
Endocannabinoid and AGE Interactions in Prediabetes: The Role of Mediterranean Diet Adherence


 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
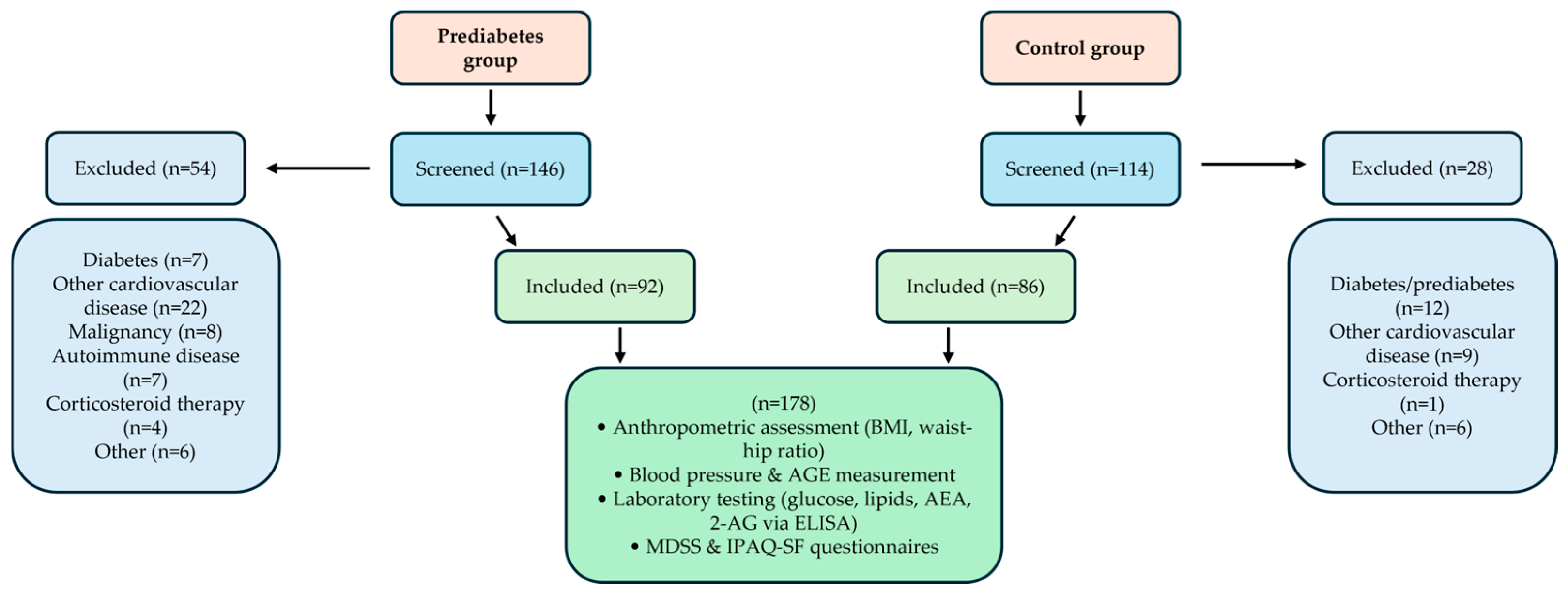
2.1. Study Design and Ethical Considerations
2.2. Participants
2.3. Anthropometric Measurements
2.4. Arterial Blood Pressure and Advanced Glycation End Products (AGEs)
2.5. Laboratory Evaluations
2.6. IPAQ-SF and MDSS Survey
2.7. Statistical Analysis
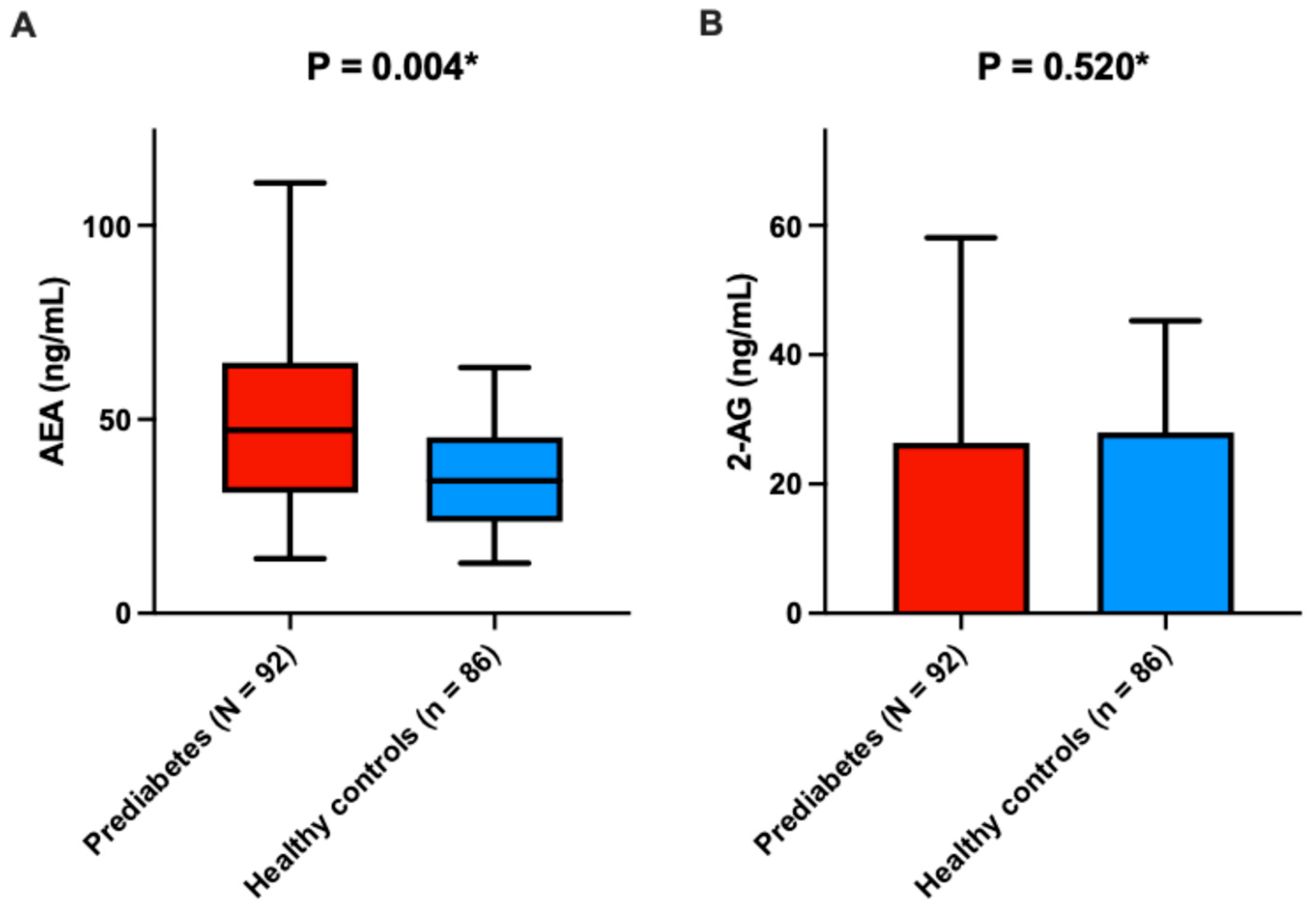
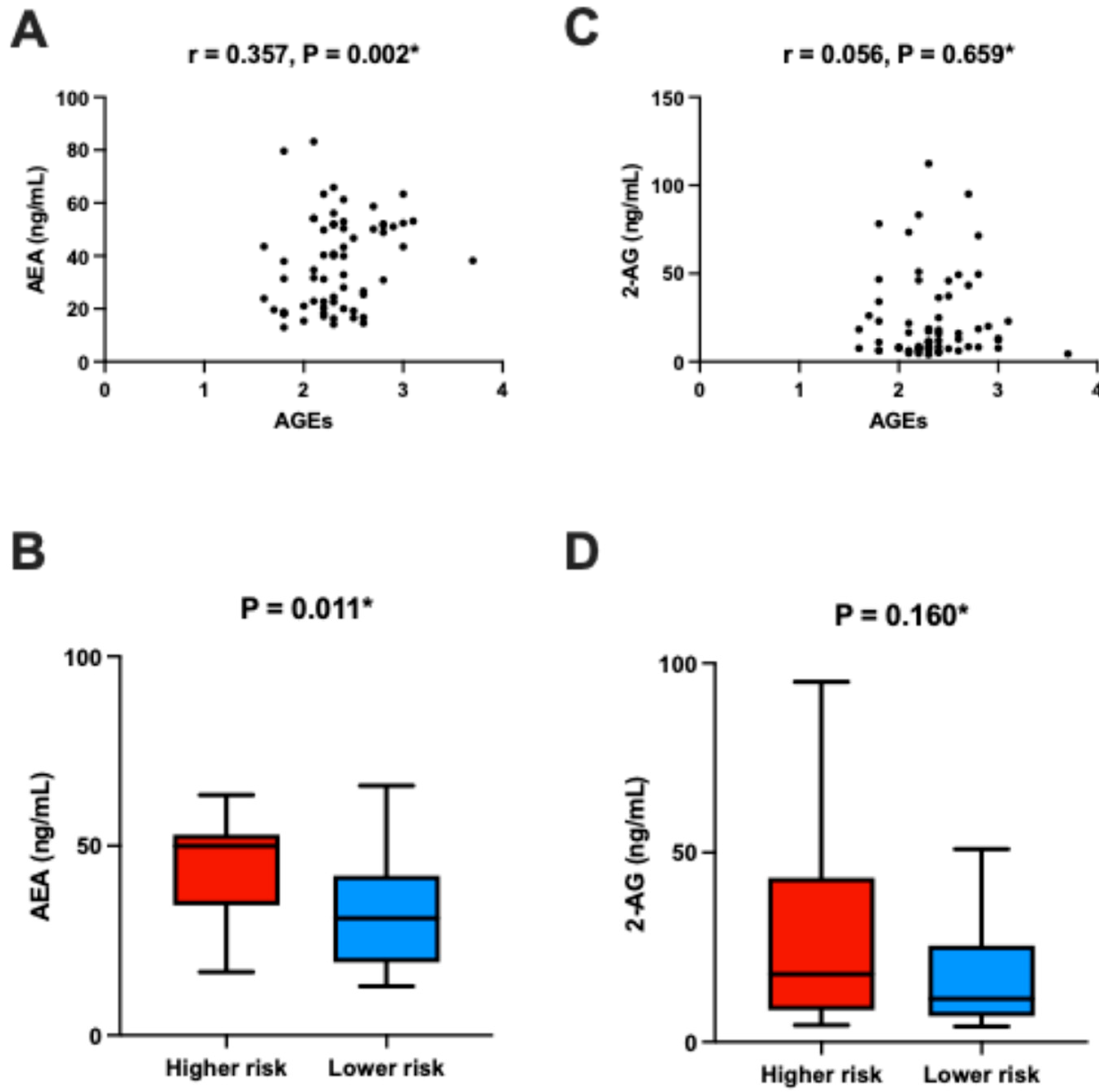
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Parameters | AEA (ng/mL) | 2-AG (ng/mL) | ||
|---|---|---|---|---|
| r—Correlation Coefficient * | p | r—Correlation Coefficient * | p | |
| Age (years) | 0.304 | <0.001 | −0.101 | 0.180 |
| BMI (kg/m2) | 0.147 | 0.050 | 0.231 | 0.002 |
| WHR | 0.065 | 0.389 | 0.124 | 0.099 |
| Body fat, % | 0.101 | 0.180 | 0.234 | 0.002 |
| Visceral fat, % | 0.045 | 0.551 | 0.121 | 0.108 |
| Systolic BP (mmHg) | 0.065 | 0.389 | 0.064 | 0.396 |
| Diastolic BP (mmHg) | −0.185 | 0.013 | −0.195 | 0.009 |
| Fasting plasma glucose (mmol/L) | −0.323 | <0.001 | −0.085 | 0.259 |
| Total cholesterol (mmol/L) | 0.034 | 0.652 | −0.094 | 0.212 |
| LDL-C (mmol/L) | −0.095 | 0.207 | 0.016 | 0.832 |
| HDL-C (mmol/L) | 0.211 | 0.005 | −0.341 | <0.001 |
| Triglycerides (mmol/L) | 0.114 | 0.130 | 0.056 | 0.458 |
| Creatinine (mmol/L) | 0.214 | 0.004 | −0.105 | 0.163 |
| IPAQ-SF (MET-min/week) | −0.089 | 0.237 | 0.312 | <0.001 |
| MDSS (points) | −0.203 | 0.007 | 0.062 | 0.437 |
References
- ElSayes, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Rooney, M.R.; Fang, M.; Ogurtsova, K.; Ozkan, B.; Echouffo-Tcheugui, J.B.; Boyko, E.J.; Magliano, D.J.; Selvin, E. Global prevalence of prediabetes. Diabetes Care 2023, 46, 1388–1394. [Google Scholar] [CrossRef]
- Huang, Z.; Wang, F.; Xiao, X.; Liu, D.; Deng, Z. Non-linear relationship between pulse pressure and the risk of prediabetes: A 5-year cohort study in Chinese adults. Sci. Rep. 2024, 14, 3824. [Google Scholar] [CrossRef]
- Liu, J.; Pan, S.; Wang, X.; Liu, Z.; Zhang, Y. Role of advanced glycation end products in diabetic vascular injury: Molecular mechanisms and therapeutic perspectives. Eur. J. Med. Res. 2023, 28, 553. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef]
- Silvestri, C.; Di Marzo, V. The endocannabinoid system in energy homeostasis and the etiopathology of metabolic disorders. Cell Metab. 2013, 17, 475–490. [Google Scholar] [CrossRef]
- Barrie, N.; Manolios, N. The endocannabinoid system in pain and inflammation: Its relevance to rheumatic disease. Eur. J. Rheumatol. 2017, 4, 210–218. [Google Scholar] [CrossRef]
- Kaczocha, M.; Haj-Dahmane, S. Mechanisms of endocannabinoid transport in the brain. Br. J. Pharmacol. 2022, 179, 4300–4310. [Google Scholar] [CrossRef]
- Pagotto, U.; Marsicano, G.; Cota, D.; Lutz, B.; Pasquali, R. The emerging role of the endocannabinoid system in endocrine regulation and energy balance. Endocr. Rev. 2006, 27, 73–100. [Google Scholar] [CrossRef]
- Dörnyei, G.; Vass, Z.; Juhász, C.B.; Nádasy, G.L.; Hunyady, L.; Szekeres, M. Role of the Endocannabinoid system in metabolic control processes and in the pathogenesis of metabolic syndrome: An update. Biomedicines 2023, 11, 306. [Google Scholar] [CrossRef]
- Gruden, G.; Barutta, F.; Kunos, G.; Pacher, P. Role of the endocannabinoid system in diabetes and diabetic complications. Br. J. Pharmacol. 2016, 173, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, M.; Bátkai, S.; Kechrid, M.; Mukhopadhyay, P.; Lee, W.S.; Horváth, B.; Holovac, E.; Cinar, R.; Liaudet, L.; Mackie, K.; et al. Cannabinoid 1 receptor promotes cardiac dysfunction, oxidative stress, inflammation, and fibrosis in diabetic cardiomyopathy. Diabetes 2012, 61, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Vasincu, A.; Rusu, R.-N.; Ababei, D.-C.; Neamțu, M.; Arcan, O.D.; Macadan, I.; Chiriac, S.B.; Bild, W.; Bild, V. Exploring the Therapeutic potential of cannabinoid receptor antagonists in inflammation, diabetes mellitus, and obesity. Biomedicines 2023, 11, 1667. [Google Scholar] [CrossRef]
- Matias, I.; Di Marzo, V. Endocannabinoids and the control of energy balance. Trends Endocrinol. Metab. 2007, 18, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Hashiesh, H.M.; Azimullah, S.; Meeran, M.F.N.; Saraswathiamma, D.; Arunachalam, S.; Jha, N.K.; Sadek, B.; Adeghate, E.; Sethi, G.; Albawardi, A.; et al. Cannabinoid 2 receptor activation protects against diabetic cardiomyopathy through inhibition of AGE/RAGE-Induced oxidative stress, fibrosis, and inflammasome activation. J. Pharmacol. Exp. Ther. 2024, 391, 241–257. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Grahovac, M.; Kumric, M.; Vilovic, M.; Martinovic, D.; Kreso, A.; Kurir, T.T.; Vrdoljak, J.; Prizmic, K.; Božić, J. Adherence to Mediterranean diet and advanced glycation endproducts in patients with diabetes. World J. Diabetes 2021, 12, 1942–1956. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef]
- Alvheim, A.R.; Malde, M.K.; Osei-Hyiaman, D.; Hong, Y.H.; Pawlosky, R.J.; Madsen, L.; Kristiansen, K.; Frøyland, L.; Hibbeln, J.R. Dietary linoleic acid elevates endogenous 2-AG and anandamide and induces obesity. Obesity 2012, 20, 1984–1994. [Google Scholar] [CrossRef]
- Artmann, A.; Petersen, G.; Hellgren, L.I.; Boberg, J.; Skonberg, C.; Nellemann, C.; Hansen, S.H.; Hansen, H.S. Influence of dietary fatty acids on endocannabinoid and N-acylethanolamine levels in rat brain, liver and small intestine. Biochim. Biophys. Acta 2008, 1781, 200–212. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; ElSayed, N.A.; Aleppo, G.; Bannuru, R.R.; Bruemmer, D.; Collins, B.S.; Ekhlaspour, L.; Gaglia, J.L.; Hilliard, M.E.; Johnson, E.L.; et al. 2. Diagnosis and Classification of Diabetes:Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. 1), S20–S42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McEvoy, J.W.; McCarthy, C.P.; Bruno, R.M.; Brouwers, S.; Canavan, M.D.; Ceconi, C.; Christodorescu, R.M.; Daskalopoulou, S.S.; Ferro, C.J.; Gerdts, E.; et al. 2024 ESC guidelines for the management of elevated blood pressure and hypertension. Eur. Heart J. 2024, 45, 3912–4018. [Google Scholar] [CrossRef] [PubMed]
- Meerwaldt, R.; Graaff, R.; Oomen, P.H.N.; Links, T.P.; Jager, J.J.; Alderson, N.L.; Thorpe, S.R.; Baynes, J.W.; Gans, R.O.; Smit, A.J. Simple non-invasive assessment of advanced glycation end-product accumulation. Diabetologia 2004, 47, 1324–1330. [Google Scholar] [CrossRef]
- Marendić, M.; Polić, N.; Matek, H.; Oršulić, L.; Polašek, O.; Kolčić, I.; Vassalle, C. Mediterranean diet assessment challenges: Validation of the Croatian version of the 14-item Mediterranean Diet Serving Score questionnaire. PLoS ONE 2021, 16, e0247269. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Nogueiras, R.; Diaz-Arteaga, A.; Lockie, S.H.; Velásquez, D.A.; Tschop, J.; López, M.; Cadwell, C.C.; Diéguez, C.; Tschöp, M.H. The endocannabinoid system: Role in glucose and energy metabolism. Pharmacol. Res. 2009, 60, 93–98. [Google Scholar] [CrossRef]
- Moreno, E.; Cavic, M.; Canela, E.I. Functional fine-tuning of metabolic pathways by the endocannabinoid system—Implications for health and disease. Int. J. Mol. Sci. 2021, 22, 3661. [Google Scholar] [CrossRef]
- Nagappan, A.; Shin, J.; Jung, M.H. Role of cannabinoid receptor type 1 in insulin resistance and its biological implications. Int. J. Mol. Sci. 2019, 20, 2109. [Google Scholar] [CrossRef]
- Quercioli, A.; Pataky, Z.; Vincenti, G.; Makoundou, V.; Di Marzo, V.; Montecucco, F.; Carballo, S.; Thomas, A.; Staub, C.; Steffens, S.; et al. Elevated endocannabinoid plasma levels are associated with coronary circulatory dysfunction in obesity. Eur. Heart J. 2011, 32, 1369–1378. [Google Scholar] [CrossRef]
- Kahn, S.E.; Hull, R.L.; Utzschneider, K.M. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006, 444, 840–846. [Google Scholar] [CrossRef]
- Matias, I.; Wang, J.; Moriello, A.S.; Nieves, A.; Woodward, D.; Di Marzo, V. Changes in endocannabinoid and palmitoylethanolamide levels in eye tissues of patients with diabetic retinopathy and age-related macular degeneration. Prostaglandins Leukot. Essent. Fat Acids 2006, 75, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Després, J.-P.; Golay, A.; Sjöström, L. Effects of rimonabant on metabolic risk factors in overweight patients with dyslipidaemia. N. Engl. J. Med. 2005, 353, 2121–2134. [Google Scholar] [CrossRef]
- Pi-Sunyer, F.X.; Aronne, L.J.; Heshmati, H.M.; Devin, J.; Rosenstock, J. Effect of rimonabant, a cannabinoid-1 receptor blocker, on weight and cardiometabolic risk factors in overweight or obese patients: RIO-North America randomised controlled trial. JAMA 2006, 295, 761–775. [Google Scholar] [CrossRef]
- Van Gaal, L.F.; Rissanen, A.M.; Scheen, A.J.; Ziegler, O.; Rössner, S. Cannabinoid-1 receptor blockade with rimonabant: 1-year results from the RIO-Europe study. Lancet 2005, 365, 1389–1397. [Google Scholar] [CrossRef]
- Scheen, A.J.; Finer, N.; Hollander, P.; Jensen, M.D.; Van Gaal, L.F.; RIO-Diabetes Study Group. Rimonabant in overweight or obese patients with type 2 diabetes: A randomised controlled study. Lancet 2006, 368, 1660–1672. [Google Scholar] [CrossRef]
- Di Marzo, V.; Stella, N.; Zimmer, A. Endocannabinoid signalling and the deteriorating brain. Nat. Rev. Neurosci. 2015, 16, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Maccarrone, M.; Gasperi, V.; Catani, M.V.; Diep, T.A.; Dainese, E.; Hansen, H.S.; Avigliano, L. The endocannabinoid system and its relevance for nutrition. Annu. Rev. Nutr. 2010, 30, 423–440. [Google Scholar] [CrossRef]
- Annuzzi, G.; Piscitelli, F.; Di Marino, L.; Patti, L.; Giacco, R.; Costabile, G.; Bozzetto, L.; Riccardi, G.; Verde, R.; Petrosino, S.; et al. Differential alterations of the concentrations of endocannabinoids and related lipids in the subcutaneous adipose tissue of obese diabetic patients. Lipids Health Dis. 2010, 9, 43. [Google Scholar] [CrossRef]
- Liu, J.; Zhou, L.; Xiong, K.; Godlewski, G.; Mukhopadhyay, B.; Tam, J.; Yin, S.; Gao, P.; Shan, X.; Pickel, J.; et al. Hepatic cannabinoid receptor-1 mediates diet-induced insulin resistance via impaired insulin signalling and clearance in mice. Gastroenterology 2012, 142, 1218–1228.e1. [Google Scholar] [CrossRef]
- Tagliamonte, S.; Laiola, M.; Ferracane, R.; Vitale, M.; Gallo, M.A.; Meslier, V.; Pons, N.; Ercolini, D.; Vitaglione, P. Mediterranean diet consumption affects the endocannabinoid system in overweight and obese subjects: Links with gut microbiome, insulin resistance and inflammation. Eur. J. Nutr. 2021, 60, 3703–3716. [Google Scholar] [CrossRef]
- Yang, H.M.; Kim, J.; Kim, B.K.; Seo, H.J.; Kim, J.Y.; Lee, J.E.; Lee, J.; You, J.; Jin, S.; Kwon, Y.-W.; et al. Resistin regulates inflammation and insulin resistance in humans via the endocannabinoid system. Research 2024, 7, 0326. [Google Scholar] [CrossRef]
- Lee, J.; Yun, J.-S.; Ko, S.-H. Advanced glycation end-products and vascular complications in type 2 diabetes mellitus. Nutrients 2022, 14, 3086. [Google Scholar] [CrossRef]
- Lu, X.; Ma, R.; Zhan, J.; Pan, X.; Liu, C.; Zhang, S.; Tian, Y. Effect of dietary intake of advanced glycation end products on biomarkers of type 2 diabetes: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2024, 25, 1–10. [Google Scholar] [CrossRef]
- Birukov, A.; Cuadrat, R.; Polemiti, E.; Eichelmann, F.; Schulze, M.B. Skin autofluorescence-measured advanced glycation end-products associate with vascular stiffness: A cross-sectional study. Cardiovasc. Diabetol. 2021, 20, 110. [Google Scholar] [CrossRef]
- Teichert, T.; Hellwig, A.; Peßler, A.; Hellwig, M.; Vossoughi, M.; Sugiri, D.; Vierkötter, A.; Schulte, T.; Freund, J.; Roden, M.; et al. Association between Advanced Glycation End Products and Impaired Fasting Glucose: Results from the SALIA Study. PLoS ONE 2015, 10, e0128293. [Google Scholar] [CrossRef]
- Müller, T.; Demizieux, L.; Troy-Fioramonti, S.; Grest, J.; Pais de Barros, J.P.; Berger, H.; Vergès, B.; Degrace, P. Overactivation of the endocannabinoid system alters the antilipolytic action of insulin in mouse adipose tissue. Am. J. Physiol. Endocrinol. Metab. 2017, 313, E26–E36. [Google Scholar] [CrossRef]
- Kumric, M.; Dujic, G.; Vrdoljak, J.; Supe-Domic, D.; Bilopavlovic, N.; Dolic, K.; Dujic, Z.; Bozic, J. Effects of CBD supplementation on ambulatory blood pressure and serum urotensin-II concentrations in Caucasian patients with essential hypertension: A sub-analysis of the HYPER-H21-4 trial. Biomed. Pharmacother. 2023, 164, 115016. [Google Scholar] [CrossRef]
- Di Marzo, V.; Fontana, A.; Cadas, H.; Schinelli, S.; Cimino, G.; Schwartz, J.-C.; Piomelli, D. Formation and inactivation of endogenous cannabinoid anandamide in central neurons. Nature 1994, 372, 686–691. [Google Scholar] [CrossRef]
- Matias, I.; Gonthier, M.P.; Orlando, P.; Martiadis, V.; De Petrocellis, L.; Cervino, C.; Petrosino, S.; Hoareau, L.; Festy, F.; Pasquali, R.; et al. Regulation, Function, and Dysregulation of Endocannabinoids in Models of Adipose and β-Pancreatic Cells and in Obesity and Hyperglycemia. J. Clin. Endocrinol. Metab. 2006, 91, 3171–3180. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Di Filippo, C.; Rossi, F.; D’Amico, M. Mediterranean diet modulates the endocannabinoid system in overweight and obese subjects: A randomised trial. Nutrients 2021, 13, 3169. [Google Scholar]
- Fernández-Iglesias, A.; Pajuelo, D.; Quesada, H.; Díaz, S.; Bladé, C.; Arola, L.; Salvadó, M.J.; Mulero, M. Grape seed proanthocyanidin extract improves the hepatic glutathione metabolism in obese Zucker rats. Mol Nutr Food Res. 2014, 58, 727–737. [Google Scholar] [CrossRef]
- Cani, P.D.; Plovier, H.; Van Hul, M.; Geurts, L.; Delzenne, N.M.; Druart, C.; Everard, A. Endocannabinoids at the crossroads between the gut microbiota and host metabolism. Nat. Rev. Endocrinol. 2016, 12, 133–143. [Google Scholar] [CrossRef]
- Richard, C.; Lewis, E.D.; Field, C.J. Omega-3 polyunsaturated fatty acids and cardiometabolic risk in children and adolescents. Nutrients 2016, 8, 329. [Google Scholar]
| Parameter | Prediabetes (n = 92) | Control Group (n = 86) | p-Value |
|---|---|---|---|
| Age (years) | 54.2 ± 8.3 | 56.6 ± 9.1 | 0.067 * |
| Male sex, n (%) | 38 (41.3) | 39 (45.3) | 0.694 ** |
| BMI (kg/m2) | 30.4 ± 3.8 | 26.4 ± 2.9 | 0.032 * |
| WHR | 0.99 ± 0.31 | 0.96 ± 0.32 | 0.684 * |
| Systolic BP (mmHg) | 134.8 ± 11.9 | 123.2 ± 9.4 | <0.001 * |
| Diastolic BP (mmHg) | 84.9 ± 10.2 | 78.3 ± 7.6 | <0.001 * |
| FPG (mmol/L) | 5.8 ± 0.6 | 5.1 ± 0.7 | 0.024 * |
| HbA1c (%) | 5.9 ± 0.4 | 5.5 ± 0.3 | 0.031 * |
| Total cholesterol (mmol/L) | 5.7 ± 0.9 | 5.2 ± 1.1 | 0.038 * |
| LDL-C (mmol/L) | 3.5 ± 0.7 | 3.3 ± 1.1 | 0.142 * |
| HDL-C (mmol/L) | 1.6 ± 0.5 | 1.4 ± 0.4 | 0.234 * |
| Triglycerides (mmol/L) | 1.5 ± 0.9 | 1.2 ± 0.3 | 0.022 * |
| AST (U/L) | 25.5 ± 7.8 | 24.1 ± 8.4 | 0.494 * |
| ALT (U/L) | 26.2 ± 9.3 | 22.3 ± 9.1 | 0.382 * |
| Creatinine (mmol/L) | 78 ± 15 | 75 ± 15 | 0.765 * |
| AGE value | 2.4 ± 0.5 | 2.2 ± 0.4 | 0.104 * |
| Parameter | AEA (ng/mL) | 2-AG (ng/mL) | ||||
|---|---|---|---|---|---|---|
| Adherent | Non-Adherent | p * | Adherent | Non-Adherent | p-Value | |
| Cereals | 35.0 (18.3–61.1) | 35.7 (21.1–55.1) | 0.423 | 31.6 (23.0–41.1) | 30.8 (24.1–39.9) | 0.723 |
| Potato | 37.5 (19.0–65.1) | 38.5 (22.0–61.1) | 0.627 | 19.0 (13.7–29.7) | 15.3 (12.5–23.0) | 0.063 |
| Olive oil | 40.2 (20.2–68.2) | 41.0 (23.2–62.3) | 0.765 | 31.0 (22.0–40.6) | 29.9 (23.5–39.0) | 0.114 |
| Nuts | 42.3 (22.3–70.3) | 42.9 (25.3–65.0) | 0.274 | 19.2 (10.0–29.0) | 20.3 (12.5–28.4) | 0.456 |
| Fruit | 38.3 (20.3–63.0) | 37.8 (24.3–60.1) | 0.857 | 27.6 (18.1–36.6) | 26.8 (19.7–36.0) | 0.534 |
| Vegetables | 41.1 (18.1–65.0) | 41.4 (21.0–58.1) | 0.539 | 32.5 (25.7–38.6) | 31.9 (26.5–37.9) | 0.798 |
| Dairy products | 36.5 (15.1–58.2) | 38.5 (19.0–54.2) | 0.092 | 21.4 (12.0–30.9) | 22.5 (13.1–31.5) | 0.555 |
| Legumes | 39.2 (17.5–64.1) | 38.4 (22.5–59.6) | 0.102 | 27.4 (22.0–33.2) | 26.2 (22.1–32.0) | 0.364 |
| Eggs | 43.6 (23.0–72.6) | 43.3 (26.6–66.5) | 0.788 | 19.1 (11.2–29.0) | 18.6 (11.9–27.8) | 0.277 |
| Fish | 37.5 (16.0–61.5) | 36.8 (21.7–57.7) | 0.234 | 21.9 (13.6–30.5) | 22.4 (15.1–29.9) | 0.355 |
| White meat | 44.2 (24.2–64.2) | 44.0 (25.3–62.3) | 0.698 | 44.4 (37.0–51.3) | 43.5 (37.5–50.4) | 0.243 |
| Red meat | 42.7 (24.3–73.3) | 44.9 (27.3–67.0) | 0.082 | 28.7 (22.5–35.8) | 29.2 (24.1–36.0) | 0.756 |
| Sweets | 39.3 (21.3–62.4) | 39.8 (24.6–62.1) | 0.586 | 25.7 (12.5–34.0) | 26.0 (21.9–34.5) | 0.819 |
| Wine | 41.5 (18.6–64.0) | 43.4 (26.0–57.1) | 0.094 | 32.1 (26.8–40.8) | 31.5 (27.4–39.9) | 0.745 |
| MD adherence † | 38.0 (20.3–51.9) | 47.5 (27.7–51.8) | 0.038 | 18.2 (12.8–30.8) | 21.5 (16.2–27.9) | 0.653 |
| Variable | β (95% CI) † | SE | p-Value |
|---|---|---|---|
| Prediabetes (vs. control) | 11.9 (3.7 to 20.1) | 4.1 | 0.005 |
| AGEs (arbitrary units) | 0.25 (0.09 to 0.41) | 0.08 | 0.003 |
| Age (years) | 0.31 (0.09 to 0.53) | 0.11 | 0.007 |
| Sex (male vs. female) | –1.4 (–8.8 to 6.0) | 3.7 | 0.712 |
| BMI (kg/m2) | 0.06 (–0.26 to 0.38) | 0.16 | 0.702 |
| Fasting plasma glucose (mmol/L) | –0.88 (–3.9 to 2.1) | 1.5 | 0.561 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grahovac, M.; Kumric, M.; Vilovic, M.; Supe-Domic, D.; Pavlovic, N.; Bukic, J.; Ticinovic Kurir, T.; Bozic, J. Endocannabinoid and AGE Interactions in Prediabetes: The Role of Mediterranean Diet Adherence. Nutrients 2025, 17, 2517. https://doi.org/10.3390/nu17152517
Grahovac M, Kumric M, Vilovic M, Supe-Domic D, Pavlovic N, Bukic J, Ticinovic Kurir T, Bozic J. Endocannabinoid and AGE Interactions in Prediabetes: The Role of Mediterranean Diet Adherence. Nutrients. 2025; 17(15):2517. https://doi.org/10.3390/nu17152517
Chicago/Turabian StyleGrahovac, Marko, Marko Kumric, Marino Vilovic, Daniela Supe-Domic, Nikola Pavlovic, Josipa Bukic, Tina Ticinovic Kurir, and Josko Bozic. 2025. "Endocannabinoid and AGE Interactions in Prediabetes: The Role of Mediterranean Diet Adherence" Nutrients 17, no. 15: 2517. https://doi.org/10.3390/nu17152517
APA StyleGrahovac, M., Kumric, M., Vilovic, M., Supe-Domic, D., Pavlovic, N., Bukic, J., Ticinovic Kurir, T., & Bozic, J. (2025). Endocannabinoid and AGE Interactions in Prediabetes: The Role of Mediterranean Diet Adherence. Nutrients, 17(15), 2517. https://doi.org/10.3390/nu17152517