Impact of a Dietary Supplementation with French Maritime Pine Bark Extract Pycnogenol® on Salivary and Serum Inflammatory Biomarkers During Non-Surgical Periodontal Therapy—A Randomized Placebo-Controlled Double-Blind Trial

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Intervention and Monitoring
2.3. Selection Criteria: Inclusion/Exclusion Criteria
2.4. Biomarkers and Salivary Polyphenol Levels
2.5. Statistical Analysis
3. Results
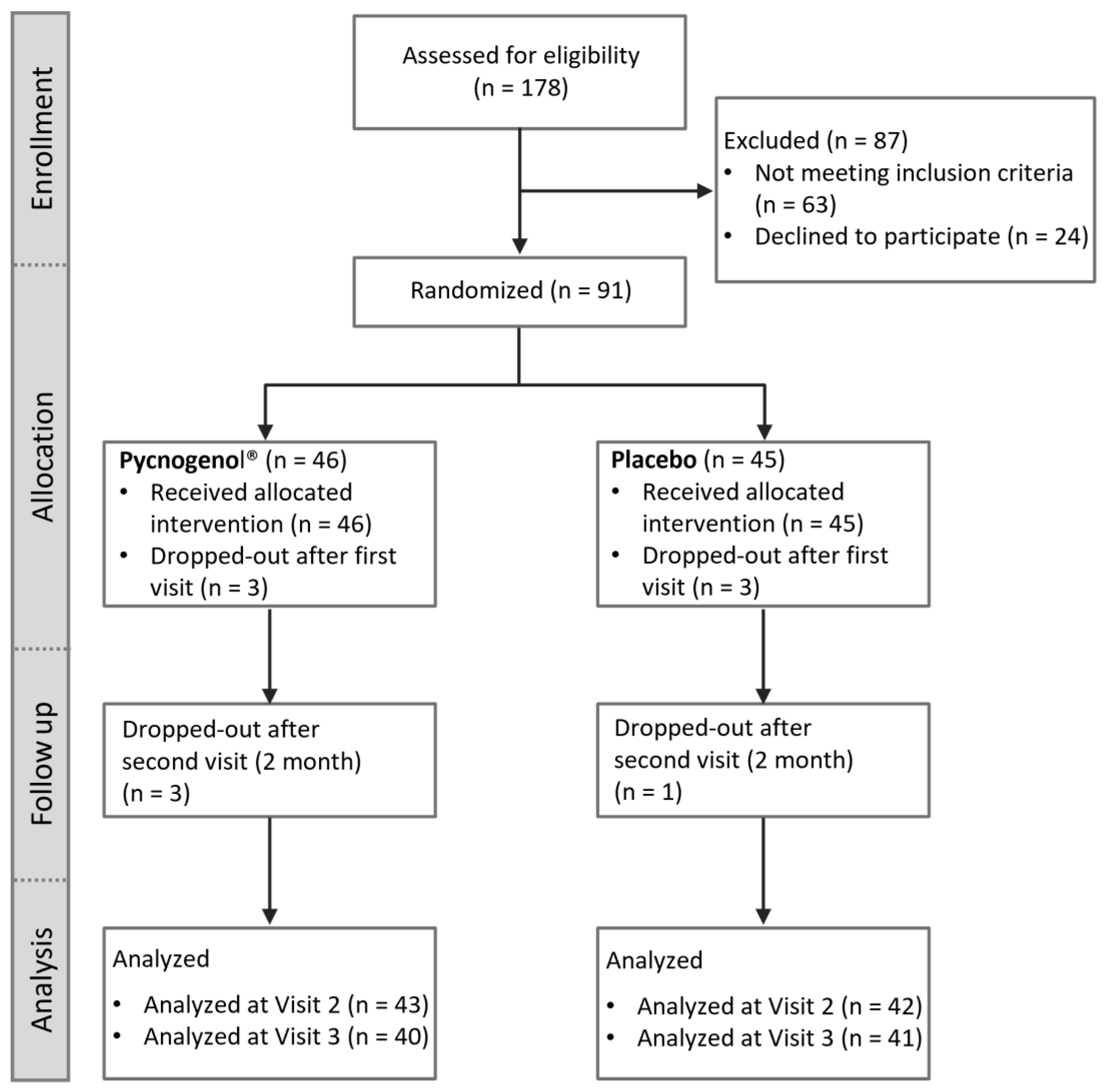
3.1. Participant Flow and Baseline Characteristics
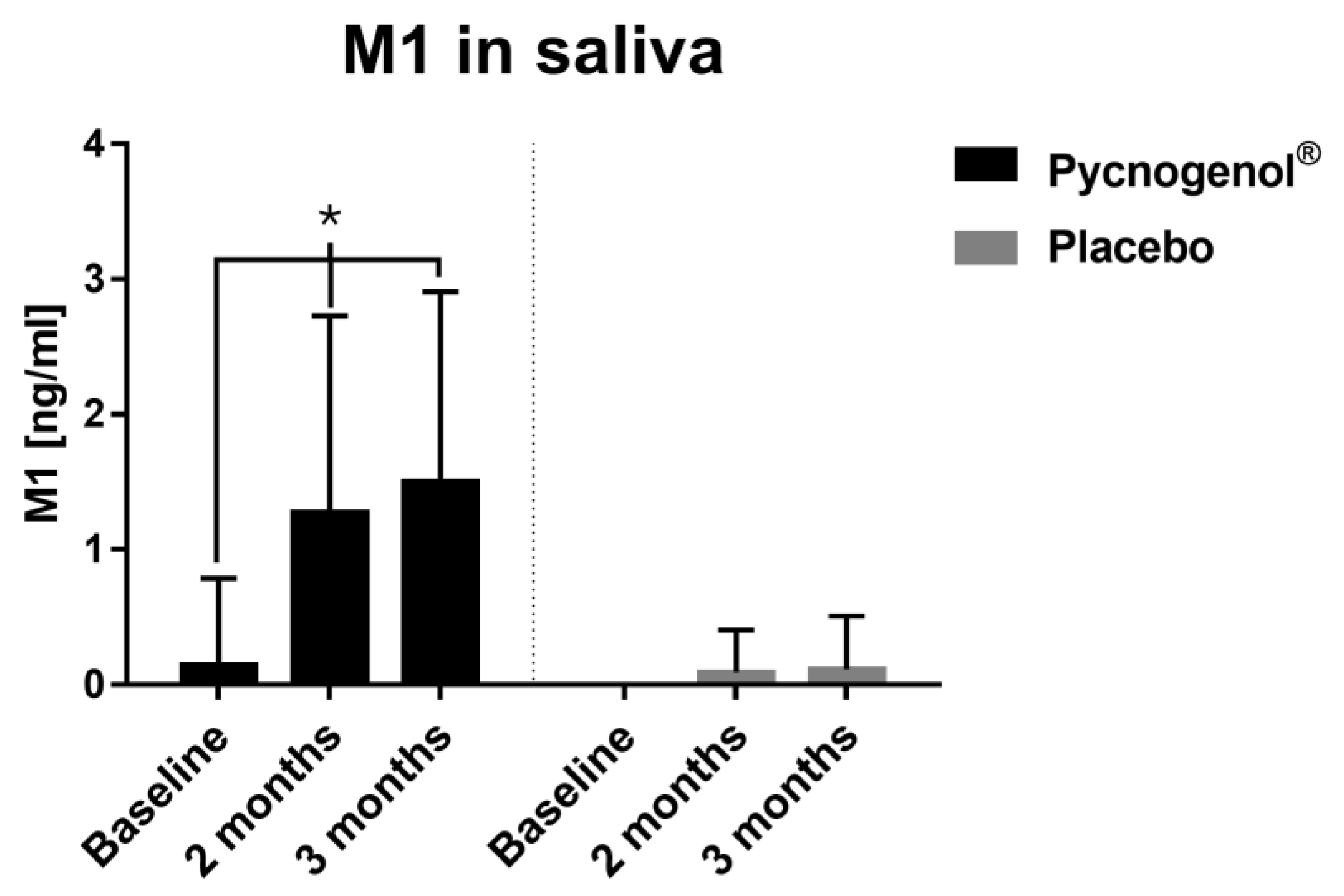
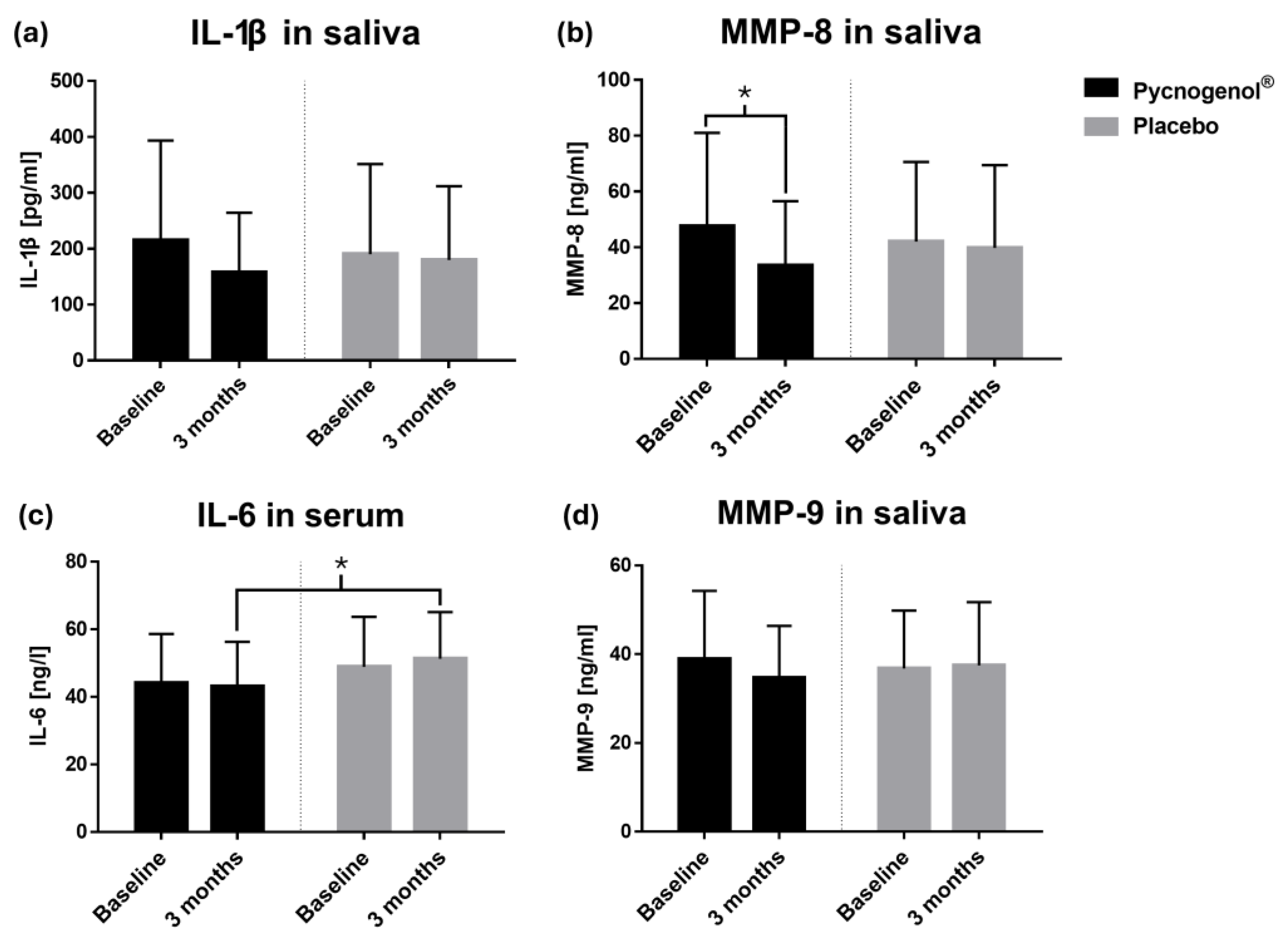
3.2. Biomarkers and Salivary Polyphenol Levels
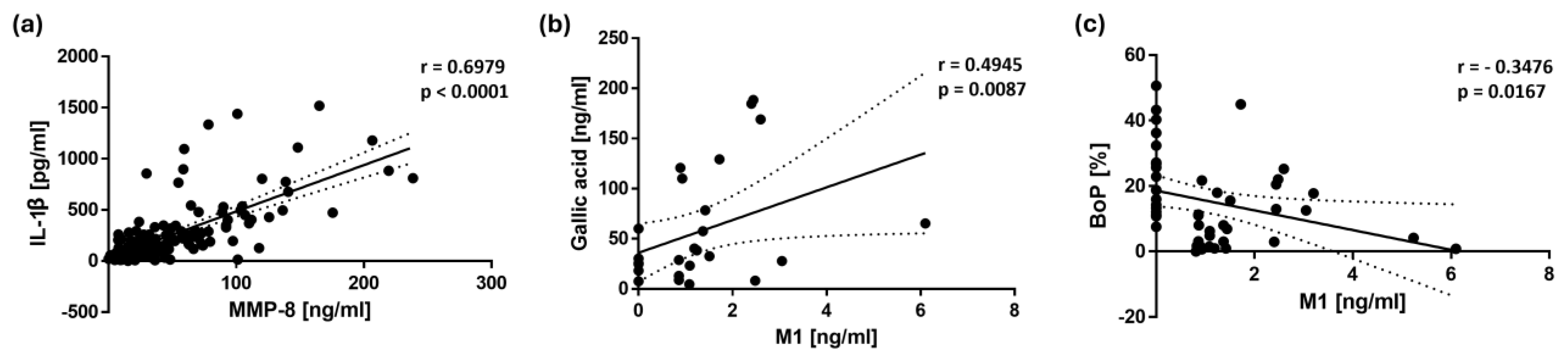
3.3. Correlation Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arango Duque, G.; Descoteaux, A. Macrophage Cytokines: Involvement in Immunity and Infectious Diseases. Front. Immunol. 2014, 5, 491. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Wang, P.; Gao, W. Microbial Dysbiosis in Periodontitis and Peri-Implantitis: Pathogenesis, Immune Responses, and Therapeutic. Front. Cell. Infect. Microbiol. 2025, 15, 1517154. [Google Scholar] [CrossRef]
- Amato, M.; Polizzi, A.; Viglianisi, G.; Leonforte, F.; Mascitti, M.; Isola, G. Impact of Periodontitis and Oral Dysbiosis Metabolites in the Modulation of Accelerating Ageing and Human Senescence. Metabolites 2025, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.; Lamster, I.B. Analysis of saliva for periodontal diagnosis—A review. J. Clin. Periodontol. 2000, 27, 453–465. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.R.; Sakellari, D. Active MMP-8 (aMMP-8) as a Grading and Staging Biomarker in the Periodontitis Classification. Diagnostics 2020, 10, 61. [Google Scholar] [CrossRef]
- Zhang, L.; Li, X.; Yan, H.; Huang, L. Salivary Matrix Metalloproteinase (MMP)-8 as a Biomarker for Periodontitis: A PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine 2018, 97, e9642. [Google Scholar] [CrossRef]
- West, N.X.; Davies, M.; Sculean, A.; Jepsen, S.; Faria-Almeida, R.; Harding, M.; Graziani, F.; Newcombe, R.G.; Creeth, J.E.; Herrera, D. Prevalence of Dentine Hypersensitivity, Erosive Tooth Wear, Gingival Recession and Periodontal Health in Seven European Countries. J. Dent. 2024, 150, 105364. [Google Scholar] [CrossRef]
- Blais, L.; Auclair-Ouellet, N.; Tremblay, A.; Binda, S. Effect of the Darolac® (Oralis SB®) Probiotic Formulation on Oral Health: A Narrative Review. Microorganisms 2025, 13, 408. [Google Scholar] [CrossRef]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative Stress and Antioxidant System in Periodontitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef]
- Muniz, F.W.; Nogueira, S.B.; Mendes, F.L.; Rösing, C.K.; Moreira, M.M.; de Andrade, G.M.; Carvalho Rde, S. The Impact of Antioxidant Agents Complimentary to Periodontal Therapy on Oxidative Stress and Periodontal Outcomes: A systematic review. Arch. Oral Biol. 2015, 60, 1203–1214. [Google Scholar] [CrossRef]
- Chapple, I.L.; Milward, M.R.; Ling-Mountford, N.; Weston, P.; Carter, K.; Askey, K.; Dallal, G.E.; De Spirt, S.; Sies, H.; Patel, D.; et al. Adjunctive Daily Supplementation with Encapsulated Fruit, Vegetable and Berry Juice Powder Concentrates and Clinical Periodontal Outcomes: A Double-Blind RCT. J. Clin. Periodontol. 2012, 39, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Bunte, K.; Hensel, A.; Beikler, T. Polyphenols in the Prevention and Treatment of Periodontal Disease: A Systematic Review of In Vivo, Ex Vivo and In Vitro Studies. Fitoterapia 2019, 132, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Zhang, D.; Wu, J.; Liu, J.; Zhou, Y.; Tan, Y.; Feng, W.; Peng, C. Interactions Between Gut Microbiota and Polyphenols: A Mechanistic and Metabolomic Review. Phytomedicine 2023, 119, 154979. [Google Scholar] [CrossRef]
- Hashim, N.T.; Babiker, R.; Chaitanya, N.; Mohammed, R.; Priya, S.P.; Padmanabhan, V.; Ahmed, A.; Dasnadi, S.P.; Islam, M.S.; Gismalla, B.G.; et al. New Insights in Natural Bioactive Compounds for Periodontal Disease: Advanced Molecular Mechanisms and Therapeutic Potential. Molecules 2025, 30, 807. [Google Scholar] [CrossRef]
- Sugimoto, H.; Watanabe, K.; Toyama, T.; Takahashi, S.S.; Sugiyama, S.; Lee, M.C.; Hamada, N. Inhibitory Effects of French Pine Bark Extract, Pycnogenol®, on Alveolar Bone Resorption and on the Osteoclast Differentiation. Phytother. Res. 2015, 29, 251–259. [Google Scholar] [CrossRef]
- Weichmann, F.; Rohdewald, P. Pycnogenol® French Maritime Pine Bark Extract in Randomized, Double-Blind, Placebo-Controlled Human Clinical Studies. Front. Nutr. 2024, 11, 1389374. [Google Scholar] [CrossRef] [PubMed]
- Bayer, J.; Högger, P. Review of the Pharmacokinetics of French Maritime Pine Bark Extract (Pycnogenol®) in Humans. Front. Nutr. 2024, 11, 1389422. [Google Scholar] [CrossRef]
- Bayer, J.; Högger, P. Development and Validation of a LC-MS/MS Method for the Quantification of Phenolic Compounds in Human Saliva After Intake of a Procyanidin-Rich Pine Bark Extract. J. Pharm. Biomed. Anal. 2024, 239, 115914. [Google Scholar] [CrossRef] [PubMed]
- Grimm, T.; Schäfer, A.; Högger, P. Antioxidant Activity and Inhibition of Matrix Metalloproteinases by Metabolites of Maritime Pine Bark Extract (Pycnogenol). Free Radic. Biol. Med. 2004, 36, 811–822. [Google Scholar] [CrossRef]
- Jockel-Schneider, Y.; Schlagenhauf, U.; Stölzel, P.; Goßner, S.; Carle, R.; Ehmke, B.; Prior, K.; Hagenfeld, D. Nitrate-Rich Diet Alters the Composition of the Oral Microbiota in Periodontal Recall Patients. J. Periodontol. 2021, 92, 1536–1545. [Google Scholar] [CrossRef]
- Jockel-Schneider, Y.; Stoelzel, P.; Hess, J.; Haubitz, I.; Fickl, S.; Schlagenhauf, U. Impact of a Specific Collagen Peptide Food Supplement on Periodontal Inflammation in Aftercare Patients-A Randomised Controlled Trial. Nutrients 2022, 14, 4473. [Google Scholar] [CrossRef] [PubMed]
- Flemming, J.; Meyer-Probst, C.T.; Speer, K.; Kölling-Speer, I.; Hannig, C.; Hannig, M. Preventive Applications of Polyphenols in Dentistry-A Review. Int. J. Mol. Sci. 2021, 22, 4892. [Google Scholar] [CrossRef]
- Slobodníková, L.; Fialová, S.; Rendeková, K.; Kováč, J.; Mučaji, P. Antibiofilm Activity of Plant Polyphenols. Molecules 2016, 21, 1717. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.; Tay, J.R.H.; Boey, S.K.; Laine, M.L.; Ivanovski, S.; Seneviratne, C.J. Antibiotic Resistance in the Microbiota of Periodontitis Patients: An Update of Current Findings. Crit. Rev. Microbiol. 2024, 50, 329–340. [Google Scholar] [CrossRef]
- Solomon, S.M.; Matei, M.N.; Badescu, A.C.; Jelihovschi, I.; Martu-Stefanache, A.; Teusan, A.; Martu, S.; Iancu, L.S. Evaluation of DNA Extraction Methods from Saliva as a Source of PCR—Amplifiable Genomic DNA. Rev. Chim. 2015, 66, 2101–2103. [Google Scholar]
- Kimbrough, C.; Chun, M.; dela Roca, G.; Lau, B.H. Pycnogenol® Chewing Gum Minimizes Gingival Bleeding and Plaque Formation. Phytomedicine 2002, 9, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Sufaru, I.G.; Macovei, G.; Stoleriu, S.; Martu, M.A.; Luchian, I.; Kappenberg-Nitescu, D.C.; Solomon, S.M. 3D Printed and Bioprinted Membranes and Scaffolds for the Periodontal Tissue Regeneration: A Narrative Review. Membranes 2022, 12, 902. [Google Scholar] [CrossRef]
- Zalewska, E.A.; Ławicka, R.; Grygorczuk, P.; Nowosielska, M.; Kicman, A.; Ławicki, S. Importance of Metalloproteinase 8 (MMP-8) in the Diagnosis of Periodontitis. Int. J. Mol. Sci. 2024, 25, 2721. [Google Scholar] [CrossRef]
- Balaji, S.; Cholan, P.K.; Victor, D.J. Evaluation of “Soluble Triggering Receptor Expressed on Myeloid Cells-1 (sTREM-1), Interleukin-1β, and Matrix Metalloproteinase-8” as a Short Panel of Salivary Biomarkers in Patients with and Without Stage III/IV Periodontitis and Type 2 Diabetes Mellitus. J. Oral Biol. Craniofac. Res. 2022, 12, 33–37. [Google Scholar] [CrossRef]
- Laky, M.; Arslan, M.; Zhu, X.; Rausch-Fan, X.; Moritz, A.; Sculean, A.; Laky, B.; Ramseier, C.A.; Stähli, A.; Eick, S. Quercetin in the Prevention of Induced Periodontal Disease in Animal Models: A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 735. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pycnogenol® Group (n = 46) | Placebo Group (n = 45) | p-Value 1 |
|---|---|---|---|
| Age (years), mean ± SD | 67.83 ± 9.18 | 66.96 ± 8.20 | 0.6348 (T) |
| Gender, n (%) | |||
| Male | 27 (58.7) | 12 (26.7) | 0.0029 * (F) |
| Female | 19 (41.3) | 33 (73.3) | |
| Vegetarian diet, n (%) | |||
| Yes | 6 (13.0) | 2 (4.4) | 0.2668 (F) |
| No | 40 (87.0) | 43 (95.6) | |
| Smoking status, n (%) | |||
| Yes | 5 (10.9) | 2 (4.4) | 0.4345 (F) |
| No | 41 (89.1) | 43 (95.6) | |
| Drinking status 2, n (%) | |||
| Yes | 22 (47.8) | 15 (33.3) | 0.2018 (F) |
| No | 24 (52.2) | 30 (66.7) |
| Analyte | Measurement Time | Pycnogenol® | Placebo | p-Value b | p-Value c | p-Value d | ||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | n 1 | Mean ± SD | n 1 | |||||
| Taxifolin [ng/mL] | Baseline (Visit 1) | 3.46 ± 2.14 | 5 | 0.00 | 0 | 0.0357 * | 0.0257 * | |
| 2 months (Visit 2) | 5.57 ± 6.12 | 8 | 4.47 ± 2.07 | 4 | 0.5697 | 0.2258 | ||
| p-Value a | 0.3750 | 0.1250 | ||||||
| 3 months (Visit 3) | 3.29 ± 2.46 | 5 | 2.89 ± 1.39 | 5 | 0.8413 | 0.1229 | 1.000 | |
| p-Value a | 0.7695 | 0.0625 | ||||||
| Ferulic acid [ng/mL] | Baseline (Visit 1) | 10.28 ± 6.76 | 11 | 6.38 ± 2.85 | 9 | 0.3410 | 0.6135 | |
| 2 months (Visit 2) | 18.47 ± 36.97 | 17 | 7.89 ± 7.53 | 7 | 0.9014 | 0.0155 * | ||
| p-Value a | 0.2774 | 0.4131 | ||||||
| 3 months (Visit 3) | 12.87 ± 16.23 | 17 | 7.56 ± 4.24 | 5 | 0.8912 | 0.5775 | 0.0027 * | |
| p-Value a | 0.2935 | 0.4697 | ||||||
| Caffeic acid [ng/mL] | Baseline (Visit 1) | 17.70 ± 21.49 | 19 | 22.90 ± 26.34 | 9 | 0.9912 | 0.0201 * | |
| 2 months (Visit 2) | 28.12 ± 28.84 | 28 | 11.30 ± 15.34 | 22 | 0.0077 * | 0.1714 | ||
| p-Value a | 0.0002 * | 0.2726 | ||||||
| 3 months (Visit 3) | 27.71 ± 30.99 | 21 | 16.38 ± 17.83 | 17 | 0.9364 | 0.0388 * | 0.3766 | |
| p-Value a | 0.1908 | 0.3209 | ||||||
| Gallic acid [ng/mL] | Baseline (Visit 1) | 45.59 ± 50.04 | 9 | 89.82 ± 66.88 | 3 | 0.4818 | 0.0667 | |
| 2 months (Visit 2) | 82.27 ± 84.34 | 15 | 68.69 ± 88.27 | 11 | 0.3051 | 0.3474 | ||
| p-Value a | 0.0046 * | 0.0020 * | ||||||
| 3 months (Visit 3) | 45.32 ± 52.92 | 14 | 63.92 ± 66.28 | 8 | 0.2973 | 0.0102 * | 0.1394 | |
| p-Value a | 0.4037 | 0.1641 | ||||||
| p-Coumaric acid [ng/mL] | Baseline (Visit 1) | 3.99 ± 2.92 | 22 | 5.09 ± 6.59 | 22 | 0.4678 | 1.000 | |
| 2 months (Visit 2) | 6.71 ± 8.75 | 25 | 4.26 ± 3.27 | 28 | 0.9472 | 0.6445 | ||
| p-Value a | 0.3369 | 0.3058 | ||||||
| 3 months (Visit 3) | 7.93 ± 15.43 | 29 | 4.41 ± 4.42 | 25 | 0.8063 | 0.2630 | 0.3774 | |
| p-Value a | 0.1827 | 0.9911 | ||||||
| Protocatechuic acid [ng/mL] | Baseline (Visit 1) | 24.17 ± 16.74 | 17 | 22.84 ± 26.36 | 22 | 0.4617 | 0.3766 | |
| 2 months (Visit 2) | 48.01 ± 87.84 | 20 | 31.19 ± 36.18 | 24 | 0.5360 | 0.5067 | ||
| p-Value a | 0.3596 | 0.2746 | ||||||
| 3 months (Visit 3) | 35.47 ± 36.43 | 18 | 29.43 ± 29.43 | 22 | 0.4228 | 0.0954 | 0.5077 | |
| p-Value a | 0.2292 | 0.9019 | ||||||
| M1 [ng/mL] | Baseline (Visit 1) | 2.60 | 1 | 0.00 | 0 | - | 0.4938 | |
| 2 months (Visit 2) | 1.67 ± 1.45 | 13 | 1.09 | 1 | 0.0929 | 0.0003 * | ||
| p-Value a | 0.0005 * | - | ||||||
| 3 months (Visit 3) | 1.96 ± 1.28 | 13 | 1.37 | 1 | 0.0643 | 0.0252 * | 0.0003 * | |
| p-Value a | 0.0024 * | - | ||||||
| IL-1β [pg/mL] | Baseline (Visit 1) | 214.69 ± 178.80 | 35 | 190.11 ± 161.39 | 38 | 0.4897 | - | |
| 3 months (Visit 3) | 157.22 ± 107.14 | 35 | 179.88 ± 132.07 | 38 | 0.6072 | 0.1145 | - | |
| p-Value a | 0.1347 | 0.6379 | ||||||
| MMP-8 [ng/mL] | Baseline (Visit 1) | 47.65 ± 33.39 | 37 | 42.06 ± 28.58 | 37 | 0.5790 | - | |
| 3 months (Visit 3) | 33.43 ± 23.15 | 37 | 39.78 ± 29.69 | 37 | 0.5209 | 0.0414 * | - | |
| p-Value a | 0.0261 * | 0.6916 | ||||||
| MMP-9 [ng/mL] | Baseline (Visit 1) | 38.91 ± 15.37 | 37 | 36.75 ± 13.09 | 38 | 0.4435 | - | |
| 3 months (Visit 3) | 34.67 ± 11.69 | 37 | 37.48 ± 14.23 | 38 | 0.8187 | 0.1215 | - | |
| p-Value a | 0.1633 | 0.8075 | ||||||
| IL-6 2 [ng/mL] | Baseline (Visit 1) | 44.20 ± 14.43 | 38 | 48.88 ± 14.83 | 40 | 0.1793 | - | |
| 3 months (Visit 3) | 43.16 ± 13.17 | 38 | 51.27 ± 13.84 | 40 | 0.0409 * | 0.2561 | - | |
| p-Value a | 0.5326 | 0.3193 | ||||||
| Variable 1 | Variable 2 | n 1 | Spearman’s r | p-Value * |
|---|---|---|---|---|
| BoP | MMP-8 | 148 | 0.1906 | 0.0203 |
| BoP | IL-1β | 146 | 0.2380 | 0.0038 |
| MMP-8 | IL-1β | 144 | 0.6979 | <0.0001 |
| M1 | Gallic acid | 27 | 0.4945 | 0.0087 |
| M1 | BoP | 47 | −0.3476 | 0.0167 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayer, J.; Petersen, N.K.; Hess, J.V.; Jockel-Schneider, Y.; Högger, P. Impact of a Dietary Supplementation with French Maritime Pine Bark Extract Pycnogenol® on Salivary and Serum Inflammatory Biomarkers During Non-Surgical Periodontal Therapy—A Randomized Placebo-Controlled Double-Blind Trial. Nutrients 2025, 17, 1546. https://doi.org/10.3390/nu17091546
Bayer J, Petersen NK, Hess JV, Jockel-Schneider Y, Högger P. Impact of a Dietary Supplementation with French Maritime Pine Bark Extract Pycnogenol® on Salivary and Serum Inflammatory Biomarkers During Non-Surgical Periodontal Therapy—A Randomized Placebo-Controlled Double-Blind Trial. Nutrients. 2025; 17(9):1546. https://doi.org/10.3390/nu17091546
Chicago/Turabian StyleBayer, Jasmin, Nicole Karoline Petersen, Jeanine Veruschka Hess, Yvonne Jockel-Schneider, and Petra Högger. 2025. "Impact of a Dietary Supplementation with French Maritime Pine Bark Extract Pycnogenol® on Salivary and Serum Inflammatory Biomarkers During Non-Surgical Periodontal Therapy—A Randomized Placebo-Controlled Double-Blind Trial" Nutrients 17, no. 9: 1546. https://doi.org/10.3390/nu17091546
APA StyleBayer, J., Petersen, N. K., Hess, J. V., Jockel-Schneider, Y., & Högger, P. (2025). Impact of a Dietary Supplementation with French Maritime Pine Bark Extract Pycnogenol® on Salivary and Serum Inflammatory Biomarkers During Non-Surgical Periodontal Therapy—A Randomized Placebo-Controlled Double-Blind Trial. Nutrients, 17(9), 1546. https://doi.org/10.3390/nu17091546