

A Narrative Review on Plant Extracts for Metabolic Syndrome: Efficacy, Safety, and Technological Advances
 , , , ,
, , , ,  , and
, and 
Highlights
- Plant extracts show promise in managing metabolic syndrome by improving metabolism, reducing inflamma-tion, and enhancing insulin sensitivity.
- Safety concerns, lack of standardized regulations, and drug interactions limit their clinical application.
- Advanced extraction and encapsulation techniques enhance stability, bioavailability, and therapeutic efficacy.
- Rigorous long-term trials are needed to confirm efficacy and safety.
Abstract
1. Introduction
2. Plant Extracts as Functional Food Ingredients
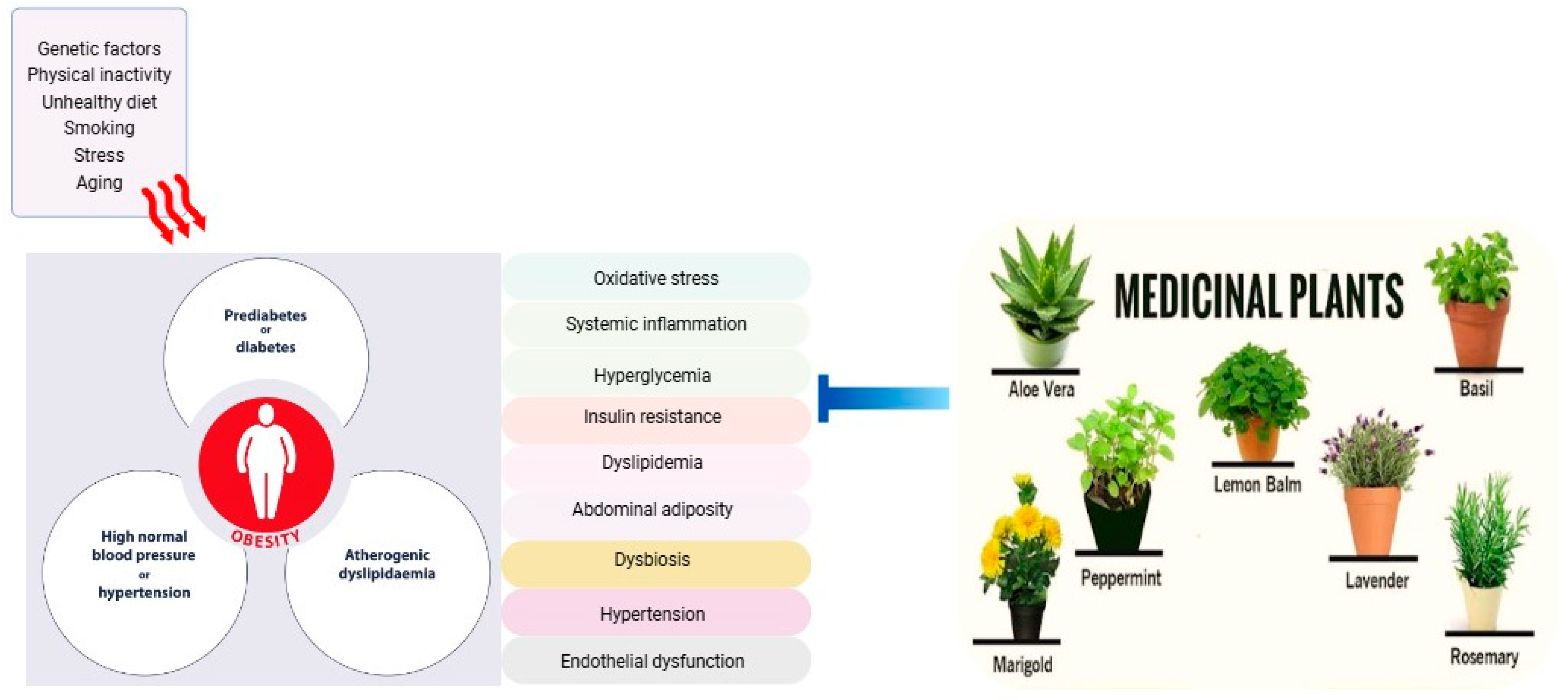
2.1. Obesity and Hyperglycemia
2.2. Dyslipidemia
2.3. Hypertension, Endothelial Dysfunction, and Pro-Inflammatory State
3. Safety Concerns
4. Technological Aspects
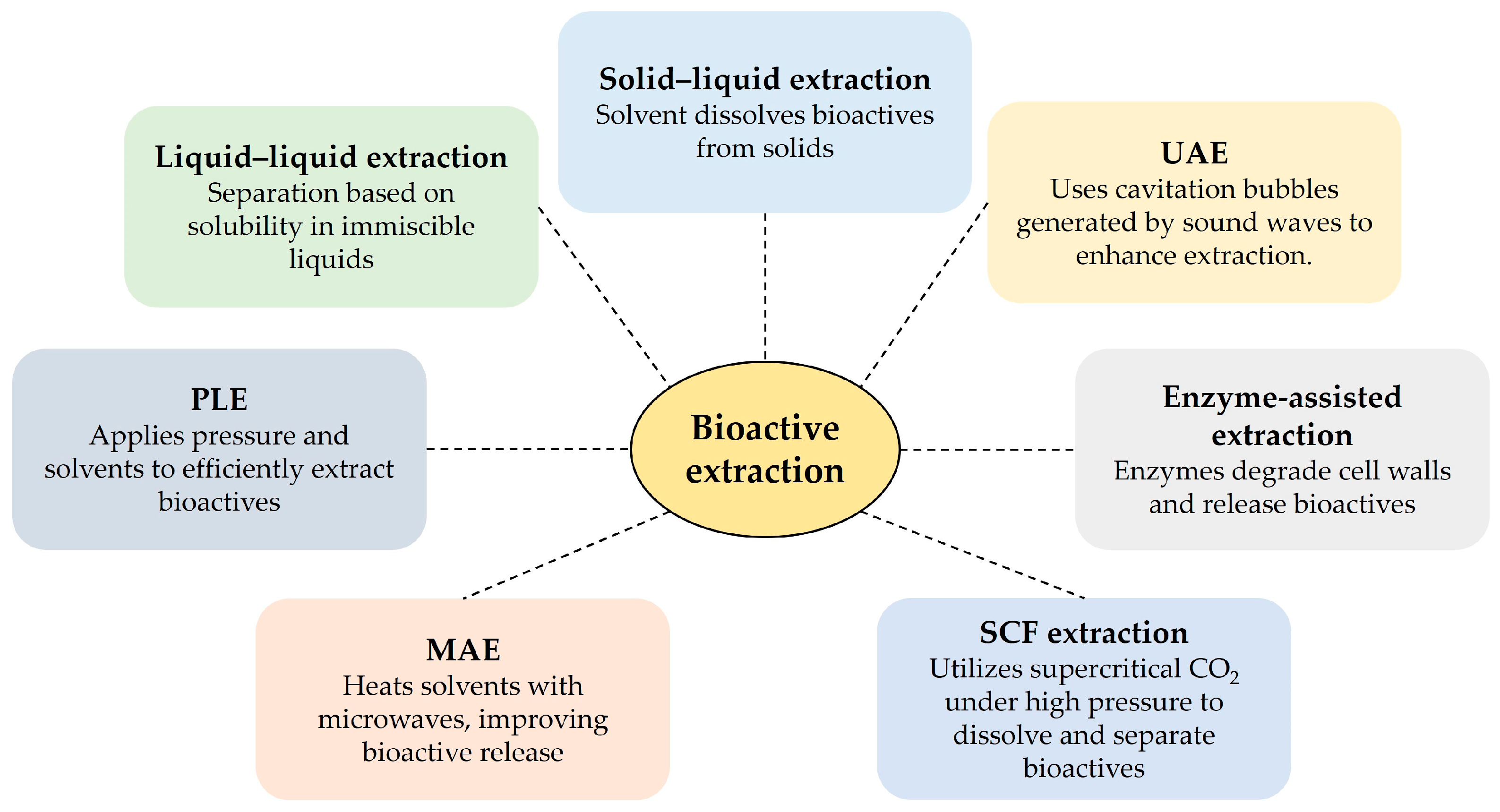
4.1. Extraction Techniques
4.2. Encapsulation and Delivery Systems
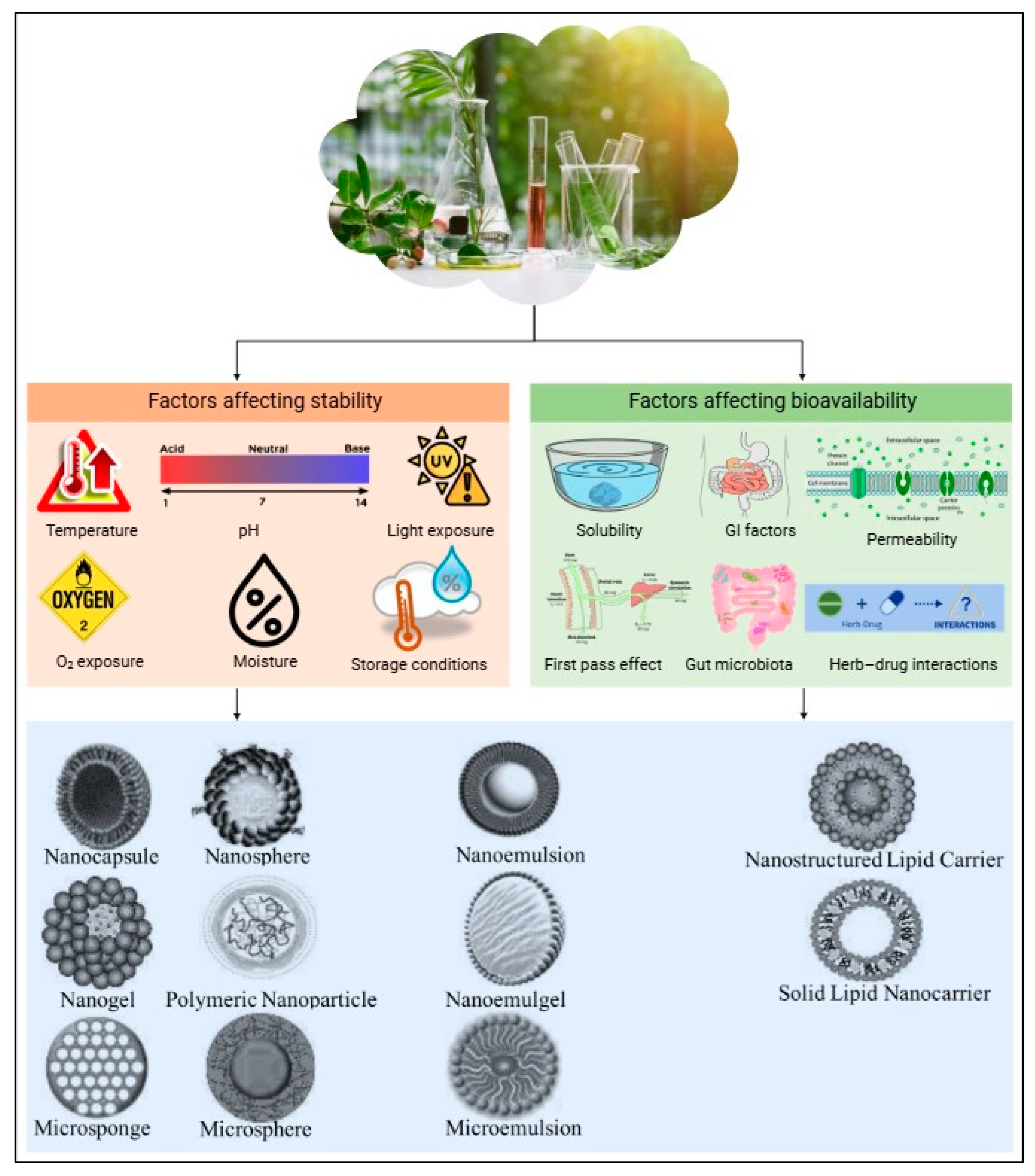
4.3. Stabilization and Shelf-Life Improvement
4.4. Formulation into Functional Foods, Scalability, and Industrial Applications
5. Conclusions
- Limited clinical translation: The majority of studies are based on in vitro and animal models, which may not fully reflect clinical effects in human populations.
- Variability in bioactive composition: The composition and concentration of bioactive compounds in plant extracts can vary due to multiple factors, including plant sources, environmental conditions, and extraction methods. This variability complicates the establishment of consistent efficacy and safety profiles.
- Confounding variables in study design: Many studies do not adequately control for lifestyle factors such as diet and physical activity. Consequently, observed effects may be influenced by external variables rather than the plant extracts alone.
- Short study durations and small sample sizes: Clinical trials investigating the effects of plant extracts on metabolic syndrome often have limited durations, small sample populations, and insufficient long-term follow-up, restricting the generalizability of findings and their broader clinical application. Large-scale, long-term, randomized controlled trials are essential to establish both efficacy and safety for widespread use.
- Underrepresentation of pediatric and adolescent populations: While metabolic syndrome is predominantly associated with adults and older individuals, its prevalence is increasing among children and adolescents. However, research on the potential benefits of plant extracts in these younger populations remains limited.
- Lack of direct comparisons with conventional therapies: Most clinical studies utilize placebo-controlled designs, with relatively few directly comparing plant extracts to conventional pharmaceutical treatments. Future research should emphasize comparative studies to draw more definitive conclusions regarding the therapeutic potential of plant extracts relative to standard medical interventions.
- Limited investigation into bioavailability: Bioavailability is a crucial determinant of the physiological effects of both pharmacological drugs and plant extracts. However, in contrast to pharmaceutical compounds, the bioavailability of plant-derived extracts in human subjects remains largely unexplored.
- Regulatory and interaction challenges: The absence of standardized regulatory frameworks and the potential for interactions between plant extracts and pharmaceutical drugs present additional challenges that must be addressed to ensure safe and effective use.
- Stability and commercial viability: While the stability and shelf-life of plant extracts have been extensively studied, their evaluation within commercially available products is limited. Further research is needed to optimize formulations for real-world applications.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ADRs | adverse drug reactions |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CHD | coronary heart disease |
| DSHEA | Dietary Supplement Health and Education Act |
| EMA | European Medicines Agency |
| FDA | Food and Drug Administration |
| HbA1c | glycated hemoglobin |
| HDL | high-density lipoprotein |
| HPLC | high-performance liquid chromatography |
| hs-CRP | high sensitivity C-reactive protein |
| IDF | International Diabetes Federation |
| LDL | low-density lipoprotein |
| MAE | microwave-assisted extraction |
| NCEP ATP III | National Cholesterol Education Program’s Adult Treatment Panel III |
| NO-cGMP | nitric oxide–cyclic guanosine monophosphate pathway |
| NO-sGC-cGMP | nitric oxide–soluble guanylate cyclase–cyclic guanosine monophosphate pathway |
| PLE | pressurized liquid extraction |
| ROS | reactive oxygen species |
| SFE | supercritical fluid extraction |
| T2DM | type 2 diabetes mellitus |
| TC | total cholesterol |
| TGs | triglycerides |
| UAE | ultrasound-assisted extraction |
| VLDL | very-low-density lipoprotein |
| WHO | World Health Organization |
References
- Costa, L.A.; Canani, L.H.; Lisboa, H.R.K.; Tres, G.S.; Gross, J.L. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in Type 2 diabetes. Diabet. Med. 2004, 21, 252–255. [Google Scholar] [CrossRef] [PubMed]
- McCracken, E.; Monaghan, M.; Sreenivasan, S. Pathophysiology of the metabolic syndrome. Clin. Dermatol. 2018, 36, 14–20. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Expert Panel on Detection, E. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486. [Google Scholar]
- IDF. International Diabetes Federation: The IDF Consensus Worldwide Definition of the Metabolic Syndrome. 2005. Available online: https://idf.org/media/uploads/2023/05/attachments-30.pdf (accessed on 9 August 2024).
- Zhang, H.; Zhou, X.D.; Shapiro, M.D.; Lip, G.Y.; Tilg, H.; Valenti, L.; Somers, V.K.; Byrne, C.D.; Targher, G.; Yang, W.; et al. Global burden of metabolic diseases, 1990–2021. Metabolism 2024, 160, 155999. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Ndoadoumgue, A.L.; et al. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals. Diabetes Res. Clin. Pract. 2022, 188, 109924. [Google Scholar] [CrossRef] [PubMed]
- WHO. Obesity and Overweight. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 August 2024).
- WHO. Diabetes. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 9 August 2024).
- WHO. Hypertension. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 9 August 2024).
- Kaur, J. Assessment and screening of the risk factors in metabolic syndrome. Med. Sci. 2014, 2, 140–152. [Google Scholar] [CrossRef]
- Åberg, F.; Helenius-Hietala, J.; Puukka, P.; Färkkilä, M.; Jula, A. Interaction between alcohol consumption and metabolic syndrome in predicting severe liver disease in the general population. Hepatology 2018, 67, 2141–2149. [Google Scholar] [CrossRef]
- Mongraw-Chaffin, M.; Foster, M.C.; Anderson, C.A.; Burke, G.L.; Haq, N.; Kalyani, R.R.; Ouyang, P.; Sibley, C.T.; Tracy, R.; Woodward, M.; et al. Metabolically healthy obesity, transition to metabolic syndrome, and cardiovascular risk. J. Am. Coll. Cardiol. 2018, 71, 1857–1865. [Google Scholar] [CrossRef]
- Prasad, H.; Ryan, D.A.; Celzo, M.F.; Stapleton, D. Metabolic syndrome: Definition and therapeutic implications. Postgrad. Med. 2012, 124, 21–30. [Google Scholar] [CrossRef]
- Rask Larsen, J.; Dima, L.; Correll, C.U.; Manu, P. The pharmacological management of metabolic syndrome. Expert Rev. Clin. Pharmacol. 2018, 11, 397–410. [Google Scholar] [CrossRef]
- Matfin, G. Developing therapies for the metabolic syndrome: Challenges, opportunities, and… the unknown. Ther. Adv. Endocrinol. Metab. 2010, 1, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Behzad, M.; Negah, R.; Suveer, B.; Neda, R. A review of thiazolidinediones and metformin in the treatment of type 2 diabetes with focus on cardiovascular complications. Vasc. Health Risk Manag. 2007, 3, 967–973. [Google Scholar]
- Cheung, K.S.; Chan, E.W.; Wong, A.Y.; Chen, L.; Seto, W.K.; Wong, I.C.; Leung, W.K. Aspirin and risk of gastric cancer after Helicobacter pylori eradication: A territory-wide study. J. Natl. Cancer Inst. 2018, 110, 743–749. [Google Scholar] [CrossRef]
- Pasnoor, M.; Barohn, R.J.; Dimachkie, M.M. Toxic myopathies. Curr. Opin. Neurol. 2018, 31, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Weir, M.R.; Bakris, G.L.; Bushinsky, D.A.; Mayo, M.R.; Garza, D.; Stasiv, Y.; Wittes, J.; Christ-Schmidt, H.; Berman, L.; Pitt, B. Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors. N. Engl. J. Med. 2015, 372, 211–221. [Google Scholar] [CrossRef]
- Guo, Z. The modification of natural products for medical use. Acta Pharm. Sin. B 2017, 7, 119–136. [Google Scholar] [CrossRef]
- Williamson, E.M.; Liu, X.; Izzo, A.A. Trends in use, pharmacology, and clinical applications of emerging herbal nutraceuticals. Br. J. Pharmacol. 2020, 177, 1227–1240. [Google Scholar] [CrossRef]
- Ekor, M. The growing use of herbal medicines: Issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Jang, B.H.; Ko, Y.; Sasaki, Y.; Park, J.S.; Hwang, E.H.; Song, Y.K.; Shin, Y.C.; Ko, S.G. Herbal medicines for treating metabolic syndrome: A systematic review of randomized controlled trials. Evid. Based Complement. Alternat. Med. 2016, 2016, 5936402. [Google Scholar] [CrossRef]
- Ullah, H.; De Filippis, A.; Khan, H.; Xiao, J.; Daglia, M. An overview of the health benefits of Prunus species with special reference to metabolic syndrome risk factors. Food Chem. Toxicol. 2020, 144, 111574. [Google Scholar] [CrossRef] [PubMed]
- Ullah, H.; Daglia, M. Phytonutrients in the management of glucose metabolism. In The Role of Phytonutrients in Metabolic Disorders; Khan, H., Akkol, E., Daglia, M., Eds.; Academic Press: Cambridge, UK, 2022; pp. 163–193. [Google Scholar]
- Ullah, H.; De Filippis, A.; Santarcangelo, C.; Daglia, M. Epigenetic regulation by polyphenols in diabetes and related complications. Med. J. Nutrition. Metab. 2020, 13, 289–310. [Google Scholar] [CrossRef]
- Sam, S.; Mazzone, T. Adipose tissue changes in obesity and the impact on metabolic function. Transl. Res. 2014, 164, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M.; Paschke, R. Visceral adipose tissue and metabolic syndrome. Dtsch. Med. Wochenschr. 2003, 128, 2319–2323. [Google Scholar]
- Lotfy, M.; Adeghate, J.; Kalasz, H.; Singh, J.; Adeghate, E. Chronic complications of diabetes mellitus: A mini review. Curr. Diabetes Rev. 2017, 13, 3–10. [Google Scholar] [CrossRef]
- Gandhi, J.; Dagur, G.; Warren, K.; Smith, N.L.; Khan, S.A. Genitourinary complications of diabetes mellitus: An overview of pathogenesis, evaluation, and management. Curr. Diabetes Rev. 2017, 13, 498–518. [Google Scholar] [CrossRef]
- Ozougwu, J.; Obimba, K.; Belonwu, C.; Unakalamba, C. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J. Physiol. Pathophysiol. 2013, 4, 46–57. [Google Scholar] [CrossRef]
- Ullah, H.; Sommella, E.; Santarcangelo, C.; D’Avino, D.; Rossi, A.; Dacrema, M.; Minno, A.D.; Di Matteo, G.; Mannina, L.; Campiglia, P.; et al. Hydroethanolic extract of Prunus domestica L.: Metabolite profiling and in vitro modulation of molecular mechanisms associated to cardiometabolic diseases. Nutrients 2022, 14, 340. [Google Scholar] [CrossRef]
- Song, J.; Kim, Y.S.; Kim, L.; Park, H.J.; Lee, D.; Kim, H. Anti-obesity effects of the flower of Prunus persica in high-fat diet-induced obese mice. Nutrients 2019, 11, 2176. [Google Scholar] [CrossRef] [PubMed]
- Belwal, T.; Bisht, A.; Devkota, H.P.; Ullah, H.; Khan, H.; Pandey, A.; Bhatt, I.D.; Echeverría, J. Phytopharmacology and clinical updates of Berberis species against diabetes and other metabolic diseases. Front. Pharmacol. 2020, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Pan, Y.; Xu, L.; Tang, D.; Dorfman, R.G.; Zhou, Q.; Yin, Y.; Li, Y.; Zhou, L.; Zhao, S.; et al. Berberine promotes glucose uptake and inhibits gluconeogenesis by inhibiting deacetylase SIRT3. Endocrine 2018, 62, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, Y.; Huang, C. Berberine inhibits PTP1B activity and mimics insulin action. Biochem. Biophys. Res. Commun. 2010, 397, 543–547. [Google Scholar] [CrossRef]
- Ko, B.-S.; Choi, S.B.; Park, S.K.; Jang, J.S.; Kim, Y.E.; Park, S. Insulin sensitizing and insulinotropic action of berberine from Cortidis rhizoma. Biol. Pharm. Bull. 2005, 28, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Xia, M.; Yan, H.; Han, Y.; Zhang, F.; Hu, Z.; Cui, A.; Ma, F.; Liu, Z.; Gong, Q.; et al. Berberine attenuates hepatic steatosis and enhances energy expenditure in mice by inducing autophagy and fibroblast growth factor 21. Br. J. Pharmacol. 2018, 175, 374–387. [Google Scholar] [CrossRef] [PubMed]
- Asekenye, C.; Alele, P.E.; Ogwang, P.E.; Olet, E.A. Hypoglycemic effect of leafy vegetables from Ankole and Teso sub-regions of Uganda: Preclinical evaluation using a high fat diet-streptozotocin model. Res. Sq. 2024. online ahead of print. [Google Scholar] [CrossRef]
- Tucakovic, L.; Colson, N.; Santhakumar, A.B.; Kundur, A.R.; Shuttleworth, M.; Singh, I. The effects of anthocyanins on body weight and expression of adipocyte’s hormones: Leptin and adiponectin. J. Funct. Foods 2018, 45, 173–180. [Google Scholar] [CrossRef]
- Ullah, H.; Esposito, C.; Piccinocchi, R.; De Lellis, L.F.; Santarcangelo, C.; Minno, A.D.; Baldi, A.; Buccato, D.G.; Khan, A.; Piccinocchi, G.; et al. Postprandial glycemic and insulinemic response by a Brewer’s spent grain extract-based food supplement in subjects with slightly impaired glucose tolerance: A monocentric, randomized, cross-over, double-blind, placebo-controlled clinical trial. Nutrients 2022, 14, 3916. [Google Scholar] [CrossRef]
- Perez-Martinez, P.; Garcia-Rios, A.; Delgado-Lista, J.; Perez-Jimenez, F.; Lopez-Miranda, J. Mediterranean diet rich in olive oil and obesity, metabolic syndrome and diabetes mellitus. Curr. Pharm. Des. 2011, 17, 769–777. [Google Scholar] [CrossRef]
- Soriguer, F.; Rojo-Martínez, G.; de Fonseca, F.R.; García-Escobar, E.; García Fuentes, E.; Olveira, G. Obesity and the metabolic syndrome in Mediterranean countries: A hypothesis related to olive oil. Mol. Nutr. Food Res. 2007, 51, 1260–1267. [Google Scholar] [CrossRef]
- Bozzetto, L.; Alderisio, A.; Giorgini, M.; Barone, F.; Giacco, A.; Riccardi, G.; Rivellese, A.A.; Annuzzi, G. Extra-virgin olive oil reduces glycemic response to a high–glycemic index meal in patients with type 1 diabetes: A randomized controlled trial. Diabetes Care 2016, 39, 518–524. [Google Scholar] [CrossRef]
- Al Jamal, A.R.; Ibrahim, A. Effects of olive oil on lipid profiles and blood glucose in type2 diabetic patients. Int. J. Diabetes Metab. 2011, 19, 19–22. [Google Scholar] [CrossRef]
- Wainstein, J.; Ganz, T.; Boaz, M.; Bar Dayan, Y.; Dolev, E.; Kerem, Z.; Madar, Z. Olive leaf extract as a hypoglycemic agent in both human diabetic subjects and in rats. J. Med. Food 2012, 15, 605–610. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, R.; Lal, B. Effect of Trigonella foenum-graecum (fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes mellitus: A double blind placebo controlled study. J. Assoc. Physicians India 2001, 49, 1057–1061. [Google Scholar]
- Sharma, R.D.; Raghuram, T.C. Hypoglycaemic effect of fenugreek seeds in non-insulin dependent diabetic subjects. Nutr. Res. 1990, 10, 731–739. [Google Scholar] [CrossRef]
- Madar, Z.; Abel, R.; Samish, S.; Arad, J. Glucose-lowering effect of fenugreek in non-insulin dependent diabetics. Eur. J. Clin. Nutr. 1988, 42, 51–54. [Google Scholar] [PubMed]
- Fukino, Y.; Ikeda, A.; Maruyama, K.; Aoki, N.; Okubo, T.; Iso, H. Randomized controlled trial for an effect of green tea-extract powder supplementation on glucose abnormalities. Eur. J. Clin. Nutr. 2008, 62, 953–960. [Google Scholar] [CrossRef]
- Venables, M.C.; Hulston, C.J.; Cox, H.R.; Jeukendrup, A.E. Green tea extract ingestion, fat oxidation, and glucose tolerance in healthy humans. Am. J. Clin. Nutr. 2008, 87, 778–784. [Google Scholar] [CrossRef]
- Brown, A.L.; Lane, J.; Coverly, J.; Stocks, J.; Jackson, S.; Stephen, A.; Bluck, L.; Coward, A.; Hendrickx, H. Effects of dietary supplementation with the green tea polyphenol epigallocatechin-3-gallate on insulin resistance and associated metabolic risk factors: Randomized controlled trial. Br. J. Nutr. 2009, 101, 886–894. [Google Scholar] [CrossRef]
- Wang, Y.J.; Zhu, W.F.; Wang, X.K. Study on the effect of Qinggan Jiangtang tablet in improving the insulin resistance in patients with multiple metabolic syndrome. Zhongguo Zhong Xi Yi Jie He Za Zhi 2005, 25, 412–415. [Google Scholar] [PubMed]
- Mohammad, A.; Shahnaz, T.; Sorayya, K. Effect of 8 weeks’ supplementation grape seed extract on insulin resistance in Iranian adolescents with metabolic syndrome: A randomized controlled trial. Diabetes Metab. Syndr. 2021, 15, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T. Pathophysiology of diabetic dyslipidemia. J. Atherosclerosis Thromb. 2018, 25, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-F.; Chang, Y.-H.; Chien, S.-C.; Lin, Y.-H.; Yeh, H.-Y. Epidemiology of dyslipidemia in the Asia pacific region. Int. J. Gerontol. 2018, 12, 2–6. [Google Scholar] [CrossRef]
- Mbikay, M. Therapeutic potential of Moringa oleifera leaves in chronic hyperglycemia and dyslipidemia: A review. Front. Pharmacol. 2012, 3, 24. [Google Scholar] [CrossRef] [PubMed]
- Haimeur, A.; Ulmann, L.; Mimouni, V.; Guéno, F.; Pineau-Vincent, F.; Meskini, N.; Tremblin, G. The role of Odontella aurita, a marine diatom rich in EPA, as a dietary supplement in dyslipidemia, platelet function and oxidative stress in high-fat fed rats. Lipids Health Dis. 2012, 11, 147. [Google Scholar] [CrossRef] [PubMed]
- Vormund, K.; Braun, J.; Rohrmann, S.; Bopp, M.; Ballmer, P.; Faeh, D. Mediterranean diet and mortality in Switzerland: An alpine paradox? Eur. J. Nutr. 2015, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Alam, F.; Saqib, Q.N.U.; Ashraf, M. Zanthoxylum armatum DC extracts from fruit, bark and leaf induce hypolipidemic and hypoglycemic effects in mice-in vivo and in vitro study. BMC Complement. Altern. Med. 2018, 18, 68. [Google Scholar] [CrossRef]
- Wat, E.; Wang, Y.; Chan, K.; Law, H.W.; Koon, C.M.; Lau, K.M.; Leung, P.C.; Yan, C.; San Lau, C.B. An in vitro and in vivo study of a 4-herb formula on the management of diet-induced metabolic syndrome. Phytomedicine 2018, 42, 112–125. [Google Scholar] [CrossRef]
- Manasa, V.; Tumaney, A.W. Evaluation of the anti-dyslipidemic effect of spice fixed oils in the in vitro assays and the high fat diet-induced dyslipidemic mice. Food Biosci. 2022, 46, 101574. [Google Scholar] [CrossRef]
- Sandoval-Gallegos, E.M.; Ramírez-Moreno, E.; Lucio, J.G.D.; Arias-Rico, J.; Cruz-Cansino, N.; Ortiz, M.I.; Cariño-Cortés, R. In vitro bioaccessibility and effect of Mangifera indica (Ataulfo) leaf extract on induced dyslipidemia. J. Med. Food 2018, 21, 47–56. [Google Scholar] [CrossRef]
- Venturini, D.; Simão, A.N.C.; Urbano, M.R.; Dichi, I. Effects of extra virgin olive oil and fish oil on lipid profile and oxidative stress in patients with metabolic syndrome. Nutrition 2015, 31, 834–840. [Google Scholar] [CrossRef] [PubMed]
- De Lellis, L.F.; Morone, M.V.; Buccato, D.G.; Cordara, M.; Larsen, D.S.; Ullah, H.; Piccinocchi, R.; Piccinocchi, G.; Balaji, P.; Baldi, A.; et al. Efficacy of food supplement based on monacolins, γ-oryzanol, and γ-aminobutyric acid in mild dyslipidemia: A randomized, double-blind, parallel-armed, placebo-controlled clinical trial. Nutrients 2024, 16, 2983. [Google Scholar] [CrossRef] [PubMed]
- Tinker, L.F.; Schneeman, B.O.; Davis, P.A.; Gallaher, D.D.; Waggoner, C.R. Consumption of prunes as a source of dietary fiber in men with mild hypercholesterolemia. Am. J. Clin. Nutr. 1991, 53, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Moghadam, M.H.; Ghasemi, Z.; Sepahi, S.; Rahbarian, R.; Mozaffari, H.M.; Mohajeri, S.A. Hypolipidemic effect of Lactuca sativa seed extract, an adjunctive treatment, in patients with hyperlipidemia: A randomized double-blind placebo-controlled pilot trial. J. Herb. Med. 2020, 23, 100373. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Three-arm, placebo-controlled, randomized clinical trial evaluating the metabolic effect of a combined nutraceutical containing a bergamot standardized flavonoid extract in dyslipidemic overweight subjects. Phytother. Res. 2019, 33, 2094–2101. [Google Scholar] [CrossRef]
- Kinoshita, H.; Ogata, Y. Effect of bitter melon extracts on lipid levels in Japanese subjects: A randomized controlled study. Evid. Based Complement. Alternat. Med. 2018, 2018, 4915784. [Google Scholar] [CrossRef] [PubMed]
- De Bock, M.; Derraik, J.G.; Brennan, C.M.; Biggs, J.B.; Smith, G.C.; Cameron-Smith, D.; Wall, C.R.; Cutfield, W.S. Psyllium supplementation in adolescents improves fat distribution & lipid profile: A randomized, participant-blinded, placebo-controlled, crossover trial. PLoS ONE 2012, 7, e41735. [Google Scholar]
- Morse, S.A.; Zhang, R.; Thakur, V.; Reisin, E. Hypertension and the metabolic syndrome. Am. J. Med. Sci. 2005, 330, 303–310. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M.; Chase, J.-A.D. Blood pressure outcomes of medication adherence interventions: Systematic review and meta-analysis. J. Behav. Med. 2016, 39, 1065–1075. [Google Scholar] [CrossRef]
- McCormack, T.; Krause, T.; O’Flynn, N. Management of hypertension in adults in primary care: NICE guideline. Br. J. Gen. Pract. 2012, 62, 163–164. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of hypertension: A systematic review and doseresponse meta-analysis of prospective studies. Adv. Nutr. 2017, 8, 793–803. [Google Scholar] [CrossRef]
- Tziomalos, K.; Athyros, V.G.; Karagiannis, A.; Mikhailidis, D.P. Endothelial dysfunction in metabolic syndrome: Prevalence, pathogenesis and management. Nutr. Metabol. Cardiovasc. Dis. 2010, 20, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Luna-Vázquez, F.J.; Ibarra-Alvarado, C.; Rojas-Molina, A.; Rojas-Molina, J.I.; Yahia, E.M.; Rivera-Pastrana, D.M.; Rojas-Molina, A.; Zavala-Sánchez, M.Á. Nutraceutical value of black cherry Prunus serotina Ehrh. fruits: Antioxidant and antihypertensive properties. Molecules 2013, 18, 14597–14612. [Google Scholar] [CrossRef]
- Liman, A.A.; Salihu, A.; Onyike, E. Effect of methanol extract of baobab (Adansonia digitata L.) fruit pulp on NG-Nitro-L-arginine methyl ester (L-NAME) induced hypertension in rats. High Blood Press. Cardiovasc. Prev. 2021, 28, 291–300. [Google Scholar] [CrossRef]
- Kim, B.; Kim, K.W.; Lee, S.; Jo, C.; Lee, K.; Ham, I.; Choi, H.Y. Endothelium-dependent vasorelaxant effect of Prunus persica branch on isolated rat thoracic aorta. Nutrients 2019, 11, 1816. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.L.; Liu, A.H.; Radavelli-Bagatini, S.; Shafaei, A.; Boyce, M.C.; Wood, L.G.; McCahon, L.; Koch, H.; Sim, M.; Hill, C.R.; et al. Cruciferous vegetables lower blood pressure in adults with mildly elevated blood pressure in a randomized, controlled, crossover trial: The VEgetableS for vaScular hEaLth (VESSEL) study. BMC Med. 2024, 22, 353. [Google Scholar] [CrossRef] [PubMed]
- Dehkordi, F.R.; Kamkhah, A.F. Antihypertensive effect of Nigella sativa seed extract in patients with mild hypertension. Fundam. Clin. Pharmacol. 2008, 22, 447–452. [Google Scholar] [CrossRef]
- Sleiman, C.; Daou, R.M.; Al Hazzouri, A.; Hamdan, Z.; Ghadieh, H.E.; Harbieh, B.; Romani, M. Garlic and Hypertension: Efficacy, Mechanism of Action, and Clinical Implications. Nutrients 2024, 16, 2895. [Google Scholar] [CrossRef]
- Ried, K.; Frank, O.R.; Stocks, N.P. Aged garlic extract lowers blood pressure in patients with treated but uncontrolled hypertension: A randomised controlled trial. Maturitas 2010, 67, 144–150. [Google Scholar] [CrossRef]
- Santhakumar, A.B.; Kundur, A.R.; Fanning, K.; Netzel, M.; Stanley, R.; Singh, I. Consumption of anthocyanin-rich Queen Garnet plum juice reduces platelet activation related thrombogenesis in healthy volunteers. J. Funct. Foods 2015, 12, 11–22. [Google Scholar] [CrossRef]
- Santhakumar, A.B.; Kundur, A.R.; Sabapathy, S.; Stanley, R.; Singh, I. The potential of anthocyanin-rich Queen Garnet plum juice supplementation in alleviating thrombotic risk under induced oxidative stress conditions. J. Funct. Foods 2015, 14, 747–757. [Google Scholar] [CrossRef]
- Burns Kraft, T.F.; Dey, M.; Rogers, R.B.; Ribnicky, D.M.; Gipp, D.M.; Cefalu, W.T.; Raskin, I.; Lila, M.A. Phytochemical composition and metabolic performance-enhancing activity of dietary berries traditionally used by native North Americans. J. Agric. Food Chem. 2008, 56, 654–660. [Google Scholar] [CrossRef]
- Akindele, A.J.; Adeneye, A.A.; Salau, O.S.; Sofidiya, M.O.; Benebo, A.S. Dose and time-dependent sub-chronic toxicity study of hydroethanolic leaf extract of Flabellaria paniculata Cav.(Malpighiaceae) in rodents. Front. Pharmacol. 2014, 5, 78. [Google Scholar] [CrossRef] [PubMed]
- Adewunmi, C.O.; Ojewole, J.A.O. Safety of traditional medicines, complementary and alternative medicines in Africa. Afr. J. Tradit. Complement. Altern. Med. 2004, 1, 1–3. [Google Scholar] [CrossRef]
- Likhitsup, A.; Chen, V.L.; Fontana, R.J. Estimated exposure to 6 potentially hepatotoxic botanicals in US adults. JAMA Netw. Open 2024, 7, e2425822. [Google Scholar] [CrossRef] [PubMed]
- de Sousa Lima, C.M.; Fujishima, M.A.T.; de Paula Lima, B.; Mastroianni, P.C.; de Sousa, F.F.O.; da Silva, J.O. Microbial contamination in herbal medicines: A serious health hazard to elderly consumers. BMC Complement. Med. Ther. 2020, 20, 17. [Google Scholar] [CrossRef]
- Luo, L.; Wang, B.; Jiang, J.; Fitzgerald, M.; Huang, Q.; Yu, Z.; Li, H.; Zhang, J.; Wei, J.; Yang, C.h.; et al. Heavy metal contaminations in herbal medicines: Determination, comprehensive risk assessments, and solutions. Front. Pharmacol. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Campbell-Tofte, J.I.A.; Mølgaard, P.; Winther, K. Harnessing the potential clinical use of medicinal plants as anti-diabetic agents. Botanics Targets Ther. 2012, 2, 7–19. [Google Scholar] [CrossRef]
- Hellión-lbarrola, M.C.; Montalbetti, Y.; Heinichen, O.; Alvarenga, N.; Figueredo, A.; Ferro, E.A. Isolation of hypotensive compounds from Solanum sisymbriifolium. J. Ethnopharmacol. 2000, 70, 301–307. [Google Scholar] [CrossRef]
- Ahmed, M.; Khan, M.A.; Arshad, M.; Zafar, M. Ethnophytotherapical approaches for the treatment of diabetes by the local inhabitants of district Attock (Pakistan). Ethnobotanical Leafl. 2006, 10, 41–48. [Google Scholar]
- Perera, L.M.S.; Escobar, A.; Souccar, C.; Remigio, M.A.; Mancebo, B. Pharmacological and toxicological evaluation of Rhizophora mangle L., as a potential antiulcerogenic drug: Chemical composition of active extract. J. Pharmacognosy Phytother. 2010, 2, 56–63. [Google Scholar]
- Afolabi, S.O.; Akindele, A.J.; Awodele, O.; Anunobi, C.C.; Adeyemi, O.O. A 90 day chronic toxicity study of Nigerian herbal preparation DAS77 in rats. BMC Complement. Altern. Med. 2012, 12, 79. [Google Scholar] [CrossRef]
- Verpoorte, R.; Choi, Y.H.; Kim, H.K. Ethnopharmacology and systems biology: A perfect holistic match. J. Ethnopharmacol. 2005, 100, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Ijinu, T.P.; Rani, M.P.; Sasidharan, S.P.; Shanmugarama, S.; Govindarajan, R.; George, V.; Pushpangadan, P. Clinical significance of herb–drug interactions. In Nutraceuticals: A Holistic Approach to Disease Prevention; Ullah, H., Rauf, A., Daglia, M., Eds.; De Gruyter: Berlin, Germany, 2024; p. 103. [Google Scholar]
- Seden, K.; Dickinson, L.; Khoo, S.; Back, D. Grapefruit-drug interactions. Drugs 2010, 70, 2373–2407. [Google Scholar] [CrossRef]
- Yuan, C.S.; Wei, G.A.N.G.; Dey, L. American ginseng reduces warfarin’s effect in healthy patients: A randomized, controlled trial. ACC Curr. J. Rev. 2004, 13, 9–10. [Google Scholar] [CrossRef]
- Mohammed Abdul, M.I.; Jiang, X.; Williams, K.M.; Day, R.O.; Roufogalis, B.D.; Liauw, W.S.; Xu, H.; McLachlan, A.J. Pharmacodynamic interaction of warfarin with cranberry but not with garlic in healthy subjects. Br. J. Pharmacol. 2008, 154, 1691–1700. [Google Scholar] [CrossRef]
- Thakkar, S.; Anklam, E.; Xu, A.; Ulberth, F.; Li, J.; Li, B.; Hugas, M.; Sarma, N.; Crerar, S.; Swift, S.; et al. Regulatory landscape of dietary supplements and herbal medicines from a global perspective. Regul. Toxicol. Pharmacol. 2020, 114, 104647. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Niazi, S.; Malmir, H.; Mirmiran, P.; Shabani, M.; Hasheminia, M.; Azizi, F. Fruit and vegetable intake modifies the association between ultra-processed food and metabolic syndrome. Nutr. Metab. 2024, 21, 58. [Google Scholar] [CrossRef]
- Joana Gil-Chávez, G.; Villa, J.A.; Fernando Ayala-Zavala, J.; Basilio Heredia, J.; Sepulveda, D.; Yahia, E.M.; González-Aguilar, G.A. Technologies for extraction and production of bioactive compounds to be used as nutraceuticals and food ingredients: An overview. Compr. Rev. Food Sci. Food Saf. 2013, 12, 5–23. [Google Scholar] [CrossRef]
- Mohammad Azmin, S.N.H.; Abdul Manan, Z.; Wan Alwi, S.R.; Chua, L.S.; Mustaffa, A.A.; Yunus, N.A. Herbal processing and extraction technologies. Sep. Purif. Rev. 2016, 45, 305–320. [Google Scholar] [CrossRef]
- Jha, A.K.; Sit, N. Extraction of bioactive compounds from plant materials using combination of various novel methods: A review. Trends Food Sci. Technol. 2021, 119, 579–591. [Google Scholar] [CrossRef]
- Wells, M.J. Principles of extraction and the extraction of semivolatile organics from liquids. In Sample Preparation Techniques in Analytical Chemistry; Mitra, S., Ed.; Wiley & Sons, Inc.: Hoboken, NJ, USA, 2003; pp. 37–138. [Google Scholar]
- Murakami, H.; Omiya, M.; Miki, Y.; Umemura, T.; Esaka, Y.; Inoue, Y.; Teshima, N. Evaluation of the adsorption properties of nucleobase-modified sorbents for a solid-phase extraction of watersoluble compounds. Talanta 2020, 217, 121052. [Google Scholar] [CrossRef] [PubMed]
- Merkle, S.; Kleeberg, K.K.; Fritsche, J. Recent developments and applications of solid phase microextraction (SPME) in food and environmental analysis—A review. Chromatography 2015, 2, 293–381. [Google Scholar] [CrossRef]
- Chemat, F.; Tomao, V.; Virot, M. Ultrasound-assisted extraction in food analysis. In Handbook of Food Analysis Instruments; Otles, S., Ed.; CRC Press: Boca Raton, FL, USA, 2008; pp. 85–103. [Google Scholar]
- Jambrak, A.R.; Mason, T.J.; Lelas, V.; Herceg, Z.; Herceg, I.L. Effect of ultrasound treatment on solubility and foaming properties of whey protein suspensions. J. Food Eng. 2008, 86, 281–287. [Google Scholar] [CrossRef]
- Nadar, S.S.; Rao, P.; Rathod, V.K. Enzyme assisted extraction of biomolecules as an approach to novel extraction technology: A review. Food Res. Int. 2018, 108, 309–330. [Google Scholar] [CrossRef]
- Yahya, N.A.; Attan, N.; Wahab, R.A. An overview of cosmeceutically relevant plant extracts and strategies for extraction of plant-based bioactive compounds. Food Bioprod. Process. 2018, 112, 69–85. [Google Scholar] [CrossRef]
- Pasrija, D.; Anandharamakrishnan, C. Techniques for extraction of green tea polyphenols: A review. Food Bioprod. Process. 2015, 8, 935–950. [Google Scholar] [CrossRef]
- Brunner, G. Supercritical fluids: Technology and application to food processing. J. Food Eng. 2005, 67, 21–33. [Google Scholar] [CrossRef]
- Gupta, A.; Naraniwal, M.; Kothari, V. Modern extraction methods for preparation of bioactive plant extracts. Int. J. Appl. Nat. Sci. 2012, 1, 8–26. [Google Scholar]
- Jadhav, D.; Rekha, B.N.; Gogate, P.R.; Rathod, V.K. Extraction of vanillin from vanilla pods: A comparison study of conventional Soxhlet and ultrasound assisted extraction. J. Food Eng. 2009, 93, 421–426. [Google Scholar] [CrossRef]
- Cho, Y.J.; Hong, J.Y.; Chun, H.S.; Lee, S.K.; Min, H.Y. Ultrasonication assisted extraction of resveratrol from grapes. J. Food Eng. 2006, 77, 725–730. [Google Scholar] [CrossRef]
- Sun, Y.; Liu, Z.; Wang, J. Ultrasound-assisted extraction of five isoflavones from Iris tectorum Maxim. Sep. Purif. Technol. 2011, 78, 49–54. [Google Scholar] [CrossRef]
- Pan, X.; Niu, G.; Lio, H. Comparision of microwave assisted extraction and conventional extraction techniques for the extraction of tanshinones from Saliva miltiorrhiza bunge. Biochem. Eng. J. 2002, 12, 71–77. [Google Scholar] [CrossRef]
- Huie, C.W. A review of modern sample-preparation techniques for the extraction and analysis of medicinal plants. Anal. Bioanal. Chem. 2002, 373, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Tripathi, R.; Kamat, S.D.; Kamat, D.V. Comparative study of phenolics and antioxidant activity of phytochemicals of T. chebula extracted using microwave and ultrasonication. Int. J. Pharm. Sci. Res. 2012, 3, 194–197. [Google Scholar]
- Reverchon, E.; Marco, I. Supercritical fluid extraction and fractionation of natural matter. J. Supercrit Fluids. 2006, 38, 146–166. [Google Scholar] [CrossRef]
- Aleksovski, S.; Sovova, H.; Urapova, B.; Poposka, F. Supercritical CO2 extraction and Soxhlet extraction of grape seeds oil. Bull. Chem. Technol. Macedonia 1998, 17, 129–134. [Google Scholar]
- Kothari, V.; Gupta, A.; Naraniwal, M. Comparative study of various methods for extraction of antioxidant and antibacterial compounds from plant seeds. J. Nat. Remedies 2012, 12, 162–173. [Google Scholar]
- Moelants, K.R.; Lemmens, L.; Vandebroeck, M.; Van Buggenhout, S.; Van Loey, A.M.; Hendrickx, M.E. Relation between particle size and carotenoid bioaccessibility in carrot-and tomato-derived suspensions. J. Agric. Food Chem. 2012, 60, 11995–12003. [Google Scholar] [CrossRef]
- Porter, C.J.; Trevaskis, N.L.; Charman, W.N. Lipids and lipidbased formulations: Optimizing the oral delivery of lipophilic drugs. Nat. Rev. Drug Discov. 2007, 6, 231–248. [Google Scholar] [CrossRef]
- Pouton, C.W.; Porter, C.J. Formulation of lipid-based delivery systems for oral administration: Materials, methods and strategies. Adv. Drug Deliv. Rev. 2008, 60, 625–637. [Google Scholar] [CrossRef]
- Martinez, M.N.; Amidon, G.L. A mechanistic approach to understanding the factors affecting drug absorption: A review of fundamentals. J. Clin. Pharmacol. 2002, 42, 620–643. [Google Scholar] [CrossRef]
- Actis-Goretta, L.; Leveques, A.; Rein, M.; Teml, A.; Schäfer, C.; Hofmann, U.; Li, H.; Schwab, M.; Eichelbaum, M.; Williamson, G. Intestinal absorption, metabolism, and excretion of (−)-epicatechin in healthy humans assessed by using an intestinal perfusion technique. Am. J. Clin. Nutr. 2013, 98, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, G.; Ceyhan, T.; Çatalkaya, G.; Rajan, L.; Ullah, H.; Daglia, M.; Capanoglu, E. Encapsulated phenolic compounds: Clinical efficacy of a novel delivery method. Phytochem. Rev. 2024, 23, 781–819. [Google Scholar] [CrossRef]
- Khan, H.; Ullah, H.; Martorell, M.; Valdes, S.E.; Belwal, T.; Tejada, S.; Sureda, A.; Kamal, M.A. Flavonoids nanoparticles in cancer: Treatment, prevention and clinical prospects. Semin. Cancer Biol. 2021, 69, 200–211. [Google Scholar] [CrossRef]
- Dias, D.R.; Botrel, D.A.; Fernandes, R.V.D.B.; Borges, S.V. Encapsulation as a tool for bioprocessing of functional foods. Curr. Opin. Food Sci. 2017, 13, 31–37. [Google Scholar] [CrossRef]
- Naczk, M.; Shahidi, F. Phenolics in cereals, fruits and vegetables: Occurrence, extraction and analysis. J. Pharm. Biomed. Anal. 2006, 41, 1523–1542. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.; Tognolini, M.; Borges, G.; Crozier, A. Dietary (poly) phenolics in human health: Structures, bioavailability, and evidence of protective effects against chronic diseases. Antioxid. Redox. Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef]
- Ezhilarasi, P.N.; Karthik, P.; Chhanwal, N.; Anandharamakrishnan, C. Nanoencapsulation techniques for food bioactive components: A review. Food Bioproc. Tech. 2013, 6, 628–647. [Google Scholar] [CrossRef]
- Fang, Z.; Bhandari, B. Encapsulation of polyphenols–a review. Trends Food Sci. Technol. 2010, 21, 510–523. [Google Scholar] [CrossRef]
- Munin, A.; Edwards-Le’vy, F. Encapsulation of natural polyphenolic compounds; a review. Pharmaceutics 2011, 3, 793–829. [Google Scholar] [CrossRef]
- Mishra, M. Materials of natural origin for encapsulation. In Handbook of Encapsulation and Controlled Release; Mishra, M., Ed.; CRC Press: Boca Raton, FL, USA, 2015; pp. 517–540. [Google Scholar]
- Fernandes, A.; Sousa, A.; Azevedo, J.; Mateus, N.; de Freitas, V. Effect of cyclodextrins on the thermodynamic and kinetic properties of cyanidin-3-O-glucoside. Food Res. Int. 2013, 51, 748–755. [Google Scholar] [CrossRef]
- Ezzat, H.M.; Elnaggar, Y.S.R.; Abdallah, O.Y. Improved oral bioavailability of the anticancer drug catechin using chitosomes: Design, in-vitro appraisal and in-vivo studies. Int. J. Pharm. 2019, 565, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Meng, Q.; Zhou, J.; Chen, B.; Xi, J.; Long, P.; Zhang, L.; Hou, R. Nanoemulsion delivery system of tea polyphenols enhanced the bioavailability of catechins in rats. Food Chem. 2018, 242, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Kadari, A.; Gudem, S.; Kulhari, H.; Bhandi, M.M.; Borkar, R.M.; Kolapalli, V.R.M.; Sistla, R. Enhanced oral bioavailability and anticancer efficacy of fisetin by encapsulating as inclusion complex with HPbCD in polymeric nanoparticles. Drug Deliv. 2017, 26, 224–232. [Google Scholar] [CrossRef]
- Salem, M.A.; Aborehab, N.M.; Abdelhafez, M.M.; Ismail, S.H.; Maurice, N.W.; Azzam, M.A.; Alseekh, S.; Fernie, A.R.; Salama, M.M.; Ezzat, S.M. Anti-obesity effect of a tea mixture nano-formulation on rats occurs via the upregulation of AMP-activated protein kinase/sirtuin-1/glucose transporter type 4 and peroxisome proliferator-activated receptor gamma pathways. Metabolites 2023, 13, 871. [Google Scholar] [CrossRef]
- Wattanathorn, J.; Kawvised, S.; Thukham-mee, W. Encapsulated mulberry fruit extract alleviates changes in an animal model of menopause with metabolic syndrome. Oxidative Med. Cell Longev. 2019, 2019, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Colorado, D.; Fernandez, M.; Orozco, J.; Lopera, Y.; Muñoz, D.L.; Acín, S.; Balcazar, N. Metabolic activity of anthocyanin extracts loaded into non-ionic niosomes in diet-induced obese mice. Pharm. Res. 2020, 37, 152. [Google Scholar] [CrossRef]
- Sreerekha, P.R.; Dara, P.K.; Vijayan, D.K.; Chatterjee, N.S.; Raghavankutty, M.; Mathew, S.; Ravishankar, C.N.; Anandan, R. Dietary supplementation of encapsulated anthocyanin loaded-chitosan nanoparticles attenuates hyperlipidemic aberrations in male Wistar rats. Carbohydr. Polym. Technol. Appl. 2021, 2, 100051. [Google Scholar] [CrossRef]
- Christman, L.M.; Dean, L.L.; Allen, J.C.; Godinez, S.F.; Toomer, O.T. Peanut skin phenolic extract attenuates hyperglycemic responses in vivo and in vitro. PLoS ONE 2019, 14, e0214591. [Google Scholar] [CrossRef]
- Faria, W.C.S.; da Silva, A.A.; Veggi, N.; Kawashita, N.H.; de França Lemes, S.A.; de Barros, W.M.; da Conceiçao Cardoso, E.; Converti, A.; de Melo Moura, W.; Bragagnolo, N. Acute and subacute oral toxicity assessment of dry encapsulated and nonencapsulated green coffee fruit extracts. J. Food Drug Anal. 2020, 28, 337. [Google Scholar] [PubMed]
- Hussain, S.A.; Hameed, A.; Nazir, Y.; Naz, T.; Wu, Y.; Suleria, H.A.R.; Song, Y. Microencapsulation and the characterization of polyherbal formulation (PHF) rich in natural polyphenolic compounds. Nutrients 2018, 10, 843. [Google Scholar] [CrossRef] [PubMed]
- Wanjiru, J.; Gathirwa, J.; Sauli, E.; Swai, H.S. Formulation, optimization, and evaluation of Moringa oleifera leaf polyphenol-loaded phytosome delivery system against breast cancer cell lines. Molecules 2022, 27, 4430. [Google Scholar] [CrossRef] [PubMed]
- Vitaglione, P.; Lumaga, R.B.; Ferracane, R.; Sellitto, S.; Morelló, J.R.; Miranda, J.R.; Shimoni, E.; Fogliano, V. Human bioavailability of flavanols and phenolic acids from cocoa-nut creams enriched with free or microencapsulated cocoa polyphenols. Br. J. Nutr. 2013, 109, 1832–1843. [Google Scholar] [CrossRef]
- Garrido, I.; Urpi-Sarda, M.; Monagas, M.; Gómez-Cordovés, C.; Martín-Álvarez, P.J.; Llorach, R.; Bartolomé, B.; Andrés-Lacueva, C. Targeted analysis of conjugated and microbial-derived phenolic metabolites in human urine after consumption of an almond skin phenolic extract. J. Nutr. 2010, 140, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Shahbaz, M.U.; Arshad, M.; Mukhtar, K.; Nabi, B.G.; Goksen, G.; Starowicz, M.; Nawaz, A.; Ahmad, I.; Walayat, N.; Manzoor, M.F.; et al. Natural plant extracts: An update about novel spraying as an alternative of chemical pesticides to extend the postharvest shelf life of fruits and vegetables. Molecules 2022, 27, 5152. [Google Scholar] [CrossRef] [PubMed]
- Zabot, G.L.; Schaefer Rodrigues, F.; Polano Ody, L.; Vinícius Tres, M.; Herrera, E.; Palacin, H.; Córdova-Ramos, J.S.; Best, I.; Olivera-Montenegro, L. Encapsulation of bioactive compounds for food and agricultural applications. Polymers 2022, 14, 4194. [Google Scholar] [CrossRef] [PubMed]
- Gouin, S. Microencapsulation: Industrial appraisal of existing technologies and trends. Trends Food Sci. Technol. 2004, 15, 330–347. [Google Scholar] [CrossRef]
- Tonon, R.V.; Brabet, C.; Hubinger, M.D. Influence of process conditions on the physicochemical properties of açai (Euterpe oleraceae Mart.) powder produced by spray drying. J. Food Eng. 2008, 88, 411–418. [Google Scholar] [CrossRef]
- Kuck, L.S.; Noreña, C.P.Z. Microencapsulation of grape (Vitis labrusca var. Bordo) skin phenolic extract using gum Arabic, polydextrose, and partially hydrolyzed guar gum as encapsulating agents. Food Chem. 2016, 194, 569–576. [Google Scholar] [CrossRef]
- Rashidinejad, A. The road ahead for functional foods: Promising opportunities amidst industry challenges. Future Postharvest Food 2024, 1, 266–273. [Google Scholar] [CrossRef]
- Kandemir, K.; Piskin, E.; Xiao, J.; Tomas, M.; Capanoglu, E. Fruit juice industry wastes as a source of bioactives. J. Agric. Food Chem. 2022, 70, 6805–6832. [Google Scholar] [CrossRef] [PubMed]
- Galanakis, C.M. Functionality of food components and emerging technologies. Foods 2021, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Alu’datt, M.H.; Alrosan, M.; Gammoh, S.; Tranchant, C.C.; Alhamad, M.N.; Rababah, T.; Alzoubi, H.; Ghatasheh, S.; Ghozlan, K.; Tan, T.C. Encapsulation-based technologies for bioactive compounds and their application in the food industry: A roadmap for food-derived functional and health-promoting ingredients. Food Biosci. 2022, 50, 101971. [Google Scholar] [CrossRef]
- Zhang, R.; Zhang, Z.; McClements, D.J. Nanoemulsions: An emerging platform for increasing the efficacy of nutraceuticals in foods. Colloids Surf. B Biointerfaces 2020, 194, 111202. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Plant Extract | Study Model | Concentration/Dose | Outcomes | References |
|---|---|---|---|---|
| Prunus domestica L. fruit pulp | In vitro | - | ↓ α-amylase, α-glucosidase, HMG-CoA reductase, and pancreatic lipase enzymes ↓ nitrate, PGE2, and IL-1β | [33] |
| Prunus persica (L.) Stokes flower | In vivo | 0.2% or 0.6% extract mixed with diet for 8 weeks | ↓ body weight, visceral fat mass, and serum levels of glucose, ALT, and AST | [34] |
| Hibiscus sabdariffa L., Vigna unguiculata L. Walp., and Solanum nigrum L. extracts | In vivo | 200 mg/kg/day for 12 days | ↓ FBG levels | [40] |
| Prunus salicina Lindl. (Queen Garnet plum juice) | Randomized, double-blinded, placebo-controlled, cross-over trial | 200 mL/day for 4 weeks | ↓ body weight, BMI, leptin levels, and increased adiponectin levels in healthy participants | [41] |
| Soluble fiber-rich brewer’s spent grain (rich in soluble fibers and ferulic acid) | Randomized, placebo-controlled, double-blind, cross-over clinical trial | 4.25 g of extract before OGTT in cross-over design | ↓ postprandial glycemia and insulinemia in healthy individuals with slightly impaired glucose tolerance | [42] |
| Extra-virgin olive oil | Randomized, controlled, cross-over clinical trial | Olive oil consumed as meal | ↓ postprandial glycemic response in type 1 diabetic patients | [45] |
| Olive oil | Interventional study | 30 mL/day for 4 weeks | ↓ FBG, TC, LDL, and TGs in diabetic patients ↑ HDL | [46] |
| Olive leaf extract | Randomized, placebo-controlled, clinical trial | 500 mg/day for 14 weeks | ↓ HbA1c and fasting insulin levels in diabetic patients | [47] |
| Fenugreek seeds | Randomized, double-blind, placebo-controlled, clinical trial | 1 g/day for 2 months | Improvement of glucose and insulin in diabetic patients Non-significant effects on FBG and OGTT | [48] |
| Fenugreek seeds | Randomized, placebo-controlled, cross-over clinical trial | 100 g/day for 10 days | ↓ FBG and improvement in OGTT in diabetic patients | [49] |
| Fenugreek seeds | Interventional study | 15 g/day | ↓ postprandial glucose levels in diabetic patients | [50] |
| Green tea extract | Randomized, placebo-controlled, cross-over clinical trial | Packet of green tea extract (containing 544 mg polyphenols) for 2 months | ↓ HbA1c levels in healthy subjects No effects on FBG | [51] |
| Exercise and green tea extract | Randomized, placebo-controlled, cross-over clinical trial | Green tea extract (containing 890 mg polyphenols) | ↓ AUC for insulin in healthy subjects ↑ insulin sensitivity | [52] |
| Epigallo-catechin-3-gallate (800 mg/day) | Randomized, double-blind, clinical trial | Epigallo-catechin-3-gallate (800 mg/day) for 8 weeks | No significant effects on FBG, HbA1c, insulin sensitivity, insulin secretion, and glucose tolerance | [53] |
| Qinggan Jiangtang tablets | Randomized, controlled, double-blind clinical trial | Three tablets twice a day for 1 month | ↓ blood glucose levels, lipid profiles, blood pressure, and insulin resistance in patients with metabolic syndrome | [54] |
| Grape seed extract (rich in resveratrol and procyanidins) | Randomized, placebo-controlled, clinical trial | 100 mg/day for 8 weeks | Improvement of insulin concentration and resistance in adolescents with metabolic syndrome. | [55] |
| Zanthoxylum armatum DC (fruits, leaves, and bark extracts) | In vivo | 500 mg/kg/day for 15 days | ↓ TC, TG, LGL levels | [61] |
| Schisandrae Fructus, milk thistle, hawthorn, and bitter melon | In vitro / In vivo | 0–1000 µg/mL (in vitro); 2–4 % herbal formula for 12 weeks (in vivo) | ↓ adipocyte differentiation, cholesterol uptake, and hepatic lipid accumulation. ↓ body weight, fat pad mass, liver weight, and improved lipid profiles. | [62] |
| Fixed oils from spices (Alpinia galanga (L.) Willd., Cinnamomum zeylanicum var. cassia, Trigonella foenum-graecum L., Foeniculum vulgare Mill., and Myristica fragrans Houtt.) | In vitro / In vivo | 12.5–100 μg/mL (in vitro); 2.5–12.5% fixed oils mixed with diet (in vivo) | ↓ accumulated lipid droplets in 3T3-L1 cell lines. Improvement of lipid profiles and antioxidant enzymes. ↓ droplets in liver and adipose tissues. | [63] |
| Mangifera indica L. leaves extract | In vivo | 400 mg/kg for 32 days | ↓ TC, TG, LDL, atherogenic index ↑ HDL levels | [64] |
| Extra-virgin olive oil plus fish oil | Interventional study | Extra-virgin olive oil (10 mL/day) and fish oil (3 g/day) for 3 months | ↓ TC, LDL, and oxidative capacity ↑ HDL levels | [65] |
| Monascus purpureus | Randomized, double-blind, placebo-controlled trial | Standardized food supplement (2.8 mg of monacolins) for 3 months | ↓ TC and LDL levels ↑ HDL levels | [66] |
| Prunes | Randomized, placebo-controlled, crossover, clinical trial | 100 g for 8 weeks | ↓ serum LDL levels and fecal lithocholic acid | [67] |
| Lettuce seed extract | Randomized, double-blind, placebo-controlled, pilot trial | 1000 mg/day for 12 weeks | ↓ TC, TG, and LDL levels ↑ HDL levels | [68] |
| Bergamot extract (120 mg flavonoids), vitamin C, phytosterols, and chlorogenic acid from dry artichoke extract | Randomized, double-blind, placebo-controlled trial | Two pills of food supplement for 8 weeks | ↓ TC, TG, LDL, and non-HDL cholesterol levels. ↓ hs-CRP and TNF-α. | [69] |
| Bitter melon extract | Randomized, placebo-controlled, clinical trial | 100 mg for 30 days | ↓ LDL levels. No significant effects on TC, TG, and blood glucose levels | [70] |
| Psyllium fibers | Randomized, placebo-controlled, crossover, clinical trial | 6 g/day for 6 weeks | Improvement of fat distribution and lipid profile in healthy adolescents | [71] |
| Black cherry fruit extract | In vivo | 300 mg/kg/day for 4 weeks | ↓ oxidative stress markers and systolic blood pressure | [77] |
| Adansonia digitata L. | In vivo | 200 mg/kg and 400 mg/kg/day for 3 weeks | Dose-dependent reduction in systolic and diastolic blood pressure, mean arterial pressure, and heart rate. ↓ ACE activity, CRP, IL-1β, malondialdehyde, creatine kinase-MB, and lactate dehydrogenase | [78] |
| Prunus persica (L.) Stokes extract | In vitro | 0.5 to 20 μg/mL | Enhanced vasorelaxation by targeting NO-sGC-cGMP and IP3R pathways | [79] |
| Cruciferous vegetables | Randomized, placebo-controlled, cross-over clinical trial | 300 g/day for 2 weeks | ↓ systolic blood pressure | [80] |
| Nigella sativa L. seed extract | Randomized, double-blind, placebo-controlled, clinical trial | 200 and 400 mg/day for 8 weeks | ↓ systolic and diastolic blood pressure | [81] |
| Garlic extract | Randomized, double-blind, placebo-controlled, clinical trial | 960 mg/day (containing 2.4 mg S-allylcysteine) for 12 weeks | ↓ systolic blood pressure | [83] |
| Anthocyanin-rich Queen Garnet plum juice | Randomized, double-blind, placebo-controlled, cross-over trial | 200 mL/day for 28 days | ↓ ADP-induced platelet aggregation and platelet activation-dependent P-selectin expression. Prolonged activated-partial thromboplastin clotting time. ↓ plasma-fibrinogen and malondialdehyde levels. | [84,85] |
| Viburnum trilobum Marshall, Amelanchier alnifolia, Shepherdia argentea (Pursh) Nutt., and Prunus virginiana L. | In vitro | - | ↓ aldose reductase. ↓ IL-1β and COX-2 gene expression. | [86] |
| Encapsulation Technique | Definition | Uses | Advantages | Disadvantages |
|---|---|---|---|---|
| Spray-drying | A method where active ingredients are mixed with a wall material, atomized in a hot chamber, and dried into powder. | Used for shelf-life enhancement and the encapsulation of various active compounds. | Low cost, easy scalability, and improved product stability. | A limited number of wall materials can be used. |
| Freeze-drying | Freezing active materials to form ice, followed by sublimation in a vacuum to create porous, powdered products. | Encapsulation of temperature-sensitive materials like aromas and volatile oils. | Simple process, preserves sensitive compounds effectively. | Time-consuming and high energy costs. |
| Extrusion | Polymer solution-containing active material is extruded through a nozzle into a gel solution. | Used for encapsulating both hydrophilic and hydrophobic compounds. | Simple, laboratory-friendly, and produces high shelf-life capsules. | Difficult and expensive to scale up. |
| Emulsification | Involves creating emulsions of two immiscible liquids (water and oil) stabilized by emulsifiers. | Encapsulation of oil-soluble compounds like dietary fats and sterols. | Provides both liquid and powder encapsulation options. | Requires specific emulsifiers for stabilization. |
| Coacervation | Separation of phases leading to the formation of encapsulated materials within polymeric walls. | High-efficiency encapsulation with controlled release properties. | High encapsulation efficiency and control over material release. | Capsules are often unstable and the production cost is high. |
| Molecular inclusion | Based on hydrogen bonding and electrostatic interactions between polar molecules. | Encapsulation of polar molecules, commonly using cyclodextrins. | Compatible with a wide range of polar compounds. | Limited use outside of specific polar interactions. |
| Ionic gelation | Encapsulation using microbeads in biopolymer gels, formed by methods like spraying or extrusion. | Commonly used for suspending active materials in polymer solutions. | Simple and adaptable to various active materials. | Limited by the biopolymer’s properties and stability in different environments. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, H.; Dacrema, M.; Buccato, D.G.; Fayed, M.A.A.; De Lellis, L.F.; Morone, M.V.; Di Minno, A.; Baldi, A.; Daglia, M. A Narrative Review on Plant Extracts for Metabolic Syndrome: Efficacy, Safety, and Technological Advances. Nutrients 2025, 17, 877. https://doi.org/10.3390/nu17050877
Ullah H, Dacrema M, Buccato DG, Fayed MAA, De Lellis LF, Morone MV, Di Minno A, Baldi A, Daglia M. A Narrative Review on Plant Extracts for Metabolic Syndrome: Efficacy, Safety, and Technological Advances. Nutrients. 2025; 17(5):877. https://doi.org/10.3390/nu17050877
Chicago/Turabian StyleUllah, Hammad, Marco Dacrema, Daniele Giuseppe Buccato, Marwa A. A. Fayed, Lorenza Francesca De Lellis, Maria Vittoria Morone, Alessandro Di Minno, Alessandra Baldi, and Maria Daglia. 2025. "A Narrative Review on Plant Extracts for Metabolic Syndrome: Efficacy, Safety, and Technological Advances" Nutrients 17, no. 5: 877. https://doi.org/10.3390/nu17050877
APA StyleUllah, H., Dacrema, M., Buccato, D. G., Fayed, M. A. A., De Lellis, L. F., Morone, M. V., Di Minno, A., Baldi, A., & Daglia, M. (2025). A Narrative Review on Plant Extracts for Metabolic Syndrome: Efficacy, Safety, and Technological Advances. Nutrients, 17(5), 877. https://doi.org/10.3390/nu17050877