
Efficacy of Oral Supplementation with Cholecalciferol Versus Calcifediol in Patients with Hypovitaminosis D After Stroke

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
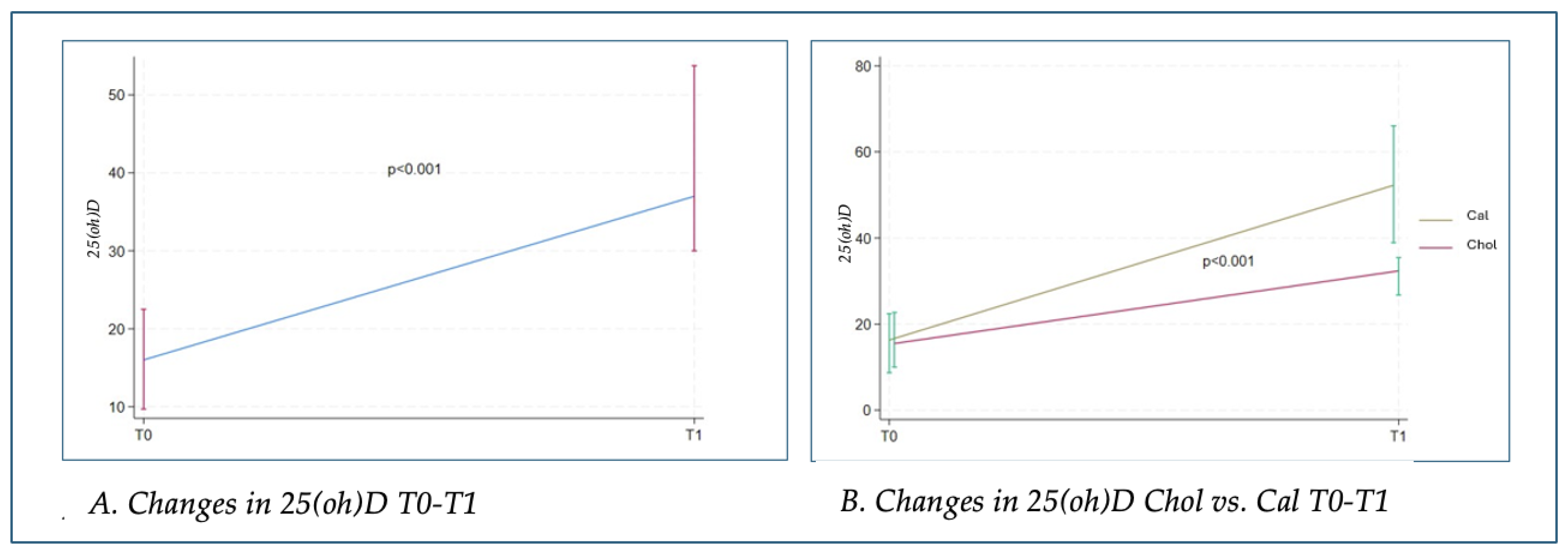
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liao, J.; Chen, J.; Wu, H.; Zhu, Q.; Tang, X.; Li, L.; Zhang, A.; Mo, P.; Liu, Y.; Yang, X.; et al. Combined 25-hydroxyvitamin D concentrations and physical activity on mortality in US stroke survivors: Findings from the NHANES. Nutr. J. 2025, 24, 5. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stöcklin, E.; Sidelnikov, E.; Willett, W.C.; Edel, J.O.; Stähelin, H.B.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3 versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Marek, K.; Cichoń, N.; Saluk-Bijak, J.; Bijak, M.; Miller, E. The Role of Vitamin D in Stroke Prevention and the Effects of Its Supplementation for Post-Stroke Rehabilitation: A Narrative Review. Nutrients 2022, 14, 2761. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Annweiler, C.; Brugg, B.; Peyrin, J.M.; Bartha, R.; Beauchet, O. Combination of memantine and vitamin D prevents axon degeneration induced by amyloid-beta and glutamate. Neurobiol. Aging 2014, 35, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Michos, E.D.; Post, W.; Astor, B. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch. Intern. Med. 2008, 168, 1629–1637. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- DeLuca, G.C.; Kimball, S.M.; Kolasinski, J.; Ramagopalan, S.V.; Ebers, G.C. Review: The role of vitamin D in nervous system health and disease. Neuropathol. Appl. Neurobiol. 2013, 39, 458–484. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Yamashita, T.; Sasaki, N.; Nakajima, K.; Kita, T.; Shinohara, M.; Ishida, T.; Hirata, K. Oral administration of an active form of vitamin D3 (calcitriol) decreases atherosclerosis in mice by inducing regulatory T cells and immature dendritic cells with tolerogenic functions. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2495–2503. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.S.; Man, R.Y.; Vanhoutte, P.M. Calcium-independent phospholipase A(2) plays a key role in the endothelium-dependent contractions to acetylcholine in the aorta of the spontaneously hypertensive rat. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H1260–H1266. [Google Scholar] [CrossRef] [PubMed]
- Balden, R.; Selvamani, A.; Sohrabji, F. Vitamin D deficiency exacerbates experimental stroke injury and dysregulates ischemia-induced inflammation in adult rats. Endocrinology 2012, 153, 2420–2435. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, Y.; Ji, H.; Tong, Y.; Zhang, Z.B. Prognostic value of serum 25-hydroxyvitamin D in patients with stroke. Neurochem. Res. 2014, 39, 1332–1337. [Google Scholar] [CrossRef] [PubMed]
- Turetsky, A.; Goddeau, R.P., Jr.; Henninger, N. Low Serum Vitamin D Is Independently Associated with Larger Lesion Volumes after Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Cichon, N.; Saluk-Bijak, J.; Miller, E.; Gorniak, L.; Redlicka, J.; Niwald, M.; Bijak, M. The Role of Supplementation with Natural Compounds in Post-Stroke Patients. Int. J. Mol. Sci. 2021, 22, 7893. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, H.; Zheng, T.; Wang, S.; Wei, L.; Wang, Q.; Sun, Z. Serum 25-hydroxyvitamin D predicts early recurrent stroke in ischemic stroke patients. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Zhou, H.; Wang, S.; Cheng, L.; Fang, Y. Low Serum Levels of 25-Hydroxyvitamin D Are Associated with Stroke Recurrence and Poor Functional Outcomes in Patients with Ischemic Stroke. J. Nutr. Health Aging 2017, 21, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Okoye, C.; Calsolaro, V.; Niccolai, F.; Calabrese, A.M.; Franchi, R.; Rogani, S.; Coppini, G.; Morelli, V.; Caraccio, N.; Monzani, F. A Randomized, Open-Label Study to Assess Efficacy of Weekly Assumption of Cholecalciferol versus Calcifediol in Older Patients with Hypovitaminosis, D. Geriatrics 2022, 7, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sosa Henríquez, M.; Gómez de Tejada Romero, M.J. Cholecalciferol or Calcifediol in the Management of Vitamin D Deficiency. Nutrients 2020, 12, 1617. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vieth, R. Vitamin D supplementation: Cholecalciferol, calcifediol, and calcitriol. Eur. J. Clin. Nutr. 2020, 74, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Castrillón, J.L.; Dueñas-Laita, A.; Brandi, M.L.; Jódar, E.; Del Pino-Montes, J.; Quesada-Gómez, J.M.; Cereto Castro, F.; Gómez-Alonso, C.; Gallego López, L.; Olmos Martínez, J.M.; et al. Calcifediol is superior to cholecalciferol in improving vitamin D status in postmenopausal women: A randomized trial. J. Bone Miner. Res. 2021, 36, 1967–1978. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mazzaferro, S.; Goldsmith, D.; Larsson, T.E.; Massy, Z.A.; Cozzolino, M. Vitamin D metabolites and/or analogs: Which D for which patient? Curr. Vasc. Pharmacol. 2014, 12, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, R.; Falchetti, A.; Attanasio, R.; Tabacco, G.; Naciu, A.M.; Palermo, A. Hypovitaminosis D: Is It Time to Consider the Use of Calcifediol? Nutrients 2019, 11, 1016. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sosa-Henríquez, M. Cholecalciferol and calcifediol for vitamin D supplementation. Osteoporos. Int. 2020, 31, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Davies, K.M.; Chen, T.C.; Holick, M.F.; Barger-Lux, M.J. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr. 2003, 77, 204–210, Erratum in Am. J. Clin. Nutr. 2003, 78, 1047. [Google Scholar] [CrossRef] [PubMed]
- Mazahery, H.; von Hurst, P.R. Factors Affecting 25-Hydroxyvitamin D Concentration in Response to Vitamin D Supplementation. Nutrients 2015, 7, 5111–5142. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giampà, E.; Di Bonito, M.; Ferretti, V.; Nuvoli, G.; Paoletti, F.; Piazzini, M.; Ranieri, M.; Tuveri, M.A.; Vinicola, V. Effects of alendronate and calcifediol compared to alendronate and cholecalciferol in osteoporotic patients. Minerva Endocrinol. 2019, 44, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Carda, S.; Cisari, C.; Invernizzi, M.; Bevilacqua, M. Osteoporosis after stroke: A review of the causes and potential treatments. Cerebrovasc. Dis. 2009, 28, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, L.; Crabtree, N.J.; Reeve, J.; Jacobsen, B.K. Ambulatory level and asymmetrical weight bearing after stroke affects bone loss in the upper and lower part of the femoral neck differently: Bone adaptation after decreased mechanical loading. Bone 2000, 27, 701–707, Erratum in Bone 2001, 28, 140. [Google Scholar] [CrossRef] [PubMed]
- Lazoura, O.; Groumas, N.; Antoniadou, E.; Papadaki, P.J.; Papadimitriou, A.; Thriskos, P.; Fezoulidis, I.; Vlychou, M. Bone mineral density alterations in upper and lower extremities 12 months after stroke measured by peripheral quantitative computed tomography and DXA. J. Clin. Densitom. 2008, 11, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Ramnemark, A.; Nyberg, L.; Lorentzon, R.; Olsson, T.; Gustafson, Y. Hemiosteoporosis after severe stroke, independent of changes in body composition and weight. Stroke 1999, 30, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Plantone, D.; Primiano, G.; Manco, C.; Locci, S.; Servidei, S.; De Stefano, N. Vitamin D in Neurological Diseases. Int. J. Mol. Sci. 2022, 24, 87. [Google Scholar] [CrossRef]
- Gezen-Ak, D.; Dursun, E. Vitamin D, a Secosteroid Hormone and Its Multifunctional Receptor, Vitamin D Receptor, in Alzheimer’s Type Neurodegeneration. J. Alzheimers Dis. 2023, 95, 1273–1299. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B. Follow-Up Period Affects the Association between Serum 25-Hydroxyvitamin D Concentration and Incidence of Dementia, Alzheimer’s Disease, and Cognitive Impairment. Nutrients 2024, 16, 3211. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grant, W.B.; Boucher, B.J. How Follow-Up Period in Prospective Cohort Studies Affects Relationship Between Baseline Serum 25(OH)D Concentration and Risk of Stroke and Major Cardiovascular Events. Nutrients 2024, 16, 3759. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alharbi, A.R.; Alali, A.S.; Samman, Y.; Alghamdi, N.A.; Albaradie, O.; Almaghrabi, M.; Makkawi, S.; Alghamdi, S.; Alzahrani, M.S.; Alsalmi, M.; et al. Vitamin D serum level predicts stroke clinical severity, functional independence, and disability-A retrospective cohort study. Front. Neurosci. 2022, 16, 951283. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Smolders, J.; van den Ouweland, J.; Geven, C.; Pickkers, P.; Kox, M. Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence. Metabolism 2021, 115, 154434. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Narasimhan, S.; Balasubramanian, P. Role of Vitamin D in the Outcome of Ischemic Stroke- A Randomized Controlled Trial. J. Clin. Diagn. Res. 2017, 11, CC06–CC10. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, A.; Prabhakar, S.; Modi, M.; Bhadada, S.K.; Kalaivani, M.; Lal, V.; Khurana, D. Effect of Vitamin D and calcium supplementation on ischaemic stroke outcome: A randomised controlled open-label trial. Int. J. Clin. Pract. 2016, 70, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Utkan Karasu, A.; Kaymak Karataş, G. Effect of vitamin D supplementation on lower extremity motor function and ambulation in stroke patients. Turk. J. Med. Sci. 2021, 51, 1413–1419. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Momosaki, R.; Abo, M.; Urashima, M. Vitamin D Supplementation and Post-Stroke Rehabilitation: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11, 1295. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Torrisi, M.; Bonanno, L.; Formica, C.; Arcadi, F.A.; Cardile, D.; Cimino, V.; Bramanti, P.; Morini, E. The role of rehabilitation and vitamin D supplementation on motor and psychological outcomes in poststroke patients. Medicine 2021, 100, e27747. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sari, A.; Durmus, B.; Karaman, C.A.; Ogut, E.; Aktas, I. A randomized, double-blind study to assess if vitamin D treatment affects the outcomes of rehabilitation and balance in hemiplegic patients. J. Phys. Ther. Sci. 2018, 30, 874–878. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clarke, R.; Shipley, M.; Lewington, S.; Youngman, L.; Collins, R.; Marmot, M.; Peto, R. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am. J. Epidemiol. 1999, 150, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Aghajafari, F.; Field, C.J.; Kaplan, B.J.; Rabi, D.M.; Maggiore, J.A.; O’Beirne, M.; Hanley, D.A.; Eliasziw, M.; Dewey, D.; Weinberg, A.; et al. APrON Study Team. The Current Recommended Vitamin D Intake Guideline for Diet and Supplements During Pregnancy Is Not Adequate to Achieve Vitamin D Sufficiency for Most Pregnant Women. PLoS ONE 2016, 11, e0157262. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
{kind=link}
| Calcifediol (N = 43) | Cholecalciferol (N = 42) | p-Value | |
|---|---|---|---|
| Age, median (IQR) | 67 (61; 76) | 66.5 (59; 73) | 0.46 |
| Female, N (%) | 19 (44%) | 15 (36%) | 0.45 |
| Ischemic stroke, N (%) | 34 (79%) | 33 (79%) | 0.96 |
| NIHSS T0, median (IQR) | 6 (3; 9) | 6 (3; 9) | 0.57 |
| BIM T0, median (IQR) | 40 (21; 81) | 41 (20; 65) | 0.61 |
| SPPB T0, median (IQR) | 0 (0; 7) |
3 (0; 6) (N = 41) | 0.57 |
| SF12PCS T0, median (IQR) |
35.9 (26.24; 42.05) (N = 42) |
34.64 (31.54; 42.9) (N = 41) | 0.59 |
| SF12MCS T0, median (IQR) |
46.12 (34.71; 53.1) (N = 42) |
46.5 (35.29; 56.92) (N = 41) | 0.56 |
| VAS, median (IQR) | 0 (0; 6) |
0 (0; 4) (N = 41) | 0.50 |
| 25(oh)D T0, median (IQR) | 16.3 (8.7; 22.4) | 15.5 (10; 22.7) | 0.93 |
| Calcium T0, median (IQR) | 9.3 (9.1; 9.5) | 9.45 (9.1; 9.8) | 0.10 |
| Phosphorus T0, median (IQR) |
3.3 (3; 3.7) (N = 42) | 3.2 (2.9; 3.6) | 0.42 |
| PTH T0, median (IQR) |
45.5 (29; 66) (N = 42) |
35.5 (27; 51) (N = 36) | 0.21 |
| T-SCORE SPINE T0, median (IQR) |
−1 (−2.1; 0.6) (N = 39) |
−0.1 (−1.6; 0.9) (N = 39) | 0.32 |
| T-SCORE NECK T0, median (IQR) |
−1.5 (−2.5; −0.8) (N = 39) |
−1.3 (−1.7; −0.8) (N = 40) | 0.46 |
| T-SCORE INTER T0, median (IQR) |
−1.1 (−1.9; 0.4) (N = 39) |
−0.75 (−1.3; 0.1) (N = 40) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canneva, S.; De Giovanni, A.; Pagella, F.; Pellegrino, L.; Iencinella, F.; Maestrini, S.; Ponzano, M.; Trompetto, C.; Mori, L. Efficacy of Oral Supplementation with Cholecalciferol Versus Calcifediol in Patients with Hypovitaminosis D After Stroke. Nutrients 2025, 17, 1035. https://doi.org/10.3390/nu17061035
Canneva S, De Giovanni A, Pagella F, Pellegrino L, Iencinella F, Maestrini S, Ponzano M, Trompetto C, Mori L. Efficacy of Oral Supplementation with Cholecalciferol Versus Calcifediol in Patients with Hypovitaminosis D After Stroke. Nutrients. 2025; 17(6):1035. https://doi.org/10.3390/nu17061035
Chicago/Turabian StyleCanneva, Stefania, Anna De Giovanni, Felicita Pagella, Lucia Pellegrino, Francesco Iencinella, Sara Maestrini, Marta Ponzano, Carlo Trompetto, and Laura Mori. 2025. "Efficacy of Oral Supplementation with Cholecalciferol Versus Calcifediol in Patients with Hypovitaminosis D After Stroke" Nutrients 17, no. 6: 1035. https://doi.org/10.3390/nu17061035
APA StyleCanneva, S., De Giovanni, A., Pagella, F., Pellegrino, L., Iencinella, F., Maestrini, S., Ponzano, M., Trompetto, C., & Mori, L. (2025). Efficacy of Oral Supplementation with Cholecalciferol Versus Calcifediol in Patients with Hypovitaminosis D After Stroke. Nutrients, 17(6), 1035. https://doi.org/10.3390/nu17061035