
Salivary pH Modulation and Antimicrobial Properties of Oregano-Oil Jelly in Relation to Menstrual and Menopausal Status

 , ,
, ,  , , , , , ,
, , , , , ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Clinical Application of Oregano-Oil Jelly
2.2. Preparation and Composition of Oregano-Oil Jelly
- P1: Jelly formulated with Origani aetheroleum (oregano essential oil);
- P2: A commercially available jelly product.
2.3. Microbial Strains
- Gram-positive bacteria: Staphylococcus aureus ATCC 25923 (LOT: 693518) and Streptococcus pyogenes ATCC 19615 (LOT: 701224);
- Gram-negative bacteria: Escherichia coli ATCC 35218 (LOT: 699211);
- Fungus: Candida albicans ATCC 14053 (LOT: 332-131-2).
2.4. Laboratory Testing Procedures
- Clindamycin (2 µg/disc) and gentamicin (120 µg/disc) for bacteria;
- Nystatin (100 IU/disc) for Candida albicans.
2.5. Incubation and Assessment of Antimicrobial Activity
2.6. Saliva Collection and pH Measurement
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Salivary pH Before and After Oregano-Oil Jelly Use
3.3. Correlations Among Variables
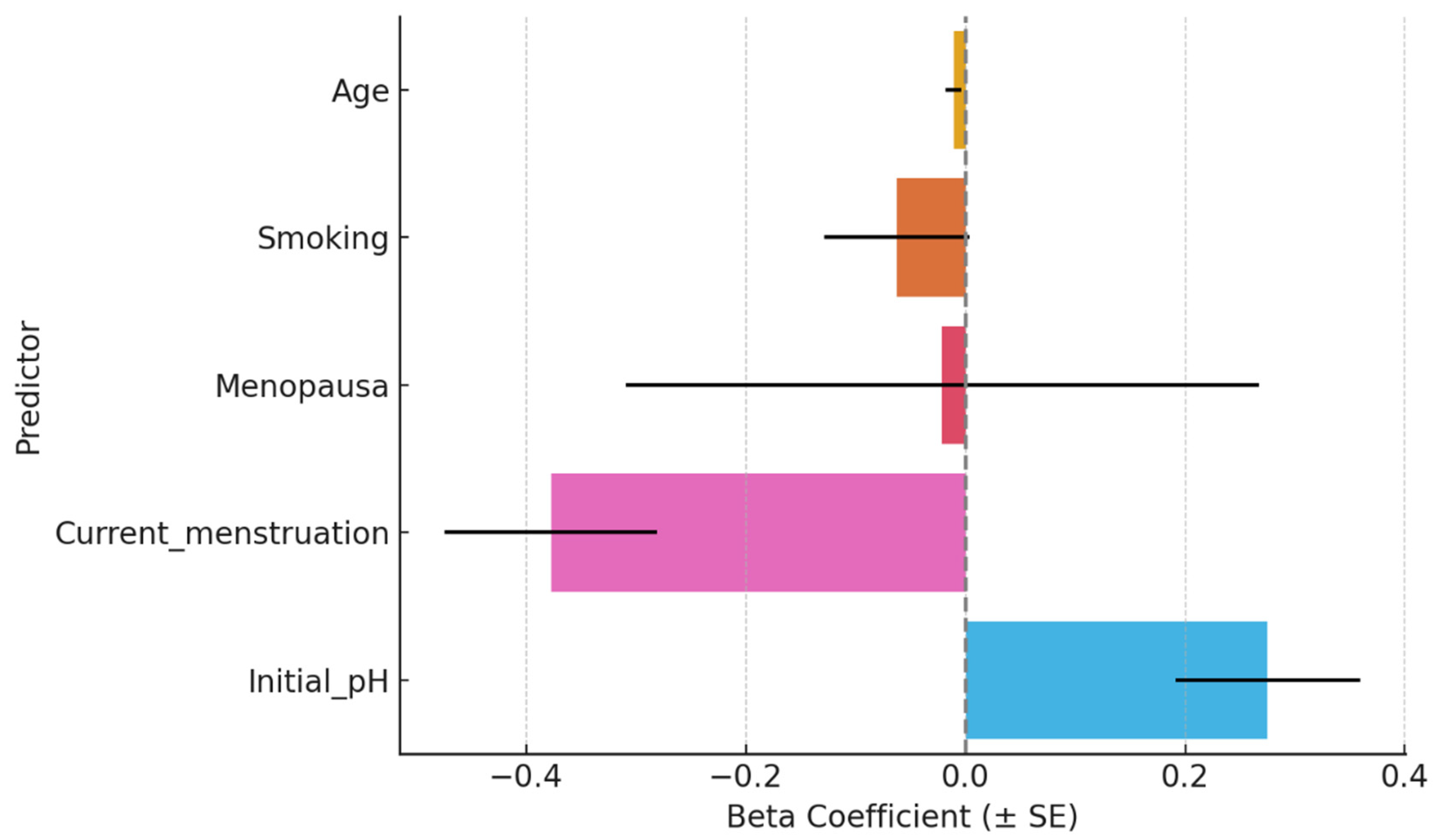
3.4. Multiple Linear Regression
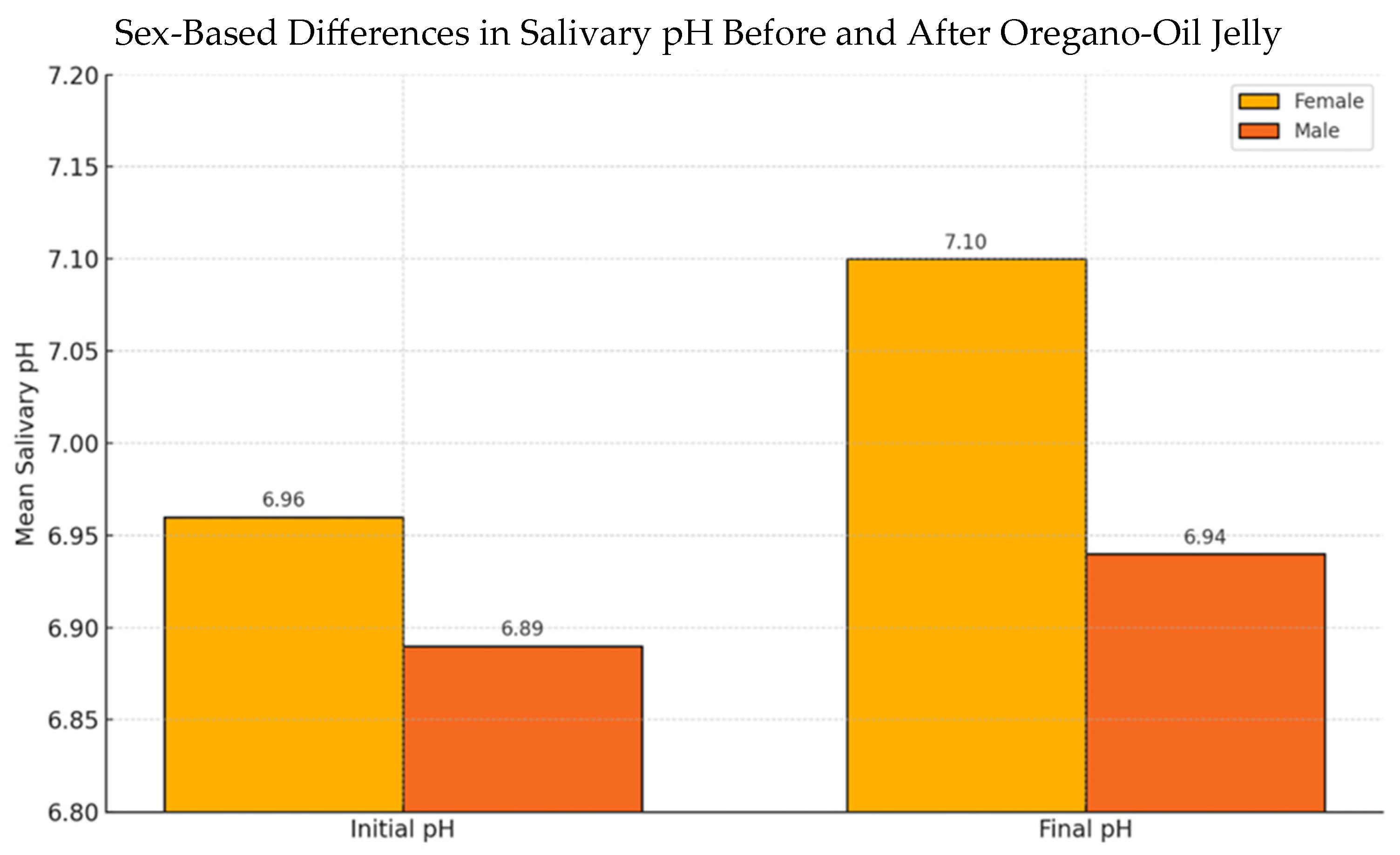
3.5. Sex-Based Differences in Salivary pH Response
3.6. Experimental Results of Antimicrobial Testing
- Staphylococcus aureus: 34 mm;
- Streptococcus pyogenes: 35 mm;
- Escherichia coli: 8 mm;
- Candida albicans: 8 mm.
- Staphylococcus aureus: 22 mm;
- Streptococcus pyogenes: 25 mm;
- Escherichia coli: 22 mm;
- Candida albicans: 19 mm.
- Clindamycin: 27 mm (S. aureus), 26 mm (S. pyogenes);
- Gentamicin: 33 mm (S. aureus), 28 mm (S. pyogenes), 24 mm (E. coli);
- Nystatin: 20 mm (C. albicans).
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Studies
4.3. Influence of Menstruation and Menopause
4.4. Strengths and Limitations
4.5. Implications and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karaday, M.; Yıldırım, V.; Güllüce, M. Antimicrobial activity and other biological properties of oregano essential oil and carvacrol. Anatol. J. Biol. 2020, 1, 52–68. [Google Scholar]
- Burt, S. Essential oils: Their antibacterial properties and potential applications in foods—A review. Int. J. Food Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef] [PubMed]
- Abrudan-Luca, D.; Floare, L.; Simerea, I.-A.; Dumitrescu, R.; Balean, O.; Bolchis, V.; Arabela, J.A. Variation in Salivary pH Based on Sugar Consumption. Med. Evol. 2024, 30, 2247–6482. [Google Scholar] [CrossRef]
- Mahanta, A.; Yadav, G.; Saha, S.; Dhinsa, K.; Sharma, A.; Rai, A. A Comparative Evaluation of the Acidogenic Potential of Lactose-based, Soy-based, Protein Hydrolysate-based, and Iron-based Milk Formulas Based on Dental Plaque pH, Salivary pH, and Buffering Capacity: An In Vivo Study. Int. J. Clin. Pediatr. Dent. 2024, 17, 851. [Google Scholar]
- Țenț, P.A.; Juncar, R.I.; Juncar, M. Clinical patterns and characteristics of midfacial fractures in western romanian population: A 10-year retrospective study. Med. Oral. Patol. Oral. Cir. Bucal 2019, 24, e792–e798. [Google Scholar] [CrossRef]
- Yuan, Y.; Sun, J.; Song, Y.; Raka, R.N.; Xiang, J.; Wu, H.; Xiao, J.; Jin, J.; Hui, X. Antibacterial activity of oregano essential oils against Streptococcus mutans in vitro and analysis of active components. BMC Complement. Med. Ther. 2023, 23, 61. [Google Scholar] [CrossRef]
- Bairamis, A.; Sotiropoulou, N.-S.D.; Tsadila, C.; Tarantilis, P.; Mossialos, D. Chemical Composition and Antimicrobial Activity of Essential Oils and Hydrosols from Oregano, Sage and Pennyroyal against Oral Pathogens. Appl. Sci. 2024, 14, 3238. [Google Scholar] [CrossRef]
- Ghitea, T.C.; El-Kharoubi, A.; Ganea, M.; Bimbo-Szuhai, E.; Nemeth, T.S.; Ciavoi, G.; Foghis, M.; Dobjanschi, L.; Pallag, A.; Micle, O. The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome. Molecules 2021, 26, 283. [Google Scholar] [CrossRef]
- Cicalău, G.I.P.; Babes, P.A.; Calniceanu, H.; Popa, A.; Ciavoi, G.; Iova, G.M.; Ganea, M.; Scrobotă, I. Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus. Molecules 2021, 26, 6899. [Google Scholar] [CrossRef]
- Cicalău, G.I.P.; Miere, F.; Mandal, A.K.; Ganea, M.; Scrobota, I.; Ciavoi, G.; Jurca, C.M. Formulation and Characterization of Hydrophilic Ointment Bases with Carvacrol and Magnolol for Periodontal Application. Pharmacophore 2022, 13, 26–32. [Google Scholar] [CrossRef]
- Potra Cicalău, G.I.; Ciavoi, G.; Scrobotă, I.; Marcu, A.O.; Romanul, I.; Marian, E.; Vicaș, L.G.; Ganea, M. Assessing the Antioxidant Benefits of Topical Carvacrol and Magnolol Periodontal Hydrogel Therapy in Periodontitis Associated with Diabetes in Wistar Rats. Dent. J. 2023, 11, 284. [Google Scholar] [CrossRef]
- Potra Cicalău, G.I.; Marcu, O.A.; Ghitea, T.C.; Ciavoi, G.; Iurcov, R.C.; Beiusanu, C.; Trifan, D.F.; Vicaș, L.G.; Ganea, M. Study of Periodontal Bacteria in Diabetic Wistar Rats: Assessing the Anti-Inflammatory Effects of Carvacrol and Magnolol Hydrogels. Biomedicines 2024, 12, 1445. [Google Scholar] [CrossRef] [PubMed]
- Reeves, J. The impact of female hormones on the periodontium—A narrative review. Int. J. Dent. Hyg. 2025. [Google Scholar] [CrossRef] [PubMed]
- Rafiei, M. Perspective Chapter: Oral Condition and Lifetime Hormonal Fluctuations; IntechOpen: London, UK, 2025. [Google Scholar]
- Kamal Asaad, N.; Abbood, H.M. Comparing gingival inflammation and salivary acidity to hormonal variation during menstruation. Saudi Dent. J. 2023, 35, 251–254. [Google Scholar] [CrossRef]
- American Society for Microbiology. Molecular Microbiology: Diagnostic Principles and Practice, 3rd ed.; Persing, D.H., Ed.; ASM Press: Washington, DC, USA, 2016. [Google Scholar]
- Chouhan, S.; Sharma, K.; Guleria, S. Antimicrobial Activity of Some Essential Oils-Present Status and Future Perspectives. Medicines 2017, 4, 58. [Google Scholar] [CrossRef]
- Marsh, P.D. Dental plaque as a biofilm and a microbial community—Implications for health and disease. BMC Oral Health 2006, 6, S14. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.M.; Casamassima, L.; Trilli, I.; Ferrante, L.; Inchingolo, F.; Palermo, A.; Inchingolo, A.D.; Dipalma, G. Effectiveness of herbal medicines with anti-inflammatory, antimicrobial, and antioxidant properties in improving oral health and treating gingivitis and periodontitis: A systematic review. Nutrients 2025, 17, 762. [Google Scholar] [CrossRef]
- Hambardzumyan, S.; Sahakyan, N.; Petrosyan, M.; Nasim, M.J.; Jacob, C.; Trchounian, A. Origanum vulgare L. Extract-mediated synthesis of silver nanoparticles, their characterization and antibacterial activities. AMB Express 2020, 10, 162. [Google Scholar] [CrossRef]
- Drăgan, F.; Moisa, C.F.; Teodorescu, A.; Burlou-Nagy, C.; Fodor, K.I.; Marcu, F.; Popa, D.E.; Teaha, D.I.M. Evaluating in vitro antibacterial and antioxidant properties of Origanum vulgare volatile oil. Farmacia 2022, 70, 1114–1122. [Google Scholar] [CrossRef]
- Ren, X.; Zhang, Y.; Xiang, Y.; Hu, T.; Cheng, R.; Cai, H. The efficacy of mouthwashes on oral microorganisms and gingivitis in patients undergoing orthodontic treatment: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 204. [Google Scholar] [CrossRef]
- Serbiak, B.; Fourre, T.; Geonnotti, A.R.; Gambogi, R.J. In vitro efficacy of essential oil mouthrinse versus dentifrices. J. Dent. 2018, 69, 49–54. [Google Scholar] [CrossRef]
- Motoc, G.V.; Juncar, R.I.; Moca, A.E.; Motoc, O.; Vaida, L.L.; Juncar, M. The Relationship between Age, Gender, BMI, Diet, Salivary pH and Periodontal Pathogenic Bacteria in Children and Adolescents: A Cross-Sectional Study. Biomedicines 2023, 11, 2374. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Kaushik, U.; Sharma, D. Overview on Phytochemistry and Pharmacological Activity of the Leaves of Origanum vulgare. Philipp. J. Sci. 2024, 153, 1757. [Google Scholar]
- Hulankova, R. Methods for Determination of Antimicrobial Activity of Essential Oils In Vitro—A Review. Plants 2024, 13, 2784. [Google Scholar] [CrossRef]
- Juncar, M.; Bran, S.; Juncar, R.I.; Baciut, M.F.; Baciut, G.; Onisor-Gligor, F. Odontogenic cervical necrotizing fasciitis, etiological aspects. Niger. J. Clin. Pract. 2016, 19, 391–396. [Google Scholar] [CrossRef]
- Yilmaz, F.; Carti Dorterler, O.; Eren Halici, S.; Kasap, B.; Demirbas, A. The effects of pregnancy on oral health, salivary pH and flow rate. BMC Oral. Health 2024, 24, 1286. [Google Scholar] [CrossRef]
- Bostanci, N. Periodontal health and pregnancy outcomes: Time to deliver. Obstet. Anesth. Dig. 2024, 44, 16–17. [Google Scholar] [CrossRef]
- Upadhyay, A.; Cao, U.; Cai, W.; Alli, B.; Khayambashi, P.; Mai, C.T.T.; Sultan, S.; Tran, S.D. Stem Cell-Based Regeneration of Salivary Glands: From Bench to Clinics. In Handbook of Stem Cell Applications; Springer: Berlin/Heidelberg, Germany, 2024; pp. 1–32. [Google Scholar]
- Zolotukhin, S. Metabolic hormones in saliva: Origins and functions. Oral. Dis. 2013, 19, 219–229. [Google Scholar] [CrossRef]
- Kasana, J.; Choudhary, P.; Bhati, D. Exploring the Effects of Hormonal Fluctuations (Such as Those Associated with Puberty, Pregnancy, and Menopause) on Oral Health and Physiology, Including Changes in Gingival Health, Saliva Composition, and Susceptibility to Dental Diseases. JCHR 2023, 14, 3555–3557. [Google Scholar]
- Alia, S.; Aquilanti, L.; Pugnaloni, S.; Di Paolo, A.; Rappelli, G.; Vignini, A. The Influence of Age and Oral Health on Taste Perception in Older Adults: A Case-Control Study. Nutrients 2021, 13, 4166. [Google Scholar] [CrossRef]
- Brading, M.G.; Joiner, A.; Kinane, D.F. Changes in oral health and condition with age. Int. Dent. J. 2009, 59, 309–320. [Google Scholar] [CrossRef]
- Ben-Aryeh, H.; Cohen, M.; Kanter, Y.; Szargel, R.; Laufer, D. Salivary composition in diabetic patients. J. Diabet. Complicat. 1988, 2, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.T.; Hande, A.; Reche, A.; Paul, P. Appraisal of Saliva and Its Sensory Perception in Reproductive Transitions of Women: A Review. Cureus 2022, 14, e31614. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S. Menopause and Oral Health: Clinical Implications and Preventive Strategies. J. Mid-Life Health 2024, 15, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Krishnan, A.; Mukherjee, A.; Kumar, V. Menopause and Oral Health. In Management of Menopause: A Guide for Practitioners; Springer: Singapore, 2025; pp. 73–88. [Google Scholar]
- García-Alfaro, P.; Pérez-López, F.R.; Martínez, S.G.; Rodríguez, I. Xerostomia and oral health-related quality of life in peri-and postmenopausal women. Maturitas 2025, 197, 108268. [Google Scholar] [CrossRef]
- de Oliveira, N.P.; de Melo Pompei, L. Effect of menopause hormone therapy and serotonin reuptake inhibitors. Climacteric 2025, 1, 1–5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) or Mean ± SD |
|---|---|
| Age (years) | 24.5 ± 8.0 |
| Female | 69 (76%) |
| Male | 22 (24%) |
| Urban residence | 78 (86%) |
| Rural residence | 13 (14%) |
| Smokers | 46 (51%) |
| Non-smokers | 45 (49%) |
| Postmenopausal | 4 (4%) |
| Current menstruation | 12 (13%) |
| Group | Initial pH |
|---|---|
| Total sample | 6.94 |
| No menopause | 6.95 |
| Menopause | 6.75 |
| No menstruation | 6.93 |
| Current menstruation | 7.03 |
| Variables | Correlation (ρ) |
|---|---|
| Age vs. Final pH | −0.25 |
| Initial pH vs. Final pH | +0.31 |
| Age vs. Initial pH | −0.08 |
| Predictor | β Coefficient | p-Value |
|---|---|---|
| Age | −0.011 | 0.143 |
| Smoking | −0.062 | 0.351 |
| Menopausal status | −0.021 | 0.942 |
| Current menstruation | −0.377 | <0.001 * |
| Initial pH | +0.275 | 0.002 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potra Cicalău, G.I.; Ciavoi, G.; Scrobota, I.; Venter, I.D.; Ganea, M.F.; Ghitea, M.C.; Ghitea, E.C.; Gîtea, M.F.; Ghitea, T.C.; Nagy, C.; et al. Salivary pH Modulation and Antimicrobial Properties of Oregano-Oil Jelly in Relation to Menstrual and Menopausal Status. Nutrients 2025, 17, 2480. https://doi.org/10.3390/nu17152480
Potra Cicalău GI, Ciavoi G, Scrobota I, Venter ID, Ganea MF, Ghitea MC, Ghitea EC, Gîtea MF, Ghitea TC, Nagy C, et al. Salivary pH Modulation and Antimicrobial Properties of Oregano-Oil Jelly in Relation to Menstrual and Menopausal Status. Nutrients. 2025; 17(15):2480. https://doi.org/10.3390/nu17152480
Chicago/Turabian StylePotra Cicalău, Georgiana Ioana, Gabriela Ciavoi, Ioana Scrobota, Ionut Daniel Venter, Madalin Florin Ganea, Marc Cristian Ghitea, Evelin Claudia Ghitea, Maria Flavia Gîtea, Timea Claudia Ghitea, Csaba Nagy, and et al. 2025. "Salivary pH Modulation and Antimicrobial Properties of Oregano-Oil Jelly in Relation to Menstrual and Menopausal Status" Nutrients 17, no. 15: 2480. https://doi.org/10.3390/nu17152480
APA StylePotra Cicalău, G. I., Ciavoi, G., Scrobota, I., Venter, I. D., Ganea, M. F., Ghitea, M. C., Ghitea, E. C., Gîtea, M. F., Ghitea, T. C., Nagy, C., Pelea, D. C., Dobjanschi, L., Gligor, O., Moisa, C., & Ganea, M. (2025). Salivary pH Modulation and Antimicrobial Properties of Oregano-Oil Jelly in Relation to Menstrual and Menopausal Status. Nutrients, 17(15), 2480. https://doi.org/10.3390/nu17152480