 | ≥35 | 24-h DR | Mediterranean dietary score 1. | No significant difference was observed across Mediterranean diet score categories (low or high) and the prevalence of diabetes in both males and females. |
| Azadbakht et al., 2006 [43] | Cross-sectional | Iranian residents | 581 | M: 51 F: 49 | ≥18 | Validated 168-items FFQ (Willet format) | Dietary diversity score (DDS) 2, which was from the five main food groups of the Food Guide Pyramid (bread/grains, fruits, vegetables, dairy, meat and meat substitutes). The five groups were divided into 23 (e.g., vegetables: vegetables, potatoes, tomatoes, starchy vegetables, legumes, yellow vegetables, green vegetables). | Although there was no protective effect of healthier diet score against diabetes, the risk of diabetes decreased significantly across quartiles of DDS (p = 0.03). Quartiles of DDS for whole-grains (OR-Q1 1.45, CI: 1.09-1.88 vs. OR-Q3 1.11, CI: 0.89–1.44), and vegetables (OR-Q1 1.12, CI: 0.54–1.88 vs. OR-Q3 1.05, CI: 0.89–1.34) did not have an inverse association with diabetes. |
| Naja et al., 2012 [44] | Case-control | Lebanon (cases: Lebanese private clinic attendees, controls: Lebanese residents) | 174 | M: 60.3 F: 39.7 | >18 | 97-items FFQ | 4 dietary patterns, Refined Grains and Desserts (e.g., pasta, pizza, deserts), Traditional Lebanese (e.g., whole wheat bread, olives and olive oil), Fast Food (e.g., mixed nuts, French fries, and full fat milk), and Meat and Alcohol patterns (e.g., red meat, eggs, carbonated beverages). | The Traditional Lebanese pattern showed significantly lower odds of T2DM (OR 0.46, CI: 0.22–0.97) while the Refined Grains (OR 3.85, CI: 1.31–11.23) and the Fast Food patterns (OR 2.80, CI: 1.41–5.59) significantly increased the odds of T2DM in Lebanese adults. |
| Esmillzadeh et al., 2008 [45] | Cross-sectional | Iranian teachers | 486 | F: 100 | ≥40 | Validated 168-items FFQ (Willet format) | 3 dietary patterns, Healthy (e.g., fruits, vegetables, legumes), Western (e.g., red meat, butter, pizza), and Iranian patterns (e.g., refined grains, potato, broth). | The prevalence of diabetes decreased significantly among quintiles of Healthy pattern (p < 0.05) and increased among quintiles of Western (p < 0.05) and Iranian patterns (p = 0.24). The Healthy pattern had a protective effect against diabetes (OR 0.29, CI: 0.11–1.07, p = 0.07). |
| Abu-Saad et al., 2012 [46] | Cross-sectional | Israel (Jewish and Arab residents) | 1104 | M: 50 F: 50 | ≥25 | 240-items FFQ | 4 dietary patterns, Ethnic (e.g., pita bread, olive oil and Arabic mixed meat), Healthy (e.g., fruits, low fat dairy products and whole grains), Fish and Meat Dishes (fish, meat and frying oil), Middle Eastern snacks and Fast Food patterns (e.g., savoury cheese, nuts, and fast food). | Scores for the Healthy and Ethnic pattern clearly differed by ethnicity. Hence, the two patterns were used for further analysis. The prevalence of diabetes was higher in increased tertiles of Ethnic pattern (T3 20% vs. T1–2 13%, p = 0.001), and participants with prevalent diabetes were more likely to be in the highest tertiles of Healthy pattern (T3 25% vs. T1–2 10%, p < 0.001). Arabs with prevalent diabetes were more likely to be in the highest tertiles of the healthy pattern (OR 5.00, CI: 2.92–8.55) in comparison to Jews with diabetes (OR 2.00, CI: 1.01–3.95). |
| Other Dietary Patterns | ||||||||
| Al Ali et al., 2011 [47] | Cross-sectional | Syrian residents | 1168 | M: 47.7 F: 52.3 | ≥25 | Frequency questionnaire | Healthy and unhealthy diets 3. | Frequent fruit and vegetable consumption was associated with a reduced risk of T2DM (OR 0.70, CI: 0.48–1.03), but this did not reach statistical significance. |
| Alrabadi et al., 2013 [48] | Cross-sectional | Jordanian residents | 286 | M: 49 F: 51 | >40 | Questionnaire | Vegetarianism 4. | The prevalence of diabetes was significantly lower among vegetarians (38%) in comparison to non-vegetarians (44%). |
| Author | Study design | Country/study population | Sample size | Sex (%) | Age (years) | Follow-up (Years) | Intervention | Results |
|---|---|---|---|---|---|---|---|---|
| Harati et al., 2010 [50] | Primary prevention intervention study | Iranian residence | 8212 | M: 41 F: 59 | >20 | 3.6 | Intervention: At baseline: intensive education to increase physical activity, reduce cigarette smoking, and face-to-face educational interviews to improve nutritional habits. The lifestyle modification intervention was based on guidelines recommendations by The American Heart Association and modified to suit the Iranian knowledge, attitude and practice that were assessed in a previous study (KAP study) [51]. Dieticians providing tailored nutrition interventions such as weight reduction diet, exchange list education, diet management, DASH diet, and ADA nutrition principles. For the next 2.6 years: nutritional classes (held for 4 days/week at clinics), group meetings, public sites, publications, public conferences, distribution of education materials and school-based programs were carried out. Control: Did not receive the intervention. | The lifestyle modification programme resulted in a statistically significant relative risk reduction of 65% in the incidence of diabetes (95% CI = 30%, 83%, p = 0.003). The incidence of diabetes was 8.2 per 1000 person-years in the intervention groups in comparison to 12.2 per 1000 person-years in the control group. |
| Sarrafzad-egan et al., 2013 [52] | Primary prevention intervention study | Iranian residence | 12,514 baseline (2001–2002) 9570 post-intervention (2007) | M: 50 F: 50 | ≥19 | 4 | Intervention: interventions began at different times throughout the study and were at a community level using different approaches (e.g., mass media, health services). Improve healthy eating, increase physical activity, reduce tobacco smoking and cope with stress. Additional secondary preventative measures were delivered to high-risk individuals (e.g., people with diabetes). Projects were tailored to meet participants needs (e.g., Healthy-lifestyles for High-risk Populations, Healthy Food for Healthy Communities, Isfahan Exercise Project, and Healthy Lifestyles for High-risk Populations). Control: Did not receive the intervention. | The prevalence of diabetes did not decrease in the intervention group in both females (2001: 6.8%, 2007: 7.1%, p = 0.38) and males (2001: 5.8%, 2007: 7.1%, p = 0.17). However, there was a borderline significant increase in males of the reference group (2001: 4.0%, 2007: 5.7%, p = 0.056), and a non-significant increase in females of the reference group (2001: 5.8%, 2007: 7.3%, p = 0.15). |
3.1. Association of Energy, Nutrients, Foods, and Beverages with T2DM
3.1.1. Energy and Nutrients
3.1.2. Foods
3.1.3. Beverages
3.1.4. Energy Density
3.2. Association between Dietary Patterns and T2DM
3.2.1. A Priori Dietary Patterns
3.2.2. A Posteriori Dietary Patterns
3.2.3. Other Patterns
3.3. Association between Lifestyle Factors and T2DM
4. Methodological Quality of Included Studies
| Cohort Study | Selection | Comparability | Outcome |
|---|---|---|---|
| Kahn et al. [34] | ** | * | * |
| Case-control Study | Selection | Comparability | Exposure |
| Midhet et al. [35] | **** | ** | * |
| Naja et al. [44] | **** | ** | ** |
5. Discussion
6. Conclusions
Conflicts of Interest
References
- Zhang, P.; Zhang, X.; Brown, J.; Vistisen, D.; Sicree, R.; Shaw, J.; Nichols, G. Global healthcare expenditure on diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2010, 87, 293–301. [Google Scholar] [CrossRef]
- Shaw, J.E.; Sicree, R.A.; Zimmet, P.Z. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2009, 87, 4–14. [Google Scholar]
- Boyle, J.; Thompson, T.; Gregg, E.; Barker, L.; Williamson, D. Projection of the year 2050 burden of diabetes in the US adult population: Dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 2010, 8, 29. [Google Scholar] [CrossRef]
- Willett, W.C. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998; pp. 50–74. [Google Scholar]
- Parillo, M.; Riccardi, G. Diet composition and the risk of type 2 diabetes: Epidimiological and clinical evidence. Br. J. Nutr. 2004, 92, 7–19. [Google Scholar] [CrossRef]
- Gross, L.S.; Li, L.; Ford, E.S.; Liu, S. Increased consumption of refined carbohydrates and the epidemic of type 2 diabetes in the United States: An ecologic assessment. Am. J. Clin. Nutr. 2004, 79, 774–779. [Google Scholar]
- Sluijs, I.; Beulens, J.W.J.; van der A, D.L.; Spijkerman, A.M.W.; Grobbee, D.E.; van der Schouw, Y.T. Dietary intake of total, animal, and vegetable protein and risk of Type 2 diabetes in the european prospective investigation into cancer and nutrition (EPIC)-NL study. Diabetes Care 2010, 33, 43–48. [Google Scholar] [CrossRef]
- Sun, Q.; Spiegelman, D.; van Dam, R.M.; Holmes, M.D.; Malik, V.S.; Walter, C.; Willett, W.C.; Hu, F.B. White rice, brown rice, and risk of Type 2 diabetes in US men and women. Arch. Intern. Med. 2010, 170, 961–969. [Google Scholar] [CrossRef]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and the incidence of type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ 2010, 341, c4229. [Google Scholar] [CrossRef]
- He, M.; van Dam, R.M.; Rimm, E.B.; Hu, F.B.; Qi, L. Whole-Grain, cereal fiber, bran and germ intake and the risk of all-cause and cardiovascular disease specific mortality among women with Type 2 diabetes millitus. Circulation 2010, 121, 2162–2168. [Google Scholar] [CrossRef]
- Hu, F.B.; Malik, V.S. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: Epidemiologic evidence. Physiol. Behav. 2010, 100, 47–54. [Google Scholar] [CrossRef]
- Wang, J.; Luben, R.; Khaw, K.-T.; Bingham, S.; Wareham, N.J.; Forouhi, N.G. Dietary energy density predicts the risk of incident Type 2 diabetes: The european prospective investigation of cancer (EPIC)-Norfolk study. Diabetes Care 2008, 31, 2120–2125. [Google Scholar] [CrossRef]
- Mendoza, J.A.; Drewnowski, A.; Christakis, D.A. Dietary energy density is associated with obesity and the metabolic syndrome in US adults. Diabetes Care 2007, 30, 974–979. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Brunner, E.J.; Mosdøl, A.; Witte, D.R.; Martikainen, P.; Stafford, M.; Shipley, M.J.; Marmot, M.G. Dietary patterns and 15-y risks of major coronary events, diabetes, and mortality. Am. J. Clin. Nutr. 2008, 87, 1414–1421. [Google Scholar]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Arch. Intern. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef]
- Schulze, M.B.; Hoffmann, K.; Manson, J.E.; Willett, W.C.; Meigs, J.B.; Weikert, C.; Heidemann, C.; Colditz, G.A.; Hu, F.B. Dietary pattern, inflammation, and incidence of type 2 diabetes in women. Am. J. Clin. Nutr. 2005, 82, 675–684. [Google Scholar]
- Hodge, A.M.; English, D.R.; O’Dea, K.; Giles, G.G. Dietary patterns and diabetes incidence in the melbourne collaborative cohort study. Am. J. Epidemiol. 2007, 165, 603–610. [Google Scholar] [CrossRef]
- Sartor, G.; Scherstén, B.; Carlström, S.; Melander, A.; Nordén, A.; Persson, G. Ten-year follow-up of subjects with impaired glucose tolerance: Prevention of diabetes by tolbutamide and diet regulation. Diabetes 1980, 29, 41–49. [Google Scholar] [CrossRef]
- Rowley, K.G.; Daniel, M.; Skinner, K.; Skinner, M.; White, G.A.; O’Dea, K. Effectiveness of a community-directed “healthy lifestyle” program in a remote Australian Aboriginal community. Aust. N. Z. J. Public Health 2000, 24, 136–144. [Google Scholar] [CrossRef]
- Eriksson, K.-F.; Lindgärde, F. Prevention of Type 2 (non-insulin-dependent) diabetes mellitus by diet and physical exercise: The 6-year Malmö feasibility study. Diabetologia 1991, 34, 891–898. [Google Scholar] [CrossRef]
- Lindström, J.; Louheranta, A.; Mannelin, M.; Rastas, M.; Salminen, V.; Eriksson, J.; Uusitupa, M.; Tuomilehto, J. The finnish diabetes prevention study (DPS). Diabetes Care 2003, 26, 3230–3236. [Google Scholar] [CrossRef]
- Uusitupa, M.; Tuomilehto, J.; Puska, P. Are we really active in the prevention of obesity and type 2 diabetes at the community level? Nutr. Metab. Cardiovasc. Dis. 2011, 21, 380–389. [Google Scholar] [CrossRef]
- AI-Othaimeen, A.I.; AI-Nozha, M.; Osman, A.K. Obesity: An emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East. Mediterr. Health J. 2007, 13, 441–448. [Google Scholar]
- Elhadd, T.A.; Al-Amoudi, A.A.; Alzahrani, A.S. Epidemiology, clinical and complications profile of diabetes in Saudi Arabia: A review. Ann. Saudi. Med. 2007, 27, 241–250. [Google Scholar] [CrossRef]
- Musaiger, A.O. Overweight and obesity in the Eastern Medirerranean Region: Can we control it? East. Mediterr. Health J. 2004, 10, 789–793. [Google Scholar]
- Musaiger, A.O.; Al-Hazzaa, H.M. Prevalence and risk factors associated with nutrition-related noncommunicable diseases in the Eastern Mediterranean region. Int. J. Gen. Med. 2012, 5, 199–217. [Google Scholar] [CrossRef]
- Al-Shoshan, A. The affluent diet and its consequences: Saudi Arabai—A case in point. World Rev. Nutr. Diet. 1992, 69, 113–165. [Google Scholar]
- Amuna, P.; Zotor, F. The epidimiological and nutrition transition in developing countries: Evolving trends and their impact in public health and human development. Proc. Nutr. Soc. 2008, 67, 82–90. [Google Scholar] [CrossRef]
- Nielsen, J.V. Diabetes in the Arab World: Prevalence and risk factors. Pract. Diabetes Int. 1999, 16, 82–86. [Google Scholar] [CrossRef]
- Ng, S.W.; Zaghloul, S.; Ali, H.I.; Harrison, G.; Popkin, B.M. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes. Rev. 2011, 12, 1–13. [Google Scholar]
- AL-Majwal, A.; Williams, P.; Batterham, M. Current dietetic practices of obesity management in Saudi Arabia and comparison with Australian practices and best practice criteria. Nutr. Diet. 2009, 66, 94–100. [Google Scholar] [CrossRef]
- Amini, M.; Shafaeizadeh, S.; Zare, M.; Khosravi Boroujeni, H.; Esmaillzadeh, A. A cross-sectional study on food patterns and adiposity among individuals with abnormal glucose homeostasis. Arch. Iran. Med. 2012, 15, 131–135. [Google Scholar]
- Kahn, H.A.; Herman, J.B.; Medalie, J.H.; Neufeld, H.N.; Riss, E.; Goldbourt, U. Factors related to diabetes incidence: A multivariate analysis of two years observation on 10,000 men. The Israel Ischemic Heart Disease Study. J. Chronic Dis. 1971, 23, 617–629. [Google Scholar] [CrossRef]
- Midhet, F.M.; Al-Mohaimeed, A.A.; Sharaf, F.K. Lifestyle related risk factors of type 2 diabetes mellitus in Saudi Arabia. Saudi Med. J. 2010, 31, 768–774. [Google Scholar]
- Esmaillzadeh, A.; Mirmiran, P.; Azizi, F. Whole-grain consumption and the metabolic syndrome: A favorable association in Tehranian adults. Eur. J. Clin. Nutr. 2005, 59, 353–362. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Azadbakht, L. Different kinds of vegetable oils in relation to individual cardiovascular risk factors among Iranian women. Br. J. Nutr. 2011, 105, 919–927. [Google Scholar] [CrossRef]
- Khosravi-Boroujeni, H.; Mohammadifard, N.; Sarrafzadegan, N.; Sajjadi, F.; Maghroun, M.; Khosravi, A.; Alikhasi, H.; Rafieian, M.; Azadbakht, L. Potato consumption and cardiovascular disease risk factors among Iranian population. Int. J. Food. Sci. Nutr. 2012, 63, 913–920. [Google Scholar] [CrossRef]
- Golozar, A.; Khademi, H.; Kamangar, F.; Poutschi, H.; Islami, F.; Abnet, C.C.; Freedman, N.D.; Taylor, P.R.; Pharoah, P.; Boffetta, P.; et al. Diabetes mellitus and its correlates in an iranian adult population. PLoS One 2011, 6, e26725. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Khosravi Boroujeni, H.; Azadbakht, L. Consumption of energy-dense diets in relation to cardiometabolic abnormalities among Iranian women. Public Health Nutr. 2012, 15, 868–875. [Google Scholar] [CrossRef]
- Kalter-Leibovici, O.; Chetrit, A.; Lubin, F.; Atamna, A.; Alpert, G.; Ziv, A.; Abu-Saad, K.; Murad, H.; Eilat-Adar, S.; Goldbourt, U. Adult-onset diabetes among Arabs and Jews in Israel: A population-based study. Diabet. Med. 2012, 29, 748–754. [Google Scholar] [CrossRef]
- Bilenko, N.; Fraser, D.; Vardi, H.; Shai, I.; Shahar, D.R. Mediterranean diet and cardiovascular diseases in an Israeli population. Prev. Med. 2005, 40, 299–305. [Google Scholar] [CrossRef]
- Azadbakht, L.; Mirmiran, P.; Esmaillzadeh, A.; Azizi, F. Dietary diversity score and cardiovascular risk factors in Tehranian adults. Public Health Nutr. 2006, 9, 728–736. [Google Scholar]
- Naja, F.; Hwalla, N.; Itani, L.; Salem, M.; Azar, S.T.; Zeidan, M.N.; Nasreddine, L. Dietary patterns and odds of Type 2 diabetes in Beirut, Lebanon: A case–control study. Nutr. Metab. (Lond.) 2012, 9. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Azadbakht, L. Food intake patterns may explain the high prevalence of cardiovascular risk factors among Iranian women. J. Nutr. 2008, 138, 1469–1475. [Google Scholar]
- Abu-Saad, K.; Murad, H.; Lubin, F.; Freedman, L.S.; Ziv, A.; Alpert, G.; Atamna, A.; Kalter-Leibovici, O. Jews and Arabs in the same region in Israel exhibit major differences in dietary patterns. J. Nutr. 2012, 142, 2175–2181. [Google Scholar] [CrossRef]
- Al Ali, R.; Rastam, S.; Fouad, F.M.; Mzayek, F.; Maziak, W. Modifiable cardiovascular risk factors among adults in Aleppo, Syria. Int. J. Public Health 2011, 56, 653–662. [Google Scholar] [CrossRef]
- Alrabadi, N.I. The effect of lifestyle food on chronic diseases: A comparison between vegetarians and non-vegetarians in Jordan. Glob. J. Health Sci. 2013, 5, 65–69. [Google Scholar]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef]
- Harati, H.; Hadaegh, F.; Momenan, A.A.; Ghanei, L.; Bozorgmanesh, M.R.; Ghanbarian, A.; Mimiran, P.; Azizi, F. Reduction in inidence of Type 2 diabetes by lifestyle intervention in a Middle Eastern Community. Am. J. Prev. Med. 2010, 38, 628–636. [Google Scholar] [CrossRef]
- Azizi, F.; Ghanbarian, A. Prevention of non communicable disease in a population in nutrition transmition: Tehran Lipid and Glucose Study phase II. Trials 2009, 10. [Google Scholar] [CrossRef]
- Sarrafzadegan, N.; Kelishadi, R.; Sadri, G.; Malekafzali, H.; Pourmoghaddas, M.; Heidari, K.; Shirani, S.; Bahonar, A.; Boshtam, M.; Asgary, S.; et al. Outcomes of a comprehensive healthy lifestyle program on cardiometabolic risk factors in a developing country: The isfahan healthy heart program. Arch. Iran. Med. 2013, 16, 4–11. [Google Scholar]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration, 2011. Available online: www.cochrane-handbook.org (accessed on 1 June 2013).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 June 2013).
- Alhazmi, A.; Stojanovski, E.; McEvoy, M.; Garg, M.L. Macronutrient intakes and development of type 2 diabetes: A systematic review and meta-analysis of cohort studies. J. Am. Coll. Nutr. 2012, 31, 243–258. [Google Scholar] [CrossRef]
- Van Dam, R.M.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J.; Hu, F.B. Dietary fat and meat intake in relation to risk of Type 2 diabetes in men. Diabetes Care 2002, 25, 417–424. [Google Scholar] [CrossRef]
- Fung, T.T.; Hu, F.B.; Pereira, M.A.; Liu, S.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C. Whole-Grain intake and the risk of type 2 diabetes: A prospective study in men. Am. J. Clin. Nutr. 2002, 76, 535–540. [Google Scholar]
- McKeown, N.M.; Meigs, J.B.; Liu, S.; Wilson, P.W.; Jacques, P.F. Whole-Grain intake is favorably associated with metabolic risk factors for type 2 diabetes and cardiovascular disease in the Framingham Offspring Study. Am. J. Clin. Nutr. 2002, 76, 390–398. [Google Scholar]
- De Munter, J.S.L.; Hu, F.B.; Spiegelman, D.; Franz, M.; van Dam, R.M. Whole grain, bran, and germ intake and risk of Type 2 diabetes: A prospective cohort study and systematic review. PLoS Med. 2007, 4, e261. [Google Scholar] [CrossRef]
- Esposito, K.; Giugliano, D. Increased consumption of green leafy vegetables, but not fruit, vegetables or fruit and vegetables combined, is associated with reduced incidence of type 2 diabets. Evid. Based Med. 2011, 16, 27–28. [Google Scholar] [CrossRef]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B. Potato and french fry consumption and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2006, 83, 284–290. [Google Scholar]
- Tonstad, S.; Butler, T.; Yan, R.; Fraser, G.E. Type of vegetarian diet, body weight, and prevalence of Type 2 diabetes. Diabetes Care 2009, 32, 791–796. [Google Scholar] [CrossRef]
- Colditz, G.A.; Manson, J.E.; Stampfer, M.J.; Rosner, B.; Willett, W.C.; Speizer, F.E. Diet and risk of clinical diabetes in women. Am. J. Clin. Nutr. 1992, 55, 1018–1023. [Google Scholar]
- Johnson, L.; Wilks, D.; Lindroos, A.; Jebb, S. Reflections from a systematic review of dietary energy density and weight gain: Is the inclusion of drinks valid? Obes. Rev. 2009, 10, 681–692. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Azadbakht, L. Dietary energy density and the metabolic syndrome among Iranian women. Eur. J. Clin. Nutr. 2011, 65, 598–605. [Google Scholar] [CrossRef]
- Perez-Escamilla, R.; Obbagy, J.E.; Altman, J.M.; Essery, E.V.; McGrane, M.M.; Wong, Y.P.; Spahn, J.M.; Williams, C.L. Dietary energy density and body weight in adults and children: A systematic review. J. Acad. Nutr. Diet. 2012, 112, 671–684. [Google Scholar] [CrossRef]
- Schatzkin, A.; Kipnis, V.; Carroll, R.J.; Midthune, D.; Subar, A.F.; Bingham, S.; Schoeller, D.A.; Troiano, R.P.; Freedman, L.S. A comparison of a food frequency questionnaire with a 24-hour recall for use in an epidemiological cohort study: Results from the biomarker-based Observing Protein and Energy Nutrition (OPEN) study. Int. J. Epidemiol. 2003, 32, 1054–1062. [Google Scholar] [CrossRef]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.K.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary patterns: Challenges and opportunities in dietary patterns research: An experimental biology workshop, April 1, 2006. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef]
- Lutsey, P.L.; Steffen, L.M.; Stevens, J. Dietary intake and the development of the metabolic syndrome: The atherosclerosis risk in communities study. Circulation 2008, 117, 754–761. [Google Scholar] [CrossRef]
- Baxter, A.J.; Coyne, T.; McClintock, C. Dietary patterns and metabolic syndrome-a review of epidemiologic evidence. Asia Pac. J. Clin. Nutr. 2006, 15, 134–142. [Google Scholar]
- Kastorini, C.-M.; Panagiotakos, D.B. Dietary Patterns and prevention of Type 2 diabetes: From research to clinical practice; a systematic review. Curr. Diabetes Rev. 2009, 5, 221–227. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; de la Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef]
- Lindström, J.; Peltonen, M.; Eriksson, J.G.; Aunola, S.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Uusitupa, M.; Tuomilehto, J. Determinants for the effectiveness of lifestyle intervention in the finnish diabetes prevention study. Diabetes Care 2008, 31, 857–862. [Google Scholar] [CrossRef]
- Kosaka, K.; Noda, M.; Kuzuya, T. Prevention of type 2 diabetes by lifestyle intervention: A Japanese trial in IGT males. Diabetes Res. Clin. Pract. 2005, 67, 152–162. [Google Scholar] [CrossRef]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.; Vijay, V. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 2009, 374, 1677–1686. [Google Scholar] [CrossRef]
- Al-Shahri, M.Z. Culturally sensitive caring for Saudi patients. J. Transcult. Nurs. 2002, 13, 133–138. [Google Scholar] [CrossRef]
- Willett, W.C.; Hu, F.B. The food frequency questionnaire. Cancer Epidemiol. Biomark. Prev. 2007, 16, 182–183. [Google Scholar] [CrossRef]
- Khani, B.R.; Ye, W.; Terry, P.; Wolk, A. Reproducibility and validity of major doetary patterns among swedish women assessed with a food-frequency questionnaire. J. Nutr. 2004, 134, 1541–1545. [Google Scholar]
- Hossain, P.; Kawar, B.; El Nahas, M. Obesity and diabetes in the developing world—A growing challenge. N. Engl. J. Med. 2007, 356, 213–215. [Google Scholar] [CrossRef]
- Willett, W.; Manson, J.; Liu, S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am. J. Clin. Nutr. 2002, 76, 274S–280S. [Google Scholar]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, lifestyle, and the risk of Type 2 diabetes mellitus in women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.W.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of Type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Mehio Sibai, A.; Nasreddine, L.; Mokdad, A.H.; Adra, N.; Tabet, M.; Hwalla, N. Nutrition transition and cardiovascular disease risk factors in Middle East and North Africa Countries: Reviewing the evidence. Ann. Nutr. Metab. 2010, 57, 193–203. [Google Scholar] [CrossRef]
- Astrup, A.; Finer, N. Redefining Type 2 diabetes: ‘Diabesity’ or ‘Obesity Dependent Diabetes Mellitus’? Obes. Rev. 2000, 1, 57–59. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Al-Khudairy, L.; Stranges, S.; Kumar, S.; Al-Daghri, N.; Rees, K. Dietary Factors and Type 2 Diabetes in the Middle East: What Is the Evidence for an Association?––A Systematic Review. Nutrients 2013, 5, 3871-3897. https://doi.org/10.3390/nu5103871
Al-Khudairy L, Stranges S, Kumar S, Al-Daghri N, Rees K. Dietary Factors and Type 2 Diabetes in the Middle East: What Is the Evidence for an Association?––A Systematic Review. Nutrients. 2013; 5(10):3871-3897. https://doi.org/10.3390/nu5103871
Chicago/Turabian StyleAl-Khudairy, Lena, Saverio Stranges, Sudhesh Kumar, Nasser Al-Daghri, and Karen Rees. 2013. "Dietary Factors and Type 2 Diabetes in the Middle East: What Is the Evidence for an Association?––A Systematic Review" Nutrients 5, no. 10: 3871-3897. https://doi.org/10.3390/nu5103871
APA StyleAl-Khudairy, L., Stranges, S., Kumar, S., Al-Daghri, N., & Rees, K. (2013). Dietary Factors and Type 2 Diabetes in the Middle East: What Is the Evidence for an Association?––A Systematic Review. Nutrients, 5(10), 3871-3897. https://doi.org/10.3390/nu5103871