


Effects of the Mediterranean Diet on the Components of Metabolic Syndrome Concerning the Cardiometabolic Risk


Abstract
1. Introduction
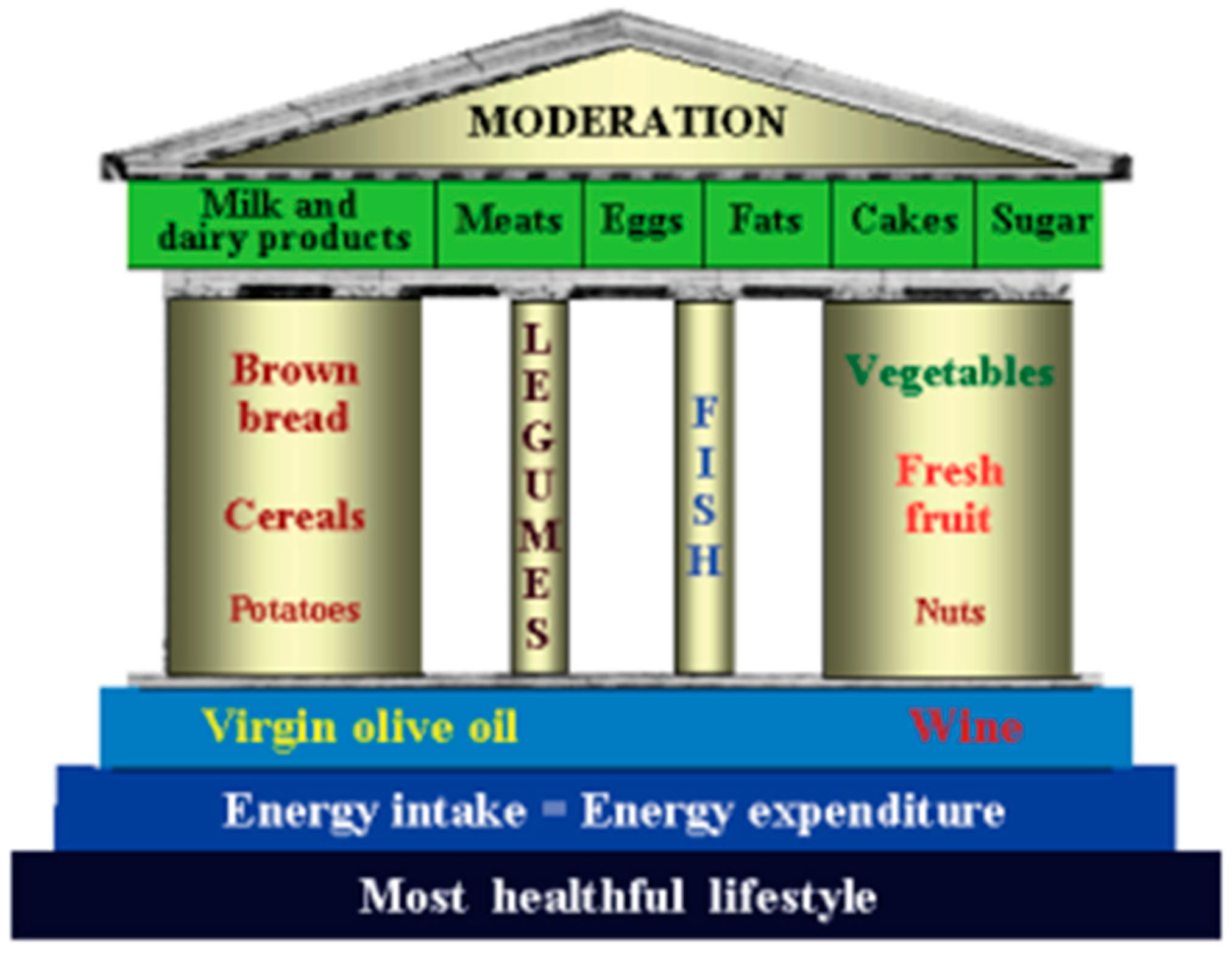
2. Mediterranean Diet from the Past to Now
3. Metabolic Syndrome and Cardiovascular Risk
3.1. History of the Relationship Between Metabolic Syndrome and Cardiovascular Risk
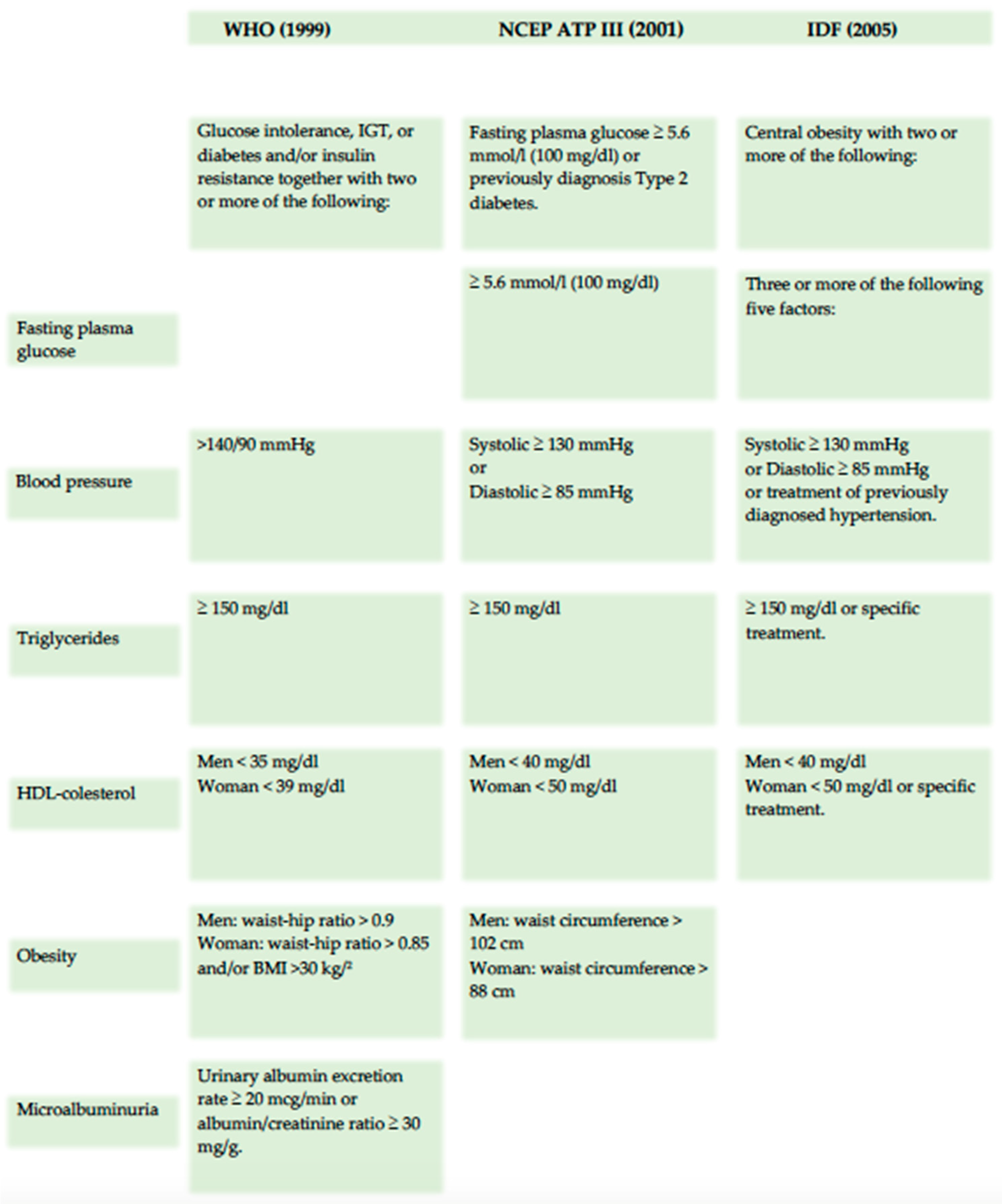
3.2. The Modern Definition of Metabolic Syndrome
3.3. Future Direction of Cardiovascular and Metabolic Diseases
4. Cardiometabolic Risk: The Scores
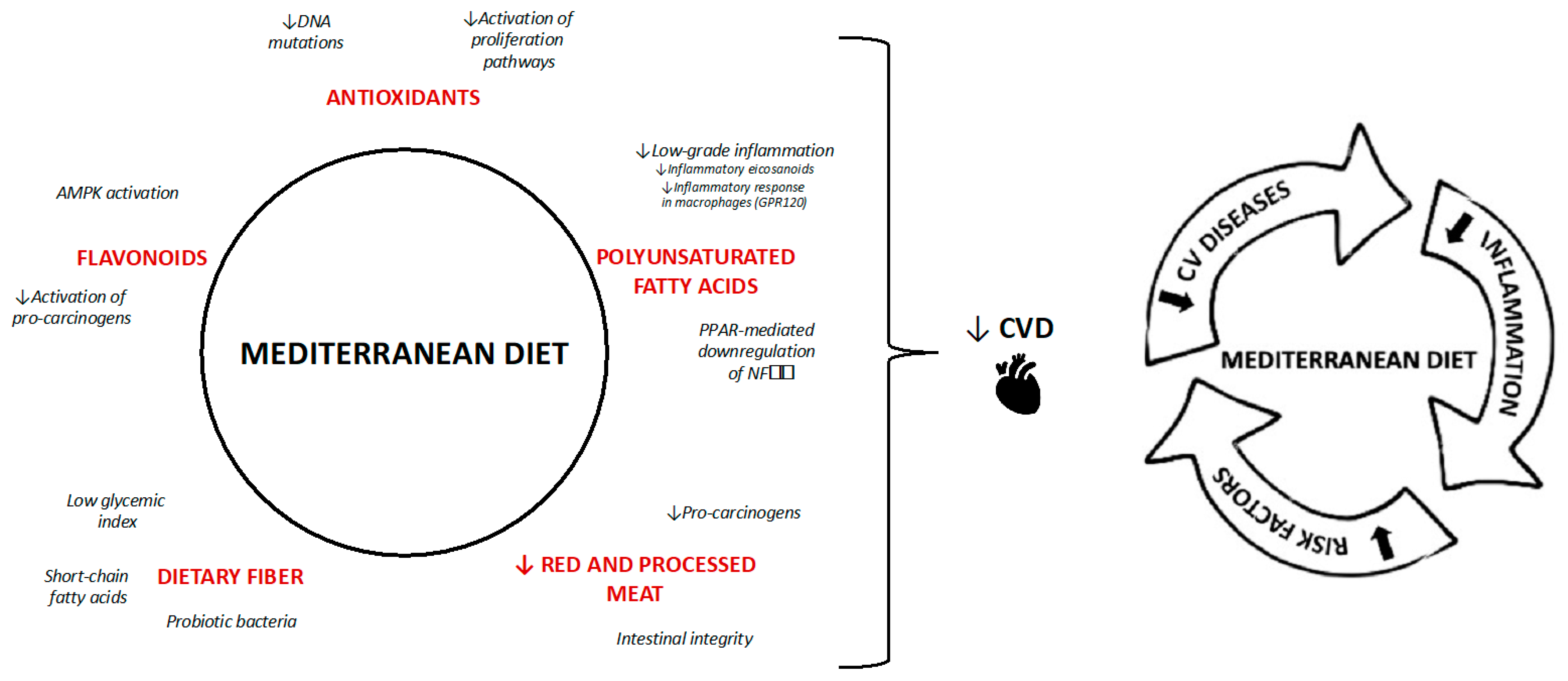
5. Effects of Mediterranean Diet on Cardiovascular Risk Factors and Metabolic Syndrome
5.1. Mediterranean Diet and Diabetes
5.2. Mediterranean Diet and Hypertension
5.3. Mediterranean Diet and Lipid Levels
5.4. Mediterranean Diet and Obesity
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tuttolomondo, A.; Casuccio, A.; Buttà, C.; Pecoraro, R.; Di Raimondo, D.; Della Corte, V.; Arnao, V.; Clemente, G.; Maida, C.; Simonetta, I.; et al. Mediterranean Diet in Patients with Acute Ischemic Stroke: Relationships between Mediterranean Diet Score, Diagnostic Subtype, and Stroke Severity Index. Atherosclerosis 2015, 243, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing Evidence on Benefits of Adherence to the Mediterranean Diet on Health: An Updated Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Babio, N.; Bulló, M.; Salas-Salvadó, J. Mediterranean Diet and Metabolic Syndrome: The Evidence. Public Health Nutr. 2009, 12, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Altomare, R.; Cacciabaudo, F.; Damiano, G.; Palumbo, V.D.; Gioviale, M.C.; Bellavia, M.; Tomasello, G.; Lo Monte, A.I. The mediterranean diet: A history of health. Iran J. Public Health 2013, 42, 449–457. [Google Scholar]
- Ferro-Luzzi, A.; Branca, F. Mediterranean Diet, Italian-Style: Prototype of a Healthy Diet. Am. J. Clin. Nutr. 1995, 61, 1338S–1345S. [Google Scholar] [CrossRef]
- Keys, A.; Menotti, A.; Aravanis, C.; Blackburn, H.; Djordevic, B.S.; Buzina, R.; Dontas, A.S.; Fidanza, F.; Karvonen, M.J.; Kimura, N. The Seven Countries Study: 2289 Deaths in 15 Years. Prev. Med. 1984, 13, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Fidanza, F.; Alberti, A.; Fruttini, D. The Nicotera Diet: The Reference Italian Mediterranean Diet. World Rev. Nutr. Diet. 2005, 95, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Fidanza, F.; Alberti, A. The Healthy Italian Mediterranean Diet Temple Food Guide. Nutr. Today 2005, 40, 71. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Mediterranean Diets: What Is So Special about the Diet of Greece? The Scientific Evidence. J. Nutr. 2001, 131, 3065S–3073S. [Google Scholar] [CrossRef] [PubMed]
- Deckert, T. Historical Aspects of Diabetes and Diabetic Renal Disease. In The Kidney and Hypertension in Diabetes Mellitus; Mogensen, C.E., Ed.; Springer: Boston, MA, USA, 1998; pp. 1–5. ISBN 978-1-4757-6752-0. [Google Scholar]
- Rojas, M.; Chávez-Castillo, M.; Pirela, D.; Parra, H.; Nava, M.; Chacín, M.; Angarita, L.; Añez, R.; Salazar, J.; Ortiz, R.; et al. Metabolic Syndrome: Is It Time to Add the Central Nervous System? Nutrients 2021, 13, 2254. [Google Scholar] [CrossRef] [PubMed]
- Toni, R. La Sindrome Metabolica. L’Endocrinologo 2017, 18, 242–245. [Google Scholar] [CrossRef]
- Himsworth, H.P. Diabetes Mellitus: Its Differentiation into Insulin-Sensitive and Insulin-Insensitive Types. 1936. Int. J. Epidemiol. 2013, 42, 1594–1598. [Google Scholar] [CrossRef] [PubMed]
- Vague, J. The Degree of Masculine Differentiation of Obesities: A Factor Determining Predisposition to Diabetes, Atherosclerosis, Gout, and Uric Calculous Disease. Am. J. Clin. Nutr. 1956, 4, 20–34. [Google Scholar] [CrossRef]
- Reaven, G.M. Banting Lecture 1988. Role of Insulin Resistance in Human Disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, N.M. The Deadly Quartet. Upper-Body Obesity, Glucose Intolerance, Hypertriglyceridemia, and Hypertension. Arch. Intern. Med. 1989, 149, 1514–1520. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E. Insulin Resistance. A Multifaceted Syndrome Responsible for NIDDM, Obesity, Hypertension, Dyslipidemia, and Atherosclerotic Cardiovascular Disease. Diabetes Care 1991, 14, 173–194. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, P.M.; Engström, G.; Hedblad, B. The Metabolic Syndrome and Incidence of Cardiovascular Disease in Non-Diabetic Subjects—A Population-Based Study Comparing Three Different Definitions. Diabet. Med. 2007, 24, 464–472. [Google Scholar] [CrossRef]
- Saely, C.H.; Koch, L.; Schmid, F.; Marte, T.; Aczel, S.; Langer, P.; Hoefle, G.; Drexel, H. Adult Treatment Panel III 2001 but Not International Diabetes Federation 2005 Criteria of the Metabolic Syndrome Predict Clinical Cardiovascular Events in Subjects Who Underwent Coronary Angiography. Diabetes Care 2006, 29, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic Syndrome: Definitions and Controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the Metabolic Syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef]
- Prevalence of Metabolic Syndrome in the United States National Health and Nutrition Examination Survey (Nhanes) 2011–2018. Eur. Heart J. 2021, 42, ehab724.2420. Available online: https://academic.oup.com/eurheartj/article/42/Supplement_1/ehab724.2420/6394450 (accessed on 2 October 2024). [CrossRef]
- Syed, M.A.; Al Nuaimi, A.S.; Latif Zainel, A.J.A.; A/Qotba, H.A. Prevalence of Metabolic Syndrome in Primary Health Settings in Qatar: A Cross Sectional Study. BMC Public Health 2020, 20, 611. [Google Scholar] [CrossRef] [PubMed]
- Naghipour, M.; Joukar, F.; Nikbakht, H.-A.; Hassanipour, S.; Asgharnezhad, M.; Arab-Zozani, M.; Mansour-Ghanaei, F. High Prevalence of Metabolic Syndrome and Its Related Demographic Factors in North of Iran: Results from the PERSIAN Guilan Cohort Study. Int. J. Endocrinol. 2021, 2021, 8862456. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Mistretta, A.; Marventano, S.; Purrello, A.; Vitaglione, P.; Calabrese, G.; Drago, F.; Galvano, F. Beneficial Effects of the Mediterranean Diet on Metabolic Syndrome. Curr. Pharm. Des. 2014, 20, 5039–5044. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. [Google Scholar] [CrossRef]
- Inflammation, Microcalcification, and Increased Expression of Osteopontin Are Histological Hallmarks of Plaque Vulnerability in Patients with Advanced Carotid Artery Stenosis. Available online: https://www.mdpi.com/2227-9059/11/3/881 (accessed on 23 September 2024).
- Beloborodova, N.; Pautova, A.; Grekova, M.; Yadgarov, M.; Grin, O.; Eremenko, A.; Babaev, M. Microbiota Metabolism Failure as a Risk Factor for Postoperative Complications after Aortic Prosthetics. Biomedicines 2023, 11, 1335. [Google Scholar] [CrossRef] [PubMed]
- Kurpas, A.; Supel, K.; Wieczorkiewicz, P.; Bodalska Duleba, J.; Zielinska, M. Fibroblast Growth Factor 23: Potential Marker of Invisible Heart Damage in Diabetic Population. Biomedicines 2023, 11, 1523. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Dawber, T.R.; Kagan, A.; Revotskie, N.; Stokes, J. Factors of Risk in the Development of Coronary Heart Disease—Six-Year Follow-up Experience. Ann. Intern. Med. 1961, 55, 33–50. [Google Scholar] [CrossRef] [PubMed]
- The Relationship of Cigarette Smoking to Coronary Heart Disease: The Second Report of the Combined Experience of the Albany, NY, and Framingham, Mass, Studies. JAMA 1964, 34, 886–890. Available online: https://jamanetwork.com/journals/jama/article-abstract/1165663 (accessed on 1 October 2024).
- II. Coronary Heart Disease in the Framingham Study. Int. J. of Epidemiology 2015, 44, 1767–1780. Available online: https://academic.oup.com/ije/article/44/6/1767/2572749 (accessed on 1 October 2024). [CrossRef] [PubMed]
- The Framingham Study an Epidemiological Approach to Coronary Heart Disease. Circulation 1966, 34, 553–555. Available online: https://www.ahajournals.org/doi/abs/10.1161/01.cir.34.4.553 (accessed on 1 October 2024).
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef]
- Wood, D.; De Backer, G.; Faergeman, O.; Graham, I.; Mancia, G.; Pyörälä, K. Prevention of Coronary Heart Disease in Clinical Practice: Recommendations of the Second Joint Task Force of European and Other Societies on Coronary Prevention. Atherosclerosis 1998, 140, 199–270. [Google Scholar] [CrossRef] [PubMed]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mascaró, C.M.; Montemayor, S.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; Vioque, J.; et al. Leisure-Time Physical Activity, Sedentary Behaviour and Diet Quality Are Associated with Metabolic Syndrome Severity: The PREDIMED-Plus Study. Nutrients 2020, 12, 1013. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef]
- The Relationship Between Smoking Level and Metabolic Syndrome in Male Health Check-up Examinees over 40 Years of Age—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/25309702/ (accessed on 2 October 2024).
- Czech Journal of Food Sciences: Alcohol and Health: Standards of Consumption, Benefits and Harm—A Review. Available online: https://cjfs.agriculturejournals.cz/artkey/cjf-201806-0001_alcohol-and-health-standards-of-consumption-benefits-and-harm-a-review.php (accessed on 2 October 2024).
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, H.E.; Koeller, E.; Greer, N.; MacDonald, R.; Kane, R.; Wilt, T.J. Effects on Health Outcomes of a Mediterranean Diet with No Restriction on Fat Intake: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2016, 165, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Koloverou, E.; Esposito, K.; Giugliano, D.; Panagiotakos, D. The Effect of Mediterranean Diet on the Development of Type 2 Diabetes Mellitus: A Meta-Analysis of 10 Prospective Studies and 136,846 Participants. Metabolism 2014, 63, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Jannasch, F.; Kröger, J.; Schulze, M.B. Dietary Patterns and Type 2 Diabetes: A Systematic Literature Review and Meta-Analysis of Prospective Studies. J. Nutr. 2017, 147, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Missbach, B.; König, J.; Hoffmann, G. Adherence to a Mediterranean Diet and Risk of Diabetes: A Systematic Review and Meta-Analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef]
- Garcia-Lunar, I.; van der Ploeg, H.P.; Fernández Alvira, J.M.; van Nassau, F.; Castellano Vázquez, J.M.; van der Beek, A.J.; Rossello, X.; Fernández-Ortiz, A.; Coffeng, J.; van Dongen, J.M.; et al. Effects of a Comprehensive Lifestyle Intervention on Cardiovascular Health: The TANSNIP-PESA Trial. Eur. Heart J. 2022, 43, 3732–3745. [Google Scholar] [CrossRef]
- Mediterranean Diet Reduces 24-Hour Ambulatory Blood Pressure, Blood Glucose, and Lipids: One-Year Randomized, Clinical Trial—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/24799608/ (accessed on 7 October 2024).
- Al-Qawasmeh, R.H.; Tayyem, R.F. Dietary and Lifestyle Risk Factors and Metabolic Syndrome: Literature Review. Curr. Res. Nutr. Food Sci. J. 2018, 6, 594–608. [Google Scholar] [CrossRef]
- A Western Dietary Pattern Is Prospectively Associated with Cardio-Metabolic Traits and Incidence of the Metabolic Syndrome. Br. J. Nutr. 2018, 119, 1168–1176. Available online: https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/western-dietary-pattern-is-prospectively-associated-with-cardiometabolic-traits-and-incidence-of-the-metabolic-syndrome/27E9CD3FE973847C9EFC120C2CAFFA4B (accessed on 2 October 2024). [CrossRef]
- Strate, L.L.; Keeley, B.R.; Cao, Y.; Wu, K.; Giovannucci, E.L.; Chan, A.T. Western Dietary Pattern Increases, and Prudent Dietary Pattern Decreases, Risk of Incident Diverticulitis in a Prospective Cohort Study. Gastroenterology 2017, 152, 1023–1030.e2. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Espeland, M.A.; Clark, J.M.; Hazuda, H.P.; Knowler, W.C.; Pownall, H.J.; Unick, J.; Wadden, T.; Wagenknecht, L. Action for Health in Diabetes (Look AHEAD) Study Group Association of Weight Loss Maintenance and Weight Regain on 4-Year Changes in CVD Risk Factors: The Action for Health in Diabetes (Look AHEAD) Clinical Trial. Diabetes Care 2016, 39, 1345–1355. [Google Scholar] [CrossRef]
- Ma, C.; Avenell, A.; Bolland, M.; Hudson, J.; Stewart, F.; Robertson, C.; Sharma, P.; Fraser, C.; MacLennan, G. Effects of Weight Loss Interventions for Adults Who Are Obese on Mortality, Cardiovascular Disease, and Cancer: Systematic Review and Meta-Analysis. BMJ 2017, 359, j4849. [Google Scholar] [CrossRef]
- The Importance of Weight Stabilization Amongst Those with Overweight or Obesity: Results from a Large Health Care System—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8684020/ (accessed on 7 October 2024).
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Yubero-Serrano, E.M.; et al. Long-Term Secondary Prevention of Cardiovascular Disease with a Mediterranean Diet and a Low-Fat Diet (CORDIOPREV): A Randomised Controlled Trial. Lancet 2022, 399, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Effect of Citrus Flavonoids, Naringin and Naringenin, on Metabolic Syndrome and Their Mechanisms of Action—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/25022990/ (accessed on 2 October 2024).
- Müller, T.D.; Blüher, M.; Tschöp, M.H.; DiMarchi, R.D. Anti-Obesity Drug Discovery: Advances and Challenges. Nat. Rev. Drug Discov. 2022, 21, 201–223. [Google Scholar] [CrossRef] [PubMed]
- Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa2032183 (accessed on 7 October 2024). [CrossRef] [PubMed]
- Hou, C.-Y.; Tain, Y.-L.; Yu, H.-R.; Huang, L.-T. The Effects of Resveratrol in the Treatment of Metabolic Syndrome. Int. J. Mol. Sci. 2019, 20, 535. [Google Scholar] [CrossRef]
- Liu, K.; Luo, M.; Wei, S. The Bioprotective Effects of Polyphenols on Metabolic Syndrome against Oxidative Stress: Evidences and Perspectives. Oxid. Med. Cell Longev. 2019, 2019, 6713194. [Google Scholar] [CrossRef] [PubMed]
- Kasprzak-Drozd, K.; Oniszczuk, T.; Stasiak, M.; Oniszczuk, A. Beneficial Effects of Phenolic Compounds on Gut Microbiota and Metabolic Syndrome. Int. J. Mol. Sci. 2021, 22, 3715. [Google Scholar] [CrossRef] [PubMed]
- Finicelli, M.; Squillaro, T.; Di Cristo, F.; Di Salle, A.; Melone, M.A.B.; Galderisi, U.; Peluso, G. Metabolic Syndrome, Mediterranean Diet, and Polyphenols: Evidence and Perspectives. J. Cell Physiol. 2019, 234, 5807–5826. [Google Scholar] [CrossRef] [PubMed]
- Rehman, K.; Haider, K.; Jabeen, K.; Akash, M.S.H. Current Perspectives of Oleic Acid: Regulation of Molecular Pathways in Mitochondrial and Endothelial Functioning against Insulin Resistance and Diabetes. Rev. Endocr. Metab. Disord. 2020, 21, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Effects of Oleic Acid. Available online: https://medscidiscovery.com/index.php/msd/article/view/53 (accessed on 2 October 2024).
- Massaro, M.; Scoditti, E.; Carluccio, M.A.; Calabriso, N.; Santarpino, G.; Verri, T.; De Caterina, R. Effects of Olive Oil on Blood Pressure: Epidemiological, Clinical, and Mechanistic Evidence. Nutrients 2020, 12, 1548. [Google Scholar] [CrossRef]
- Poudyal, H.; Panchal, S.K.; Diwan, V.; Brown, L. Omega-3 Fatty Acids and Metabolic Syndrome: Effects and Emerging Mechanisms of Action. Prog. Lipid Res. 2011, 50, 372–387. [Google Scholar] [CrossRef]
- Effect of N-3 (Omega-3) Polyunsaturated Fatty Acid Supplementation on Metabolic and Inflammatory Biomarkers and Body Weight in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of RCTs—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/34822400/ (accessed on 2 October 2024).
- Chen, J.-P.; Chen, G.-C.; Wang, X.-P.; Qin, L.; Bai, Y. Dietary Fiber and Metabolic Syndrome: A Meta-Analysis and Review of Related Mechanisms. Nutrients 2017, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L. Dietary Fiber and Body Weight. Nutrition 2005, 21, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Examining the Effects of Diet Composition, Soluble Fiber, and Species on Total Fecal Excretion of Bile Acids: A Meta-Analysis—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/34692814/ (accessed on 2 October 2024).
- Antioxidants and Exercise Performance: With a Focus on Vitamin E and C Supplementation—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33203106/ (accessed on 2 October 2024).
- Said, E.; Mousa, S.; Fawzi, M.; Sabry, N.A.; Farid, S. Combined Effect of High-Dose Vitamin A, Vitamin E Supplementation, and Zinc on Adult Patients with Diabetes: A Randomized Trial. J. Adv. Res. 2021, 28, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.-F.; Venkatakrishnan, K.; Golovinskaia, O.; Wang, C.-K. Impact of Micronutrients on Hypertension: Evidence from Clinical Trials with a Special Focus on Meta-Analysis. Nutrients 2021, 13, 588. [Google Scholar] [CrossRef]
- Schellenberg, E.S.; Dryden, D.M.; Vandermeer, B.; Ha, C.; Korownyk, C. Lifestyle Interventions for Patients with and at Risk for Type 2 Diabetes: A Systematic Review and Meta- Analysis. Ann. Intern. Med. 2013, 159, 543–551. [Google Scholar] [CrossRef]
- Bendall, C.L.; Mayr, H.L.; Opie, R.S.; Bes-Rastrollo, M.; Itsiopoulos, C.; Thomas, C.J. Central Obesity and the Mediterranean Diet: A Systematic Review of Intervention Trials. Crit. Rev. Food Sci. Nutr. 2018, 58, 3070–3084. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.-I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; et al. Prevention of Diabetes with Mediterranean Diets: A Subgroup Analysis of a Randomized Trial. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef]
- Dieta DASH: Alimentación Saludable Para Disminuir La Presión Arterial—Mayo Clinic. Available online: https://www.mayoclinic.org/es/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/dash-diet/art-20048456 (accessed on 4 October 2024).
- Esposito, K.; Chiodini, P.; Maiorino, M.I.; Bellastella, G.; Panagiotakos, D.; Giugliano, D. Which Diet for Prevention of Type 2 Diabetes? A Meta-Analysis of Prospective Studies. Endocrine 2014, 47, 107–116. [Google Scholar] [CrossRef]
- Chen, Z.; Zuurmond, M.G.; van der Schaft, N.; Nano, J.; Wijnhoven, H.A.H.; Ikram, M.A.; Franco, O.H.; Voortman, T. Plant versus Animal Based Diets and Insulin Resistance, Prediabetes and Type 2 Diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2018, 33, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Tzima, N.; Pitsavos, C.; Chrysohoou, C.; Zampelas, A.; Toussoulis, D.; Stefanadis, C. The Association between Adherence to the Mediterranean Diet and Fasting Indices of Glucose Homoeostasis: The ATTICA Study. J. Am. Coll. Nutr. 2007, 26, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-Style Diet on Cardiovascular Risk Factors: A Randomized Trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, C.; Filesi, C.; Varì, R.; Scazzocchio, B.; Filardi, T.; Fogliano, V.; D’Archivio, M.; Giovannini, C.; Lenzi, A.; Morano, S.; et al. Consumption of Extra-Virgin Olive Oil Rich in Phenolic Compounds Improves Metabolic Control in Patients with Type 2 Diabetes Mellitus: A Possible Involvement of Reduced Levels of Circulating Visfatin. J. Endocrinol. Investig. 2016, 39, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Tierney, A.C.; Roche, H.M. The Potential Role of Olive Oil-Derived MUFA in Insulin Sensitivity. Mol. Nutr. Food Res. 2007, 51, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, M.; Krogh, V.; Freudenheim, J.; Blake, A.; Muti, P.; Panico, S.; Farinaro, E.; Mancini, M.; Menotti, A.; Ricci, G. Consumption of Olive Oil, Butter, and Vegetable Oils and Coronary Heart Disease Risk Factors. The Research Group ATS-RF2 of the Italian National Research Council. JAMA 1990, 263, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of Diabetes Mellitus and Impaired Glucose Regulation in Spain: The Di@bet.Es Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Prospective Studies Collaboration Age-Specific Relevance of Usual Blood Pressure to Vascular Mortality: A Meta- Analysis of Individual Data for One Million Adults in 61 Prospective Studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Rapsomaniki, E.; Timmis, A.; George, J.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; White, I.R.; Caulfield, M.J.; Deanfield, J.E.; Smeeth, L.; et al. Blood Pressure and Incidence of Twelve Cardiovascular Diseases: Lifetime Risks, Healthy Life-Years Lost, and Age-Specific Associations in 1·25 Million People. Lancet 2014, 383, 1899–1911. [Google Scholar] [CrossRef]
- Malik, R.; Georgakis, M.K.; Vujkovic, M.; Damrauer, S.M.; Elliott, P.; Karhunen, V.; Giontella, A.; Fava, C.; Hellwege, J.N.; Shuey, M.M.; et al. Relationship Between Blood Pressure and Incident Cardiovascular Disease: Linear and Nonlinear Mendelian Randomization Analyses. Hypertension 2021, 77, 2004–2013. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, M.; Qi, G.; Bhatt, D.L.; Post, W.S.; Chatterjee, N.; Battle, A.; McEvoy, J.W. Linear and Nonlinear Mendelian Randomization Analyses of the Association Between Diastolic Blood Pressure and Cardiovascular Events: The J-Curve Revisited. Circulation 2021, 143, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Bhatt, D.L.; Catapano, A.L.; Packard, C.J.; Graham, I.; Kaptoge, S.; Ference, T.B.; Guo, Q.; Laufs, U.; Ruff, C.T.; et al. Association of Genetic Variants Related to Combined Exposure to Lower Low-Density Lipoproteins and Lower Systolic Blood Pressure With Lifetime Risk of Cardiovascular Disease. JAMA 2019, 322, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Risk-Factor Clustering and Cardiovascular Disease Risk in Hypertensive Patients—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/17531915/ (accessed on 4 October 2024).
- Kannel, W.B. Risk Stratification in Hypertension: New Insights from the Framingham Study. Am. J. Hypertens. 2000, 13, 3S–10S. [Google Scholar] [CrossRef] [PubMed]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood Pressure Lowering for Prevention of Cardiovascular Disease and Death: A Systematic Review and Meta-Analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Sundström, J.; Arima, H.; Jackson, R.; Turnbull, F.; Rahimi, K.; Chalmers, J.; Woodward, M.; Neal, B. Blood Pressure Lowering Treatment Trialists’ Collaboration Effects of Blood Pressure Reduction in Mild Hypertension: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2015, 162, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Blood Pressure Lowering Treatment Trialists’ Collaboration Pharmacological Blood Pressure Lowering for Primary and Secondary Prevention of Cardiovascular Disease across Different Levels of Blood Pressure: An Individual Participant-Level Data Meta-Analysis. Lancet 2021, 397, 1625–1636. [CrossRef] [PubMed]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef]
- Moore, K.J.; Sheedy, F.J.; Fisher, E.A. Macrophages in Atherosclerosis: A Dynamic Balance. Nat. Rev. Immunol. 2013, 13, 709–721. [Google Scholar] [CrossRef]
- Candás-Estébanez, B.; Fernández-Cidón, B.; Corbella, E.; Tebé, C.; Fanlo-Maresma, M.; Esteve-Luque, V.; Salas-Salvadó, J.; Fitó, M.; Riera-Mestre, A.; Ros, E.; et al. The Impact of the Mediterranean Diet and Lifestyle Intervention on Lipoprotein Subclass Profiles among Metabolic Syndrome Patients: Findings of a Randomized Controlled Trial. Int. J. Mol. Sci. 2024, 25, 1338. [Google Scholar] [CrossRef] [PubMed]
- Andreo-López, M.C.; Contreras-Bolívar, V.; Muñoz-Torres, M.; García-Fontana, B.; García-Fontana, C. Influence of the Mediterranean Diet on Healthy Aging. Int. J. Mol. Sci. 2023, 24, 4491. [Google Scholar] [CrossRef] [PubMed]
- Altamimi, M.; Zidan, S.; Badrasawi, M. Effect of Tree Nuts Consumption on Serum Lipid Profile in Hyperlipidemic Individuals: A Systematic Review. Nutr. Metab. Insights 2020, 13, 1178638820926521. [Google Scholar] [CrossRef] [PubMed]
- Akinloye, O.A.; Akinloye, D.I.; Onigbinde, S.B.; Metibemu, D.S. Phytosterols Demonstrate Selective Inhibition of COX-2: In-Vivo and in-Silico Studies of Nicotiana Tabacum. Bioorg. Chem. 2020, 102, 104037. [Google Scholar] [CrossRef]
- Allaire, J.; Couture, P.; Leclerc, M.; Charest, A.; Marin, J.; Lépine, M.-C.; Talbot, D.; Tchernof, A.; Lamarche, B. A Randomized, Crossover, Head-to-Head Comparison of Eicosapentaenoic Acid and Docosahexaenoic Acid Supplementation to Reduce Inflammation Markers in Men and Women: The Comparing EPA to DHA (ComparED) Study. Am. J. Clin. Nutr. 2016, 104, 280–287. [Google Scholar] [CrossRef]
- ovitamin A Carotenoids and Immune Function. Request PDF. Available online: https://www.researchgate.net/publication/302102324_Provitamin_A_Carotenoids_and_Immune_Function (accessed on 7 October 2024).
- Gammone, M.A.; Riccioni, G.; D’Orazio, N. Carotenoids: Potential Allies of Cardiovascular Health? Food Nutr. Res. 2015, 59, 26762. [Google Scholar] [CrossRef]
- Damasceno, N.R.; Sala-Vila, A.; Cofán, M.; Pérez-Heras, A.M.; Fitó, M.; Ruiz-Gutiérrez, V.; Martínez-González, M.Á..; Corella, D.; Arós, F.; Estruch, R.; et al. Mediterranean Diet Supplemented with Nuts Reduces Waist Circumference and Shifts Lipoprotein Subfractions to a Less Atherogenic Pattern in Subjects at High Cardiovascular Risk. Atherosclerosis 2013, 230, 347–353. [Google Scholar] [CrossRef]
- Visceral Obesity: The Link Among Inflammation, Hypertension, and Cardiovascular Disease—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/19237685/ (accessed on 7 October 2024).
- Neter, J.E.; Stam, B.E.; Kok, F.J.; Grobbee, D.E.; Geleijnse, J.M. Influence of Weight Reduction on Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. Hypertension 2003, 42, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Weight Loss and Risk Reduction of Obesity-Related Outcomes in 0.5 Million People: Evidence from a UK Primary Care Database—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33658682/ (accessed on 7 October 2024).
- Moore, L.L.; Visioni, A.J.; Qureshi, M.M.; Bradlee, M.L.; Ellison, R.C.; D’Agostino, R. Weight Loss in Overweight Adults and the Long-Term Risk of Hypertension: The Framingham Study. Arch. Intern. Med. 2005, 165, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, R.; Di Chiara, T.; Cariello, T.; Licata, G. Visceral Obesity and Metabolic Syndrome: Two Faces of the Same Medal? Intern. Emerg. Med. 2010, 5, 111–119. [Google Scholar] [CrossRef]
- Zomer, E.; Gurusamy, K.; Leach, R.; Trimmer, C.; Lobstein, T.; Morris, S.; James, W.P.T.; Finer, N. Interventions That Cause Weight Loss and the Impact on Cardiovascular Risk Factors: A Systematic Review and Meta-Analysis. Obes. Rev. 2016, 17, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.; Færch, L.; Jeppesen, O.K.; Pakseresht, A.; Pedersen, S.D.; Perreault, L.; Rosenstock, J.; Shimomura, I.; Viljoen, A.; Wadden, T.A.; et al. Semaglutide 2·4 Mg Once a Week in Adults with Overweight or Obesity, and Type 2 Diabetes (STEP 2): A Randomised, Double-Blind, Double-Dummy, Placebo-Controlled, Phase 3 Trial. Lancet 2021, 397, 971–984. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Foods of the Mediterranean Diet |
|---|
| vegetables |
| fruits |
| extra virgin olive oil |
| wholegrain breads and cereals |
| legumes or beans |
| low-fat dairy |
| poultry |
| fish |
| nuts and seeds |
| fish and seafood |
| onion, garlic and other herbs and spices (e.g., oregano, coriander, cumin, etc.) |
| Mediterranean-Style Major Bioactives/Nutrients |
|---|
| Dietary fibers |
| Increased ratio of MUFA to SFA |
| Antioxidants |
| Zn |
| Iodine |
| Mg |
| Fe |
| Calcium |
| Vitamin B12 |
| Vitamin B6 |
| Vitamin B3 |
| Vitamin B2 |
| Vitamin B1 |
| Vitamin A |
| Vitamin C |
| Vitamin D |
| Vitamin E |
| Vitamin A |
| Se |
| Folic acid |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaglione, S.; Di Chiara, T.; Daidone, M.; Tuttolomondo, A. Effects of the Mediterranean Diet on the Components of Metabolic Syndrome Concerning the Cardiometabolic Risk. Nutrients 2025, 17, 358. https://doi.org/10.3390/nu17020358
Scaglione S, Di Chiara T, Daidone M, Tuttolomondo A. Effects of the Mediterranean Diet on the Components of Metabolic Syndrome Concerning the Cardiometabolic Risk. Nutrients. 2025; 17(2):358. https://doi.org/10.3390/nu17020358
Chicago/Turabian StyleScaglione, Stefania, Tiziana Di Chiara, Mario Daidone, and Antonino Tuttolomondo. 2025. "Effects of the Mediterranean Diet on the Components of Metabolic Syndrome Concerning the Cardiometabolic Risk" Nutrients 17, no. 2: 358. https://doi.org/10.3390/nu17020358
APA StyleScaglione, S., Di Chiara, T., Daidone, M., & Tuttolomondo, A. (2025). Effects of the Mediterranean Diet on the Components of Metabolic Syndrome Concerning the Cardiometabolic Risk. Nutrients, 17(2), 358. https://doi.org/10.3390/nu17020358