
Impact of Different Low-Volume Concurrent Training Regimens on Cardiometabolic Health, Inflammation, and Fitness in Obese Metabolic Syndrome Patients

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Patients
2.3. Testing Procedures
2.3.1. Assessment of Blood Pressure
2.3.2. Blood Sample Collection and Analysis
2.3.3. Assessment of Body Composition
2.3.4. Calculation of the Metabolic Syndrome z-Score
2.3.5. Assessment of Cardiorespiratory Fitness Outcomes
2.3.6. Assessment of One-Repetition Maximum Strength and Overall Fitness z-Score
2.4. Nutritional Guidance
2.5. Low-Volume Concurrent Training Program
2.6. Statistical Analysis
3. Results
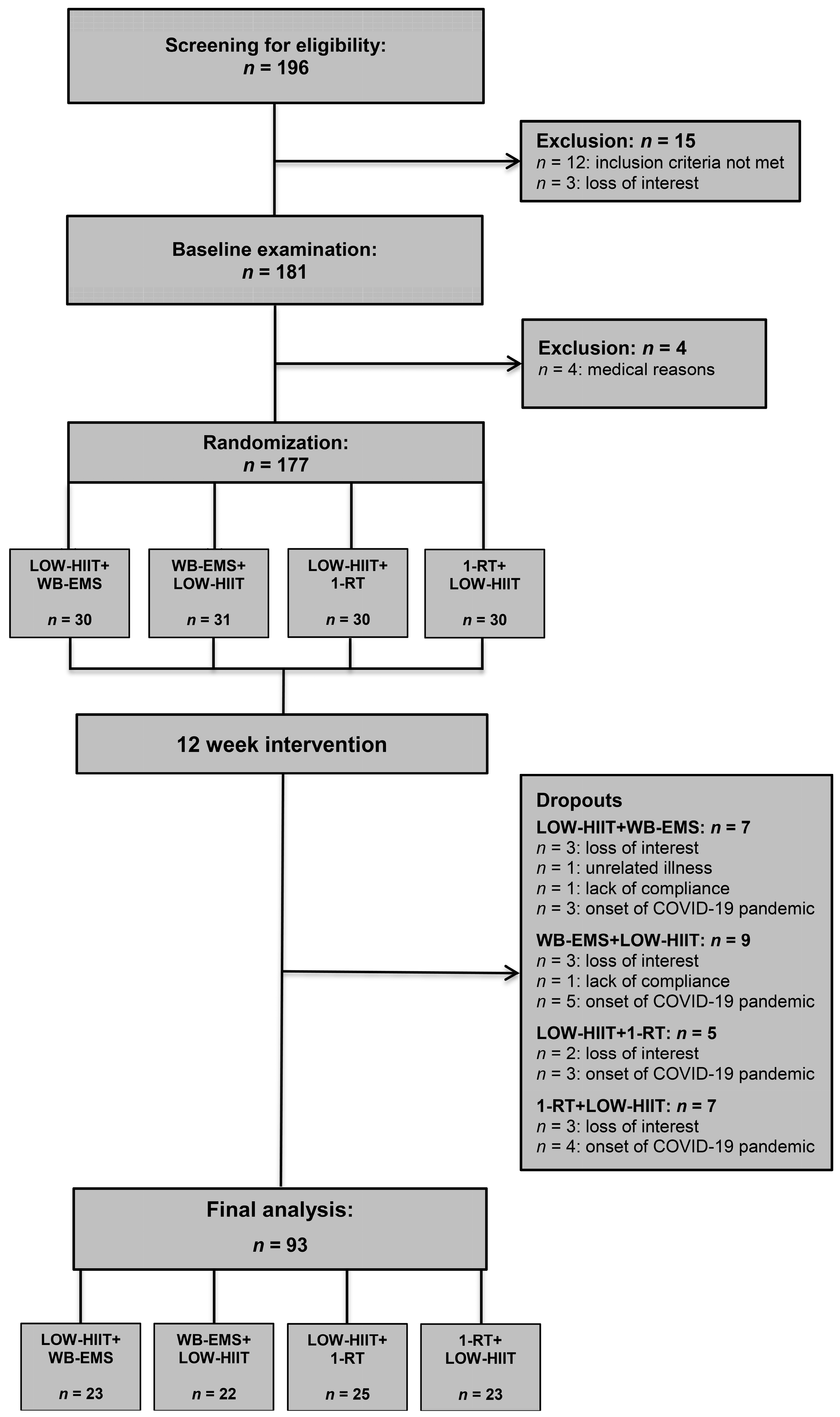
3.1. Study Flow, Training Data, and Adverse Events
3.2. Nutritional Intakes in All Groups
3.3. Study Part 1: Impact of Exercise Order in LOW-HIIT and WB-EMS
3.3.1. Anthropometric Variables in LOW-HIIT and WB-EMS Groups
3.3.2. Cardiometabolic and Inflammation Variables in LOW-HIIT and WB-EMS Groups
3.3.3. Physical Fitness Variables in LOW-HIIT and WB-EMS Groups
3.4. Study Part 1: Impact of Exercise Order in LOW-HIIT and 1-RT
3.4.1. Anthropometric Variables in LOW-HIIT and 1-RT Groups
3.4.2. Cardiometabolic and Inflammation Variables in LOW-HIIT and 1-RT Groups
3.4.3. Physical Fitness Variables in LOW-HIIT and 1-RT Groups
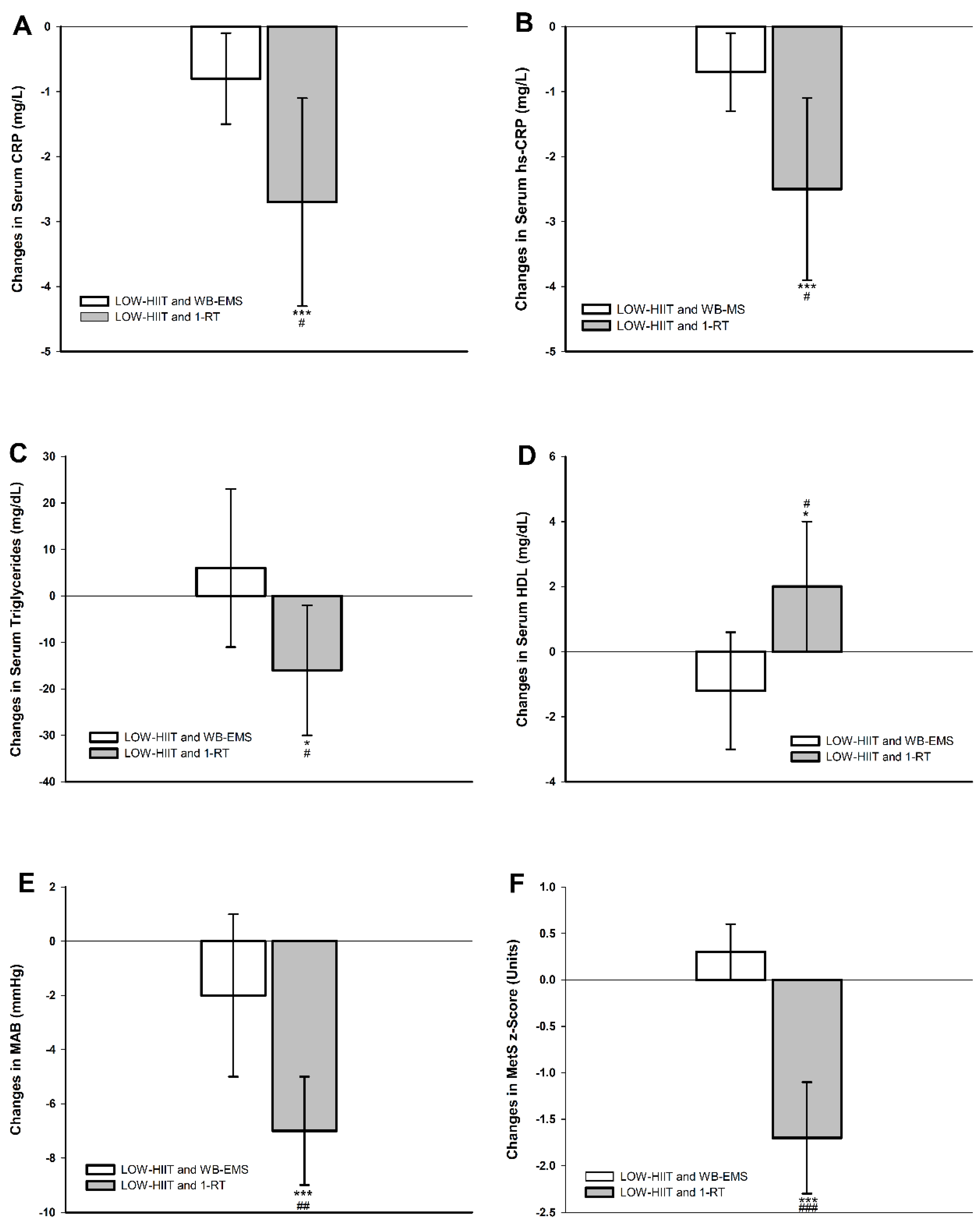
3.5. Study Part 2: Comparison of LOW-HIIT and WB-EMS Versus LOW-HIIT and 1-RT
3.5.1. Comparison of Anthropometric Variables in the Pooled Groups
3.5.2. Comparison of Cardiometabolic and Inflammation Variables in the Pooled Groups
3.5.3. Comparison of Physical Fitness Variables in the Pooled Groups
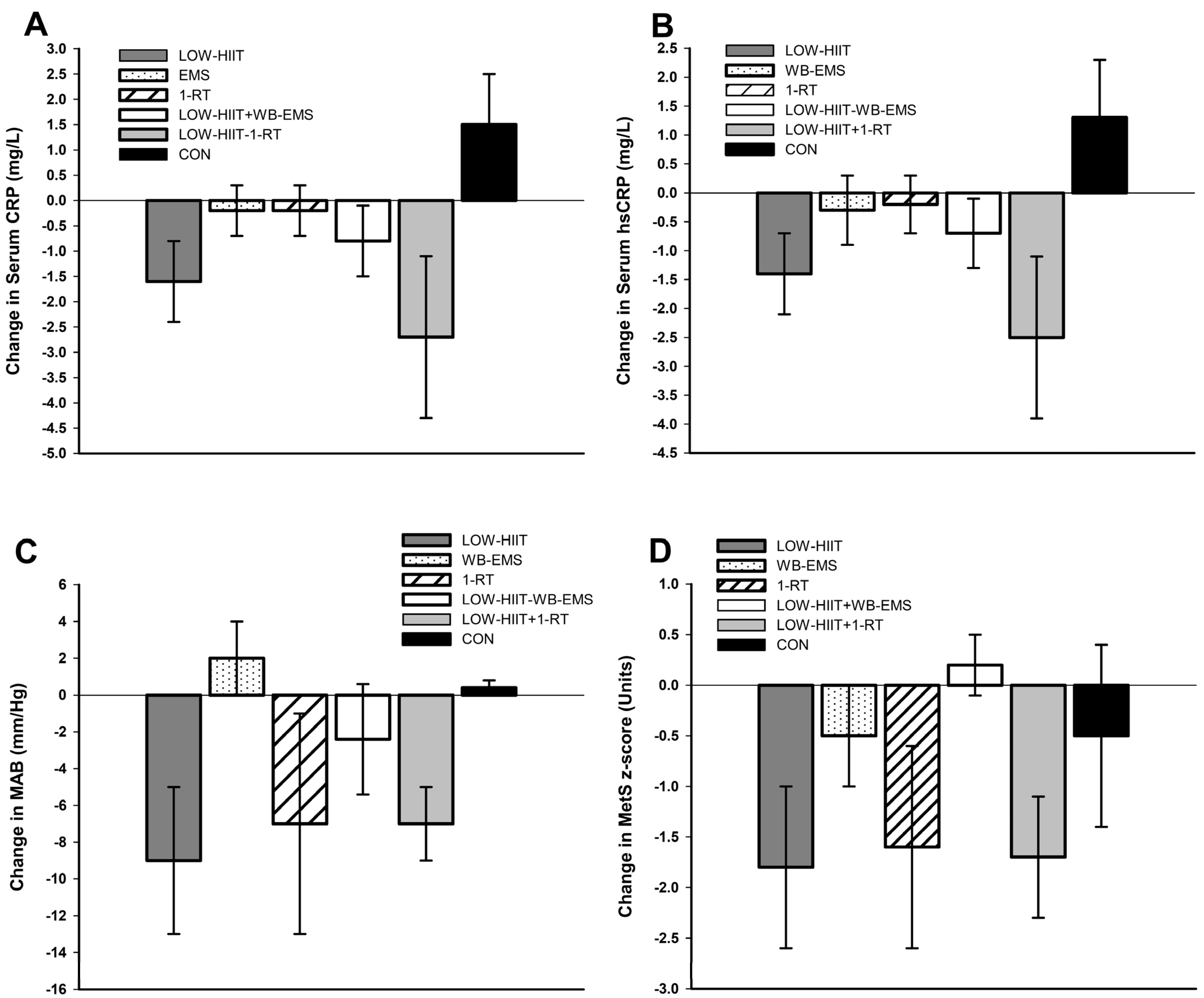
3.6. Comparison of Changes in Inflammation and Cardiometabolic Variables in the Low-Volume CT Programs Versus Single-Modality Low-Volume Training Programs from Previous Research
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Marott, S.C.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Benn, M. Components of the metabolic syndrome and risk of type 2 diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 3212–3221. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Qiu, X.; Ma, H.; Geng, Q. Incidence and long-term specific mortality trends of metabolic syndrome in the United States. Front. Endocrinol. 2023, 13, 1029736. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ju, H.; Xie, K.; Zhao, X. Association of inflammatory score with all-cause and cardiovascular mortality in patients with metabolic syndrome: NHANES longitudinal cohort study. Front. Immunol. 2024, 15, 1410871. [Google Scholar] [CrossRef]
- De la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; Ramirez de Molina, A. Dietary strategies implicated in the prevention and treatment of metabolic syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef] [PubMed]
- Carels, R.A.; Young, K.M.; Coit, C.; Clayton, A.M.; Spencer, A.; Hobbs, M. Can following the caloric restriction recommendations from the Dietary Guidelines for Americans help individuals lose weight? Eat. Behav. 2008, 9, 328–335. [Google Scholar] [CrossRef]
- Joseph, M.S.; Tincopa, M.A.; Walden, P.; Jackson, E.; Conte, M.L.; Rubenfire, M. The impact of structured exercise programs on metabolic syndrome and its components: A systematic review. Diabetes Metab. Syndr. Obes. 2019, 12, 2395–2404. [Google Scholar] [CrossRef] [PubMed]
- Thyfault, J.P.; Bergouignan, A. Exercise and metabolic health: Beyond skeletal muscle. Diabetologia 2020, 63, 1464–1474. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.; Fang, Z. Evaluating the impact of exercise on intermediate disease markers in overweight and obese individuals through a network meta-analysis of randomized controlled trials. Sci. Rep. 2024, 14, 12137. [Google Scholar] [CrossRef]
- Silva, F.M.; Duarte-Mendes, P.; Teixeira, A.M.; Soares, C.M.; Ferreira, J.P. The effects of combined exercise training on glucose metabolism and inflammatory markers in sedentary adults: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 1936. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Lu, B.; Su, W.; Song, X.; Shang, X.; Zheng, J.; Wang, J.; Yun, H. Comprehensive assessment of the effects of concurrent strength and endurance training on lipid profile, glycemic control, and insulin resistance in type 2 diabetes: A meta-analysis. Medicine 2024, 103, e37494. [Google Scholar] [CrossRef]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Cavallini, M.F.; Callaghan, M.E.; Premo, C.B.; Scott, J.W.; Dyck, D.J. Lack of time is the consistent barrier to physical activity and exercise in 18 to 64 year-old males and females from both South Carolina and Southern Ontario. J. Phys. Act. Res. 2020, 5, 100–106. [Google Scholar] [CrossRef]
- Baillot, A.; Chenail, S.; Barros Polita, N.; Simoneau, M.; Libourel, M.; Nazon, E.; Riesco, E.; Bond, D.S.; Romain, A.J. Physical activity motives, barriers, and preferences in people with obesity: A systematic review. PLoS ONE 2021, 16, e0253114. [Google Scholar] [CrossRef]
- Gillen, J.B.; Gibala, M.J. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl. Physiol. Nutr. Metab. 2014, 39, 409–412. [Google Scholar] [CrossRef]
- Kemmler, W.; Kleinöder, H.; Fröhlich, M. Editorial: Whole-body electromyostimulation: A training technology to improve health and performance in humans? Front. Physiol. 2020, 11, 523. [Google Scholar] [CrossRef]
- Iversen, V.M.; Norum, M.; Schoenfeld, B.J.; Fimland, M.S. No time to lift? Designing time-efficient training programs for strength and hypertrophy: A narrative review. Sports Med. 2021, 51, 2079–2095. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Dieterich, W.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. “HIIT the inflammation”: Comparative effects of low-volume interval training and resistance exercises on inflammatory indices in obese metabolic syndrome patients undergoing caloric restriction. Nutrients 2022, 14, 1996. [Google Scholar] [CrossRef]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Effects of very low volume high intensity versus moderate intensity interval training in obese metabolic syndrome patients: A randomized controlled study. Sci. Rep. 2021, 11, 2836. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Iron beats electricity: Resistance training but not whole-body electromyostimulation improves cardiometabolic health in obese metabolic syndrome patients during caloric restriction-a randomized-controlled study. Nutrients 2021, 13, 1640. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Koller, A.; Herrmann, H.J.; Ekici, A.B.; Neurath, M.F.; Zopf, Y. Differential effects of very-low-volume exercise modalities on telomere length, inflammation, and cardiometabolic health in obese metabolic syndrome patients: A subanalysis from two randomized controlled trials. Antioxidants 2023, 12, 1847. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Granacher, U.; Warneke, K.; Aragão-Santos, J.C.; Da Silva-Grigoletto, M.E.; Konrad, A. Minimalist training: Is lower dosage or intensity resistance training effective to improve physical fitness? A narrative review. Sports Med. 2024, 54, 289–302. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Shojaa, M.; von Stengel, S.; Filipovic, A.; Kleinöder, H.; Berger, J.; Fröhlich, M. Efficacy and safety of low frequency whole-body electromyostimulation (WB-EMS) to improve health-related outcomes in non-athletic adults. A systematic review. Front. Physiol. 2018, 9, 573. [Google Scholar] [CrossRef]
- Yin, M.; Li, H.; Bai, M.; Liu, H.; Chen, Z.; Deng, J.; Deng, S.; Meng, C.; Vollaard, N.B.J.; Little, J.P.; et al. Is low-volume high-intensity interval training a time-efficient strategy to improve cardiometabolic health and body composition? A meta-analysis. Appl. Physiol. Nutr. Metab. 2024, 49, 273–292. [Google Scholar] [CrossRef]
- Coffey, V.G.; Hawley, J.A. Concurrent exercise training: Do opposites distract? J. Physiol. 2017, 595, 2883–2896. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Bishop, D.J.; Stepto, N.K. Interference between concurrent resistance and endurance exercise: Molecular bases and the role of individual training variables. Sports Med. 2014, 44, 743–762. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Marin, P.J.; Rhea, M.R.; Wilson, S.M.; Loenneke, J.P.; Anderson, J.C. Concurrent training: A meta-analysis examining interference of aerobic and resistance exercises. J. Strength Cond. Res. 2012, 26, 2293–2307. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Feng, X.; Huang, L.; Wang, K.; Mi, J. Comparative efficacy of concurrent training types on lower limb strength and muscular hypertrophy: A systematic review and network meta-analysis. J. Exerc. Sci. Fit. 2024, 22, 86–96. [Google Scholar] [CrossRef]
- Eddens, L.; van Someren, K.; Howatson, G. The role of intra-session exercise sequence in the interference effect: A systematic review with meta-analysis. Sports Med. 2018, 48, 177–188. [Google Scholar] [CrossRef]
- Gao, J.; Yu, L. Effects of concurrent training sequence on VO2max and lower limb strength performance: A systematic review and meta-analysis. Front. Physiol. 2023, 14, 1072679. [Google Scholar] [CrossRef]
- Saghaei, M.; Saghaei, S. Implementation of an open-source customizable minimization program for allocation of patients to parallel groups in clinical trials. J. Biomed. Sci. Eng. 2011, 4, 734–739. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 26–27. [Google Scholar]
- Tholl, U.; Lüders, S.; Bramlage, P.; Dechend, R.; Eckert, S.; Mengden, T.; Nürnberger, J.; Sanner, B.; Anlauf, M. The German Hypertension League (Deutsche Hochdruckliga) Quality Seal Protocol for blood pressure-measuring devices: 15-year experience and results from 105 devices for home blood pressure control. Blood Press. Monit. 2016, 21, 197–205. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Müller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-sensitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Earnest, C.P.; Artero, E.G.; Sui, X.; Lee, D.C.; Church, T.S.; Blair, S.N. Maximal estimated cardiorespiratory fitness, cardiometabolic risk factors, and metabolic syndrome in the aerobics center longitudinal study. Mayo Clin. Proc. 2013, 88, 259–270. [Google Scholar] [CrossRef]
- Johnson, J.L.; Slentz, C.A.; Houmard, J.A.; Samsa, G.P.; Duscha, B.D.; Aiken, L.B.; McCartney, J.S.; Tanner, C.J.; Kraus, W.E. Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise). Am. J. Cardiol. 2007, 100, 1759–1766. [Google Scholar] [CrossRef]
- Meyer, T.; Lucía, A.; Earnest, C.P.; Kindermann, W. A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters--theory and application. Int. J. Sports Med. 2005, 26 (Suppl. 1), S38–S48. [Google Scholar] [CrossRef]
- Howley, E.T.; Bassett, D.R., Jr.; Welch, H.G. Criteria for maximal oxygen uptake: Review and commentary. Med. Sci. Sports Exerc. 1995, 27, 1292–1301. [Google Scholar] [CrossRef]
- Borg, G. Ratings of perceived exertion and heart rates during shortterm cycle exercise and their use in a new cycling strength test. Int. J. Sports Med. 1982, 3, 153–158. [Google Scholar] [CrossRef]
- Reynolds, J.M.; Gordon, T.J.; Robergs, R.A. Prediction of one repetition maximum strength from multiple repetition maximum testing and anthropometry. J. Strength Cond. Res. 2006, 20, 584–592. [Google Scholar]
- Dohoney, P.; Chromiak, J.A.; Lemire, D.; Abadie, B.R.; Kovacs, C. Prediction of one repetition maximum (1-RM) strength from a 4–6 RManda7–10RMsubmaximalstrength test in healthy young adult males. J. Exerc. Physiol. Online 2002, 5, 54–59. [Google Scholar]
- Brzycki, M. Strength testing: Predicting a one-rep max from repetitions to fatigue. J. Phys. Educ. Recreat. Danc. 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Al-Nimr, R.I. Optimal protein intake during weight loss interventions in older adults with obesity. J. Nutr. Gerontol. Geriatr. 2019, 38, 50–68. [Google Scholar] [CrossRef]
- Reljic, D.; Wittmann, F.; Fischer, J.E. Effects of low-volume high-intensity interval training in a community setting: A pilot study. Eur. J. Appl. Physiol. 2018, 118, 1153–1167. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Delgado-Floody, P.; Soriano-Maldonado, A.; Rodríguez-Pérez, M.A.; Latorre-Román, P.Á.; Martínez-Salazar, C.; Vargas, C.A.; Caamaño-Navarrete, F.; Jerez-Mayorga, D.; Álvarez, C. The effects of two different concurrent training configurations on markers of metabolic syndrome and fitness in women with severe/morbid obesity: A randomised controlled trial. Front. Physiol. 2021, 12, 694798. [Google Scholar] [CrossRef]
- Greenway, F. Physiological adaptations to weight loss and factors favouring weight regain. Int. J. Obes. 2015, 39, 1188–1196. [Google Scholar] [CrossRef]
- Sundfør, T.M.; Svendsen, M.; Tonstad, S. Effect of intermittent versus continuous energy restriction on weight loss, maintenance and cardiometabolic risk: A randomized 1-year trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, N.V.; Schoeller, D.; Brown, A.W.; Heymsfield, S.B.; Thomas, D.; Sørensen, T.I.; Speakman, J.R.; Jeansonne, M.; Allison, D.B.; Energy Balance Measurement Working Group. Energy balance measurement: When something is not better than nothing. Int. J. Obes. 2015, 39, 1109–1113. [Google Scholar] [CrossRef]
- Lichtman, S.W.; Pisarska, K.; Berman, E.R.; Pestone, M.; Dowling, H.; Offenbacher, E.; Weisel, H.; Heshka, S.; Matthews, D.E.; Heymsfield, S.B. Discrepancy between self-reported and actual caloric intake and exercise in obese subjects. N. Engl. J. Med. 1992, 327, 1893–1898. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133 (Suppl. 3), 895S–920S. [Google Scholar] [CrossRef]
- Tremblay, A.; Royer, M.M.; Chaput, J.P.; Doucet, E. Adaptive thermogenesis can make a difference in the ability of obese individuals to lose body weight. Int. J. Obes. 2013, 37, 759–764. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The role of exercise and physical activity in weight loss and maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef]
- Keating, S.E.; Johnson, N.A.; Mielke, G.I.; Coombes, J.S. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes. Rev. 2017, 18, 943–964. [Google Scholar] [CrossRef]
- Willert, S.; von Stengel, S.; Kohl, M.; Uder, M.; Kemmler, W. Effects of whole-body electromyostimulation and lifestyle modifications on the metabolic syndrome in premenopausal overweight women. A randomized controlled trials. Dtsch. Z. Sportmed. 2024, 75, 72–78. [Google Scholar] [CrossRef]
- De Koning, L.; Merchant, A.T.; Pogue, J.; Anand, S.S. Waist circumference and waist-to-hip ratio as predictors of cardiovascular events: Meta-regression analysis of prospective studies. Eur. Heart J. 2007, 28, 850–856. [Google Scholar] [CrossRef]
- Mulligan, A.A.; Lentjes, M.A.; Luben, R.N.; Wareham, N.J.; Khaw, K.T. Changes in waist circumference and risk of all-cause and CVD mortality: Results from the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) cohort study. BMC Cardiovasc. Disord. 2019, 19, 238. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, R.; Robinson, I.; Moradi, S.; Purcell, J.; Schwab, E.; Silva, T.; Baker, B.; Camera, D.M. Muscle protein synthesis responses following aerobic-based exercise or high-intensity interval training with or without protein ingestion: A systematic review. Sports Med. 2022, 52, 2713–2732. [Google Scholar] [CrossRef]
- Witard, O.C.; Bannock, L.; Tipton, K.D. Making sense of muscle protein synthesis: A focus on muscle growth during resistance training. Int. J. Sport Nutr. Exerc. Metab. 2022, 32, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Wedig, I.J.; Sallis, R.E.; Lavie, C.J.; Elmer, S.J. Physical activity and cardiorespiratory fitness as modulators of health outcomes: A compelling research-based case presented to the medical community. Mayo Clin. Proc. 2023, 98, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.L.; Rezende, L.F.M.; Lee, D.H. Muscle-strengthening activities and risk of cardiovascular disease, type 2 diabetes, cancer and mortality: A review of prospective cohort studies. J. Intern. Med. 2021, 290, 789–805. [Google Scholar] [CrossRef]
- Kavanagh, T.; Mertens, D.J.; Hamm, L.F.; Beyene, J.; Kennedy, J.; Corey, P.; Shephard, R.J. Prediction of long-term prognosis in 12 169 men referred for cardiac rehabilitation. Circulation 2002, 106, 666–671. [Google Scholar] [CrossRef]
- Mora, S.; Redberg, R.F.; Cui, Y.; Whiteman, M.K.; Flaws, J.A.; Sharrett, A.R.; Blumenthal, R.S. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: A 20-year follow-up of the lipid research clinics prevalence study. JAMA 2003, 290, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Seals, D.R. Endurance exercise performance in Masters athletes: Age-associated changes and underlying physiological mechanisms. J. Physiol. 2008, 586, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Androulakis-Korakakis, P.; Fisher, J.P.; Steele, J. The minimum effective training dose required to increase 1RM strength in resistance-trained men: A systematic review and meta-analysis. Sports Med. 2020, 50, 751–765. [Google Scholar] [CrossRef]
- Fyfe, J.J.; Hamilton, D.L.; Daly, R.M. Minimal-dose resistance training for improving muscle mass, strength, and function: A narrative review of current evidence and practical considerations. Sports Med. 2022, 52, 463–479. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Lampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scand. J. Med. Sci. Sports 2019, 29, 1288–1304. [Google Scholar] [CrossRef]
- Hussain, R.N.; Shari, M.; Radzi, N.A.; Adnan, M.A. Comparison between traditional resistance training and whole-body electrical stimulation in improving muscular strength. Malays. J. Mov. Health Exerc. 2021, 10, 77–83. [Google Scholar] [CrossRef]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009, 338, b1665. [Google Scholar] [CrossRef] [PubMed]
- Blood Pressure Lowering Treatment Trialists’ Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M.; et al. Resting heart rate in cardiovascular disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Canakinumab for residual inflammatory risk. Eur. Heart J. 2017, 38, 3545–3548. [Google Scholar] [CrossRef]
- Ramos-Nino, M.E. The role of chronic inflammation in obesity-associated cancers. ISRN Oncol. 2013, 2013, 697521. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.T.; Wareham, N.; Luben, R.; Bingham, S.; Oakes, S.; Welch, A.; Day, N. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of european prospective investigation of cancer and nutrition (EPIC-Norfolk). BMJ 2001, 322, 15–158. [Google Scholar] [CrossRef] [PubMed]
- Drexel, H.; Tamargo, J.; Kaski, J.C.; Lewis, B.S.; Saely, C.H.; Fraunberger, P.; Dobrev, D.; Komiyama, M.; Plattner, T.; Agewall, S.; et al. Triglycerides revisited: Is hypertriglyceridaemia a necessary therapeutic target in cardiovascular disease? Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 570–582. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, M.; Wang, R.; Jiang, J.; Hu, Y.; Wang, W.; Wang, Y.; Li, H. The predictive value of the hs-CRP/HDL-C ratio, an inflammation-lipid composite marker, for cardiovascular disease in middle-aged and elderly people: Evidence from a large national cohort study. Lipids Health Dis. 2024, 23, 66. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H.; Coeckelberghs, E.; Vanhees, L. Impact of resistance training on blood pressure and other cardiovascular risk factors: A meta-analysis of randomized, controlled trials. Hypertension 2011, 58, 950–958. [Google Scholar] [CrossRef]
- Cheng, X.; Yang, Z. Effect of resistance training on inflammatory markers in middle-aged and older adults: A meta-analysis. Arch. Gerontol. Geriatr. 2024, 126, 105536. [Google Scholar] [CrossRef] [PubMed]
- Ashton, R.E.; Tew, G.A.; Aning, J.J.; Gilbert, S.E.; Lewis, L.; Saxton, J.M. Effects of short-term, medium-term and long-term resistance exercise training on cardiometabolic health outcomes in adults: Systematic review with meta-analysis. Br. J. Sports Med. 2020, 54, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernández-González, V.; Reverter-Masia, J. Effects of whole-body ELECTROMYOSTIMULATION on health and performance: A systematic review. BMC Complement. Altern. Med. 2019, 19, 87. [Google Scholar] [CrossRef]
- Gonzalo-Encabo, P.; Maldonado, G.; Valadés, D.; Ferragut, C.; Pérez-López, A. The role of exercise training on low-grade systemic inflammation in adults with overweight and obesity: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 13258. [Google Scholar] [CrossRef] [PubMed]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef] [PubMed]
- van Baak, M.A.; Pramono, A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of different types of regular exercise on physical fitness in adults with overweight or obesity: Systematic review and meta-analyses. Obes. Rev. 2021, 22 (Suppl. 4), e13239. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | LOW-HIIT+ WB-EMS (n = 30) | WB-EMS+ LOW-HIIT (n = 31) | LOW-HIIT+ 1-RT (n = 30) | 1-RT+ LOW-HIIT (n = 30) |
|---|---|---|---|---|
| Age (years) | 50.8 ± 11.5 | 48.4 ± 13.6 | 50.8 ± 10.0 | 50.1 ± 11.0 |
| Gender, male/female (n) | 12/18 | 11/20 | 14/16 | 12/18 |
| BMI (kg/m2) | 37.8 ± 5.6 | 39.3 ± 5.4 | 38.4 ± 7.8 | 38.2 ± 6.5 |
| MetS z-score | 2.10 ± 2.35 | 2.43 ± 3.26 | 2.47 ± 3.47 | 2.36 ± 2.51 |
| VO2max (mL/kg/min) | 20.7 ± 5.5 | 19.9 ± 5.2 | 21.9 ± 6.8 | 21.7 ± 4.7 |
| Fit-score | 40 ± 12 | 39 ± 12 | 41 ± 11 | 40 ± 10 |
| Outcome | LOW-HIIT+ WB-EMS (n = 23) | WB-EMS+ LOW-HIIT (n = 22) | LOW-HIIT+ 1-RT (n = 25) | 1-RT+ LOW-HIIT (n = 23) | ||||
|---|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | Week 0 | Week 12 | Week 0 | Week 12 | |
| Nutrition | ||||||||
| Energy (kcal/d) | 2224 ± 467 | 1901 ± 438 c | 2389 ± 666 | 1966 ± 703 c | 2568 ± 676 | 2174 ± 632 c | 2204 ± 690 | 1720 ± 559 c |
| Protein (g/kg/d) | 0.9 ± 0.3 | 0.9 ± 0.2 | 0.9 ± 0.3 | 0.8 ± 0.3 | 1.1 ± 0.4 | 1.0 ± 0.5 | 0.9 ± 0.3 | 0.8 ± 0.3 |
| Fat (g/kg/d) | 0.9 ± 0.3 | 0.7 ± 0.2 b | 0.9 ± 0.4 | 0.7 ± 0.4 a | 0.9 ± 0.3 | 0.8 ± 0.2 b | 0.8 ± 0.3 | 0.7 ± 0.3 c |
| CHO (g/kg/d) | 2.1 ± 0.5 | 1.7 ± 0.7 b | 2.0 ± 0.7 | 1.7 ± 0.7 a | 2.5 ± 1.0 | 2.0 ± 0.7 c | 2.0 ± 0.6 | 1.7 ± 0.6 b |
| Fibres (g/d) | 26 ± 14 | 26 ± 13 | 21 ± 9 | 20 ± 7 | 25 ± 7 | 23 ± 7 c | 22 ± 9 | 21 ± 8 |
| LOW-HIIT+ WB-EMS (n = 23) | WB-EMS+ LOW-HIIT (n = 22) | |||
|---|---|---|---|---|
| Variable | T-1 | T-2 | T-1 | T-2 |
| Age (years) | 51.3 ± 12.3 | --- | 49.3 ± 14.9 | --- |
| Gender, male/female (n) | 11/12 | --- | 7/15 | --- |
| Anthropometric variables | ||||
| Body weight (kg) | 108.6 ± 17.9 | 107.0 ± 16.6 a | 115.1 ± 23.4 | 113.7 ± 23.4 a |
| Body mass index (kg/m2) | 38.1 ± 5.7 | 37.6 ± 5.3 a | 40.4 ± 5.9 | 39.9 ± 5.9 a |
| Fat mass (kg) | 47.5 ± 12.3 | 46.8 ± 11.3 | 54.4 ± 13.3 | 53.3 ± 12.7 a |
| Body fat (%) | 43.5 ± 7.2 | 43.1 ± 7.0 | 47.0 ± 5.1 | 46.6 ± 5.5 |
| Fat-free mass (kg) | 61.1 ± 11.0 | 60.4 ± 11.3 | 60.7 ± 12.7 | 60.3 ± 13.6 |
| Total body water (L) | 45.5 ± 7.7 | 45.1 ± 8.0 | 45.5 ± 9.2 | 45.1 ± 10.0 |
| Waist circumference (cm) | 114 ± 12 | 113 ± 11 | 116 ± 14 | 114 ± 14 a |
| Blood pressure | ||||
| Systolic blood pressure (mmHg) | 134 ± 15 | 129 ± 13 | 133 ± 14 | 133 ± 13 |
| Diastolic blood pressure (mmHg) | 87 ± 8 | 85 ± 7 | 86 ± 8 | 85 ± 9 |
| MAB (mmHg) | 103 ± 8 | 99 ± 8 | 101 ± 12 | 100 ± 8 |
| Resting heart rate (b/min) | 75 ± 10 | 71 ± 8 a | 75 ± 10 | 74 ± 10 |
| Clinical chemistry | ||||
| CRP (mg/L) | 5.0 ± 3.3 | 3.8 ± 2.0 | 5.4 ± 4.1 | 5.1 ± 3.7 |
| hsCRP (mg/L) | 3.8 ± 2.6 | 2.8 ± 1.6 b | 4.2 ± 3.2 | 3.9 ± 3.0 |
| Glucose (mg/dL) | 106 ± 14 | 108 ± 14 a | 109 ± 21 | 111 ± 23 |
| HbA1c (%) | 5.7 ± 0.5 | 5.7 ± 0.5 | 5.7 ± 0.6 | 5.7 ± 0.6 |
| Insulin (µE/mL) | 18 ± 8 | 17 ± 9 | 20 ± 11 | 22 ± 12 |
| HOMA-IR (units) | 4.6 ± 2.3 | 4.6 ± 2.6 | 5.5 ± 3.7 | 5.7 ± 4.1 |
| Triglycerides (mg/dL) | 139 ± 48 | 160 ± 83 | 135 ± 77 | 126 ± 66 |
| Cholesterol (mg/dL) | 216 ± 35 | 213 ± 34 | 225 ± 42 | 223 ± 43 |
| HDL (mg/dL) | 51 ± 10 | 50 ± 10 | 55 ± 13 | 54 ± 13 |
| LDL (mg/dL) | 144 ± 28 | 140 ± 26 | 147 ± 32 | 148 ± 33 |
| MetS z-score (units) | 2.3 ± 2.2 | 2.7 ± 2.3 | 2.6 ± 3.7 | 2.7 ± 3.7 |
| CPET variables | ||||
| VO2max (L) | 2.23 ± 0.57 | 2.39 ± 0.58 b | 2.17 ± 0.61 | 2.28 ± 0.64 b |
| VO2max (mL/kg/min) | 21.0 ± 5.9 | 22.6 ± 5.5 b | 19.1 ± 5.0 | 20.3 ± 5.2 b |
| Wmax (W) | 159 ± 39 | 181 ± 41 c | 158 ± 41 | 179 ± 48 c |
| WVT (W) | 72 ± 11 | 87 ± 16 c | 70 ± 18 | 85 ± 25 c |
| Muscle strength | ||||
| 1-RM abdominals (kg) | 28 ± 9 | 33 ± 9 c | 27 ± 10 | 32 ± 11 c |
| 1-RM lower back (kg) | 58 ± 26 | 67 ± 30 a | 57 ± 21 | 71 ± 32 c |
| 1-RM chest (kg) | 34 ± 12 | 43 ± 16 c | 36 ± 21 | 44 ± 20 c |
| 1-RM upper back (kg) | 48 ± 10 | 58 ± 12 c | 50 ± 18 | 59 ± 21 c |
| 1-RM legs (kg) | 147 ± 64 | 174 ± 82 c | 128 ± 45 | 150 ± 63 c |
| Fit-score (units) | 42 ± 12 | 49 ± 14 c | 39 ± 12 | 46 ± 16 c |
| LOW-HIIT+ 1-RT (n = 25) | 1-RT+ LOW-HIIT (n = 23) | |||
|---|---|---|---|---|
| Variable | T-1 | T-2 | T-1 | T-2 |
| Age (years) | 51.8 ± 10.0 | --- | 51.5 ± 11.1 | --- |
| Gender, male/female (n) | 11/14 | --- | 10/13 | --- |
| Anthropometric variables | ||||
| Body weight (kg) | 112.1 ± 25.8 | 110.1 ± 26.6 c | 107.4 ± 19.2 | 103.6 ± 19.1 b |
| Body mass index (kg/m2) | 37.8 ± 7.9 | 37.1 ± 8.1 c | 36.2 ± 4.4 | 35.0 ± 4.9 b |
| Fat mass (kg) | 48.7 ± 16.9 | 47.5 ± 17.7 a | 45.1 ± 8.6 | 42.0 ± 10.1 a |
| Body fat (%) | 42.9 ± 9.6 | 42.4 ± 9.7 | 42.2 ± 5.0 | 40.6 ± 6.6 a |
| Fat-free mass (kg) | 63.4 ± 15.5 | 62.6 ± 15.1 | 62.3 ± 13.4 | 61.6 ± 13.3 |
| Total body water (L) | 47.2 ± 11.0 | 46.7 ± 11.0 | 46.6 ± 9.6 | 45.9 ± 9.5 |
| Waist circumference (cm) | 112 ± 17 | 109 ± 18 a | 111 ± 13 | 106 ± 12 c |
| Blood pressure | ||||
| Systolic blood pressure (mmHg) | 136 ± 12 | 129 ± 10 c | 134 ± 13 | 123 ± 10 c |
| Diastolic blood pressure (mmHg) | 89 ± 7 | 83 ± 7 c | 90 ±9 | 82 ± 6 c |
| MAB (mmHg) | 105 ± 6 | 99 ± 7 c | 104 ± 10 | 96 ± 6 c |
| Resting heart rate (b/min) | 74 ± 12 | 71 ± 10 a | 78 ± 10 | 73 ± 11 a |
| Clinical chemistry | ||||
| CRP (mg/L) | 6.8 ± 5.5 | 4.8 ± 4.2 c | 6.0 ± 7.5 | 2.5 ± 1.9 a |
| hsCRP (mg/L) | 5.6 ± 5.0 | 3.6 ± 3.4 c | 4.9 ± 6.8 | 1.8 ± 1.5 a |
| Glucose (mg/dL) | 104 ± 20 | 104 ± 15 | 103 ± 13 | 102 ± 10 |
| HbA1c (%) | 5.6 ± 0.5 | 5.5 ± 0.4 | 5.4 ± 0.8 | 5.2 ± 0.7 a |
| Insulin (µE/mL) | 16 ± 10 | 15 ± 14 | 19 ± 14 | 14 ± 5 b |
| HOMA-IR (units) | 4.3 ± 3.4 | 4.0 ± 4.5 | 5.1 ± 4.6 | 3.5 ± 1.5 a |
| Triglycerides (mg/dL) | 145 ± 56 | 134 ± 49 | 132 ± 67 | 109 ± 46 a |
| Cholesterol (mg/dL) | 232 ± 46 | 229 ± 41 | 225 ± 42 | 223 ± 43 |
| HDL (mg/dL) | 52 ± 7 | 54 ± 6 | 53 ± 13 | 56 ± 16 a |
| LDL (mg/dL) | 155 ± 36 | 155 ± 35 | 143 ± 35 | 137 ± 33 |
| MetS z-score (units) | 2.4 ± 3.5 | 1.0 ± 3.4 c | 1.9 ± 2.4 | 0.1 ± 1.8 c |
| CPET variables | ||||
| VO2max (L) | 2.38 ± 0.65 | 2.54 ± 0.61 b | 2.37 ± 0.48 | 2.57 ± 0.56 b |
| VO2max (mL/kg/min) | 22.0 ± 7.2 | 23.9 ± 6.8 c | 22.8 ± 4.4 | 25.2 ± 4.2 c |
| Wmax (W) | 170 ± 44 | 202 ± 48 c | 179 ± 36 | 207 ± 46 c |
| WVT (W) | 77 ± 22 | 102 ± 27 c | 73 ± 9 | 95 ± 21 c |
| Muscle strength | ||||
| 1-RM abdominals (kg) | 32 ± 13 | 41 ± 14 c | 32 ± 11 | 42 ± 13 c |
| 1-RM lower back (kg) | 59 ± 27 | 80 ± 33 c | 53 ± 17 | 73 ± 27 c |
| 1-RM chest (kg) | 36 ± 16 | 48 ± 21 c | 36 ± 16 | 43 ± 17 c |
| 1-RM upper back (kg) | 49 ± 19 | 62 ± 21 c | 50 ± 18 | 62 ± 18 c |
| 1-RM legs (kg) | 125 ± 38 | 167 ± 63 c | 131 ± 40 | 159 ± 50 c |
| Fit-score (units) | 41 ± 11 | 53 ± 15 c | 41 ± 9 | 50 ± 11 c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Impact of Different Low-Volume Concurrent Training Regimens on Cardiometabolic Health, Inflammation, and Fitness in Obese Metabolic Syndrome Patients. Nutrients 2025, 17, 561. https://doi.org/10.3390/nu17030561
Reljic D, Herrmann HJ, Neurath MF, Zopf Y. Impact of Different Low-Volume Concurrent Training Regimens on Cardiometabolic Health, Inflammation, and Fitness in Obese Metabolic Syndrome Patients. Nutrients. 2025; 17(3):561. https://doi.org/10.3390/nu17030561
Chicago/Turabian StyleReljic, Dejan, Hans Joachim Herrmann, Markus Friedrich Neurath, and Yurdagül Zopf. 2025. "Impact of Different Low-Volume Concurrent Training Regimens on Cardiometabolic Health, Inflammation, and Fitness in Obese Metabolic Syndrome Patients" Nutrients 17, no. 3: 561. https://doi.org/10.3390/nu17030561
APA StyleReljic, D., Herrmann, H. J., Neurath, M. F., & Zopf, Y. (2025). Impact of Different Low-Volume Concurrent Training Regimens on Cardiometabolic Health, Inflammation, and Fitness in Obese Metabolic Syndrome Patients. Nutrients, 17(3), 561. https://doi.org/10.3390/nu17030561