Effect of the Glycemic Index of Carbohydrates on Acne vulgaris



Abstract
:
1. Introduction
2. Methods
2.1. Subjects
2.2. Study protocol
2.3. Diets
2.4. Assessment of acne severity
2.5. Blood analysis
2.6. Statistical analysis
3. Results and Discussion

{kind=link}
{kind=link}
| Low GI, n = 23 | High GI, n = 20 | P | |
|---|---|---|---|
| Mean ± SEM | Mean ± SEM | ||
| Age (y) | 16.6 ± 0.2 | 16.5 ± 0.3 | 0.92 |
| BMI (kg/m2) | 24.0 ± 1.0 a | 23.1 ± 0.6 b | 0.45 |
| Weight (kg) | 76.0 ± 3.3 | 75.4 ± 1.8 | 0.87 |
| Facial acne score/3 | 2.1 ± 0.1 | 1.9 ± 0.2 | 0.30 |
| Glucose (mmol/L) | 4.7 ± 0.1 c | 4.8 ± 0.1 | 0.54 |
| Insulin (pmol/L) | 22.7 ± 4.1 c | 22.9 ± 2.3 | 0.98 |
| HOMA-IR | 0.7 ± 0.1 c | 0.8 ± 0.1 | 0.51 |
| Testosterone (nmol/L) | 34.3 ± 1.8 c | 32.4 ± 1.6 | 0.43 |
| SHBG (nmol/L) | 23.7 ± 2.4 c | 26.4 ± 2.1 | 0.59 |
| FAI (nmol/L) | 177.7 ± 20.6 c | 142.6 ± 12.7 | 0.16 |
| DHEA-S (µmol/L) | 5.9 ± 0.6 c | 4.5 ± 0.4 | 0.04 |
| IGF-1 (nmol/L) | 56.6 ± 4.7 c | 57.8 ± 3.6 | 0.84 |
| IGFBP-1 (ng/mL) | 33.4 ± 6.0 c | 30.8 ± 3.1 | 0.71 |
| IGFBP-3 (µg/mL) | 6.2 ± 0.3 c | 6.3 ± 0.4 | 0.84 |
| Low GI, n = 20 a | High GI, n = 17 b | p | |
|---|---|---|---|
| Mean ± SEM | Mean ± SEM | ||
| E (kJ) | 8164 ± 584 | 9417 ± 571 | 0.14 |
| Protein (%E) | 21 ± 1 | 19 ± 1 | 0.06 |
| Fat (%E) | 34 ± 1 | 36 ± 1 | 0.11 |
| Monounsaturated fat (%E) | 13 ± 0 | 13 ± 0 | 0.46 |
| Polyunsaturated fat (%E) | 4 ± 0 | 4 ± 0 | 0.85 |
| Saturated fat (%E) | 13 ± 0 | 15 ± 1 | 0.01 |
| Carbohydrate (%E) | 39 ± 2 | 42 ± 2 | 0.25 |
| Fiber (g) | 16 ± 2 | 15 ± 1 | 0.5 |
| Zinc (mg) | 13 ± 1 | 14 ± 1 | 0.44 |
| Calcium (mg) | 640 ± 67 | 796 ± 83 | 0.15 |
| Glycemic index | 51 ± 1 | 61 ± 2 | 0.0002 |
| Glycemic load | 102 ± 9 | 157 ± 18 | 0.01 |
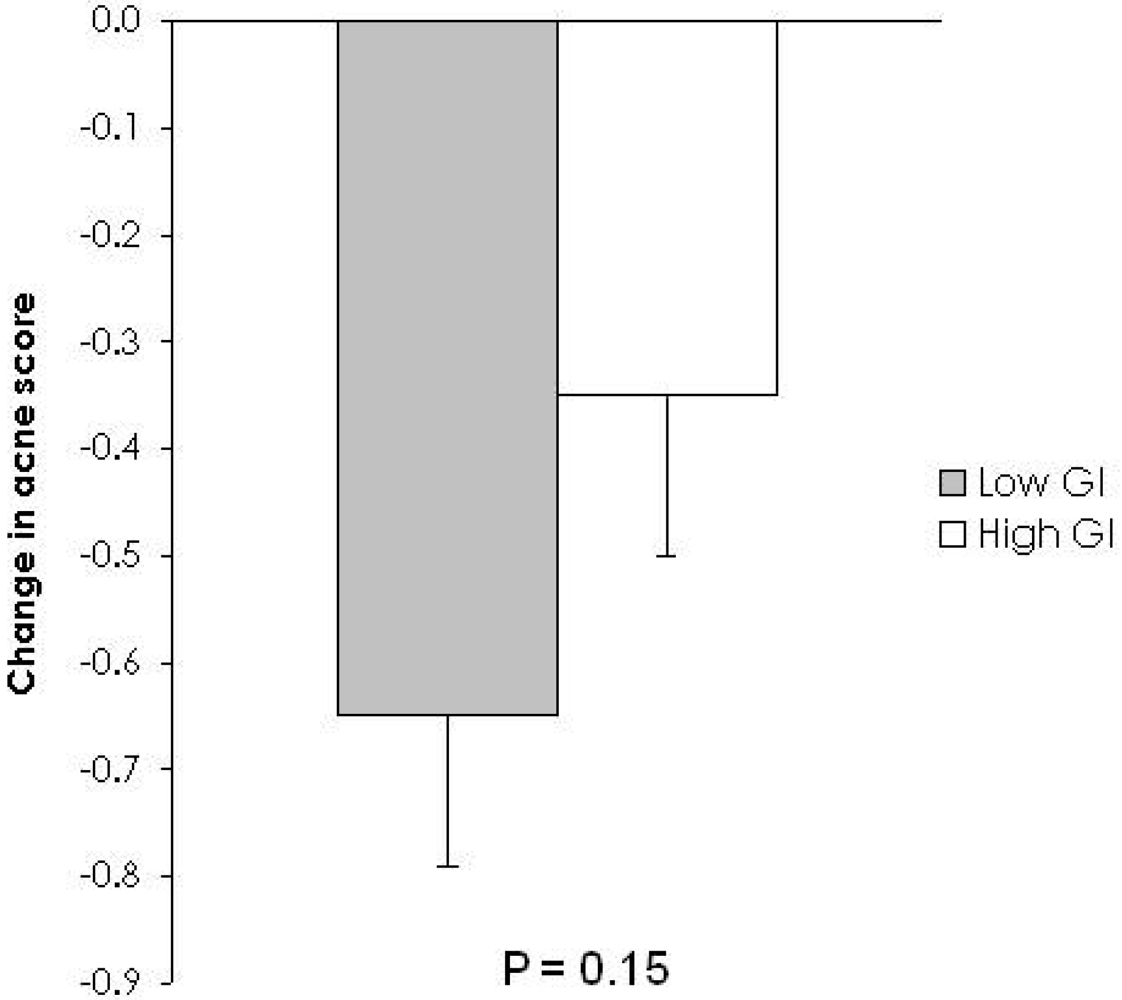
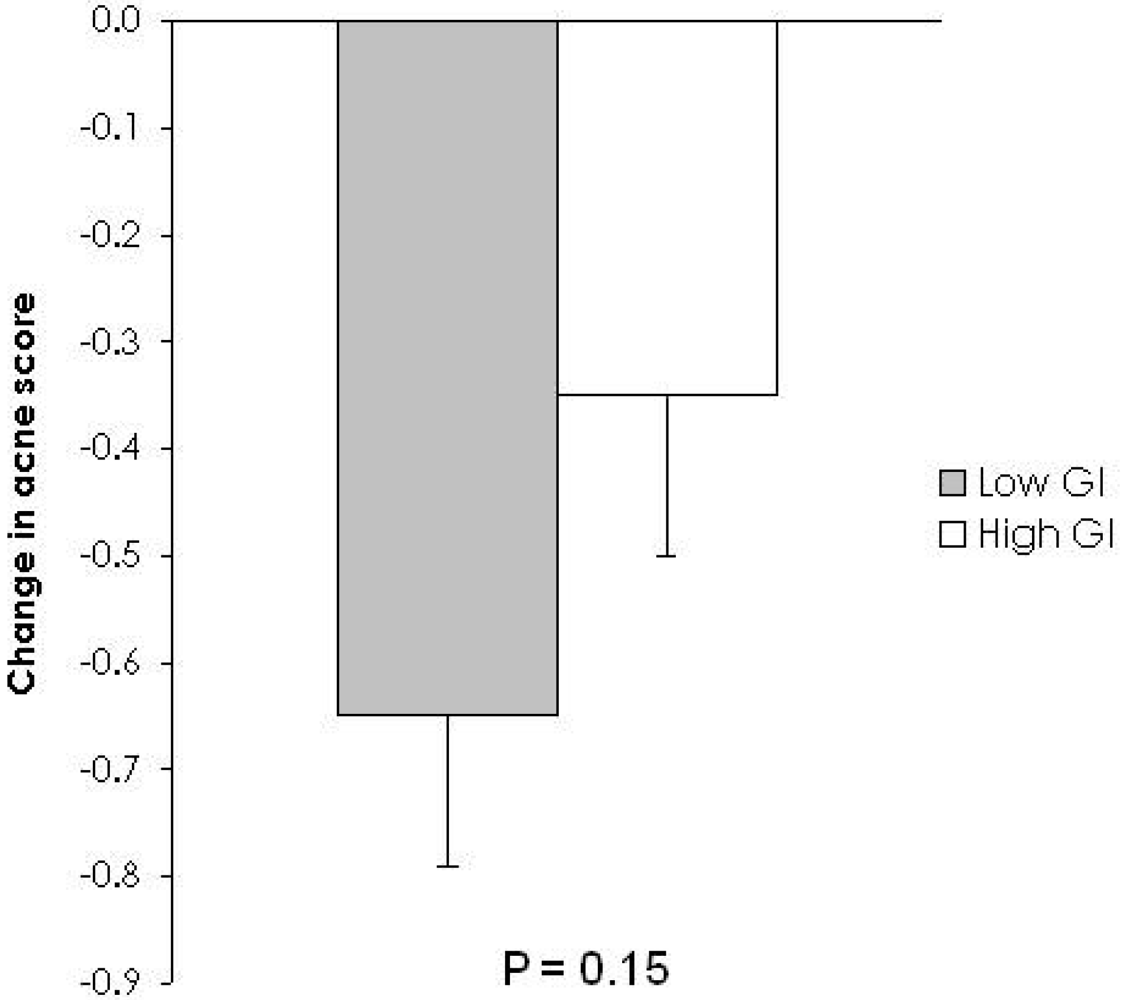
| Diet | Mean ± SEM | p 2 | Covariate and (p value) 3 | |
|---|---|---|---|---|
| Facial acne 4 | Low GI | −0.65 ± 0.14 | 0.15 | |
| High GI | −0.35 ± 0.15 | |||
| Facial acne 5 | Low GI | −0.61 ± 0.13 | 0.28 | −0.42 (0.004) |
| High GI | −0.40 ± 0.14 |
| Diet | Mean ± SEM | p 2 | p 3 | |
|---|---|---|---|---|
| Glucose (mmol/L) | Low GI | −0.1 ± 0.1 | 0.58 | 0.74 |
| High GI | −0.1 ± 0.1 | 0.32 | ||
| Insulin (pmol/L) | Low GI | 5.5 ± 3.0 | 0.09 | 0.49 |
| High GI | 2.3 ± 3.2 | 0.27 | ||
| HOMA-IR | Low GI | 0.2 ± 0.1 | 0.10 | 0.60 |
| High GI | 0.1 ± 0.1 | 0.39 | ||
| Testosterone (nmol/L) | Low GI | 3.4 ± 1.8 | 0.07 | 0.50 |
| High GI | 5.0 ± 1.7 | 0.03 | ||
| SHBG (nmol/L) | Low GI | 0.4 ± 1.2 | 0.71 | 0.75 |
| High GI | −0.1 ± 1.0 | 0.81 | ||
| FAI (nmol/L) | Low GI | 14.4 ± 10.3 | 0.17 | 0.92 |
| High GI | 11.4 ± 7.9 | 0.16 | ||
| DHEA-S (µmol/L) | Low GI | 0.2 ± 0.2 | 0.35 | 0.86 |
| High GI | 0.3 ± 0.2 | 0.17 | ||
| IGF-1 (nmol/L) | Low GI | 1.8 ± 1.9 | 0.35 | 0.10 |
| High GI | 1.9 ± 2.4 | 0.43 | ||
| IGFBP-1 (ng/mL) | Low GI | −6.2 ± 3.7 | 0.11 | 0.02 |
| High GI | 4.0 ± 2.6 | 0.14 | ||
| IGFBP-3 (µg/mL) | Low GI | −0.3 ± 0.4 | 0.46 | 0.86 |
| High GI | −0.1 ± 0.2 | 0.58 |
4. Conclusions
Conflict of Interest
Acknowledgements
References
- Cordain, L. Implications for the role of diet in acne. Semin. Cutan. Med. Surg. 2005, 24, 84–91. [Google Scholar]
- Smith, R.N.; Mann, N.J.; Braue, A.; Mäkeläinen, H.; Varigos, G.A. The effect of a high-protein, low glycemic-load diet versus a conventional, high glycemic-load diet on biochemical parameters associated with acne vulgaris: a randomized, investigator-masked, controlled trial. J. Am. Acad. Dermatol. 2007, 57, 247–256. [Google Scholar]
- Chew, I.; Brand, J.C.; Thorburn, A.W.; Truswell, A.S. Application of glycemic index to mixed meals. Am. J. Clin. Nutr. 1988, 47, 53–56. [Google Scholar]
- Bjorck, I.; Liljeberg, H.; Ostman, E. Low glycaemic-index foods. Br. J. Nutr. 2000, 83 (Suppl. 1), S149–S155. [Google Scholar]
- Cunliffe, W.; Simpson, N.B. Disorders of the Sebaceous Glands; Blackwell Scientific Publications: Oxford, England, UK, 1998. [Google Scholar]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Invest. 2006, 116, 1793–1801. [Google Scholar]
- Moran, A.; Jacobs, D.R., Jr.; Steinberger, J.; Hong, C.P.; Prineas, R.; Luepker, R.; Sinaiko, A.R. Insulin resistance during puberty: results from clamp studies in 357 children. Diabetes 1999, 48, 2039–2044. [Google Scholar]
- Preziosi, P.; Barrett-Connor, E.; Papoz, L.; Roger, M.; Saint-Paul, M.; Nahoul, K.; Simon, D. Interrelation between plasma sex hormone-binding globulin and plasma insulin in healthy adult women: the telecom study. J. Clin. Endocrinol. Metab. 1993, 76, 283–287. [Google Scholar]
- Holly, J.M.; Smith, C.P.; Dunger, D.B.; Howell, R.J.; Chard, T.; Perry, L.A.; Savage, M.O.; Cianfarani, S.; Rees, L.H.; Wass, J.A. Relationship between the pubertal fall in sex hormone binding globulin and insulin-like growth factor binding protein-I. A synchronized approach to pubertal development? Clin. Endocrinol. (Oxf.) 1989, 31, 277–284. [Google Scholar]
- Deplewski, D.; Rosenfield, R.L. Role of hormones in pilosebaceous unit development. Endocr. Rev. 2000, 21, 363–392. [Google Scholar]
- Aizawa, H.; Niimura, M. Elevated serum insulin-like growth factor-1 (IGF-1) levels in women with postadolescent acne. J. Dermatol. 1995, 22, 249–252. [Google Scholar]
- Edmondson, S.R.; Thumiger, S.P.; Werther, G.A.; Wraight, C.J. Epidermal homeostasis: the role of the growth hormone and insulin-like growth factor systems. Endocr. Rev. 2003, 24, 737–764. [Google Scholar]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar]
- Baxter, R.C.; Martin, J.L.; Wood, M.H. Two immunoreactive binding proteins for insulin-like growth factors in human amniotic fluid: relationship to fetal maturity. J. Clin. Endocrinol. Metab. 1987, 65, 423–431. [Google Scholar]
- Baxter, R.C.; Martin, J.L. Radioimmunoassay of growth hormone-dependent insulinlike growth factor binding protein in human plasma. J. Clin. Invest. 1986, 78, 1504–1512. [Google Scholar]
- Seaton, E.D.; Charakida, A.; Mouser, P.E.; Grace, I.; Clement, R.M.; Chu, A.C. Pulsed-dye laser treatment for inflammatory acne vulgaris: randomised controlled trial. Lancet 2003, 362, 1347–1352. [Google Scholar]
- McLeod, L.D.; Fehnel, S.E.; Brandman, J.; Symonds, T. Evaluating minimal clinically important differences for the acne-specific quality of life questionnaire. Pharmacoeconomics 2003, 21, 1069–1079. [Google Scholar]
- Mauras, N.; Rogol, A.D.; Haymond, M.W.; Veldhuis, J.D. Sex steroids, growth hormone, insulin-like growth factor-1: neuroendocrine and metabolic regulation in puberty. Horm. Res. 1996, 45, 74–80. [Google Scholar]
- Thiboutot, D.; Gilliland, K.; Light, J.; Lookingbill, D. Androgen metabolism in sebaceous glands from subjects with and without acne. Arch. Dermatol. 1999, 135, 1041–1045. [Google Scholar]
- Cappel, M.; Mauger, D.; Thiboutot, D. Correlation between serum levels of insulin-like growth factor 1, dehydroepiandrosterone sulfate, and dihydrotestosterone and acne lesion counts in adult women. Arch. Dermatol. 2005, 141, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Downing, D.T.; Stewart, M.E.; Wertz, P.W.; Strauss, J.S. Essential fatty acids and acne. J. Am. Acad. Dermatol. 1986, 14, 221–225. [Google Scholar]
- Katsuta, Y.; Iida, T.; Inomata, S.; Denda, M. Unsaturated fatty acids induce calcium influx into keratinocytes and cause abnormal differentiation of epidermis. J. Invest. Dermatol. 2005, 124, 1008–1013. [Google Scholar]
- Smith, K.R.; Thiboutot, D.M. Thematic review series: skin lipids. Sebaceous gland lipids: friend or foe? J. Lipid. Res. 2008, 49, 271–281. [Google Scholar] [PubMed]
- Bowen, J.; Noakes, M.; Trenerry, C.; Clifton, P.M. Energy intake, ghrelin, and cholecystokinin after different carbohydrate and protein preloads in overweight men. J. Clin. Endocrinol. Metab. 2006, 91, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.; Ryttig, K.R.; Leeds, A.R.; Bard, D.; Apfelbaum, M. Effects of a moderate dietary fibre supplement on hunger rating, energy input and faecal energy output in young, healthy volunteers. A randomized, double-blind, cross-over trial. Int. J. Obes. 1987, 11 (Suppl. 1), 73–78. [Google Scholar]
- Chandalia, M.; Garg, A.; Lutjohann, D.; von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar]
- Frid, A.H.; Nilsson, M.; Holst, J.J.; Björck, I.M. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects. Am. J. Clin. Nutr. 2005, 82, 69–75. [Google Scholar]
- Brand-Miller, J.C.; Liu, V.; Petocz, P.; Baxter, R.C. The glycemic index of foods influences postprandial insulin-like growth factor-binding protein responses in lean young subjects. Am. J. Clin. Nutr. 2005, 82, 350–354. [Google Scholar]
- Slayden, S.M.; Moran, C.; Sams, W.M., Jr.; Boots, L.R.; Azziz, R. Hyperandrogenemia in patients presenting with acne. Fertil. Steril. 2001, 75, 889–892. [Google Scholar]
- Lucky, A.W.; Biro, F.M.; Huster, G.A.; Leach, A.D.; Morrison, J.A.; Ratterman, J. Acne vulgaris in premenarchal girls. An early sign of puberty associated with rising levels of dehydroepiandrosterone. Arch. Dermatol. 1994, 130, 308–314. [Google Scholar] [PubMed]
- Berrino, F.; Bellati, C.; Secreto, G.; Camerini, E.; Pala, V.; Panico, S.; Allegro, G.; Kaaks, R. Reducing bioavailable sex hormones through a comprehensive change in diet: the diet and androgens (DIANA) randomized trial. Cancer Epidemiol. Biomarkers Prev. 2001, 10, 25–33. [Google Scholar]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes: a meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar]
- Yosipovitch, G.; Tang, M.; Dawn, A.G.; Chen, M.; Goh, C.L.; Huak, Y.; Seng, L.F. Study of psychological stress, sebum production and acne vulgaris in adolescents. Acta Derm. Venereol. 2008, 87, 135–139. [Google Scholar]
- Zouboulis, C.C.; Böhm, M. Neuroendocrine regulation of sebocytes—a pathogenetic link between stress and acne. Exp. Dermatol. 2004, 13 (Suppl. 4), 31–35. [Google Scholar]
- Cordain, L.; Lindeberg, S.; Hurtado, M.; Hill, K.; Eaton, S.B.; Brand-Miller, J. Acne vulgaris: a disease of Western civilization. Arch. Dermatol. 2001, 138, 1584–1590. [Google Scholar]
- Calder, P.C. Dietary modification of inflammation with lipids. Proc. Nutr. Soc. 2002, 61, 345–358. [Google Scholar]
- Li, Y.; Seifert, M.F.; Ney, D.M.; Grahn, M.; Grant, A.L.; Allen, K.G.; Watkins, B.A. Dietary conjugated linoleic acids alter serum IGF-I and IGF binding protein concentrations and reduce bone formation in rats fed (n-6) or (n-3) fatty acids. J. Bone Miner. Res. 1999, 14, 1153–1162. [Google Scholar]
- Bhathena, S.J.; Berlin, E.; Judd, J.T.; Kim, Y.C.; Law, J.S.; Bhagavan, H.N.; Ballard-Barbash, R.; Nair, P.P. Effects of omega 3 fatty acids and vitamin E on hormones involved in carbohydrate and lipid metabolism in men. Am. J. Clin. Nutr. 1991, 54, 684–688. [Google Scholar]
- Reichrath, J. Vitamin D and the skin: an ancient friend, revisited. Exp. Dermatol. 2007, 16, 618–625. [Google Scholar]
- Adebamowo, C.A.; Spiegelman, D.; Danby, F.W.; Frazier, A.L.; Willett, W.C.; Holmes, M.D. High school dietary dairy intake and teenage acne. J. Am. Acad. Dermatol. 2005, 52, 207–214. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Reynolds, R.C.; Lee, S.; Choi, J.Y.J.; Atkinson, F.S.; Stockmann, K.S.; Petocz, P.; Brand-Miller, J.C. Effect of the Glycemic Index of Carbohydrates on Acne vulgaris. Nutrients 2010, 2, 1060-1072. https://doi.org/10.3390/nu2101060
Reynolds RC, Lee S, Choi JYJ, Atkinson FS, Stockmann KS, Petocz P, Brand-Miller JC. Effect of the Glycemic Index of Carbohydrates on Acne vulgaris. Nutrients. 2010; 2(10):1060-1072. https://doi.org/10.3390/nu2101060
Chicago/Turabian StyleReynolds, Rebecca C., Stephen Lee, James Y. J. Choi, Fiona S. Atkinson, Karola S. Stockmann, Peter Petocz, and Jennie C. Brand-Miller. 2010. "Effect of the Glycemic Index of Carbohydrates on Acne vulgaris" Nutrients 2, no. 10: 1060-1072. https://doi.org/10.3390/nu2101060
APA StyleReynolds, R. C., Lee, S., Choi, J. Y. J., Atkinson, F. S., Stockmann, K. S., Petocz, P., & Brand-Miller, J. C. (2010). Effect of the Glycemic Index of Carbohydrates on Acne vulgaris. Nutrients, 2(10), 1060-1072. https://doi.org/10.3390/nu2101060