


Low Mediterranean Diet Adherence Is Associated with Poor Socioeconomic Status and Quality of Life: A Cross-Sectional Analysis



Highlights
- No statistically significant correlation was found between Mediterranean Diet adherence and overall HRQoL scores.
- Age negatively impacts HRQoL, while daily physical activity improves health outcomes.
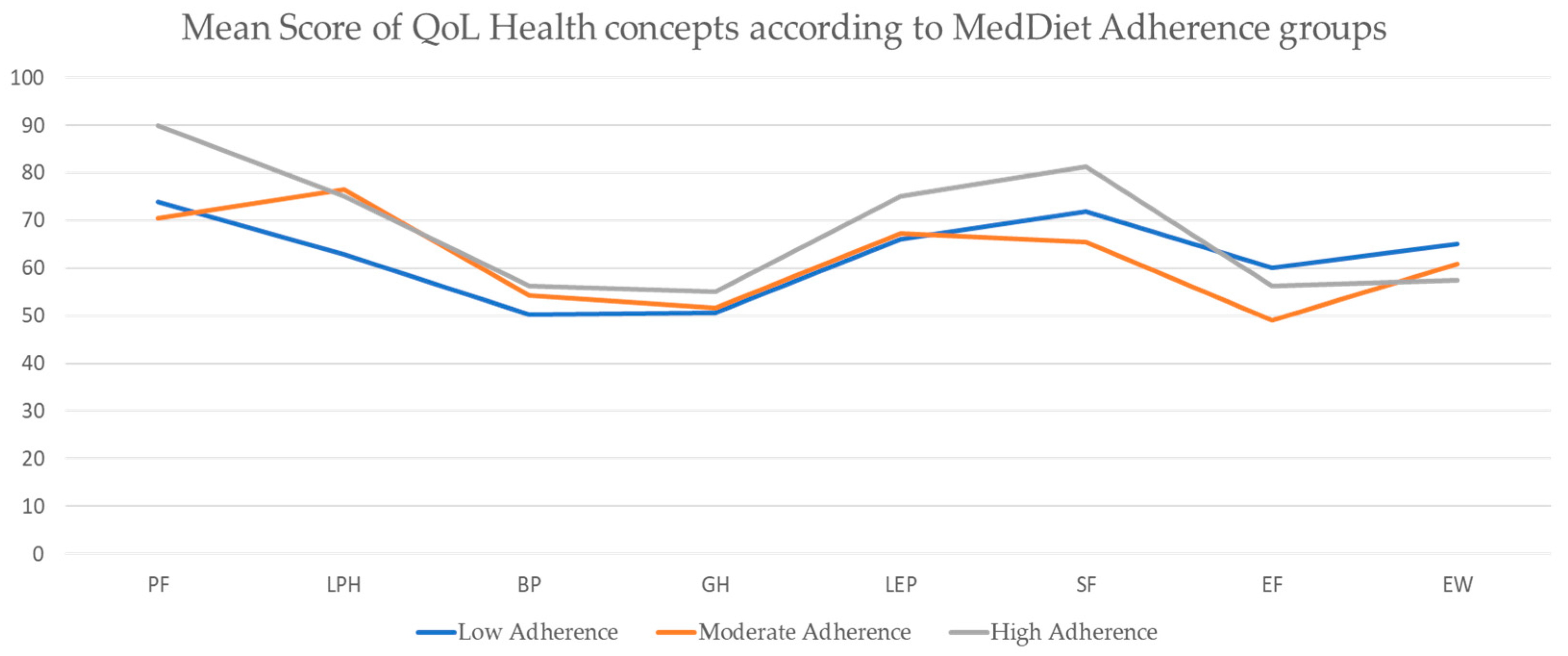
- SF-36 physical health concepts show a linear relationship with MedDiet adherence, while mental health concepts exhibit inconsistent patterns.
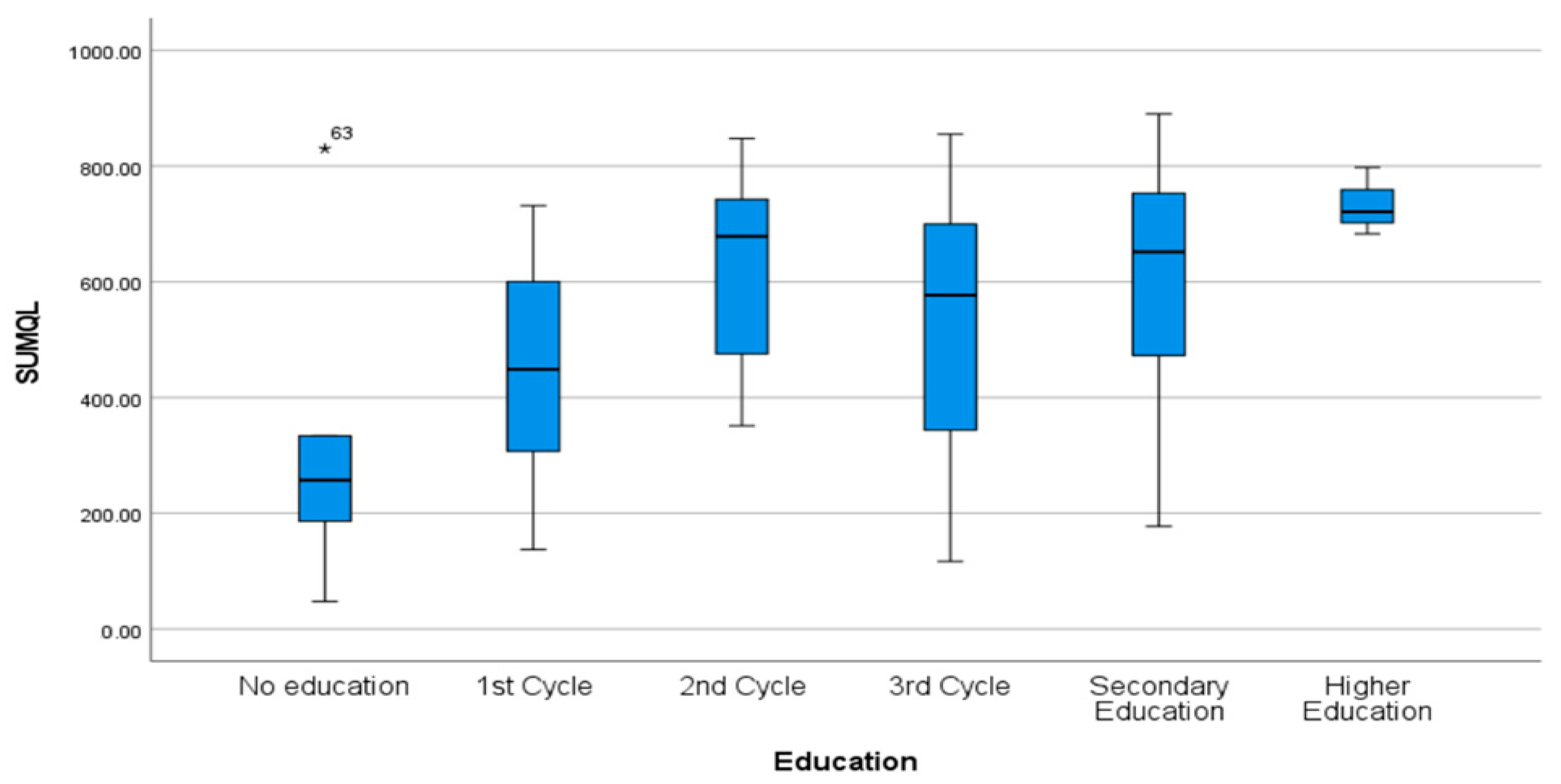
- Higher education is associated with better HRQoL, while a greater waist circumference negatively affects energy and vitality.
- The findings highlight the importance of factors beyond diet, such as physical activity, education, and body composition, in shaping HRQoL in disadvantaged communities.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Data Collection—Questionnaires (SF-36 and MEDAS)
2.2.1. MEDAS (Mediterranean Diet)
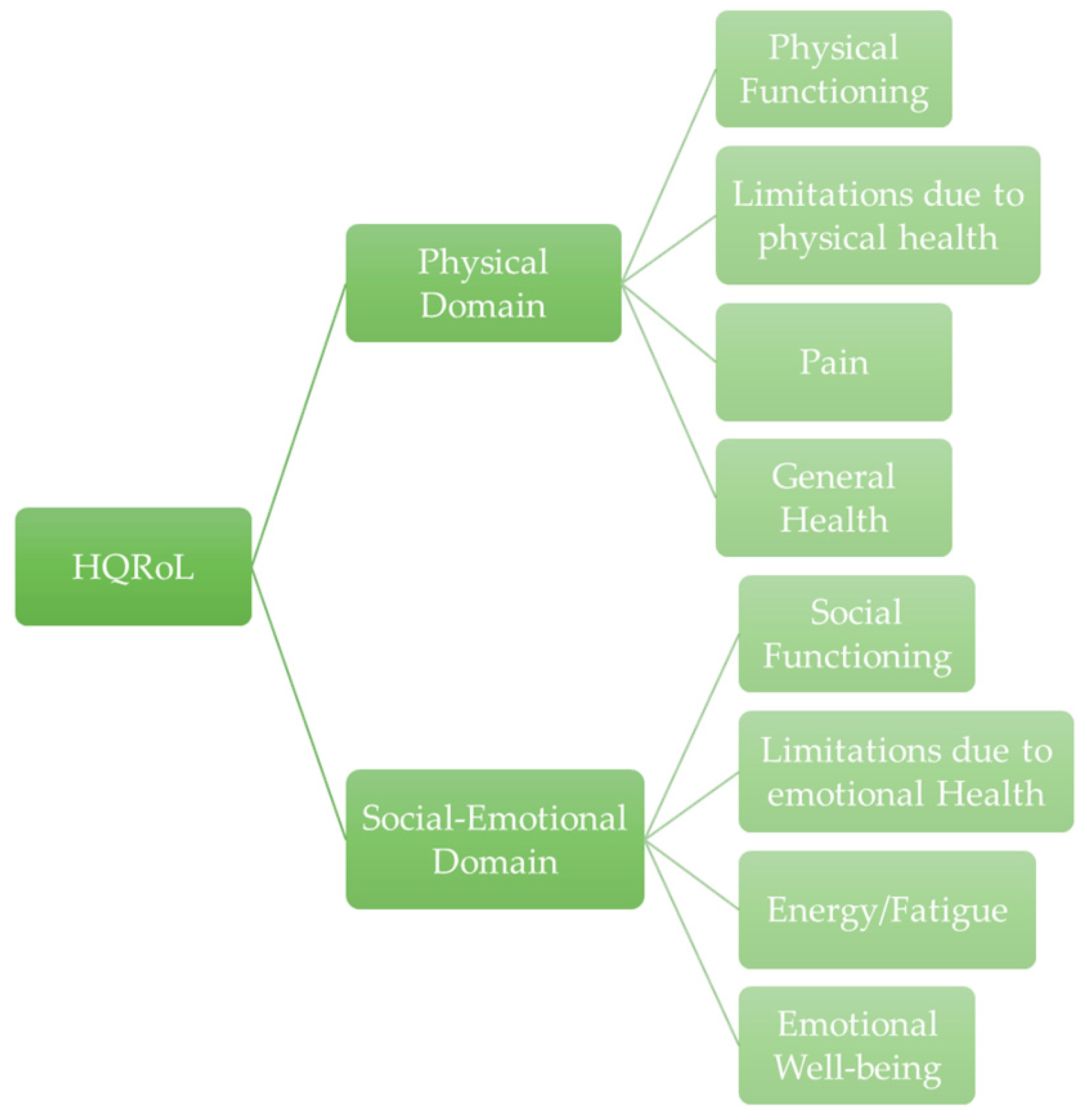
2.2.2. SF-36 (Health-Related Quality of Life)
2.3. Ethical Issues
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. Outcome Measures
3.2.1. MedDiet Adherence Groups
3.2.2. SF-36 Score Distribution Based on MedDiet Adherence Groups
3.3. Correlation Analysis Between the Variables of Interest
3.3.1. Relation Between Quality of Life and Mediterranean Diet Adherence
3.3.2. Relation Between Quality of Life and Baseline Characteristics
3.3.3. Relation Between Mediterranean Diet Adherence and Baseline Characteristics
3.3.4. Multivariable Logistic Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- A Saúde dos Portugueses 2016. Available online: http://www.dgs.pt (accessed on 12 July 2023).
- Velhinho, A.R.; Perelman, J. Socioeconomic Inequalities in Food Consumption: A Cross-Sectional Study in Portuguese Adults. Port. J. Public Health 2021, 39, 11–20. [Google Scholar]
- Bonaccio, M.; Donati, M.; Iacoviello, L.; de Gaetano, G. Socioeconomic Determinants of the Adherence to the Mediterranean Diet at a Time of Economic Crisis: The Experience of the MOLI-SANI Study1. Agric. Agric. Sci. Procedia 2016, 8, 741–747. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Persichillo, M.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Decline of the Mediterranean diet at a time of economic crisis. Results from the Moli-sani study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Pribisalić, A.; Popović, R.; Salvatore, F.P.; Vatavuk, M.; Mašanović, M.; Hayward, C.; Polašek, O.; Kolčić, I. The role of socioeconomic status in adherence to the mediterranean diet and body mass index change: A follow-up study in the general population of southern croatia. Nutrients 2021, 13, 3802. [Google Scholar] [CrossRef] [PubMed]
- Nemitz, J. Increasing longevity and life satisfaction: Is there a catch to living longer? J. Popul. Econ. 2022, 35, 557–589. [Google Scholar] [CrossRef]
- Brown, G.C. Living too long. EMBO Rep. 2015, 16, 137–141. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 3191–3200. [Google Scholar] [CrossRef]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Missbach, B.; König, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Martín-Calvo, N. Mediterranean diet and life expectancy; beyond olive oil, fruits and vegetables HHS Public Access. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 401–407. [Google Scholar] [CrossRef]
- Estudo de Adesão ao Estudo de Adesão ao Padrão Alimentar Mediterrânico. Available online: www.dgs.pt (accessed on 28 June 2023).
- Mendonça, N.; Gregório, M.J.; Salvador, C.; Henriques, A.R.; Canhão, H.; Rodrigues, A.M. Low Adherence to the Mediterranean Diet Is Associated with Poor Socioeconomic Status and Younger Age: A Cross-Sectional Analysis of the EpiDoC Cohort. Nutrients 2022, 14, 1239. [Google Scholar] [CrossRef] [PubMed]
- Galilea-Zabalza, I.; Buil-Cosiales, P.; Salas-Salvadó, J.; Toledo, E.; Ortega-Azorín, C.; Díez-Espino, J.; Vázquez-Ruiz, Z.; Zomeño, M.D.; Vioque, J.; Martínez, J.A.; et al. Mediterranean diet and quality of life: Baseline cross-sectional analysis of the PREDIMED-PLUS trial. PLoS ONE 2018, 13, e0198974. [Google Scholar] [CrossRef]
- Mantzorou, M.; Mentzelou, M.; Vasios, G.K.; Kontogiorgis, C.; Antasouras, G.; Vadikolias, K.; Psara, E.; Vorvolakos, T.; Poulios, E.; Serdari, A.; et al. Mediterranean Diet Adherence Is Associated with Favorable Health-Related Quality of Life, Physical Activity, and Sleep Quality in a Community-Dwelling Greek Older Population. Antioxidants 2023, 12, 983. [Google Scholar] [CrossRef] [PubMed]
- Ruano-Rodríguez, C.; Serra-Majem, L.; Dubois, D. Assessing the impact of dietary habits on health-related quality of life requires contextual measurement tools. Front. Pharmacol. 2015, 6, 141256. [Google Scholar] [CrossRef] [PubMed]
- EU_SHAFE. (n.d.). Interreg Europe. Available online: https://projects2014-2020.interregeurope.eu/eushafe/ (accessed on 30 May 2023).
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2011; 39p. [Google Scholar]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Gregório, M.J.; Rodrigues, A.M.; Salvador, C.; Dias, S.S.; de Sousa, R.D.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Lopes, C.; Martínez-González, M.A.; et al. Validation of the Tele-phone-Administered Version of the Mediterranean Diet Adherence Screener (MEDAS) Questionnaire. Nutrients 2020, 12, 1511. [Google Scholar] [CrossRef]
- Stewart, A.; Sherbourne, C.D.; Ware, J.E.; Hays, R.D.; Wells, K.B.; Berry, S.H.; Kamberg, C.; Nelson, E.C.; Davies, A.R.; Rogers, W.H.; et al. Measuring Functioning and Well-Being: The Medical Outcomes Study Approach. 1992. Available online: https://www.rand.org/pubs/commercial_books/CB361.html (accessed on 14 July 2023).
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef]
- Ferreira, P.L. Criação da versão portuguesa do MOS SF-36. Parte I—Adaptação cultural e linguistica. Acta Med. Port. 2000, 13, 55–56. [Google Scholar]
- RAND. RAND Corporation Provides Objective Research Services and Public Policy Analysis. Available online: https://www.rand.org/ (accessed on 14 July 2023).
- IBM (n.d.). IBM SPSS Statistics. Available online: https://www.ibm.com/products/spss-statistics (accessed on 12 July 2023).
- Ministério da Saúde Direção-Geral da Saúde; João Gregório, M.; Irving, S.; Teixeira, D.; Mendes de Sousa, S.; Ferreira, B. FICHA TÉCNICApt AUTORIA Programa Nacional para a Promoção da Alimentação Saudável. Available online: https://alimentacaosaudavel.dgs.pt (accessed on 12 July 2023).
- Bonaccio, M.; Bes-Rastrollo, M.; de Gaetano, G.; Iacoviello, L. Challenges to the Mediterranean diet at a time of economic crisis. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 1057–1063. [Google Scholar] [CrossRef]
- Rizal, H.; Said, M.A.; Majid, H.A.; Su, T.T.; Pin, T.M.; Ismail, R.; Shah Zaidi, M.A. Health-related quality of life of younger and older low-er-income households in Malaysia. PLoS ONE 2022, 17, e0263751. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Tasigchana, R.F.; León-Muñoz, L.M.; López-García, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Mediterranean diet and health-related quality of life in two cohorts of community-dwelling older adults. PLoS ONE 2016, 11, e0151596. [Google Scholar]
- Maug39eri, A.; Barchitta, M.; Fiore, V.; Rosta, G.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Agodi, A. Determinants of adherence to the mediterranean diet: Findings from a cross-sectional study in women from Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 2963. [Google Scholar] [CrossRef] [PubMed]
- Vitolo, M.R. Avaliação nutricional do adulto. In Nutrição: Da Gestação ao Envelhecimento; Rubio: Rio de Janeiro, Brazil, 2015; pp. 339–354. [Google Scholar]
- Departamento da Qualidade na Saúde. Avaliação Antropométrica no Adulto. DGS Orientação no 017/2013 de 05/12/2013. 2013. Available online: https://www.dgs.pt/directrizes-da-dgs/orientacoes-e-circulares-informativas/orientacao-n-0172013-de-05122013-pdf.aspx (accessed on 8 May 2023).
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Luchini, C.; Maggi, S. Adherence to the Mediterranean diet is associated with better quality of life: Data from the Osteoarthritis Initiative. Am. J. Clin. Nutr. 2016, 104, 1403–1409. [Google Scholar] [CrossRef]
- Vajdi, M.; Farhangi, M.A. A systematic review of the association between dietary patterns and health-related quality of life. Health Qual. Life Outcomes 2020, 18, 337. [Google Scholar] [CrossRef]
- Sanchez-Aguadero, N.; Alonso-Dominguez, R.; Garcia-Ortiz, L.; Agudo-Conde, C.; Rodriguez-Martin, C.; de Cabo-Laso, A.; Sanchez-Salgado, B.; Ramos, R.; Maderuelo-Fernandez, J.A.; Gomez-Marcos, M.A.; et al. Diet and physical activity in people with intermediate cardiovascular risk and their relationship with the health-related quality of life: Results from the MARK study. Health Qual. Life Outcomes 2016, 14, 169. [Google Scholar] [CrossRef]
- Fard, N.R.P.; Amirabdollahian, F.; Haghighatdoost, F. Dietary patterns and frailty: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 498–513. [Google Scholar] [CrossRef]
- Mlinac, M.E.; Feng, M.C. Assessment of Activities of Daily Living, Self-Care, and Independence. Arch. Clin. Neuropsychol. 2016, 31, 506–516. [Google Scholar] [CrossRef]
- Turrell, G.; Hewitt, B.; Patterson, C.; Oldenburg, B.; Gould, T. Socioeconomic differences in food purchasing behaviour and suggested implications for diet-related health promotion. J. Hum. Nutr. Diet. 2002, 15, 355–364. [Google Scholar] [CrossRef]
- de Mestral, C.; Stringhini, S.; Marques-Vidal, P. Barriers to healthy eating in Switzerland: A nationwide study. Clin. Nutr. 2016, 35, 1490–1498. [Google Scholar] [CrossRef]
- Poínhos, R.; Franchini, B.; Afonso, C.; Correia, F.; Teixeira, V.H.; Moreira, P.; Durão, C.; Pinho, O.; Silva, D.; Lima Reis, J.P.; et al. Alimentação e Estilos de Vida da População Portuguesa: Metodologia e Resultados Preliminares. Aliment. Humana 2009, 15, 43–60. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Adherence | Moderate Adherence | High Adherence | |
|---|---|---|---|
| N * | 87 | 13 | 2 |
| MedDiet score, mean (SD) | 6.44 (1.33) | 9.38 (0.51) | 11 (0.0) |
| SF-36 score, mean (SD) | 545.99 (202) | 541.25 (233.4) | 608.75 (243.95) |
| Age (years), median (IQR) | 55 (19) | 59 (30) | 49 (0) |
| Female gender, n (%) | 59 (67.8%) | 9 (69%) | 2 (100%) |
| Marital status, n (%) | |||
| Single | 34 (39%) | 7 (53.8%) | 0 |
| Married | 22 (25.3%) | 3 (23%) | 1 (50%) |
| Widowed/widower | 5 (5.7%) | 1 (7.7%) | 0 |
| Divorced | 26 (27.9%) | 2 (15.4%) | 1 (50%) |
| Level of education, n (%) | |||
| No education | 4 (4.6%) | 1 (7.7%) | 0 |
| 1st cycle | 20 (23.0%) | 3 (23%) | 0 |
| 2nd cycle | 28 (32.2%) | 2 (15.4%) | 1 (50%) |
| 3rd cycle | 21 (24.1%) | 3 (23%) | 0 |
| Secondary education | 12 (13.8%) | 3 (23%) | 1 (50%) |
| Higher education | 2 (2.3%) | 1 (7.7%) | 0 |
| Household, n (%) | |||
| Homeless | 8 (9.2%) | 0 | 0 |
| Rented | 73 (83.9%) | 12 (92.3%) | 2 (100%) |
| Own housing | 6 (6.9%) | 1 (7.7%) | 0 |
| Work situation, n (%) | |||
| Unemployed | 51 (58.6%) | 9 (69.2%) | 2 (100%) |
| Sick leave | 4 (4.6%) | 0 | 0 |
| Self-employed | 9 (10.3%) | 1 (7.7%) | 0 |
| Employee | 2 (2.3%) | 1 (7.7%) | 0 |
| Retired | 21 (24.1%) | 2 (15.4%) | 0 |
| Tobacco consumption, n (%) | |||
| Non-smoker | 61 (70.1%) | 8 (61.5%) | 2 (100%) |
| Smoker | 26 (29.9%) | 5 (38.5%) | 0 |
| Physical activity, n (%) | |||
| None | 49 (56.3%) | 5 (38.5%) | 0 |
| <30 min per day | 10 (11.5%) | 0 | 0 |
| ≥30 min per day | 28 (32.2%) | 8 (61.5%) | 2 (100%) |
| Alcohol consumption, n (%) | |||
| <2 drinks per day | 86 (98.9%) | 11 (84.6%) | 2 (100%) |
| 2–4 drinks per day | 0 | 2 (15.4%) | 0 |
| ≥5 drinks per day | 1 (1.1%) | 0 | 0 |
| Do you consider that you have a healthy diet? n (%) | |||
| No | 20 (23.0%) | 0 | 0 |
| Yes | 50 (57.5%) | 11 (84.6%) | 2 (100%) |
| Maybe | 17 (19.5%) | 2 (15.4%) | 0 |
| Body weight **, median (IQR) | 80.95 (27.6) | 66.85 (10.9) | 72.25 (-) |
| BMI **, median (IQR) | 30.14 (9.45) | 25.9 (6.4) | 29.45 (-) |
| Arm circumference (cm) **, median (IQR) | 34.25 (5.7) | 32 (4.4) | 32 (-) |
| Waist circumference (cm) **, median (IQR) | 97.2 (14.9) | 91.85 (15.1) | 92.75 (-) |
| Hip circumference (cm) **, median (IQR) | 105 (16) | 100.45 (15.4) | 109.7 (-) |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | |||
| SUMPD | 0.000 | 0.002 | 0.020 | 0.145 | 0.885 | −0.004 | 0.005 |
| SUMSED | −0.001 | 0.002 | −0.076 | −0.566 | 0.573 | −0.006 | 0.003 |
| Spearman Correlation | |||||
|---|---|---|---|---|---|
| Variables | MedDiet Adherence Score (MEDAS) | Total Score (SF-36) | Social–Emotional Domain (SF-36) | Energy/Fatigue, Median (IQR) | Physical Domain (SF-36) |
| MedDiet Adherence | 1 | 0.21 (0.832) | −0.06 (0.547) | −0.126 (0.205) | 0.08 (0.444) |
| Health concepts | |||||
| Energy/fatigue, median (IQR) | −0.13 (0.205) | 0.78 (<0.001) | 0.80 (<0.001) ** | 1 | 0.62 (<0.001) ** |
| Participant characteristics | |||||
| Physical activity | 0.22 (0.029) * | 0.361 (<0.01) | 0.28 (<0.01) ** | 0.26 (<0.01) ** | 0.345 (<0.01) ** |
| Healthy diet | 0.095 (0.34) | 0.189 (0.057) | 0.177 (0.075) | 0.210 (0.034) * | 0.197 (0.047) * |
| Alcohol consumption | 0.25 (0.01) | 0.13 (0.198) | 0.15 (0.128) | 0.09(0.39) | 0.1 (0.294) |
| Education | 0.1 (0.34) | 0.28 (<0.01) | 0.216 (0.03) * | 0.19(0.05) * | 0.28 (<0.01) |
| Body weight | −0.25 (0.057) | −0.12 (0.4) | −0.14 (0.29) | −0.25(0.05) * | −0.07 (0.5) |
| Body circumferences | |||||
| Waist circumference (cm) | −0.22 (0.09) | −0.15 (0.25) | −0.19 (0.2) | −0.3 (0.02) * | −0.08 (0.83) |
| Hip circumference (cm) | −0.07 (0.59) | −0.14 (0.29) | −0.23 (0.08) | −0.31 (0.02) * | −0.03 (0.82) |
| Arm circumference (cm) ** | −0.22 (0.07) | −0.16 (0.2) | −0.19 (0.15) | −0.3 (0.02) * | −0.11 (0.39) |
| Influencing Factors (Model) | Unstandardized B | SE | p-Value |
|---|---|---|---|
| Constant | 685.332 | 113.583 | <0.001 ** |
| Age | −0.308 | 1.753 | <0.001 ** |
| Gender | 72.541 | 40.047 | 0.073 |
| Education | 17.402 | 17.394 | 0.320 |
| Household | 54.668 | 49.669 | 0.274 |
| Marital status | 2.494 | 16.047 | 0.877 |
| Employment status | 17.206 | 12.120 | 0.159 |
| Physical activity | 123.701 | 39.263 | 0.002 ** |
| Smoking habits | −33.359 | 39.453 | 0.400 |
| Alcohol consumption | 25.187 | 79.073 | 0.751 |
| Healthy eating | 50.361 | 29.314 | 0.089 |
| MedDiet Score | −33.784 | 43.013 | 0.434 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, C.; Campos, A.; Pereira, T.; Lima, J.P.M. Low Mediterranean Diet Adherence Is Associated with Poor Socioeconomic Status and Quality of Life: A Cross-Sectional Analysis. Nutrients 2025, 17, 906. https://doi.org/10.3390/nu17050906
Duarte C, Campos A, Pereira T, Lima JPM. Low Mediterranean Diet Adherence Is Associated with Poor Socioeconomic Status and Quality of Life: A Cross-Sectional Analysis. Nutrients. 2025; 17(5):906. https://doi.org/10.3390/nu17050906
Chicago/Turabian StyleDuarte, Carolina, Andrea Campos, Telmo Pereira, and João P. M. Lima. 2025. "Low Mediterranean Diet Adherence Is Associated with Poor Socioeconomic Status and Quality of Life: A Cross-Sectional Analysis" Nutrients 17, no. 5: 906. https://doi.org/10.3390/nu17050906
APA StyleDuarte, C., Campos, A., Pereira, T., & Lima, J. P. M. (2025). Low Mediterranean Diet Adherence Is Associated with Poor Socioeconomic Status and Quality of Life: A Cross-Sectional Analysis. Nutrients, 17(5), 906. https://doi.org/10.3390/nu17050906