
Impact of Gut Microbiome Modulation on Uremic Toxin Reduction in Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis


 ,
,  , , and
, , and
Abstract
1. Introduction
1.1. Probiotics, Prebiotics, and Synbiotics
1.2. Uremic Toxins, CKD, and the Risk of Cardiovascular Disease
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
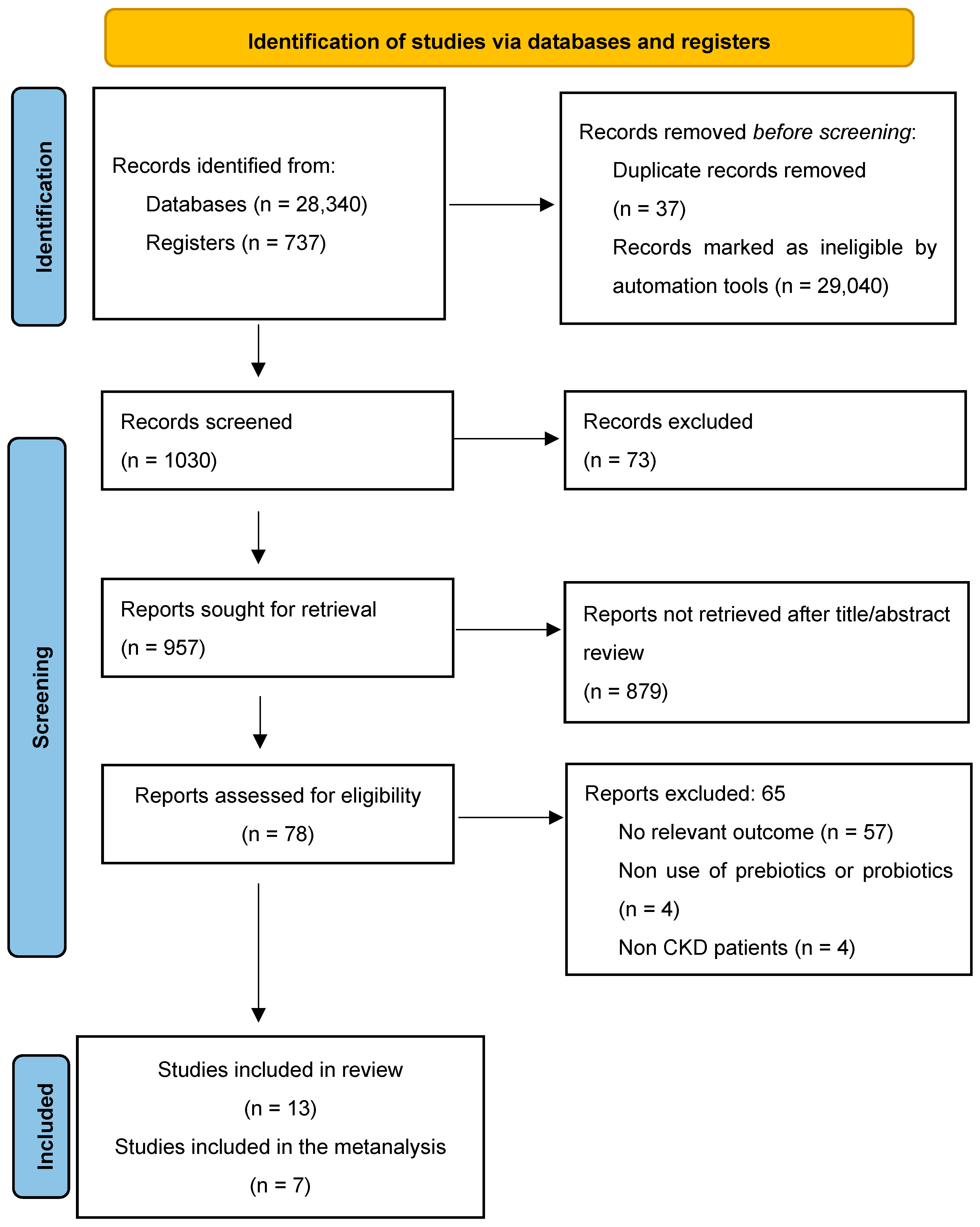
2.5. Selection Process
2.6. Assessment of Methodological Quality and Risk of Bias
2.7. Statistical Analyses
2.8. Synthesis Methods
3. Results
3.1. Data Availability and Study Characteristics
3.2. Risk of Bias in Studies
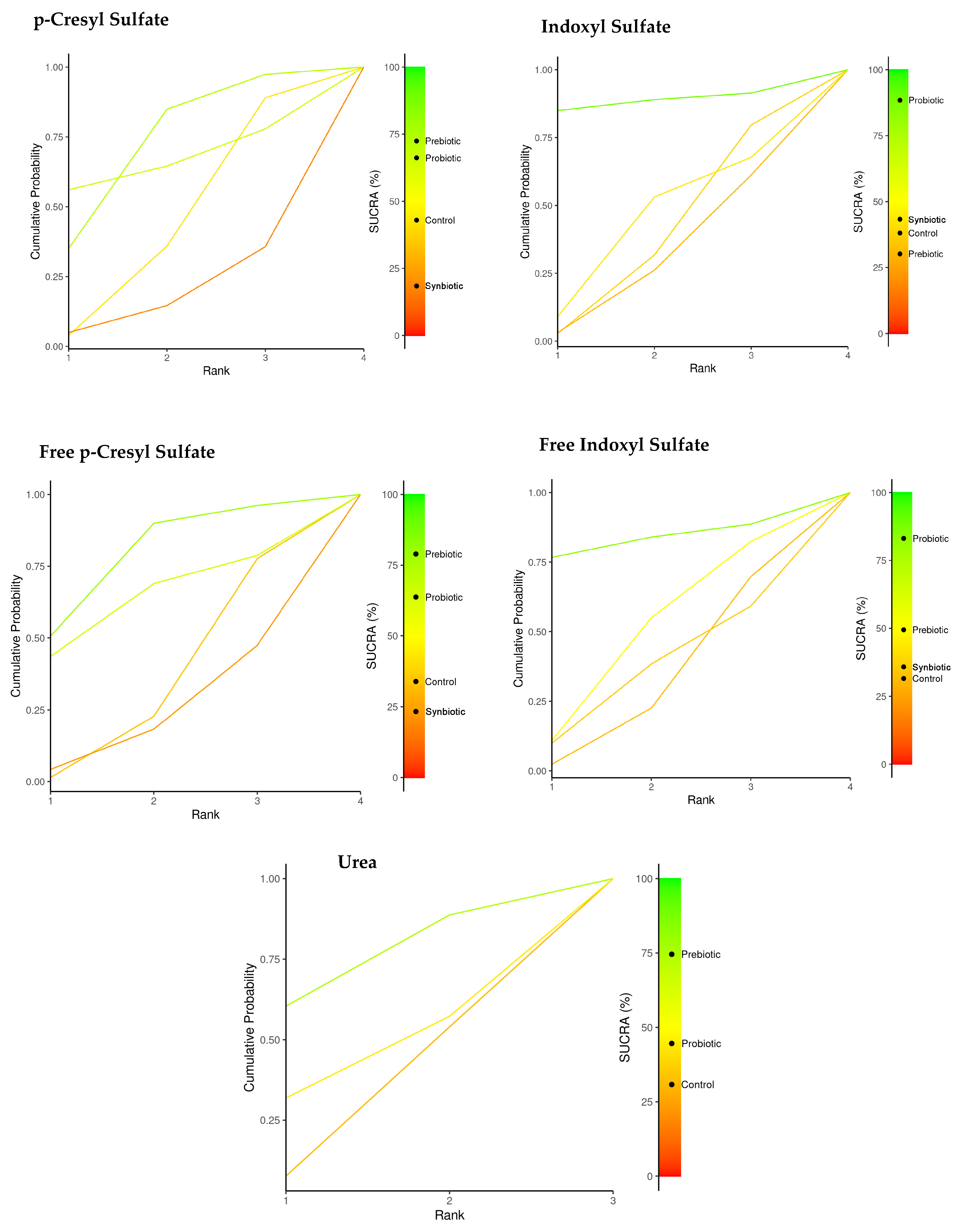
3.3. Network Meta-Analysis (Immunonutrition and Uremic Toxins)
3.4. Individual Immunonutrition and Reduction of Uremic Toxins
4. Discussion
4.1. Implications for Clinical Practice
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar]
- Guldris, S.C.; Parra, E.G.; Amenós, A.C. Microbiota intestinal en la enfermedad renal crónica. Nefrologia 2017, 37, 9–19. [Google Scholar] [CrossRef]
- Khiabani, S.A.; Asgharzadeh, M.; Kafil, H.S. Chronic kidney disease and gut microbiota. Heliyon 2023, 9, e18991. [Google Scholar] [CrossRef]
- Tsuji, K.; Uchida, N.; Nakanoh, H.; Fukushima, K.; Haraguchi, S.; Kitamura, S.; Wada, J. The Gut–Kidney Axis in Chronic Kidney Diseases. Diagnostics 2025, 15, 21. [Google Scholar]
- Beker, B.M.; Colombo, I.; Gonzalez-Torres, H.; Musso, C.G. Decreasing microbiota-derived uremic toxins to improve CKD outcomes. Clin. Kidney J. 2022, 15, 2214–2219. [Google Scholar] [CrossRef]
- Kotanko, P.; Carter, M.; Levin, N.W. Intestinal bacterial microflora—A potential source of chronic inflammation in patients with chronic kidney disease. Nephrol. Dial. Transplant. 2006, 21, 2057–2060. Available online: https://academic.oup.com/ndt/article/21/8/2057/1820863 (accessed on 30 March 2023).
- Pivari, F.; Mingione, A.; Piazzini, G.; Ceccarani, C.; Ottaviano, E.; Brasacchio, C.; Cas, M.D.; Vischi, M.; Cozzolino, M.G.; Fogagnolo, P.; et al. Curcumin Supplementation (Meriva®) Modulates Inflammation, Lipid Peroxidation and Gut Microbiota Composition in Chronic Kidney Disease. Nutrients 2022, 14, 231. [Google Scholar] [CrossRef]
- Filipska, I.; Winiarska, A.; Knysak, M.; Stompór, T. Contribution of Gut Microbiota-Derived Uremic Toxins to the Cardiovascular System Mineralization. Toxins 2021, 13, 274. [Google Scholar] [CrossRef]
- Poesen, R.; Evenepoel, P.; de Loor, H.; Delcour, J.A.; Courtin, C.M.; Kuypers, D.; Augustijns, P.; Verbeke, K.; Meijers, B. The influence of prebiotic arabinoxylan oligosaccharides on microbiota derived uremic retention solutes in patients with chronic kidney disease: A randomized controlled trial. PLoS ONE 2016, 11, e0153893. [Google Scholar] [CrossRef]
- Pandey, K.R.; Naik, S.R.; Vakil, B.V. Probiotics, prebiotics and synbiotics—A review. J. Food Sci. Technol. 2015, 52, 7577. Available online: https://pubmed.ncbi.nlm.nih.gov/26604335/ (accessed on 2 April 2023).
- Chaudhari, A.; Dwivedi, M.K. The concept of probiotics, prebiotics, postbiotics, synbiotics, nutribiotics, and pharmabiotics. In Probiotics in the Prevention and Management of Human Diseases; Academic Press: Cambridge, MA, USA, 2022; pp. 1–11. [Google Scholar]
- Wang, J.; Cassone, M.; Gibson, K.; Lansing, B.; Mody, L.; Snitkin, E.S.; Rao, K. Gut Microbiota Features on Nursing Home Admission Are Associated With Subsequent Acquisition of Antibiotic-resistant Organism Colonization. Clin. Infect. Dis. 2020, 71, 3244–3247. [Google Scholar] [CrossRef] [PubMed]
- González Cordero, E.M.; Cuevas-Budhart, M.A.; Pérez Morán, D.; Trejo Villeda, M.A.; Gomez-del-Pulgar Ga-Madrid, M. Relationship Between the Gut Microbiota and Alzheimer’s Disease: A Systematic Review. J. Alzheimer’s Dis. 2022, 87, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Lewis, E.D.; Pae, M.; Meydani, S.N. Nutritional Modulation of Immune Function: Analysis of Evidence, Mechanisms, and Clinical Relevance. Front. Immunol. 2019, 9, 3160. [Google Scholar] [CrossRef]
- Zapatera, B.; Prados, A.; Gómez-Martínez, S.; Marcos, A. Immunonutrition: Methodology and applications. Nutr. Hosp. 2015, 31, 145–154. [Google Scholar]
- Jovanovich, A.; Isakova, T.; Stubbs, J. Microbiome and Cardiovascular Disease in CKD. Clin. J. Am. Soc. Nephrol. 2018, 13, 1598–1604. [Google Scholar] [CrossRef]
- Hatem-Vaquero, M.; de Frutos, S.; Luengo, A.; González Abajo, A.; Griera, M.; Rodríguez-Puyol, M.; Rodríguez-Puyol, D.; Calleros, L. Contribución de las toxinas urémicas a la fibrosis vascular asociada a la enfermedad renal crónica. Nefrología 2018, 38, 639–646. Available online: https://www.revistanefrologia.com/es-contribucion-toxinas-uremicas-fibrosis-vascular-articulo-S0211699518301401 (accessed on 3 April 2023).
- Pan, Y.; Yang, L.; Dai, B.; Lin, B.; Lin, S.; Lin, E. Effects of Probiotics on Malnutrition and Health-Related Quality of Life in Patients Undergoing Peritoneal Dialysis: A Randomized Controlled Trial. J. Ren. Nutr. 2021, 31, 199–205. [Google Scholar] [CrossRef]
- Armani, R.G.; Carvalho, A.B.; Ramos, C.I.; Hong, V.; Bortolotto, L.A.; Cassiolato, J.L.; Oliveira, N.F.; Cieslarova, Z.; Lago, C.L.D.; Klassen, A.; et al. Effect of fructooligosaccharide on endothelial function in CKD patients: A randomized controlled trial. Nephrol. Dial. Transplant. 2022, 37, 85–91. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.; Barrett, J.K.; Rice, S.; White, I.R.; Higgins, J.P.T. A design-by-treatment interaction model for network meta-analysis with random inconsistency effects. Stat Med. 2014, 33, 3639–3654. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Jackson, D.; Barrett, J.K.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Simeoni, M.; Citraro, M.L.; Cerantonio, A.; Deodato, F.; Provenzano, M.; Cianfrone, P.; Capria, M.; Corrado, S.; Libri, E.; Comi, A.; et al. An open-label, randomized, placebo-controlled study on the effectiveness of a novel probiotics administration protocol (ProbiotiCKD) in patients with mild renal insufficiency (stage 3a of CKD). Eur. J. Nutr. 2019, 58, 2145–2156. [Google Scholar]
- De Mauri, A.; Carrera, D.; Bagnati, M.; Rolla, R.; Vidali, M.; Chiarinotti, D.; Pane, M.; Amoruso, A.; Del Piano, M. Probiotics-Supplemented Low-Protein Diet for Microbiota Modulation in Patients with Advanced Chronic Kidney Disease (ProLowCKD): Results from a Placebo-Controlled Randomized Trial. Nutrients 2022, 14, 1637. [Google Scholar] [CrossRef]
- Cosola, C.; Rocchetti, M.T.; Cupisti, A.; Gesualdo, L. Microbiota metabolites: Pivotal players of cardiovascular damage in chronic kidney disease. Pharmacol. Res. 2018, 130, 132–142. [Google Scholar] [CrossRef]
- Ramos, C.I.; Armani, R.G.; Fernandes Canziani, M.E.; Dalboni, M.A.; Juliana, C.; Dolenga, R.; Nakao, L.S.; Campbell, K.L.; Cuppari, L. Effect of prebiotic (fructooligosaccharide) on uremic toxins of chronic kidney disease patients: A randomized controlled trial. Nephrol. Dial. Transplant. 2019, 34, 1876–1884. Available online: https://academic.oup.com/ndt/article/34/11/1876/5042969 (accessed on 8 January 2023).
- Ebrahim, Z.; Proost, S.; Tito, R.Y.; Raes, J.; Glorieux, G.; Moosa, M.R.; Blaauw, R. The Effect of ß-Glucan Prebiotic on Kidney Function, Uremic Toxins and Gut Microbiome in Stage 3 to 5 Chronic Kidney Disease (CKD) Predialysis Participants: A Randomized Controlled Trial. Nutrients 2022, 14, 805. [Google Scholar] [CrossRef] [PubMed]
- Cosola, C.; Rocchetti, M.M.; di Bari, I.; Acquaviva, P.M.; Maranzano, V.; Corciulo, S.; Di Ciaula, A.; Di Palo, D.M.; La Forgia, F.M.; Fontana, S.; et al. An Innovative Synbiotic Formulation Decreases Free Serum Indoxyl Sulfate, Small Intestine Permeability and Ameliorates Gastrointestinal Symptoms in a Randomized Pilot Trial in Stage IIIb-IV CKD Patients. Toxins 2021, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, C.; Krishnasamy, R.; Stanton, T.; Savill, E.; Snelson, M.; Mihala, G.; Kelly, J.T.; Morrison, M.; Johnson, D.W.; Campbell, K.L. Synbiotics Easing Renal Failure by Improving Gut Microbiology II (SYNERGY II): A Feasibility Randomized Controlled Trial. Nutrients 2021, 13, 4481. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Liu, H.; Chen, L.; Liang, S.-S.; Shi, K.; Meng, W.; Xue, J.; He, Q.; Jiang, H. Effect of probiotics on the intestinal microbiota of hemodialysis patients: A randomized trial. Eur. J. Nutr. 2020, 59, 3755–3766. [Google Scholar]
- Cruz-Mora, J.; Martínez-Hernández, N.E.; Martin del Campo-Lopez, F.; Viramontes-Hörner, D.; Vizmanos-Lamotte, B.; Muñoz-Valle, J.F.; García-García, G.; Parra-Rojas, I.; Castro-Alarcón, N. Effects of a Symbiotic on Gut Microbiota in Mexican Patients With End-Stage Renal Disease. J. Ren. Nutr. 2014, 24, 330–335. [Google Scholar] [CrossRef]
- Lydia, A.; Indra, T.A.; Rizka, A.; Abdullah, M. The effects of synbiotics on indoxyl sulphate level, constipation, and quality of life associated with constipation in chronic haemodialysis patients: A randomized controlled trial. BMC Nephrol. 2022, 23, 259. Available online: https://bmcnephrol.biomedcentral.com/articles/10.1186/s12882-022-02890-9 (accessed on 8 January 2023).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) Country | Aim | Design | Sample Size | Intervention | Statistics Analysis | Main Results |
|---|---|---|---|---|---|---|
| De Mauri (2022) Italy [29] | Evaluate whether the association of selected probiotics on top of a low protein diet was able to reduce the burden of uremic, microbiota-derived, and proatherogenic toxins in patients with advanced renal failure who were not on dialysis. | Placebo-controlled, randomized study | IG = 24 CG = 23 | Probiotic | Analysis of blood and urine samples. Shapiro–Wilk and q–q plot tests, Mann–Whitney U-test, Wilcoxon signed rank test and Kaplan–Meier analysis | Patients in the placebo group showed increased serum values of total cholesterol, LDL cholesterol, lipoprotein-associated phospholipase, and IS, while the 24 subjects in the probiotics group showed a trend in the reduction of microbiota toxins. A reduction of antihypertensive and diuretic medications was possible in the probiotics group. |
| Cosola (2021) Italy [33] | Investigate the effects of the synbiotic on the barrier permeability of different gastrointestinal tracts and on gastrointestinal symptoms assessed by the GSRS questionnaire. | Randomized trial | IG = 23 CG = 24 | Synbiotic | Urine and blood samples Linear regression analysis. Mann–Whitney test, Kruskal–Wallis multiple-comparison, Spearman, Fisher’s LSD. | Two-month administration of the synbiotic resulted in a decrease in free IS in the CKD group. After supplementation, reduction of small intestinal permeability and amelioration of abdominal pain and constipation syndromes were observed only in the CKD group. |
| McFarlane (2021) Australia [34] | Evaluate the feasibility of a trial of long-term synbiotic supplementation in adults with stage 3–4 CKD. | Double-blind, placebo-controlled, randomized trial | IG = 28 CG = 28 | Synbiotic | Blood and stool samples were collected. Chi-square, Fisher’s exact tests, Student’s t-test, and Mann–Whitney test | No differences were observed between free and total uremic toxins between placebo and synbiotic groups. Synbiotic supplementation resulted in a 3.14 mL/min/1.73 m2 reduction in eGFR and a 20.8 µmol/L increase in serum creatinine concentration. |
| Ramos (2019) Brazil [31] | Investigate the effect of a prebiotic fructooligosaccharide (FOS) on uremic toxins of non-dialysis-dependent CKD (NDD-CKD) patients. | Randomized trial | IG = 23 CG = 23 | Prebiotic | Blood samples were collected. Shapiro–Wilk test, chi-square, Fisher’s exact tests, Student’s t-test, and Mann–Whitney test. | There was a trend in the difference of serum total DPCS and serum-free Δ%PCS between the groups. Aside from the decreased high-density lipoprotein cholesterol in the intervention, no differences were observed in the change in IS, IAA, or other secondary outcome between the groups. |
| Simeoni (2019) Italy [28] | Describe gut dysbiosis in initial stages of CKD. | Clinical trial | IG = 24 CG = 23 | Probiotic | Blood, urine, and stool samples were collected. Student’s paired t test, Wilcoxon test, simple t test, Mann–Whitney U test, Pearson. | Mean fecal Lactobacillales and Bifidobacteria concentrations were increased only in the probiotics group. Conversely, mean urinary indican and 3-MI levels increased only in the group treated with probiotics. Compared to placebo group, significant improvements in C-reactive protein, iron, ferritin, transferrin saturation, β2-microglobulin, serum iPTH, and serum calcium were observed only in the probiotics group. |
| Ebrahim (2022) South Africa [32] | Investigate the effect of a ß-glucan prebiotic on kidney function, uremic toxins, and the gut microbiome in stage 3 to 5 CKD participants. | Randomized control trial | IG = 23 CG = 22 | Prebiotic | Blood samples for quantification of uremic toxins and stool samples for characterization of the gut microbiome were obtained. Kolmogorov, Mann–Whitney and chi-square tests. | There was a significant reduction in uremic toxin levels at different time points, in free IS at 8 weeks and 14 weeks, free pCS at 14 weeks, and total and free pCG. There were no differences in relative abundances of genera between groups. The ß-glucan prebiotic significantly altered uremic toxin levels of intestinal origin and favorably affected the gut microbiome. |
| Armani (2022) Brazil [19] | Evaluate the effect of the prebiotic FOS on endothelial function and arterial stiffness in non-dialysis CKD patients. | Randomized controlled trial | IG = 23 CG = 23 | Prebiotic | Fasting blood samples were collected. Kolmogorov–Smirnov, Student’s t-test, Mann–Whitney U-test, Wilcoxon, chi-squared analysis, Fischer’s test, and McNemar’s test. | There was a significant decrease in IL-6 levels and a trend toward pCS reduction only in the prebiotic group. Comparing both groups, there was no difference in FMD and PWV. FMD remained stable in the prebiotic group, while it decreased in the placebo group. |
| Probiotics | Prebiotics | Synbiotics | Control | |
|---|---|---|---|---|
| P-Cresyl Sulfate | 66.2 | 72.4 | 18.4 | 43.0 |
| Free p-Cresyl | 63.8 | 78.9 | 23.3 | 34.0 |
| Total Indoxyl Sulfate | 88.5 | 30.2 | 43.3 | 38.1 |
| Free Indoxyl Sulfate | 83.1 | 49.4 | 35.9 | 31.6 |
| Urea | 44.6 | 74.6 | -- | 30.8 |
| Creatinine | 60.5 | 56.9 | 19.4 | 63.2 |
| Phosphate | 67.8 | 21.1 | 39.3 | 71.8 |
| eGFR | 47.9 | 39.0 | 59.7 | 53.4 |
| All-Outcomes-Combined | 65.3 | 52.8 | 39.5 | 45.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cedillo-Flores, R.; Cuevas-Budhart, M.A.; Cavero-Redondo, I.; Kappes, M.; Ávila-Díaz, M.; Paniagua, R. Impact of Gut Microbiome Modulation on Uremic Toxin Reduction in Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis. Nutrients 2025, 17, 1247. https://doi.org/10.3390/nu17071247
Cedillo-Flores R, Cuevas-Budhart MA, Cavero-Redondo I, Kappes M, Ávila-Díaz M, Paniagua R. Impact of Gut Microbiome Modulation on Uremic Toxin Reduction in Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis. Nutrients. 2025; 17(7):1247. https://doi.org/10.3390/nu17071247
Chicago/Turabian StyleCedillo-Flores, Renata, Miguel Angel Cuevas-Budhart, Iván Cavero-Redondo, Maria Kappes, Marcela Ávila-Díaz, and Ramón Paniagua. 2025. "Impact of Gut Microbiome Modulation on Uremic Toxin Reduction in Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis" Nutrients 17, no. 7: 1247. https://doi.org/10.3390/nu17071247
APA StyleCedillo-Flores, R., Cuevas-Budhart, M. A., Cavero-Redondo, I., Kappes, M., Ávila-Díaz, M., & Paniagua, R. (2025). Impact of Gut Microbiome Modulation on Uremic Toxin Reduction in Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis. Nutrients, 17(7), 1247. https://doi.org/10.3390/nu17071247