

Erythrocyte DHA/EPA Ratio Surpasses Its Individual Fatty Acid Levels in Predicting Metabolic Syndrome in Chinese Adults: A Prospective Study



Abstract
1. Introduction
2. Materials and Methods
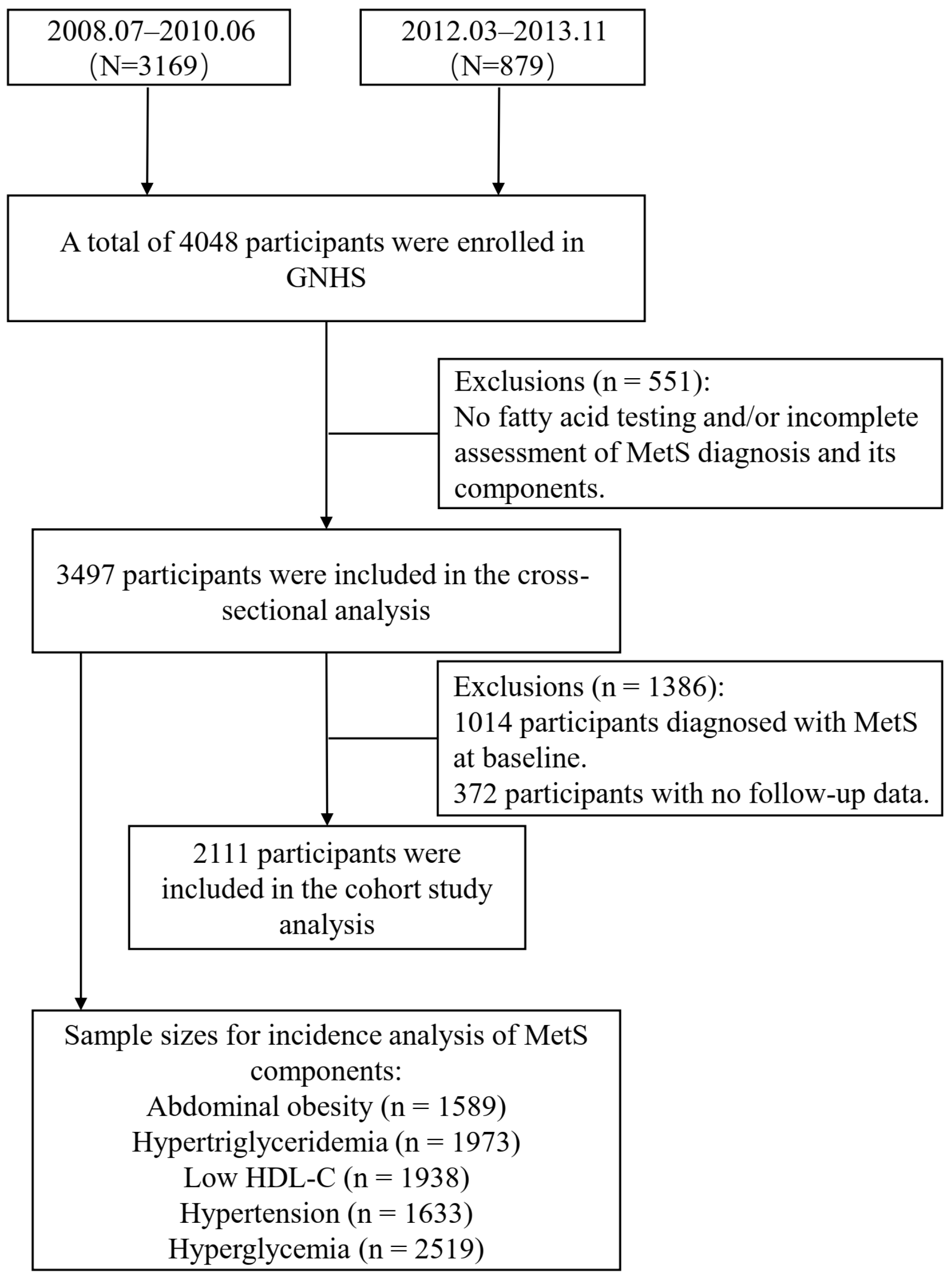
2.1. Study Participants
2.2. Data Collection
2.3. Laboratory Measurements
2.4. Definition of Metabolic Syndrome
2.5. Data Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Associations of EPA, DHA, and the DHA/EPA Ratio with the Prevalence of MetS and Its Components
3.3. Associations of EPA, DHA, and the DHA/EPA Ratio with 12-Year Incidence of MetS and Its Components
4. Discussion
4.1. EPA and Metabolic Health
4.2. DHA and Metabolic Health
4.3. DHA to EPA Ratio and Metabolic Health
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Özmen, M.; Yersal, Ö.; Öztürk, S.; Soysal, D.; Köseeoğlu, M.H. Prevalence of the metabolic syndrome in rheumatoid arthritis. Eur. J. Rheumatol. 2014, 1, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Wormser, D.; Kaptoge, S.; Di Angelantonio, E.; Wood, A.M.; Pennells, L.; Thompson, A.; Sarwar, N.; Kizer, J.R.; Lawlor, D.A.; Nordestgaard, B.G.; et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: Collaborative analysis of 58 prospective studies. Lancet 2011, 377, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wang, L.; Li, M.; Xu, Y.; Jiang, Y.; Wang, W.; Li, J.; Mi, S.; Zhang, M.; Li, Y.; et al. Metabolic Syndrome Among Adults in China: The 2010 China Noncommunicable Disease Surveillance. J. Clin. Endocrinol. Metab. 2017, 102, 507–515. [Google Scholar] [CrossRef]
- Gheldof, N.; Francey, C.; Rytz, A.; Egli, L.; Delodder, F.; Bovetto, L.; Piccardi, N.; Darimont, C. Effect of Different Nutritional Supplements on Glucose Response of Complete Meals in Two Crossover Studies. Nutrients 2022, 14, 2674. [Google Scholar] [CrossRef]
- Su, K.P.; Huang, S.Y.; Chiu, T.H.; Huang, K.C.; Huang, C.L.; Chang, H.C.; Pariante, C.M. Omega-3 fatty acids for major depressive disorder during pregnancy: Results from a randomized, double-blind, placebo-controlled trial. J. Clin. Psychiatry 2008, 69, 644–651. [Google Scholar] [CrossRef]
- Lopez-Huertas, E. The effect of EPA and DHA on metabolic syndrome patients: A systematic review of randomised controlled trials. Br. J. Nutr. 2012, 107 (Suppl. S2), S185–S194. [Google Scholar] [CrossRef]
- Aldhafiri, F.K. Investigating the Role of EPA and DHA on Cellular Oxidative Stress; Profiling Antidiabetic and Antihypertensive Potential. J. Pharm. Bioallied Sci. 2022, 14, 178–185. [Google Scholar] [CrossRef]
- Pall, M.L.; Levine, S. Nrf2, a master regulator of detoxification and also antioxidant, anti-inflammatory and other cytoprotective mechanisms, is raised by health promoting factors. Sheng Li Xue Bao 2015, 67, 1–18. [Google Scholar]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef]
- Serhan, C.N.; Levy, B.D. Resolvins in inflammation: Emergence of the pro-resolving superfamily of mediators. J. Clin. Investig. 2018, 128, 2657–2669. [Google Scholar] [CrossRef]
- Chiang, N.; Serhan, C.N. Specialized pro-resolving mediator network: An update on production and actions. Essays Biochem. 2020, 64, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.W.; Chen, Y.M.; Zeng, F.F.; Sun, L.L.; Chen, C.G.; Su, Y.X. Association between n-3 polyunsaturated fatty acids in erythrocytes and metabolic syndrome in Chinese men and women. Eur. J. Nutr. 2016, 55, 981–989. [Google Scholar] [CrossRef]
- Mori, T.A.; Burke, V.; Puddey, I.; Irish, A.; Cowpland, C.A.; Beilin, L.; Dogra, G.; Watts, G.F. The effects of [omega]3 fatty acids and coenzyme Q10 on blood pressure and heart rate in chronic kidney disease: A randomized controlled trial. J. Hypertens. 2009, 27, 1863–1872. [Google Scholar] [CrossRef]
- Andone, S.; Farczádi, L.; Imre, S.; Bălașa, R. Fatty Acids and Lipid Paradox-Neuroprotective Biomarkers in Ischemic Stroke. Int. J. Mol. Sci. 2022, 23, 10810. [Google Scholar] [CrossRef] [PubMed]
- AbuMweis, S.; Abu Omran, D.; Al-Shami, I.; Jew, S. The ratio of eicosapentaenoic acid to docosahexaenoic acid as a modulator for the cardio-metabolic effects of omega-3 supplements: A meta-regression of randomized clinical trials. Complement. Ther. Med. 2021, 57, 102662. [Google Scholar] [CrossRef] [PubMed]
- Dasilva, G.; Pazos, M.; García-Egido, E.; Pérez-Jiménez, J.; Torres, J.L.; Giralt, M.; Nogués, M.R.; Medina, I. Lipidomics to analyze the influence of diets with different EPA:DHA ratios in the progression of Metabolic Syndrome using SHROB rats as a model. Food Chem. 2016, 205, 196–203. [Google Scholar] [CrossRef]
- Andersen, G.; Harnack, K.; Erbersdobler, H.F.; Somoza, V. Dietary eicosapentaenoic acid and docosahexaenoic acid are more effective than alpha-linolenic acid in improving insulin sensitivity in rats. Ann. Nutr. Metab. 2008, 52, 250–256. [Google Scholar] [CrossRef]
- Lluís, L.; Taltavull, N.; Muñoz-Cortés, M.; Sánchez-Martos, V.; Romeu, M.; Giralt, M.; Molinar-Toribio, E.; Torres, J.L.; Pérez-Jiménez, J.; Pazos, M.; et al. Protective effect of the omega-3 polyunsaturated fatty acids: Eicosapentaenoic acid/Docosahexaenoic acid 1:1 ratio on cardiovascular disease risk markers in rats. Lipids Health Dis. 2013, 12, 140. [Google Scholar] [CrossRef]
- Dasilva, G.; Pazos, M.; García-Egido, E.; Gallardo, J.M.; Rodríguez, I.; Cela, R.; Medina, I. Healthy effect of different proportions of marine ω-3 PUFAs EPA and DHA supplementation in Wistar rats: Lipidomic biomarkers of oxidative stress and inflammation. J. Nutr. Biochem. 2015, 26, 1385–1392. [Google Scholar] [CrossRef]
- Wang, P.; Chen, Y.M.; He, L.P.; Chen, C.G.; Zhang, B.; Xue, W.Q.; Su, Y.X. Association of natural intake of dietary plant sterols with carotid intima-media thickness and blood lipids in Chinese adults: A cross-section study. PLoS ONE 2012, 7, e32736. [Google Scholar] [CrossRef]
- Yang, Y.X.; Wang, G.; Pan, X. China Food Composition Table 2002; Beijing Medical University: Beijing, China, 2002. [Google Scholar]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Ding, D.; Li, Y.H.; Xiao, M.L.; Dong, H.L.; Lin, J.S.; Chen, G.D.; Chen, Z.Y.; Tang, X.Y.; Chen, Y.M. Erythrocyte Membrane Polyunsaturated Fatty Acids Are Associated with Incidence of Metabolic Syndrome in Middle-Aged and Elderly People-An 8.8-Year Prospective Study. J. Nutr. 2020, 150, 1488–1498. [Google Scholar] [CrossRef]
- Jang, H.; Park, K. Omega-3 and omega-6 polyunsaturated fatty acids and metabolic syndrome: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 765–773. [Google Scholar] [CrossRef]
- Woodman, R.J.; Mori, T.A.; Burke, V.; Puddey, I.B.; Watts, G.F.; Beilin, L.J. Effects of purified eicosapentaenoic and docosahexaenoic acids on glycemic control, blood pressure, and serum lipids in type 2 diabetic patients with treated hypertension. Am. J. Clin. Nutr. 2002, 76, 1007–1015. [Google Scholar] [CrossRef]
- Mori, T.A.; Bao, D.Q.; Burke, V.; Puddey, I.B.; Beilin, L.J. Docosahexaenoic acid but not eicosapentaenoic acid lowers ambulatory blood pressure and heart rate in humans. Hypertension 1999, 34, 253–260. [Google Scholar] [CrossRef]
- Yang, X.; Li, X.; Hu, M.; Huang, J.; Yu, S.; Zeng, H.; Mao, L. EPA and DHA differentially improve insulin resistance by reducing adipose tissue inflammation-targeting GPR120/PPARγ pathway. J. Nutr. Biochem. 2024, 130, 109648. [Google Scholar] [CrossRef]
- Kalupahana, N.S.; Claycombe, K.; Newman, S.J.; Stewart, T.; Siriwardhana, N.; Matthan, N.; Lichtenstein, A.H.; Moustaid-Moussa, N. Eicosapentaenoic acid prevents and reverses insulin resistance in high-fat diet-induced obese mice via modulation of adipose tissue inflammation. J. Nutr. 2010, 140, 1915–1922. [Google Scholar] [CrossRef]
- Yu, S.; Xie, Q.; Tan, W.; Hu, M.; Xu, G.; Zhang, X.; Xie, G.; Mao, L. Different ratios of DHA/EPA reverses insulin resistance by improving adipocyte dysfunction and lipid disorders in HFD-induced IR mice. Food Funct. 2023, 14, 1179–1197. [Google Scholar] [CrossRef]
- Greupner, T.; Kutzner, L.; Nolte, F.; Strangmann, A.; Kohrs, H.; Hahn, A.; Schebb, N.H.; Schuchardt, J.P. Effects of a 12-week high-α-linolenic acid intervention on EPA and DHA concentrations in red blood cells and plasma oxylipin pattern in subjects with a low EPA and DHA status. Food Funct. 2018, 9, 1587–1600. [Google Scholar] [CrossRef]
- Flachs, P.; Horakova, O.; Brauner, P.; Rossmeisl, M.; Pecina, P.; Franssen-van Hal, N.; Ruzickova, J.; Sponarova, J.; Drahota, Z.; Vlcek, C.; et al. Polyunsaturated fatty acids of marine origin upregulate mitochondrial biogenesis and induce beta-oxidation in white fat. Diabetologia 2005, 48, 2365–2375. [Google Scholar] [CrossRef]
- Minihane, A.M. Impact of Genotype on EPA and DHA Status and Responsiveness to Increased Intakes. Nutrients 2016, 8, 123. [Google Scholar] [CrossRef]
- Bertrand, C.; Pignalosa, A.; Wanecq, E.; Rancoule, C.; Batut, A.; Deleruyelle, S.; Lionetti, L.; Valet, P.; Castan-Laurell, I. Effects of dietary eicosapentaenoic acid (EPA) supplementation in high-fat fed mice on lipid metabolism and apelin/APJ system in skeletal muscle. PLoS ONE 2013, 8, e78874. [Google Scholar] [CrossRef]
- Ghasemi Fard, S.; Wang, F.; Sinclair, A.J.; Elliott, G.; Turchini, G.M. How does high DHA fish oil affect health? A systematic review of evidence. Crit. Rev. Food Sci. Nutr. 2019, 59, 1684–1727. [Google Scholar] [CrossRef]
- Hashimoto, M.; Shinozuka, K.; Gamoh, S.; Tanabe, Y.; Hossain, M.S.; Kwon, Y.M.; Hata, N.; Misawa, Y.; Kunitomo, M.; Masumura, S. The hypotensive effect of docosahexaenoic acid is associated with the enhanced release of ATP from the caudal artery of aged rats. J. Nutr. 1999, 129, 70–76. [Google Scholar] [CrossRef]
- McLennan, P.; Howe, P.; Abeywardena, M.; Muggli, R.; Raederstorff, D.; Mano, M.; Rayner, T.; Head, R. The cardiovascular protective role of docosahexaenoic acid. Eur. J. Pharmacol. 1996, 300, 83–89. [Google Scholar] [CrossRef]
- Pifferi, F.; Cunnane, S.C.; Guesnet, P. Evidence of the Role of Omega-3 Polyunsaturated Fatty Acids in Brain Glucose Metabolism. Nutrients 2020, 12, 1382. [Google Scholar] [CrossRef]
- Mori, T.A.; Burke, V.; Puddey, I.B.; Watts, G.F.; O’Neal, D.N.; Best, J.D.; Beilin, L.J. Purified eicosapentaenoic and docosahexaenoic acids have differential effects on serum lipids and lipoproteins, LDL particle size, glucose, and insulin in mildly hyperlipidemic men. Am. J. Clin. Nutr. 2000, 71, 1085–1094. [Google Scholar] [CrossRef]
- Nakasatomi, M.; Kim, H.; Arai, T.; Hirako, S.; Shioda, S.; Iizuka, Y.; Sakurai, K.; Matsumoto, A. Fish oil and fenofibrate inhibit pancreatic islet hypertrophy, and improve glucose and lipid metabolic dysfuntions with different ways in diabetic KK mice. Obes. Res. Clin. Pract. 2018, 12, 29–38. [Google Scholar] [CrossRef]
- Prostek, A.; Gajewska, M.; Bałasińska, B. The influence of eicosapentaenoic acid and docosahexaenoic acid on expression of genes connected with metabolism and secretory functions of ageing 3T3-L1 adipocytes. Prostaglandins Other Lipid Mediat. 2016, 125, 48–56. [Google Scholar] [CrossRef]
- Pal, A.; Metherel, A.H.; Fiabane, L.; Buddenbaum, N.; Bazinet, R.P.; Shaikh, S.R. Do Eicosapentaenoic Acid and Docosahexaenoic Acid Have the Potential to Compete against Each Other? Nutrients 2020, 12, 3718. [Google Scholar] [CrossRef]
- Preston Mason, R. New Insights into Mechanisms of Action for Omega-3 Fatty Acids in Atherothrombotic Cardiovascular Disease. Curr. Atheroscler. Rep. 2019, 21, 2. [Google Scholar] [CrossRef]
- Liu, L.; Hu, Q.; Wu, H.; Xue, Y.; Cai, L.; Fang, M.; Liu, Z.; Yao, P.; Wu, Y.; Gong, Z. Protective role of n6/n3 PUFA supplementation with varying DHA/EPA ratios against atherosclerosis in mice. J. Nutr. Biochem. 2016, 32, 171–180. [Google Scholar] [CrossRef]
- Shang, T.; Liu, L.; Zhou, J.; Zhang, M.; Hu, Q.; Fang, M.; Wu, Y.; Yao, P.; Gong, Z. Protective effects of various ratios of DHA/EPA supplementation on high-fat diet-induced liver damage in mice. Lipids Health Dis. 2017, 16, 65. [Google Scholar] [CrossRef]
- Toth, P.P.; Chapman, M.J.; Parhofer, K.G.; Nelson, J.R. Differentiating EPA from EPA/DHA in cardiovascular risk reduction. Am. Heart J. Plus 2022, 17, 100148. [Google Scholar] [CrossRef]
- Shimokawa, H.; Vanhoutte, P.M. Dietary omega 3 fatty acids and endothelium-dependent relaxations in porcine coronary arteries. Am. J. Physiol. 1989, 256, H968–H973. [Google Scholar] [CrossRef]
- Yin, K.; Chu, Z.M.; Beilin, L.J. Blood pressure and vascular reactivity changes in spontaneously hypertensive rats fed fish oil. Br. J. Pharmacol. 1991, 102, 991–997. [Google Scholar] [CrossRef]
- Chu, Z.M.; Yin, K.; Beilin, L.J. Fish oil feeding selectively attenuates contractile responses to noradrenaline and electrical stimulation in the perfused mesenteric resistance vessels of spontaneously hypertensive rats. Clin. Exp. Pharmacol. Physiol. 1992, 19, 177–181. [Google Scholar] [CrossRef]
- McVeigh, G.E.; Brennan, G.M.; Cohn, J.N.; Finkelstein, S.M.; Hayes, R.J.; Johnston, G.D. Fish oil improves arterial compliance in non-insulin-dependent diabetes mellitus. Arterioscler. Thromb. 1994, 14, 1425–1429. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Participants (n = 3497) | Non-MetS (n = 2483) | MetS (n = 1014) | P |
|---|---|---|---|---|
| Age, year | 58.00 (54.00, 63.00) | 57.00 (54.00, 62.00) | 60.00 (55.00, 65.30) | <0.001 |
| gender n (%) | <0.001 | |||
| women | 2390 (68.34) | 1651 (66.49) | 739 (72.87) | |
| men | 1107 (31.65) | 832 (33.51) | 275 (27.13) | |
| Current smoker n (%) | 631 (18.04) | 417 (16.79) | 160 (15.78) | 0.494 |
| Current drinker n (%) | 239 (6.83) | 164 (6.60) | 75 (7.39) | 0.443 |
| Education level n (%) | <0.001 | |||
| Middle school | 1056 (30.19) | 703 (28.31) | 353 (34.81) | |
| High school or professional college | 1591 (45.49) | 1171 (47.16) | 420 (41.42) | |
| University | 850 (24.30) | 609 (24.53) | 241 (23.77) | |
| Household income (Chinese Yuan/month/person) n (%) | 0.012 | |||
| <1500 | 1729 (49.44) | 1254 (50.50) | 475 (46.84) | |
| 1500–3000 | 851(24.34) | 613 (24.69) | 238 (23.47) | |
| ≥3000 | 917 (26.22) | 616 (24.81) | 301 (29.68) | |
| Physical activity MET/d | 35.60 (30.50, 49.70) | 36.20 (30.90, 52.20) | 34.20 (29.80, 45.20) | <0.001 |
| BMI kg/m2 | 23.20 (21.20, 25.30) | 22.40 (20.60, 24.20) | 25.20 (23.40, 26.90) | <0.001 |
| Waist circumference cm | 83.00 (77.00, 89.30) | 80.30 (75.00, 86.50) | 89.00 (84.00, 94.00) | <0.001 |
| SBP mmHg | 122 (110, 135) | 120 (110, 130) | 131 (121, 141) | <0.001 |
| DBP mmHg | 79 (70, 83) | 76 (70, 80) | 80 (75, 89) | <0.001 |
| Fasting glucose mmol/L | 4.70 (4.30, 5.20) | 4.60 (4.20, 5.00) | 5.10 (4.50, 5.82) | <0.001 |
| Serum lipids mmol/L | ||||
| TG mmol/L | 1.31 (0.93, 1.83) | 1.12 (0.84, 1.49) | 1.97 (1.44, 2.72) | <0.001 |
| TC mmol/L | 5.44 (4.75, 6.16) | 5.41 (4.75, 6.11) | 5.49 (4.77, 6.26) | 0.044 |
| HDL-c mmol/L | 1.36 (1.16, 1.59) | 1.45 (1.25, 1.67) | 1.16 (1.01, 1.29) | <0.001 |
| LDL-c mmol/L | 3.54 (2.98, 4.13) | 3.54 (3.02, 4.11) | 3.55 (2.90, 4.19) | 0.579 |
| Erythrocyte FA composition% of total fatty acids | ||||
| EPA(C20:5)% | 0.56 (0.37, 1.26) | 0.55 (0.36, 1.07) | 0.60 (0.38, 1.46) | <0.001 |
| DHA(C22:6)% | 4.54 (3.73, 5.31) | 4.63 (3.80, 5.43) | 4.33 (3.65, 5.02) | <0.001 |
| DHA/EPA ratio% | 8.38 (4.03, 11.36) | 8.64 (5.03, 11.50) | 7.75 (2.97, 10.87) | <0.001 |
| Dietary daily intakes | ||||
| DHA(C22:6) mg/d | 0.03 (0.02, 0.05) | 0.03 (0.02, 0.05) | 0.03 (0.02, 0.05) | 0.132 |
| EPA(C20:5) mg/d | 0.02 (0.01, 0.03) | 0.02 (0.01, 0.03) | 0.02 (0.01, 0.03) | 0.039 |
| DHA/EPA intake ratio% | 1.60 (1.33, 2.00) | 1.57 (1.33, 2.00) | 1.67 (1.33, 2.00) | 0.148 |
| Energy intake kcal/d | 1687 (1408, 2068) | 1708 (1432, 2098) | 1645 (1352, 1988) | <0.001 |
| Fiber g/d | 10.54 (8.08, 13.64) | 10.61 (8.15, 13.74) | 10.22 (7.95, 13.19) | 0.018 |
| SFA g/d | 14.10 (10.50, 18.70) | 14.20 (10.70, 19.00) | 13.70 (10.10, 18.00) | 0.002 |
| Variables | ORs (95% CI) by Quartiles of n-3 PUFA Concentrations | P-Trend | |||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | ||
| EPA(C20:5) | |||||
| Median (%) | 0.27 | 0.45 | 0.72 | 1.62 | |
| Case/n | 240/875 | 239/874 | 218/873 | 317/875 | |
| Crude Model | 1.00 | 1.00 (0.81, 1.23) | 0.88 (0.71, 1.09) | 1.50 (1.23, 1.84) | <0.001 |
| Model 1 | 1.00 | 0.99 (0.80, 1.23) | 0.86 (0.70, 1.07) | 1.36 (1.10, 1.67) | 0.016 |
| Model 2 | 1.00 | 0.98 (0.79, 1.22) | 0.86 (0.69, 1.07) | 1.32 (1.07, 1.62) | 0.033 |
| DHA(C22:6) | |||||
| Median | 3.02 | 4.16 | 4.89 | 5.86 | |
| Case/n | 292/875 | 307/874 | 243/873 | 172/875 | |
| Crude Model | 1.00 | 1.08 (0.89, 1.32) | 0.77 (0.63, 0.94) | 0.49 (0.39, 0.61) | <0.001 |
| Model 1 | 1.00 | 1.05 (0.86, 1.29) | 0.71 (0.58, 0.88) | 0.48 (0.39, 0.60) | <0.001 |
| Model 2 | 1.00 | 1.04 (0.85, 1.28) | 0.70 (0.57, 0.86) | 0.48 (0.39, 0.60) | <0.001 |
| DHA/EPA ratio | |||||
| Median | 2.60 | 6.76 | 9.86 | 13.61 | |
| Case/n | 326/875 | 236/874 | 229/873 | 223/875 | |
| Crude Model | 1.00 | 0.62 (0.51, 0.76) | 0.60 (0.49, 0.73) | 0.58 (0.47, 0.71) | <0.001 |
| Model 1 | 1.00 | 0.65 (0.53, 0.80) | 0.65 (0.53, 0.80) | 0.63 (0.51, 0.77) | <0.001 |
| Model 2 | 1.00 | 0.66 (0.53, 0.81) | 0.67 (0.54, 0.83) | 0.64 (0.52, 0.79) | <0.001 |
| Variables | Abdominal Obesity | HTG | LOW HDL-C | Hypertension | Hyperglycemia |
|---|---|---|---|---|---|
| Cases/n | 1652/3497 | 1168/3497 | 1193/3497 | 1628/3497 | 549/3497 |
| EPA(C20:5) | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 1 | 1.19 (0.98, 1.45) | 0.97 (0.80, 1.19) | 0.82 (0.67, 1.01) | 1.03 (0.84, 1.25) | 1.01 (0.76, 1.36) |
| Quartile 3 1 | 1.19 (0.98, 1.46) | 0.80 (0.65, 0.98) | 0.84 (0.68, 1.02) | 1.01 (0.83, 1.23) | 1.12 (0.84, 1.49) |
| Quartile 4 1 | 1.29 (1.06, 1.58) | 1.24 (1.01, 1.51) | 1.11 (0.91, 1.35) | 1.40 (1.15, 1.70) | 1.91 (1.46, 2.48) |
| P-trend | 0.263 | 0.263 | 0.560 | 0.010 | <0.001 |
| DHA(C22:6) | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 | 1.05 (0.86, 1.28) | 0.88 (0.72, 1.06) | 1.04 (0.85, 1.27) | 1.03 (0.85, 1.25) | 1.11 (0.86, 1.42) |
| Quartile 3 | 0.85 (0.69, 1.04) | 0.74 (0.61, 0.91) | 0.88 (0.72, 1.08) | 0.78 (0.64, 0.95) | 0.89 (0.69, 1.16) |
| Quartile 4 | 0.80 (0.66, 0.98) | 0.53 (0.43, 0.65) | 0.80 (0.65, 0.98) | 0.60 (0.49, 0.73) | 0.54 (0.40, 0.72) |
| P-trend | 0.855 | <0.001 | 0.073 | <0.001 | <0.001 |
| DHA/EPA ratio | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 | 0.97 (0.79, 1.18) | 0.69 (0.56, 0.84) | 0.73 (0.60, 0.89) | 0.75 (0.62, 0.91) | 0.48 (0.37, 0.61) |
| Quartile 3 | 0.88 (0.72, 1.08) | 0.66 (0.54, 0.81) | 0.82 (0.67, 1.01) | 0.72 (0.59, 0.87) | 0.44 (0.33, 0.57) |
| Quartile 4 | 0.72 (0.59, 0.88) | 0.70 (0.58, 0.86) | 0.79 (0.65, 0.97) | 0.64 (0.52, 0.77) | 0.51 (0.40, 0.66) |
| P-trend | 0.068 | 0.003 | 0.185 | <0.001 | <0.001 |
| Variables | HRs (95% CI) by Quartiles of n-3 PUFA Concentrations | P-Trend | |||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | ||
| EPA(C20:5) | |||||
| Median (%) | 0.27 | 0.45 | 0.73 | 1.61 | |
| Case/n | 171/532 | 188/537 | 213/583 | 194/459 | |
| Crude Model | 1.00 | 1.05 (0.86, 1.30) | 1.15 (0.94, 1.40) | 1.37 (1.12, 1.68) | 0.002 |
| Model 1 | 1.00 | 1.05 (0.86, 1.30) | 1.13 (0.93, 1.38) | 1.28 (1.04, 1.57) | 0.015 |
| Model 2 | 1.00 | 1.06 (0.86, 1.31) | 1.12 (0.91, 1.37) | 1.26 (1.02, 1.55) | 0.032 |
| DHA(C22:6) | |||||
| Median | 3.04 | 4.15 | 4.89 | 5.88 | |
| Case/n | 178/481 | 172/482 | 216/534 | 200/614 | |
| Crude Model | 1.00 | 0.98 (0.80, 1.21) | 1.12 (0.92, 1.37) | 0.85 (0.70, 1.04) | 0.240 |
| Model 1 | 1.00 | 0.99 (0.81, 1.23) | 1.12 (0.91, 1.36) | 0.87 (0.71, 1.06) | 0.294 |
| Model 2 | 1.00 | 1.00 (0.81, 1.24) | 1.14 (0.93, 1.40) | 0.89 (0.72, 1.09) | 0.422 |
| DHA/EPA ratio | |||||
| Median | 2.65 | 6.72 | 9.88 | 13.51 | |
| Case/n | 189/452 | 216/562 | 209/549 | 152/548 | |
| Crude Model | 1.00 | 0.89 (0.73, 1.08) | 0.86 (0.71, 1.05) | 0.63 (0.51, 0.78) | <0.001 |
| Model 1 | 1.00 | 0.93 (0.76, 1.13) | 0.92 (0.76, 1.13) | 0.67 (0.54, 0.83) | <0.001 |
| Model 2 | 1.00 | 0.95 (0.78, 1.16) | 0.95 (0.78, 1.17) | 0.70 (0.56, 0.86) | 0.002 |
| Variables | Abdominal Obesity | HTG | LOW HDL-C | Hypertension | Hyperglycemia |
|---|---|---|---|---|---|
| Cases/n | 751/1589 | 736/1973 | 668/1938 | 558/1633 | 924/2519 |
| EPA(C20:5) | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 1 | 0.99 (0.81, 1.21) | 1.02 (0.83, 1.25) | 0.97 (0.78, 1.21) | 0.81 (0.64, 1.02) | 1.00 (0.83, 1.22) |
| Quartile 3 1 | 1.06 (0.87, 1.29) | 0.94 (0.77, 1.16) | 0.98 (0.79, 1.22) | 0.84 (0.67, 1.06) | 1.19 (0.99, 1.43) |
| Quartile 4 1 | 1.10 (0.89, 1.36) | 1.10 (0.89, 1.36) | 1.03 (0.83, 1.29) | 0.88 (0.69, 1.12) | 1.24 (1.02, 1.50) |
| P-trend | 0.311 | 0.564 | 0.780 | 0.338 | 0.007 |
| DHA(C22:6) | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 | 0.98 (0.79, 1.21) | 0.99 (0.80, 1.23) | 1.02 (0.82, 1.27) | 0.82 (0.65, 1.05) | 1.09 (0.90, 1.32) |
| Quartile 3 | 1.04 (0.85, 1.27) | 1.06 (0.86, 1.31) | 1.06 (0.86, 1.31) | 0.67 (0.53, 0.86) | 1.04 (0.86, 1.26) |
| Quartile 4 | 0.89 (0.73, 1.10) | 0.87 (0.71, 1.08) | 0.80 (0.64, 1.00) | 0.76 (0.61, 0.96) | 1.05 (0.87, 1.26) |
| P-trend | 0.392 | 0.279 | 0.071 | <0.001 | 0.748 |
| DHA/EPA ratio | |||||
| Quartile 1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Quartile 2 | 0.99 (0.80, 1.22) | 0.90 (0.73, 1.11) | 0.94 (0.76, 1.17) | 1.08 (0.85, 1.38) | 1.00 (0.83, 1.20) |
| Quartile 3 | 0.88 (0.71, 1.09) | 0.99 (0.81, 1.22) | 1.09 (0.88, 1.36) | 0.89 (0.69, 1.14) | 0.89 (0.74, 1.07) |
| Quartile 4 | 0.93 (0.75, 1.14) | 0.80 (0.64, 0.99) | 0.90 (0.72, 1.12) | 0.96 (0.75, 1.23) | 0.79 (0.65, 0.96) |
| P-trend | 0.318 | 0.104 | 0.637 | 0.381 | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, P.; Yan, Y.; Chen, H.; Ru, D.; Wang, X.; Chen, Y. Erythrocyte DHA/EPA Ratio Surpasses Its Individual Fatty Acid Levels in Predicting Metabolic Syndrome in Chinese Adults: A Prospective Study. Nutrients 2025, 17, 1096. https://doi.org/10.3390/nu17061096
Feng P, Yan Y, Chen H, Ru D, Wang X, Chen Y. Erythrocyte DHA/EPA Ratio Surpasses Its Individual Fatty Acid Levels in Predicting Metabolic Syndrome in Chinese Adults: A Prospective Study. Nutrients. 2025; 17(6):1096. https://doi.org/10.3390/nu17061096
Chicago/Turabian StyleFeng, Pinning, Yan Yan, Hanzu Chen, Dongmei Ru, Xinyue Wang, and Yuming Chen. 2025. "Erythrocyte DHA/EPA Ratio Surpasses Its Individual Fatty Acid Levels in Predicting Metabolic Syndrome in Chinese Adults: A Prospective Study" Nutrients 17, no. 6: 1096. https://doi.org/10.3390/nu17061096
APA StyleFeng, P., Yan, Y., Chen, H., Ru, D., Wang, X., & Chen, Y. (2025). Erythrocyte DHA/EPA Ratio Surpasses Its Individual Fatty Acid Levels in Predicting Metabolic Syndrome in Chinese Adults: A Prospective Study. Nutrients, 17(6), 1096. https://doi.org/10.3390/nu17061096