
Impact of Iron Overload and Hypomagnesemia Combination on Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Outcomes

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Data Collection
2.3. Assessment and Categorization of Iron Overload
2.4. Assessment and Categorization of Serum Magnesium Levels
2.5. Statistical Analysis
3. Results
3.1. Patients
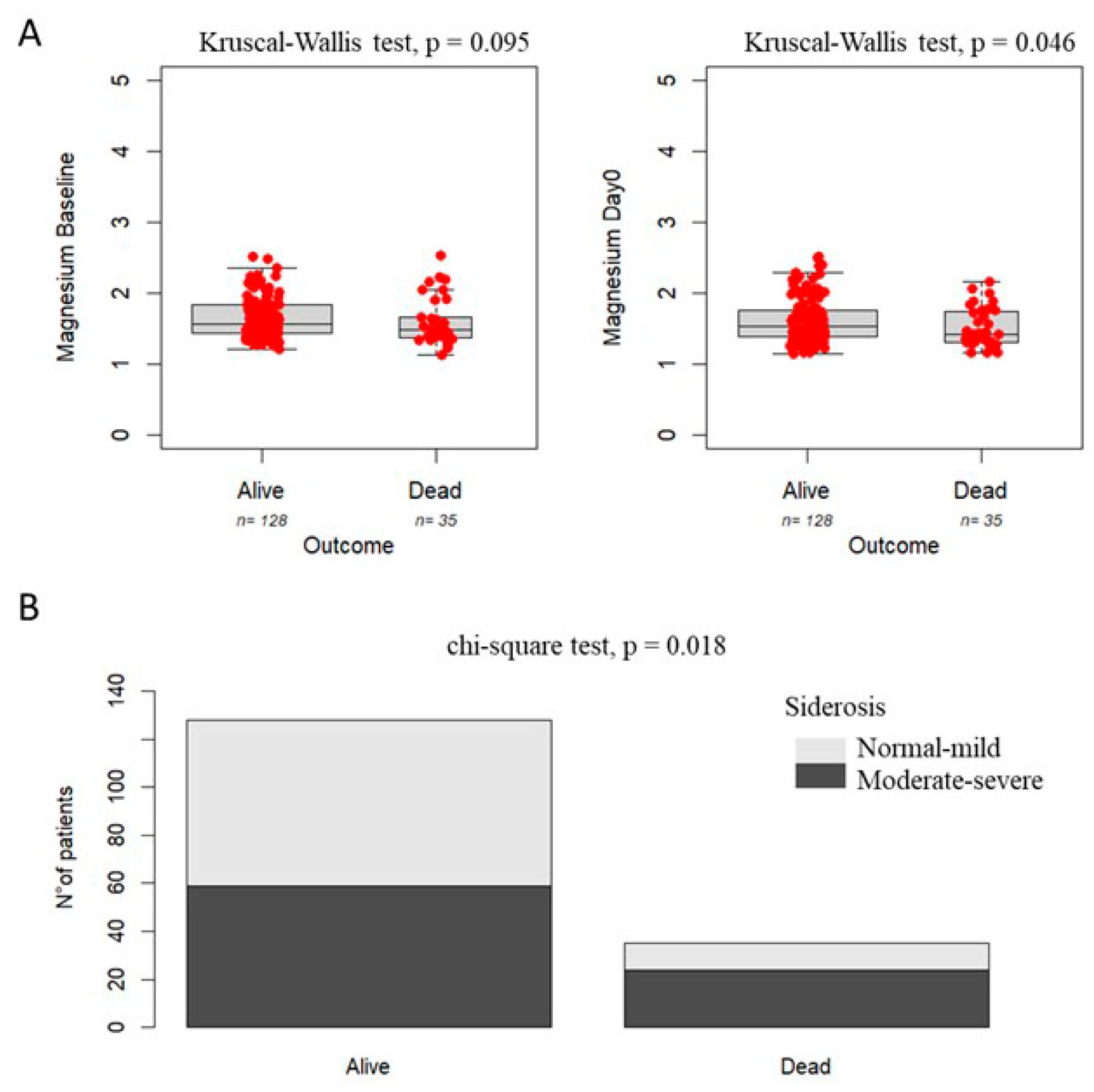
3.2. Magnesium Levels and Grade of Siderosis as Prognostic Factors for Survival
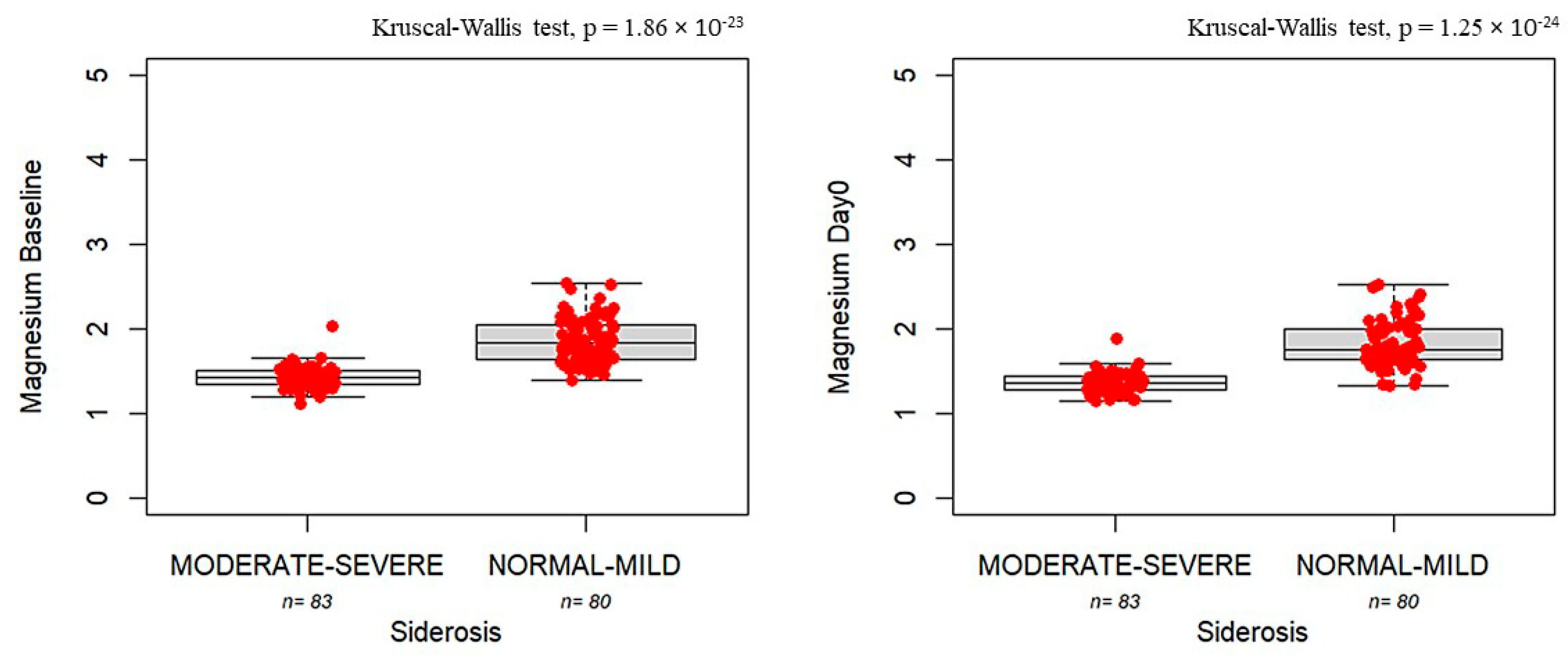
3.3. Association Between Magnesium Levels and Siderosis
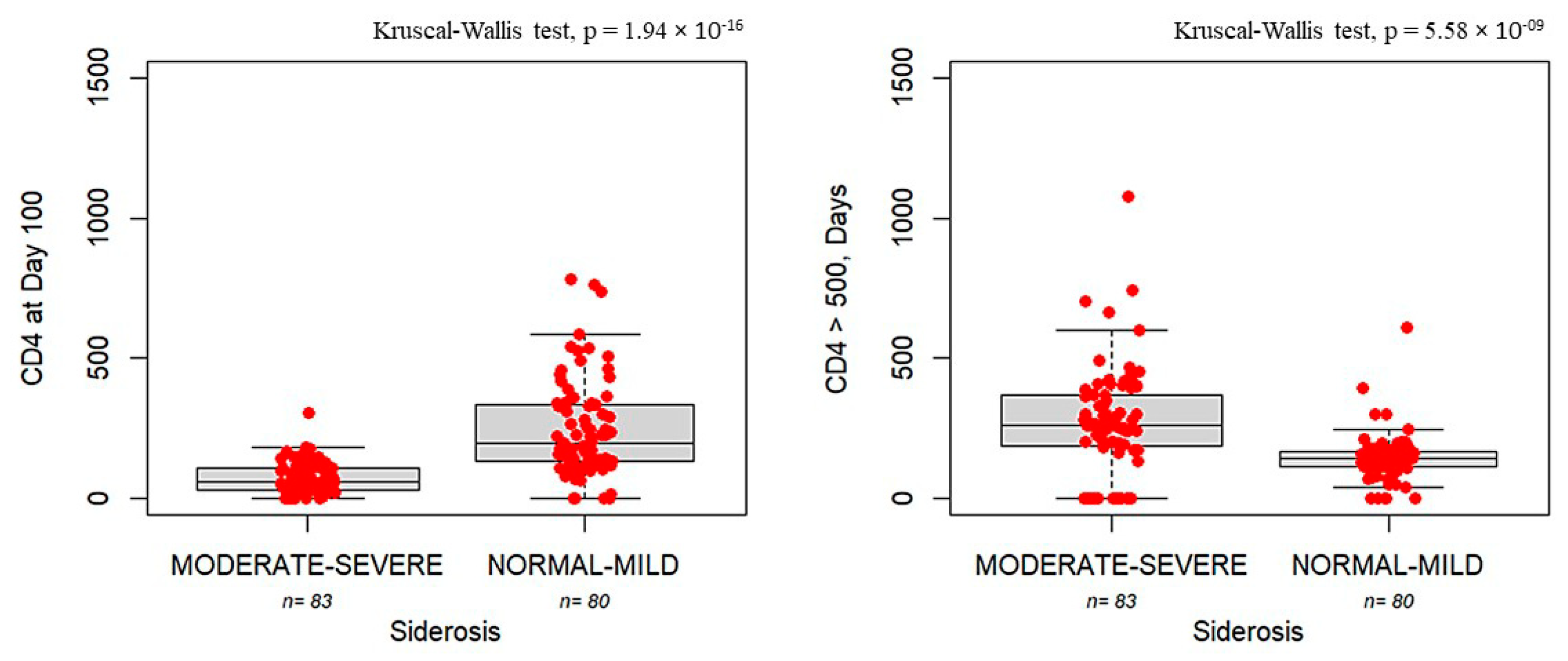
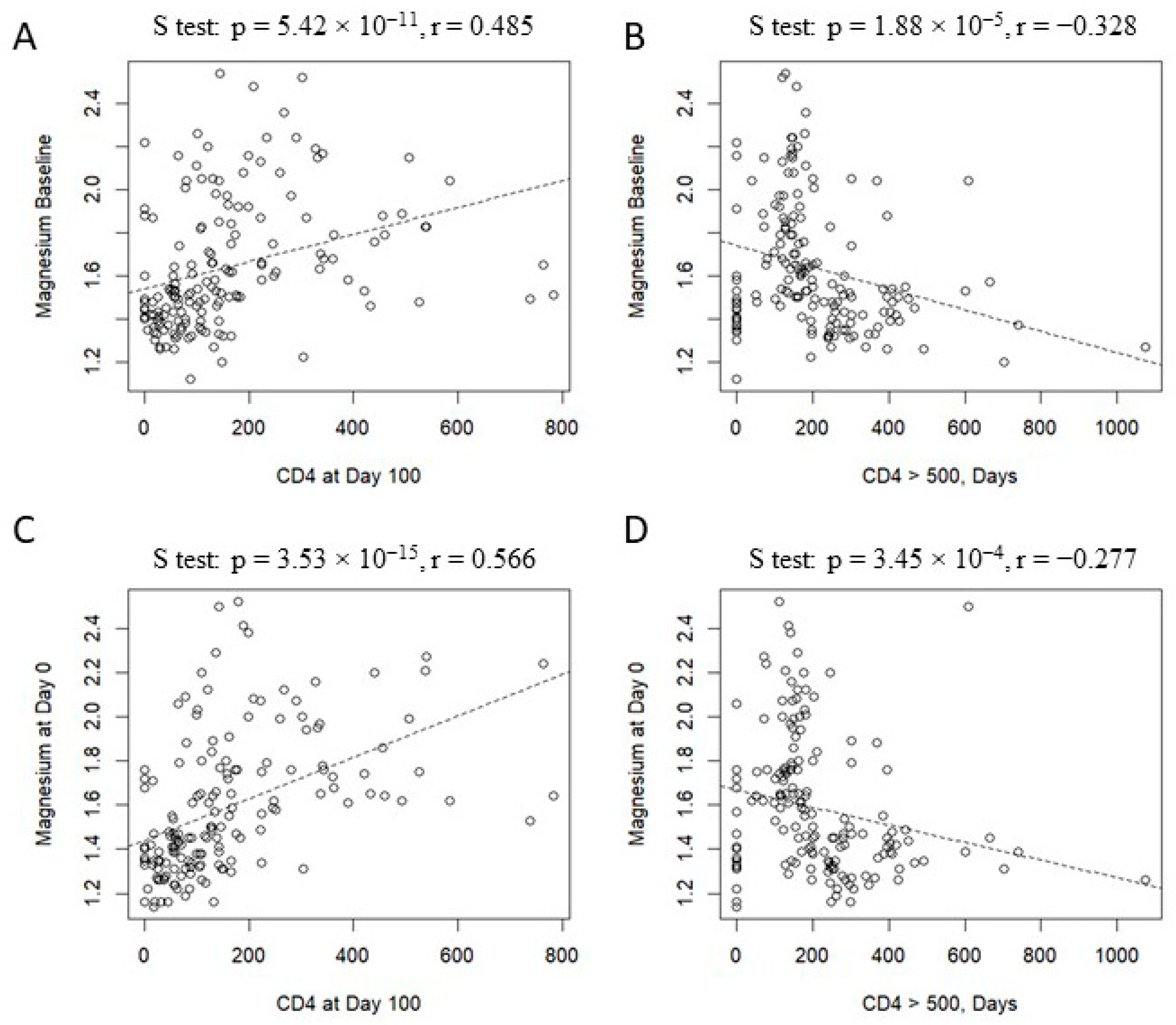
3.4. Delayed Immune Reconstitution in Patients with Siderosis and Hypomagnesemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giralt, S.; Bishop, M.R. Principles and overview of allogeneic hematopoietic stem cell transplantation. Hematop. Stem Cell Transplant. 2009, 144, 1–21. [Google Scholar]
- Kumar, A.; Israr, J. Allogeneic Stem Cell Transplantation: Current Status and Future Directions. OBM Transplant. 2025, 9, 241. [Google Scholar] [CrossRef]
- Osei-Hyiaman, U.; Liu, J.; Zhou, L.; Godlewski, G.; Harvey-White, J.; Jeong, W.-I.; Bátkai, S.; Marsicano, G.; Lutz, B.; Buettner, C.; et al. Hepatic CB1 receptor is required for development of diet-induced steatosis, dyslipidemia, and insulin and leptin resistance in mice. J. Clin. Investig. 2008, 118, 3160–3169. [Google Scholar] [CrossRef] [PubMed]
- Pan, T.; Ji, Y.; Liu, H.; Tang, B.; Song, K.; Wan, X.; Yao, W.; Sun, G.; Wang, J.; Sun, Z. Impact of Iron Overload and Iron Chelation with Deferasirox on Outcomes of Patients with Severe Aplastic Anemia after Allogeneic Hematopoietic Stem Cell Transplantation. Transplant. Cell. Ther. 2023, 29, 507.e1–507.e8. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.; Loscocco, F.; Visani, G.; Chiarucci, M.; Musto, P.; Kubasch, A.-S.; Platzbecker, U.; Vinchi, F. Iron Toxicity and Chelation Therapy in Hematopoietic Stem Cell Transplant. Transplant. Cell. Ther. 2021, 27, 371–379. [Google Scholar] [CrossRef]
- Maximova, N.; Gregori, M.; Boz, G.; Simeone, R.; Zanon, D.; Schillani, G.; Zennaro, F. MRI-based evaluation of multiorgan iron overload is a predictor of adverse outcomes in pediatric patients undergoing allogeneic hematopoietic stem cell transplantation. Oncotarget 2017, 8, 79650–79661. [Google Scholar] [CrossRef] [PubMed]
- MaxMaximova, N.; Gregori, M.; Simeone, R.; Sonzogni, A.; Boz, G.; Fucile, C.; Marini, V.; Martelli, A.; Mattioli, F. Safety and tolerability of deferasirox in pediatric hematopoietic stem cell transplant recipients: One facility’s five years’ experience of chelation treatment. Oncotarget 2017, 8, 63177–63186. [Google Scholar] [CrossRef]
- Sirlin, C.B.; Reeder, S.B. Magnetic resonance imaging quantification of liver iron. Magn. Reson. Imaging Clin. N. Am. 2010, 18, 359–381. [Google Scholar] [CrossRef]
- St Pierre, T.G.; Clark, P.R.; Chua-Anusorn, W. Measurement and mapping of liver iron concentrations using magnetic resonance imaging. Ann. N. Y. Acad. Sci. 2005, 1054, 379–385. [Google Scholar] [CrossRef]
- Pierre, T.G.S.; Clark, P.R.; Chua-Anusorn, W.; Fleming, A.J.; Jeffrey, G.P.; Olynyk, J.K.; Pootrakul, P.; Robins, E.; Lindeman, R. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 2005, 105, 855–861. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Feske, S.; Skolnik, E.Y.; Prakriya, M. Ion channels and transporters in lymphocyte function and immunity. Nat. Rev. Immunol. 2012, 12, 532–547. [Google Scholar] [CrossRef]
- Angenendt, L.; Hilgefort, I.; Mikesch, J.-H.; Schlüter, B.; Berdel, W.E.; Lenz, G.; Stelljes, M.; Schliemann, C. Magnesium levels and outcome after allogeneic hematopoietic stem cell transplantation in acute myeloid leukemia. Ann. Hematol. 2021, 100, 1871–1878. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Carlone, G.; Torelli, L.; Maestro, A.; Zanon, D.; Barbi, E.; Maximova, N. Pentaglobin ® Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study. J. Clin. Med. 2020, 9, 1592. [Google Scholar] [CrossRef] [PubMed]
- Maximova, N.; Schillani, G.; Simeone, R.; Maestro, A.; Zanon, D. Comparison of Efficacy and Safety of Caspofungin Versus Micafungin in Pediatric Allogeneic Stem Cell Transplant Recipients: A Retrospective Analysis. Adv. Ther. 2017, 34, 1184–1199. [Google Scholar] [CrossRef]
- Braidotti, S.; Curci, D.; Maestro, A.; Zanon, D.; Maximova, N.; Di Paolo, A. Effect of early post-hematopoietic stem cell transplant tacrolimus concentration on transplant outcomes in pediatric recipients: One facility’s ten-year experience of immunosuppression with tacrolimus. Int. Immunopharmacol. 2024, 138, 112636. [Google Scholar] [CrossRef] [PubMed]
- Carlone, G.; Simeone, R.; Baraldo, M.; Maestro, A.; Zanon, D.; Barbi, E.; Maximova, N. Area-under-the-Curve-Based Mycophenolate Mofetil Dosage May Contribute to Decrease the Incidence of Graft-versus-Host Disease after Allogeneic Hematopoietic Cell Transplantation in Pediatric Patients. J. Clin. Med. 2021, 10, 406. [Google Scholar] [CrossRef]
- Schoemans, H.M.; Lee, S.J.; Ferrara, J.L.; Wolff, D.; Levine, J.E.; Schultz, K.R.; Shaw, B.E.; Flowers, M.E.; Ruutu, T.; Greinix, H.; et al. EBMT-NIH-CIBMTR Task Force position statement on standardized terminology & guidance for graft-versus-host disease assessment. Bone Marrow Transplant. 2018, 53, 1401–1415. [Google Scholar] [PubMed]
- Hutt, D. Engraftment, Graft Failure, and Rejection. In The European Blood and Marrow Transplantation Textbook for Nurses: Under the Auspices of EBMT; Kenyon, M., Babic, A., Eds.; Springer: Cham, Switzerland, 2018; pp. 259–270. [Google Scholar]
- Salmon, R.J. [J.L. Salmon in reply to the article by F. Herin, C. Vaysse et al. entitled “Damage repair in breast cancer has to evolve”, Gynecol Obstet Fertil 2021; 49(9): 698–702: Doi: 10.1016/j.gofs.2021.04.007]. Gynecol. Obstet. Fertil. Senol. 2021, 50, 104. [Google Scholar]
- Gandon, Y.; Olivié, D.; Guyader, D.; Aubé, C.; Oberti, F.; Sebille, V.; Deugnier, Y. Non-invasive assessment of hepatic iron stores by MRI. Lancet 2004, 363, 357–362. [Google Scholar] [CrossRef]
- Dissaux, B.; Eugène, F.; Ognard, J.; Gauvrit, J.Y.; Gentric, J.C.; Ferré, J.C. Assessment of 4D MR Angiography at 3T Compared with DSA for the Follow-up of Embolized Brain Dural Arteriovenous Fistula: A Dual-Center Study. Am. J. Neuroradiol. 2021, 42, 340–346. [Google Scholar] [CrossRef]
- Zeng, J.M.; Hapuarachchi, S.V.; Shafik, S.H.; Martin, R.E.; Kirk, K.; van Dooren, G.G.; Lehane, A.M. Identifying the major lactate transporter of Toxoplasma gondii tachyzoites. Sci. Rep. 2021, 11, 6787. [Google Scholar] [CrossRef]
- Lima, F.D.S.; Fock, R.A. A Review of the Action of Magnesium on Several Processes Involved in the Modulation of Hematopoiesis. Int. J. Mol. Sci. 2020, 21, 7084. [Google Scholar] [CrossRef]
- Ashique, S.; Kumar, S.; Hussain, A.; Mishra, N.; Garg, A.; Gowda, B.H.J.; Farid, A.; Gupta, G.; Dua, K.; Taghizadeh-Hesary, F. A narrative review on the role of magnesium in immune regulation, inflammation, infectious diseases, and cancer. J. Health Popul. Nutr. 2023, 42, 74. [Google Scholar] [CrossRef]
- Fatima, G.; Dzupina, A.; Alhmadi, H.B.; Magomedova, A.; Siddiqui, Z.; Mehdi, A.; Hadi, N. Magnesium Matters: A Comprehensive Review of Its Vital Role in Health and Diseases. Cureus 2024, 16, e71392. [Google Scholar] [CrossRef] [PubMed]
- Tam, M.; Gómez, S.; González-Gross, M.; Marcos, A. Possible roles of magnesium on the immune system. Eur. J. Clin. Nutr. 2003, 57, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.H.; Vaziri, N.D.; Martin, D.C.; Choi, S.; Alikhani, S. Hypomagnesemia and renal magnesium wasting in renal transplant recipients receiving cyclosporine. Am. J. Med. 1987, 83, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Aisa, Y.; Mori, T.; Nakazato, T.; Shimizu, T.; Yamazaki, R.; Ikeda, Y.; Okamoto, S. Effects of immunosuppressive agents on magnesium metabolism early after allogeneic hematopoietic stem cell transplantation. Transplantation 2005, 80, 1046–1050. [Google Scholar] [CrossRef]
- Woo, M.; Przepiorka, D.; Ippoliti, C.; Warkentin, D.; Khouri, I.; Fritsche, H.; Körbling, M. Toxicities of tacrolimus and cyclosporin A after allogeneic blood stem cell transplantation. Bone Marrow Transplant. 1997, 20, 1095–1098. [Google Scholar] [CrossRef]
- Huo, C.; Li, G.; Hu, Y.; Sun, H. The Impacts of Iron Overload and Ferroptosis on Intestinal Mucosal Homeostasis and Inflammation. Int. J. Mol. Sci. 2022, 23, 14195. [Google Scholar] [CrossRef] [PubMed]
- Cohlan, S.Q.; Jansen, V.; Dancis, J.; Piomelli, S. Microcytic anemia with erythroblastosis in offspring of magnesium-deprived rats. Blood 1970, 36, 500–506. [Google Scholar] [CrossRef]
- Kimura, M.; Yokoi, K. Iron accumulation in tissues of magnesium-deficient rats with dietary iron overload. Biol. Trace Element Res. 1996, 51, 177–197. [Google Scholar] [CrossRef]
- Ishizaki, N.; Kotani, M.; Funaba, M.; Matsui, T. Hepcidin expression in the liver of rats fed a magnesium-deficient diet. Br. J. Nutr. 2011, 106, 1169–1172. [Google Scholar] [CrossRef]
- Schneidawind, D.; Pierini, A.; Negrin, R.S. Regulatory T cells and natural killer T cells for modulation of GVHD following allogeneic hematopoietic cell transplantation. Blood 2013, 122, 3116–3121. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.; Castiglioni, S.; Locatelli, L.; Zocchi, M.; Mazur, A. Magnesium and inflammation: Advances and perspectives. Semin. Cell Dev. Biol. 2021, 115, 37–44. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Clinical Data | Cohort (n = 163) |
|---|---|
| Age at transplant: | |
| Median [IQR], years | 8.5 [4–17] |
| Gender, number (%): | |
| Male, n° (%) | 107 (66%) |
| Female, n° (%) | 56 (34%) |
| Primary disease, number (%): | |
| Acute lmphoblastic leukemia (ALL) | 70 (42.9%) |
| Acute myeloid leukemia (AML)/Myelodysplastic syndrome (MDS) | 31 (19.0%) |
| Inborn errors | 34 (20.8%) |
| Hemoglobinopathies | 26 (15.9%) |
| Lymphoma | 2 (1.2%) |
| Allogenic donor type, number (%): | |
| Matched unrelated donor | 76 (46.6%) |
| Matched related donor/Sibling donor | 68 (41.7%) |
| Haploidentical donor | 19 (11.6%) |
| Stem cell source, number (%): | |
| Bone marrow | 82 (50.3%) |
| Peripheral blood stem cell (PBSC) | 81 (49.7%) |
| Myeloablative conditioning regimen, number (%): | |
| MCHT-based | 111 (68.1%) |
| TBI-based | 52 (31.9%) |
| Immunosuppression, number (%): | |
| Cyclosporin A | 10 (6.1%) |
| Tacrolimus | 148 (90.8%) |
| Other | 5 (3.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curci, D.; Braidotti, S.; Paternuosto, G.; Flamigni, A.; Schillani, G.; Longo, A.; De Vita, N.; Maximova, N. Impact of Iron Overload and Hypomagnesemia Combination on Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Outcomes. Nutrients 2025, 17, 2462. https://doi.org/10.3390/nu17152462
Curci D, Braidotti S, Paternuosto G, Flamigni A, Schillani G, Longo A, De Vita N, Maximova N. Impact of Iron Overload and Hypomagnesemia Combination on Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Outcomes. Nutrients. 2025; 17(15):2462. https://doi.org/10.3390/nu17152462
Chicago/Turabian StyleCurci, Debora, Stefania Braidotti, Gilda Paternuosto, Anna Flamigni, Giulia Schillani, Antonella Longo, Nicole De Vita, and Natalia Maximova. 2025. "Impact of Iron Overload and Hypomagnesemia Combination on Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Outcomes" Nutrients 17, no. 15: 2462. https://doi.org/10.3390/nu17152462
APA StyleCurci, D., Braidotti, S., Paternuosto, G., Flamigni, A., Schillani, G., Longo, A., De Vita, N., & Maximova, N. (2025). Impact of Iron Overload and Hypomagnesemia Combination on Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Outcomes. Nutrients, 17(15), 2462. https://doi.org/10.3390/nu17152462