


Trend and Burden of Suboptimal Breastfeeding in Children Under Five Years of Age in 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021

 ,
, _Qi.png) and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Data Sources
2.3. Sociodemographic Index (SDI)
2.4. Statistical Analysis
2.5. Ethics
2.6. Role of Funding Source
3. Results
3.1. Global
3.2. Sociodemographic Index
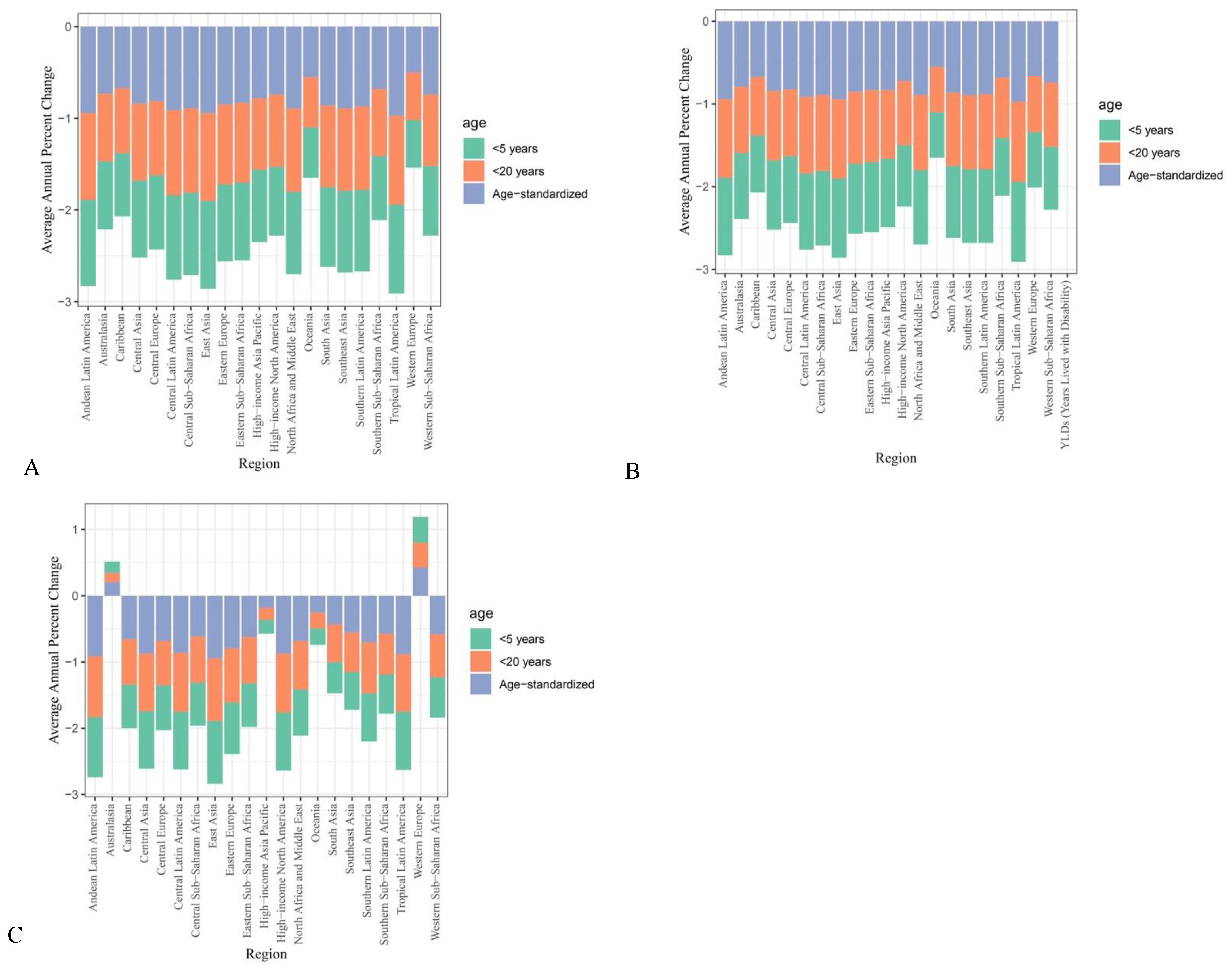
3.3. Regional
3.4. National
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| LMICs | Low-to-middle income countries |
| WHO | World Health Organization |
| DALYs | Disability-Adjusted Life Years |
| YLDs | Years Lost to Disability |
| AAPC | Average Annual Percentage Change |
| ASR | Age-Standardized Rate |
| SDI | Sociodemographic Index Score |
| ILO | International Labor Organization |
| BMS | Breastmilk Substitutes |
| WHA | World Health Assembly |
| LDI | Lag-Distributed Income |
| CI | Confidence Interval |
References
- Sankar, M.J.; Sinha, B.; Chowdhury, R.; Bhandari, N.; Taneja, S.; Martines, J.; Bahl, R. Optimal breastfeeding practices and infant and child mortality: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 3–13. [Google Scholar] [CrossRef]
- Victora, C.G.; Allen, K.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- North, K.; Gao, M.; Allen, G.; Lee, A.C. Breastfeeding in a global context: Epidemiology, impact, and future directions. Clin. Ther. 2022, 44, 228–244. [Google Scholar]
- World Health Organization. Guideline: Counselling of Women to Improve Breastfeeding Practices; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S. How many child deaths can we prevent this year? Lancet 2003, 362, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Likhar, A.; Patil, M.S. Importance of Maternal Nutrition in the First 1,000 Days of Life and Its Effects on Child Development: A Narrative Review. Cureus 2022, 14, e30083. [Google Scholar] [CrossRef] [PubMed]
- Snyder, K.; Hulse, E.; Dingman, H.; Cantrell, A.; Hanson, C.; Dinkel, D. Examining supports and barriers to breastfeeding through a socio-ecological lens: A qualitative study. Int. Breastfeed. J. 2021, 16, 52. [Google Scholar] [CrossRef] [PubMed]
- Piwoz, E.G.; Huffman, S.L. The impact of marketing of breast-milk substitutes on WHO-recommended breastfeeding practices. Food Nutr. Bull. 2015, 36, 373–386. [Google Scholar]
- Addati, L. Extending maternity protection to all women: Trends, challenges and opportunities. Int. Social. Secur. Rev. 2015, 68, 69–93. [Google Scholar]
- World Health Organization. Marketing of Breast-Milk Substitutes: National Implementation of the International Code, Status Report 2016; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Nguyen, T.T.; Weissman, A.; Cashin, J.; Ha, T.T.; Zambrano, P.; Mathisen, R. Assessing the Effectiveness of Policies Relating to Breastfeeding Promotion, Protection, and Support in Southeast Asia: Protocol for a Mixed Methods Study. JMIR Res. Protoc. 2020, 9, e21286. [Google Scholar] [CrossRef]
- Ferrari, A.J.; Santomauro, D.F.; Aali, A.; Abate, Y.H.; Abbafati, C.; Abbastabar, H.; Abd ElHafeez, S.; Abdelmasseh, M.; Abd-Elsalam, S.; Abdollahi, A.; et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2133–2161. [Google Scholar] [CrossRef]
- McLain, A.C.; Frongillo, E.A.; Hess, S.Y.; Piwoz, E.G. Comparison of Methods Used to Estimate the Global Burden of Disease Related to Undernutrition and Suboptimal Breastfeeding. Adv. Nutr. 2019, 10, 380–390. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, J.; Carter, A.; Casey, D.C.; Charlson, F.J.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Qi, Y.; Sun, J. Trend and Burden of Vitamin A Deficiency in 1990–2021 and Projection to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Nutrients 2025, 17, 572. [Google Scholar] [CrossRef] [PubMed]
- Go, D.S.; Kim, Y.E.; Yoon, S.J. Subnational Burden of Disease According to the Sociodemographic Index in South Korea. Int. J. Environ. Res. Public Health 2020, 17, 5788. [Google Scholar] [CrossRef]
- Magnano San Lio, R.; Maugeri, A.; La Rosa, M.C.; Cianci, A.; Panella, M.; Giunta, G.; Agodi, A.; Barchitta, M. The Impact of Socio-Demographic Factors on Breastfeeding: Findings from the “Mamma & Bambino” Cohort. Medicina 2021, 57, 103. [Google Scholar] [CrossRef] [PubMed]
- Kimuli, D.; Nakaggwa, F.; Namuwenge, N.; Nsubuga, R.N.; Isabirye, P.; Kasule, K.; Katwesige, J.F.; Nyakwezi, S.; Sevume, S.; Mubiru, N.; et al. Sociodemographic and health-related factors associated with exclusive breastfeeding in 77 districts of Uganda. Int. Breastfeed. J. 2023, 18, 66. [Google Scholar] [CrossRef]
- Unicef. Breastfeeding: A Mother’s Gift, for Every Child; Unicef: New York, NY, USA, 2018. [Google Scholar]
- Tariku, A.; Alemu, K.; Gizaw, Z.; Muchie, K.F.; Derso, T.; Abebe, S.M.; Yitayal, M.; Fekadu, A.; Ayele, T.A.; Alemayehu, G.A.; et al. Mothers’ education and ANC visit improved exclusive breastfeeding in Dabat Health and Demographic Surveillance System Site, northwest Ethiopia. PLoS ONE 2017, 12, e0179056. [Google Scholar] [CrossRef]
- Mohammed, S.; Yakubu, I.; Fuseini, A.G.; Abdulai, A.M.; Yakubu, Y.H. Systematic review and meta-analysis of the prevalence and determinants of exclusive breastfeeding in the first six months of life in Ghana. BMC Public Health 2023, 23, 920. [Google Scholar] [CrossRef]
- Temple Newhook, J.; Newhook, L.A.; Midodzi, W.K.; Murphy Goodridge, J.; Burrage, L.; Gill, N.; Halfyard, B.; Twells, L. Poverty and Breastfeeding: Comparing Determinants of Early Breastfeeding Cessation Incidence in Socioeconomically Marginalized and Privileged Populations in the FiNaL Study. Health Equity 2017, 1, 96–102. [Google Scholar] [CrossRef]
- Azeredo, C.M.; Conde, W.L.; Ferreira Antunes, J.L.; Lamounier, D.M.B.; Rinaldi, A.E.M. Sociodemographic, health and pro-breast-feeding policies and programmes associated with breast-feeding duration in Latin American countries. Public Health Nutr. 2021, 24, 4985–4996. [Google Scholar] [CrossRef]
- Carrijo, D.N.; Santos, M.N.; Azevedo, V.; Rinaldi, A.E.M. The trend of services provided by human milk banks between 2010 and 2019 in Brazil. J. Pediatr. 2022, 98, 572–578. [Google Scholar] [CrossRef]
- Cristiano Siqueira, B.; Elisa Maria de Aquino, L.; Neilane, B.; Natália, O.; Nadya Helena, A.-S.; Dayana Rodrigues, F.; Sandra Patricia, C.; Leticia Barroso Vertulli, C.; Raquel Machado, S.; Elsa Regina Justo, G.; et al. Trends of breastfeeding indicators in Brazil from 1996 to 2019 and the gaps to achieve the WHO/UNICEF 2030 targets. BMJ Glob. Health 2023, 8, e012529. [Google Scholar] [CrossRef]
- Murray, C.J.L. The Global Burden of Disease Study at 30 years. Nat. Med. 2022, 28, 2019–2026. [Google Scholar] [CrossRef]
- Naghavi, M.; Ong, K.L.; Aali, A.; Ababneh, H.S.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasian, M.; Abbasi-Kangevari, M.; Abbastabar, H.; et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2100–2132. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| DALYs 1 | Mortalities | YLDs 2 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1990 | 2021 | AAPC 3 (95% CI 4) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC | 1990 | 2021 | AAPC (95% CI) | |
| Rate | Rate | Number | Number | Rate | Rate | Number | Number | Rate | Rate | Rate | Number | Number | Rate | |||||
| Global | 7493.66 | 1391.89 | −0.82 (−0.85, −0.78) | 47,368,654.78 | 9,161,024.86 | −0.81 (−0.84, −0.76) | 84.23 | 15.35 | −0.82 (−0.85, −0.78) | 532,453.25 | 101,023.15 | −0.81 (−0.84, −0.76) | 44.84 | 14.71 | −0.6 (−0.63, −0.57) | 283,438.12 | 96,845.1 | −0.58 (−0.61, −0.55) |
| High SDI | 206.84 | 55.18 | −0.78 (−0.81, −0.74) | 119,226.91 | 29,712.3 | −0.81 (−0.84, −0.77) | 2.01 | 0.49 | −0.81 (−0.84, −0.78) | 1158.91 | 265.06 | −0.83 (−0.86, −0.81) | 29.1 | 11.01 | −0.31 (−0.37, −0.25) | 16,775.75 | 5930.56 | −0.39 (−0.45, −0.34) |
| High–middle SDI | 2414.48 | 150.89 | −0.92 (−0.94, −0.9) | 2,523,277.81 | 105,688.91 | −0.94 (−0.95, −0.93) | 26.83 | 1.61 | −0.92 (−0.94, −0.9) | 28,043.47 | 1128.24 | −0.94 (−0.95, −0.93) | 41.34 | 6.32 | −0.78 (−0.8, −0.76) | 43,202.94 | 4428.47 | −0.83 (−0.85, −0.82) |
| Middle SDI | 5908.91 | 612.07 | −0.89 (−0.91, −0.86) | 12,103,370.6 | 1,081,028.22 | −0.9 (−0.92, −0.88) | 66.29 | 6.7 | −0.89 (−0.91, −0.86) | 135,778.97 | 11,836.11 | −0.9 (−0.92, −0.88) | 47.33 | 10.77 | −0.73 (−0.75, −0.71) | 96,955.83 | 19,015.58 | −0.76 (−0.78, −0.75) |
| Low–middle SDI | 10,712.25 | 1509.13 | −0.87 (−0.9, −0.84) | 18,018,609.29 | 2,891,162.01 | −0.86 (−0.89, −0.82) | 120.61 | 16.62 | −0.87 (−0.9, −0.84) | 202,867.48 | 31,831.85 | −0.86 (−0.89, −0.83) | 45.64 | 18.01 | −0.56 (−0.6, −0.52) | 76,770.74 | 34,512.35 | −0.52 (−0.56, −0.47) |
| Low SDI | 15,091.25 | 3046.93 | −0.8 (−0.84, −0.75) | 14,574,421.08 | 5,044,966.15 | −0.63 (−0.71, −0.54) | 170.1 | 33.74 | −0.8 (−0.84, −0.75) | 164,270.38 | 55,868.35 | −0.63 (−0.71, −0.55) | 51.28 | 19.86 | −0.58 (−0.61, −0.53) | 49,522.23 | 32,881.08 | −0.23 (−0.29, −0.14) |
| DALYs 1 | Mortality | YLDs 2 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1990 | 2021 | AAPC 3 (95% CI 4) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | 1990 | 2021 | AAPC (95% CI) | |
| Rate | Rate | Number | Number | Rate | Rate | Number | Number | Rate | Rate | Number | Number | |||||||
| Andean Latin America | 6157.96 | 344.16 | −0.94 (−0.96, −0.92) | 335,398.76 | 21,186.1 | −0.93 (−0.95, −0.91) | 68.95 | 3.78 | −0.94 (−0.96, −0.92) | 3755.27 | 232.92 | −0.93 (−0.95, −0.91) | 64.64 | 4.79 | −0.91 (−0.93, −0.9) | 3520.88 | 295.1 | −0.9 (−0.91, −0.89) |
| Australasia | 80.95 | 26.64 | −0.74 (−0.8, −0.66) | 1248.83 | 483.78 | −0.69 (−0.76, −0.6) | 0.76 | 0.21 | −0.8 (−0.85, −0.74) | 11.77 | 3.89 | −0.76 (−0.82, −0.69) | 13.46 | 7.46 | 0.17 (−0.05, 0.44) | 207.65 | 135.44 | 0.37 (0.12, 0.69) |
| Caribbean | 10,859.59 | 3080.31 | −0.69 (−0.78, −0.57) | 449,488.73 | 119,151.75 | −0.71 (−0.8, −0.6) | 121.99 | 34.21 | −0.69 (−0.78, −0.57) | 5049.45 | 1323.21 | −0.71 (−0.8, −0.6) | 71.33 | 12.08 | −0.66 (−0.7, −0.62) | 2952.44 | 467.45 | −0.69 (−0.72, −0.65) |
| Central Asia | 8110.97 | 1098.18 | −0.84 (−0.87, −0.8) | 768,863.1 | 109,785.3 | −0.83 (−0.86, −0.79) | 91.13 | 12.17 | −0.84 (−0.87, −0.8) | 8638.89 | 1216.24 | −0.83 (−0.86, −0.79) | 49.3 | 5.71 | −0.87 (−0.88, −0.85) | 4673.73 | 570.92 | −0.86 (−0.87, −0.84) |
| Central Europe | 1163.02 | 213.85 | −0.81 (−0.85, −0.77) | 103,900.53 | 11,944.88 | −0.89 (−0.91, −0.86) | 12.69 | 2.34 | −0.81 (−0.85, −0.77) | 1133.97 | 130.95 | −0.89 (−0.91, −0.86) | 40.26 | 3.45 | −0.68 (−0.7, −0.65) | 3596.33 | 192.98 | −0.8 (−0.82, −0.79) |
| Central Latin America | 5588.09 | 485.52 | −0.92 (−0.94, −0.89) | 1,279,358.78 | 97,542.08 | −0.93 (−0.95, −0.91) | 62.63 | 5.37 | −0.92 (−0.94, −0.89) | 14,338.26 | 1079.76 | −0.93 (−0.95, −0.91) | 53.82 | 3.82 | −0.87 (−0.88, −0.85) | 12,322.29 | 767.78 | −0.88 (−0.9, −0.87) |
| Central Sub-Saharan Africa | 16,350.04 | 1544.68 | −0.9 (−0.93, −0.86) | 1,757,623.67 | 325,410.83 | −0.8 (−0.86, −0.71) | 184.23 | 17 | −0.9 (−0.93, −0.86) | 19,805.11 | 3580.34 | −0.8 (−0.86, −0.71) | 62.4 | 19.84 | −0.65 (−0.7, −0.59) | 6707.63 | 4179.27 | −0.29 (−0.39, −0.17) |
| East Asia | 4887.01 | 140.91 | −0.96 (−0.97, −0.95) | 5,856,276.32 | 112,830.93 | −0.97 (−0.98, −0.96) | 54.81 | 1.55 | −0.96 (−0.97, −0.94) | 65,684.81 | 1244.34 | −0.97 (−0.98, −0.96) | 39.95 | 1.4 | −0.95 (−0.96, −0.94) | 47,875.09 | 1124.01 | −0.97 (−0.97, −0.96) |
| Eastern Europe | 799.7 | 134.6 | −0.84 (−0.87, −0.82) | 137,776.53 | 13,619.94 | −0.91 (−0.92, −0.9) | 8.54 | 1.4 | −0.85 (−0.87, −0.82) | 1471.18 | 141.74 | −0.91 (−0.92, −0.9) | 43.92 | 8.87 | −0.78 (−0.8, −0.76) | 7566 | 897.72 | −0.87 (−0.88, −0.86) |
| Eastern Sub-Saharan Africa | 13,006.23 | 2121.74 | −0.85 (−0.89, −0.79) | 4,684,830.02 | 1,353,593.81 | −0.73 (−0.8, −0.63) | 146.55 | 23.46 | −0.85 (−0.89, −0.79) | 52,787.84 | 14,964.1 | −0.73 (−0.8, −0.63) | 50.58 | 17.37 | −0.66 (−0.69, −0.61) | 18,219.89 | 11,080.48 | −0.39 (−0.45, −0.32) |
| High-Income Asia Pacific | 110.68 | 38.29 | −0.79 (−0.83, −0.73) | 11,345.1 | 2470.41 | −0.87 (−0.9, −0.83) | 1.21 | 0.31 | −0.83 (−0.87, −0.79) | 124.23 | 19.71 | −0.9 (−0.92, −0.86) | 3.5 | 10.89 | −0.21 (−0.32, −0.12) | 358.46 | 702.74 | −0.5 (−0.57, −0.44) |
| High-Income North America | 117.28 | 40.95 | −0.75 (−0.79, −0.71) | 25,211.85 | 8393.38 | −0.77 (−0.8, −0.73) | 1.02 | 0.44 | −0.74 (−0.78, −0.7) | 218.85 | 89.31 | −0.75 (−0.79, −0.71) | 27.23 | 1.85 | −0.88 (−0.89, −0.86) | 5853.15 | 378.27 | −0.88 (−0.9, −0.87) |
| North Africa and Middle East | 7268.88 | 636.43 | −0.9 (−0.92, −0.87) | 3,877,351.15 | 389,093.75 | −0.88 (−0.91, −0.85) | 81.45 | 6.92 | −0.9 (−0.92, −0.87) | 43,448.23 | 4232.88 | −0.88 (−0.91, −0.85) | 64.07 | 15.09 | −0.7 (−0.74, −0.65) | 34,174.64 | 9225.34 | −0.64 (−0.68, −0.59) |
| Oceania | 4288.67 | 2210.15 | −0.55 (−0.67, −0.38) | 42,164.73 | 42,754.3 | −0.14 (−0.36, 0.19) | 47.98 | 24.42 | −0.55 (−0.67, −0.39) | 471.77 | 472.46 | −0.14 (−0.37, 0.18) | 48.45 | 20.75 | −0.25 (−0.36, −0.14) | 476.34 | 401.49 | 0.44 (0.23, 0.67) |
| South Asia | 7476.08 | 1364 | −0.87 (−0.9, −0.82) | 12,094,148.3 | 2,163,224.14 | −0.87 (−0.9, −0.82) | 84.14 | 15.01 | −0.87 (−0.9, −0.82) | 136,117.95 | 23,799.33 | −0.87 (−0.9, −0.82) | 32.66 | 16.92 | −0.47 (−0.51, −0.42) | 52,834.88 | 26,832.32 | −0.46 (−0.5, −0.41) |
| Southeast Asia | 7687.73 | 952.71 | −0.89 (−0.92, −0.86) | 4,572,961.7 | 536,227.27 | −0.9 (−0.92, −0.86) | 86.35 | 10.37 | −0.89 (−0.92, −0.86) | 51,361.64 | 5837.11 | −0.9 (−0.92, −0.86) | 51.22 | 21.98 | −0.57 (−0.6, −0.53) | 30,468.09 | 12,372.6 | −0.58 (−0.61, −0.55) |
| Southern Latin America | 862.57 | 120.19 | −0.89 (−0.91, −0.85) | 44,502.05 | 5142.12 | −0.9 (−0.93, −0.88) | 9.43 | 1.27 | −0.89 (−0.92, −0.85) | 486.68 | 54.17 | −0.91 (−0.93, −0.88) | 28.59 | 6.59 | −0.73 (−0.76, −0.69) | 1474.82 | 281.99 | −0.77 (−0.8, −0.74) |
| Southern Sub-Saharan Africa | 10,117.1 | 3481.01 | −0.7 (−0.76, −0.62) | 725,792.52 | 279,494.2 | −0.68 (−0.75, −0.59) | 113.77 | 38.53 | −0.7 (−0.77, −0.62) | 8161.72 | 3093.78 | −0.68 (−0.75, −0.59) | 58.48 | 25.32 | −0.59 (−0.62, −0.55) | 4195.5 | 2032.87 | −0.55 (−0.6, −0.51) |
| Tropical Latin America | 10,418.53 | 239.76 | −0.97 (−0.98, −0.96) | 1,828,996.76 | 41,256.33 | −0.97 (−0.98, −0.96) | 117.13 | 2.6 | −0.97 (−0.98, −0.96) | 20,561.64 | 447.27 | −0.97 (−0.98, −0.96) | 63.67 | 6.63 | −0.88 (−0.9, −0.86) | 11,177.75 | 1141.03 | −0.88 (−0.9, −0.86) |
| Western Europe | 118.82 | 58.6 | −0.52 (−0.61, −0.41) | 27,280.25 | 12,439.56 | −0.55 (−0.64, −0.46) | 0.87 | 0.37 | −0.67 (−0.73, −0.6) | 199.13 | 79.6 | −0.7 (−0.75, −0.63) | 42.12 | 24.97 | 0.39 (0.28, 0.51) | 9669.37 | 5300.24 | 0.28 (0.19, 0.39) |
| Western Sub-Saharan Africa | 24,511.9 | 4396.03 | −0.76 (−0.81, −0.7) | 8,744,135.08 | 3,514,980.01 | −0.46 (−0.57, −0.33) | 276.47 | 48.75 | −0.76 (−0.81, −0.7) | 98,624.85 | 38,980.03 | −0.46 (−0.57, −0.33) | 70.4 | 23.09 | −0.61 (−0.65, −0.56) | 25,113.18 | 18,465.06 | −0.13 (−0.21, −0.02) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, B.; Lin, K.; Buys, N.; Zhang, B.; Qi, Y.; Sun, J. Trend and Burden of Suboptimal Breastfeeding in Children Under Five Years of Age in 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Nutrients 2025, 17, 1134. https://doi.org/10.3390/nu17071134
Jiang B, Lin K, Buys N, Zhang B, Qi Y, Sun J. Trend and Burden of Suboptimal Breastfeeding in Children Under Five Years of Age in 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Nutrients. 2025; 17(7):1134. https://doi.org/10.3390/nu17071134
Chicago/Turabian StyleJiang, Bengui, Kelly Lin, Nicholas Buys, Bei Zhang, Yanfei Qi, and Jing Sun. 2025. "Trend and Burden of Suboptimal Breastfeeding in Children Under Five Years of Age in 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021" Nutrients 17, no. 7: 1134. https://doi.org/10.3390/nu17071134
APA StyleJiang, B., Lin, K., Buys, N., Zhang, B., Qi, Y., & Sun, J. (2025). Trend and Burden of Suboptimal Breastfeeding in Children Under Five Years of Age in 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Nutrients, 17(7), 1134. https://doi.org/10.3390/nu17071134