Serum 25-Hydroxyvitamin D Is Decreased with Metabolic Syndrome Following Anterior Cruciate Ligament Reconstruction

 ,
, 
Highlights
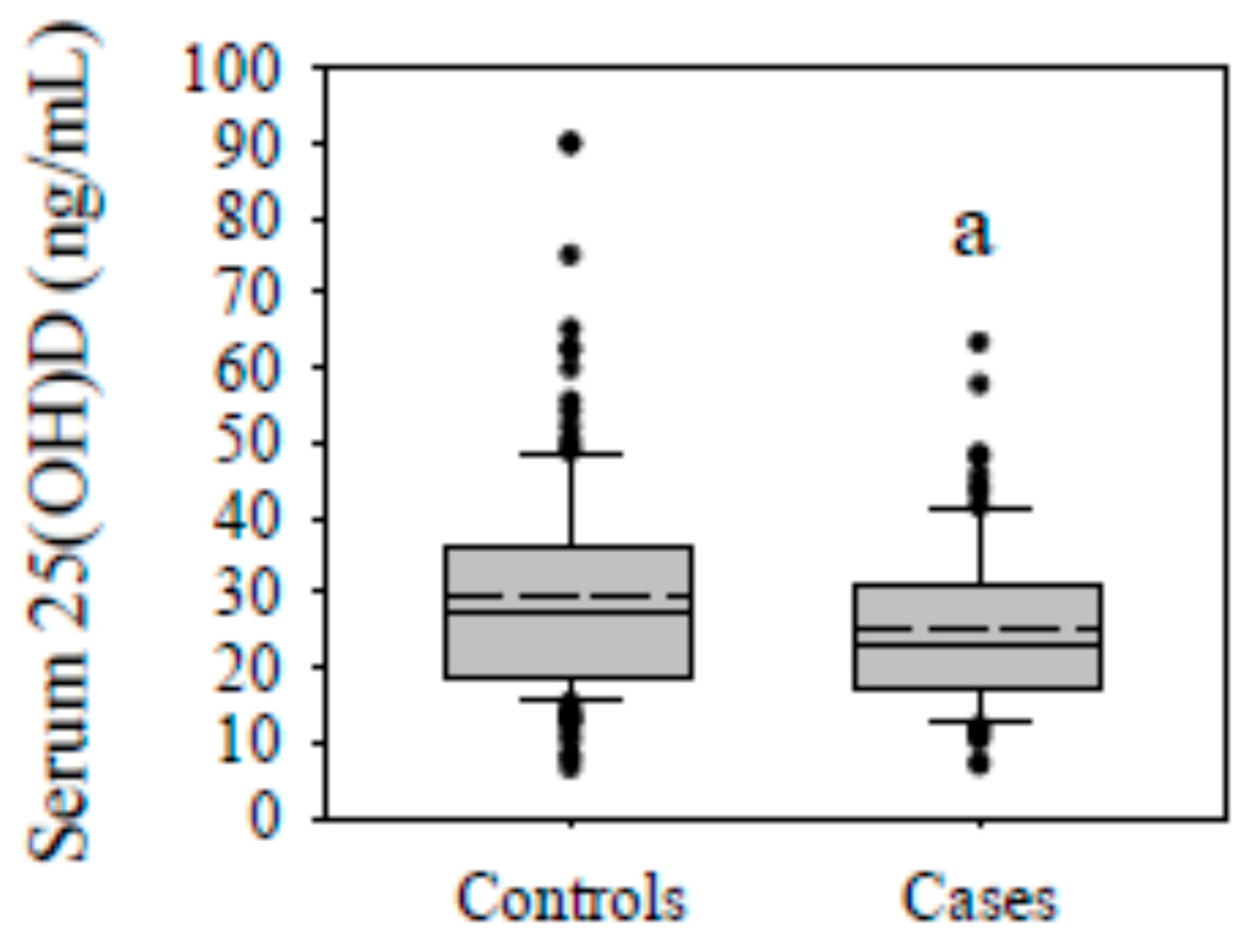
- Metabolic syndrome was associated with a decrease in serum 25-hydroxyvitamin D in patients that underwent anterior cruciate ligament reconstruction.
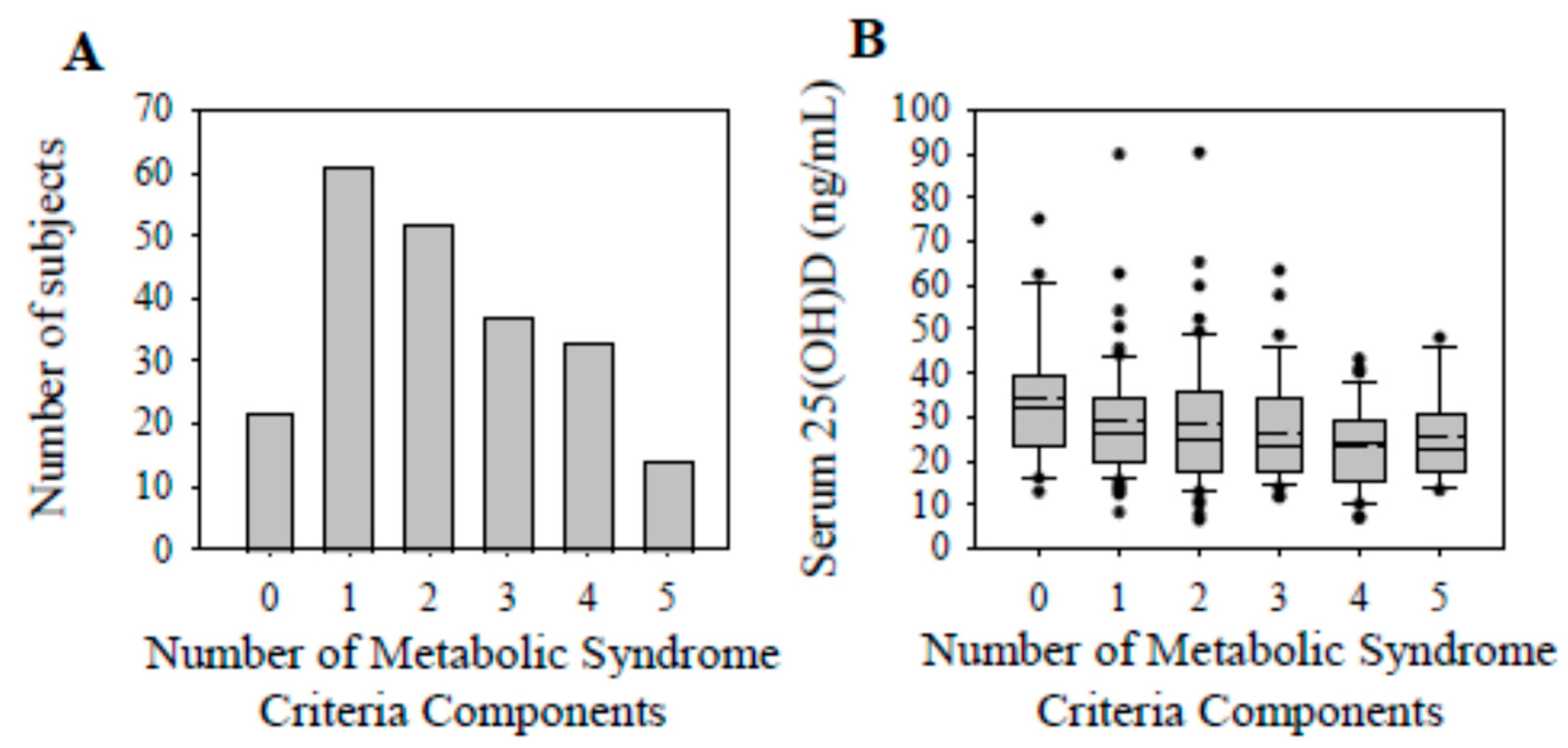
- The prevalence of vitamin D sufficiency decreased with accruing components of metabolic syndrome.
- The preliminary findings from this study could provide justification for assessing serum 25-hydroxyvitamin D following anterior cruciate ligament reconstruction in patients with metabolic syndrome and assist with risk stratification.
Abstract
1. Introduction
2. Materials and Methods
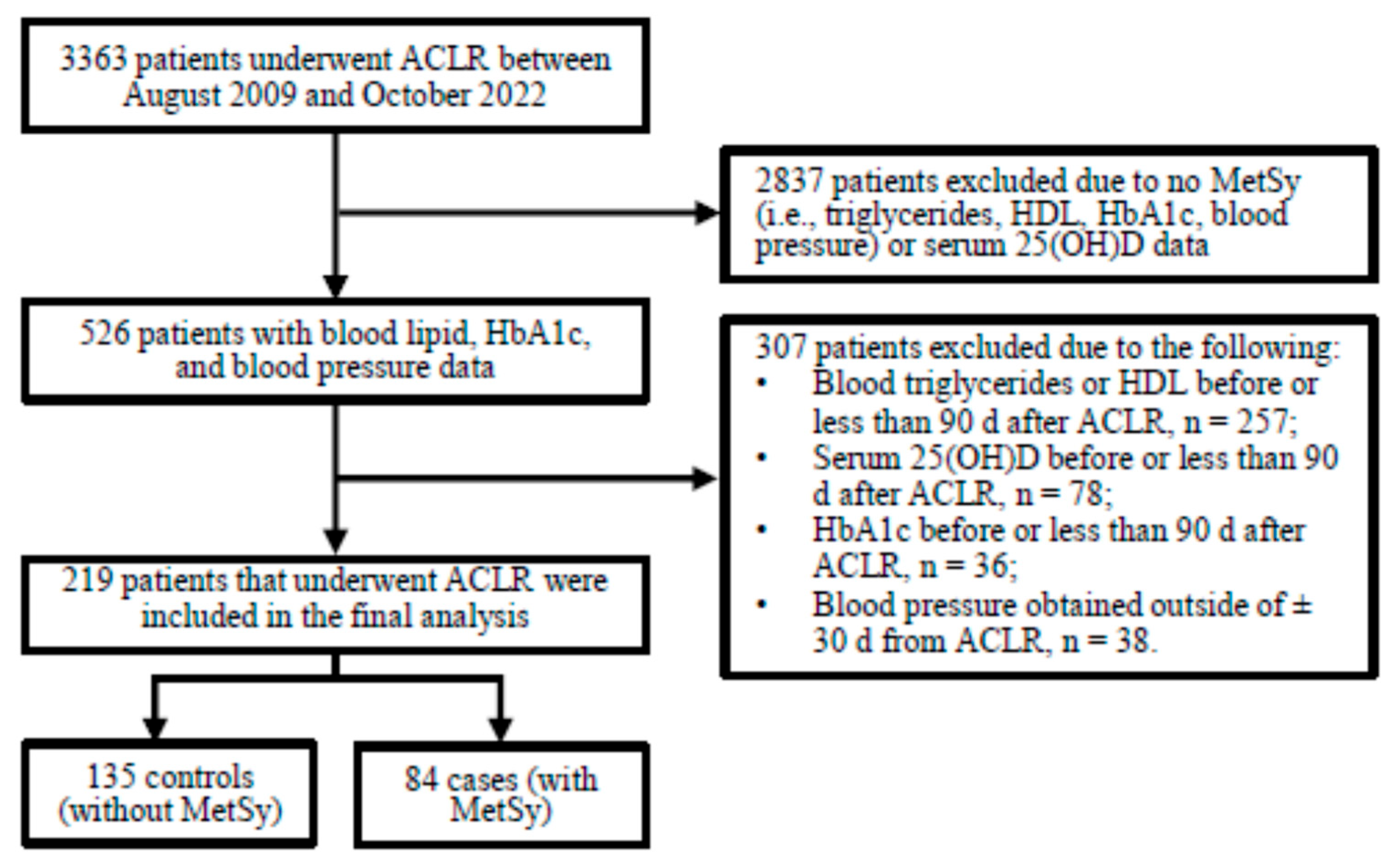
2.1. Subjects
2.2. Clinical Blood Chemistries and Blood Pressures
2.3. Metabolic Syndrome
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Serum 25(OH)D Concentrations and Vitamin D Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neeland, I.J.; Lim, S.; Tchernof, A.; Gastaldelli, A.; Rangaswami, J.; Ndumele, C.E.; Powell-Wiley, T.M.; Després, J.-P. Metabolic syndrome. Nat. Rev. Dis. Primers 2024, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Nolan, P.B.; Carrick-Ranson, G.; Stinear, J.W.; Reading, S.A.; Dalleck, L.C. Prevalence of metabolic syndrome and metabolic syndrome components in young adults: A pooled analysis. Prev. Med. Rep. 2017, 7, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Cheung, B.M.Y.; Wat, N.M.S.; Tam, S.; Thomas, G.N.; Leung, G.M.; Cheng, C.H.; Woo, J.; Janus, E.D.; Lau, C.P.; Lam, T.H.; et al. Components of the metabolic syndrome predictive of its development: A 6-year longitudinal study in Hong Kong Chinese. Clin. Endocrinol. 2008, 68, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Gündogan, K.; Bayram, F.; Capak, M.; Tanriverdi, F.; Karaman, A.; Ozturk, A.; Altunbas, H.; Gökce, C.; Kalkan, A.; Yazici, C. Prevalence of metabolic syndrome in the Mediterranean region of Turkey: Evaluation of hypertension, diabetes mellitus, obesity, and dyslipidemia. Metab. Syndr. Relat. Disord. 2009, 7, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Tian, J.; Mattap, S.M.; Cicuttini, F.; Jones, G. Association between metabolic syndrome and knee structural change on MRI. Rheumatology 2020, 59, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, N.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Nakamura, K.; Akune, T. Accumulation of metabolic risk factors such as overweight, hypertension, dyslipidaemia, and impaired glucose tolerance raises the risk of occurrence and progression of knee osteoarthritis: A 3-year follow-up of the ROAD study. Osteoarthr. Cartil. 2012, 20, 1217–1226. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef] [PubMed]
- Friel, N.A.; Chu, C.R. The role of ACL injury in the development of posttraumatic knee osteoarthritis. Clin. Sports Med. 2013, 32, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.G.; Fields, S.K.; Yard, E.E.; Comstock, R.D. Epidemiology of knee injuries among boys and girls in US high school athletics. Am. J. Sports Med. 2008, 36, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Ajani, U.A.; McGuire, L.C.; Liu, S. Concentrations of serum vitamin D and the metabolic syndrome among U.S. adults. Diabetes Care 2005, 28, 1228–1230. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, N.; Raghavan, R.; Zhang, G.; Talegawkar, S.A.; Jacques, P.F. Vitamin D status and prevalence of metabolic syndrome by race and Hispanic origin in US adults: Findings from the 2007–2014 NHANES. Am. J. Clin. Nutr. 2022, 116, 1400–1408. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Su, D.; Huang, L.; He, M.; Han, D.; Zhao, D.; Zou, Y.; Zhang, R. Prevalence of metabolic syndrome with different serum vitamin D levels in middle-aged and older adults. Nutr. Metab. 2025, 22, 4. [Google Scholar] [CrossRef] [PubMed]
- Kayaniyil, S.; Harris, S.B.; Retnakaran, R.; Vieth, R.; Knight, J.A.; Gerstein, H.C.; Perkins, B.A.; Zinman, B.; Hanley, A.J. Prospective association of 25(OH)D with metabolic syndrome. Clin. Endocrinol. 2014, 80, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Jiang, S.; Dong, C.; Jiang, D. Association between fat-soluble vitamins and metabolic syndromes in US adults: A cross-section study from NHANES database. BMC Endocr. Disord. 2024, 24, 178. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-M.; Chang, C.-S.; Chang, Y.-F.; Wu, S.-J.; Chiu, C.-J.; Hou, M.-T.; Chen, C.-Y.; Liu, P.-Y.; Wu, C.-H. Inverse Relationship between Metabolic Syndrome and 25-Hydroxyvitamin D Concentration in Elderly People without Vitamin D deficiency. Sci. Rep. 2018, 8, 17052. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.L.; May, H.T.; Horne, B.D.; Bair, T.L.; Hall, N.L.; Carlquist, J.F.; Lappé, D.L.; Muhlestein, J.B.; Intermountain Heart Collaborative (IHC) Study Group. Relation of vitamin D deficiency to cardiovascular risk factors, disease status, and incident events in a general healthcare population. Am. J. Cardiol. 2010, 106, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Kuhn, J.; Dreier, J.; Knabbe, C.; Gummert, J.F.; Börgermann, J. Vitamin D status and the risk of major adverse cardiac and cerebrovascular events in cardiac surgery. Eur. Heart J. 2013, 34, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Resurrection of vitamin D deficiency and rickets. J. Clin. Investig. 2006, 116, 2062–2072. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Bogunovic, L.; Kim, A.D.; Beamer, B.S.; Nguyen, J.; Lane, J.M. Hypovitaminosis D in patients scheduled to undergo orthopaedic surgery: A single-center analysis. J. Bone Jt. Surg. Am. 2010, 92, 2300–2304. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Martins, T.B.; Hill, H.R.; Kjeldsberg, C.R.; Trawick, R.H.; Weaver, L.K.; Traber, M.G. Low vitamin D impairs strength recovery after anterior cruciate ligament surgery. J. Evid.-Based Complement. Altern. Med. 2011, 16, 201–209. [Google Scholar] [CrossRef]
- Wen, Y.; Latham, C.M.; Moore, A.N.; Thomas, N.T.; Lancaster, B.D.; Reeves, K.A.; Keeble, A.R.; Fry, C.S.; Johnson, D.L.; Thompson, K.L.; et al. Vitamin D status associates with skeletal muscle loss after anterior cruciate ligament reconstruction. JCI Insight 2023, 8, e170518. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Martins, T.B.; Kjeldsberg, C.R.; Trawick, R.H.; Hill, H.R. Circulating interferon-gamma correlates with 1,25(OH)D and the 1,25(OH)D-to-25(OH)D ratio. Cytokine 2012, 60, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Maddah, S.; Mahdizadeh, J. Association of Metabolic Syndrome and Its Components with Knee Osteoarthritis. Acta Med. Iran. 2015, 53, 743–748. [Google Scholar] [PubMed]
- Gierach, M.; Junik, R. Metabolic syndrome in women—correlation between BMI and waist circumference. Endokrynol. Pol. 2022, 73, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Kuenen, J.; Borg, R.; Zheng, H.; Schoenfeld, D.; Heine, R.J.; for the A1c-Derived Average Glucose (ADAG) Study Group. Translating the A1C assay into estimated average glucose values. Diabetes Care 2008, 31, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Demay, M.B.; Pittas, A.G.; Bikle, D.D.; Diab, D.L.; Kiely, M.E.; Lazaretti-Castro, M.; Lips, P.; Mitchell, D.M.; Murad, M.H.; Powers, S.; et al. Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2024, 109, 1907–1947. [Google Scholar] [CrossRef] [PubMed]
- McCartney, C.R.; McDonnell, M.E.; Corrigan, M.D.; Lash, R.W. Vitamin D Insufficiency and Epistemic Humility: An Endocrine Society Guideline Communication. J. Clin. Endocrinol. Metab. 2024, 109, 1948–1954. [Google Scholar] [CrossRef] [PubMed]
- Albright, J.A.; Chang, K.; Byrne, R.A.; Quinn, M.S.; Meghani, O.; Daniels, A.H.; Owens, B.D. A Diagnosis of Vitamin D Deficiency Is Associated With Increased Rates of Anterior Cruciate Ligament Tears and Reconstruction Failure. Arthroscopy 2023, 39, 2477–2486. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Choi, C.-Y.; Man, G.C.-W.; He, X.; Yu, M.; Cao, M.; Wang, Q.; Ng, J.P.; Yung, P.S.-H.; Ong, M.T.-Y. Serum vitamin D insufficiency is correlated with quadriceps neuromuscular functions in patients with anterior cruciate ligament injury: A preliminary study. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2024, 35, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Schmitt, L.C.; Burnett, Z.; Milliron, E.M.; Cavendish, P.A.; Magnussen, R.A.; Kaeding, C.C.; Flanigan, D.C.; Barker, T. Vitamin D Deficiency after Anterior Cruciate Ligament Reconstruction Associates with Knee Osteoarthritis: A Retrospective Study. Nutrients 2024, 16, 3029. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Singhal, A.; Kapoor, A.; Bohat, V.; Masih, G.D.; Mehta, R. Vitamin D deficiency in athletes and its impact on outcome of Anterior Cruciate Ligament surgery. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Zhang, Y.; Niu, J.; Goggins, J.; Amin, S.; LaValley, M.P.; Guermazi, A.; Genant, H.; Gale, D.; Felson, D.T. Increase in bone marrow lesions associated with cartilage loss: A longitudinal magnetic resonance imaging study of knee osteoarthritis. Arthritis Rheum. 2006, 54, 1529–1535. [Google Scholar] [CrossRef] [PubMed]
- Michaud, A.; Tordjman, J.; Pelletier, M.; Liu, Y.; Laforest, S.; Noël, S.; Le Naour, G.; Bouchard, C.; Clément, K.; Tchernof, A. Relevance of omental pericellular adipose tissue collagen in the pathophysiology of human abdominal obesity and related cardiometabolic risk. Int. J. Obes. 2016, 40, 1823–1831. [Google Scholar] [CrossRef] [PubMed]
- Harman-Boehm, I.; BlühEr, M.; Redel, H.; Sion-Vardy, N.; Ovadia, S.; Avinoach, E.; Shai, I.; KlötIng, N.; Stumvoll, M.; Bashan, N.; et al. Macrophage infiltration into omental versus subcutaneous fat across different populations: Effect of regional adiposity and the comorbidities of obesity. J. Clin. Endocrinol. Metab. 2007, 92, 2240–2247. [Google Scholar] [CrossRef] [PubMed]
- Tchernof, A.; Després, J.-P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.F.; Mehta, N.N.; Baker, D.G.; Toedter, G.; Shults, J.; Von Feldt, J.M.; Leonard, M.B. Vitamin D, metabolic dyslipidemia, and metabolic syndrome in rheumatoid arthritis. Am. J. Med. 2012, 125, 1036.e9–1036.e15. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Grimnes, G. Vitamin D and metabolic health with special reference to the effect of vitamin D on serum lipids. Prog. Lipid Res. 2011, 50, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Jaimungal, S.; Wehmeier, K.; Mooradian, A.D.; Haas, M.J. The emerging evidence for vitamin D—mediated regulation of apolipoprotein A-I synthesis. Nutr. Res. 2011, 31, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Jiao, Y.; Li, J. Higher Genetically Predicted Triglycerides, LDL, and HDL Increase the Vitamin D Deficiency: A Mendelian Randomization Study. Front. Nutr. 2022, 9, 862942. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Zhao, J.; Zhuo, S.; Hu, Z.; Ouyang, S.; Wunier; Yu, S.; Chen, Y.; Li, Y.; Le, Y. High Fat Diet and High Cholesterol Diet Reduce Hepatic Vitamin D-25-Hydroxylase Expression and Serum 25-Hydroxyvitamin D3 Level through Elevating Circulating Cholesterol, Glucose, and Insulin Levels. Mol. Nutr. Food Res. 2021, 65, 2100220. [Google Scholar] [CrossRef] [PubMed]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; García-Recio, E.; De Luna-Bertos, E.; Ruiz, C.; Illescas-Montes, R. Role of Vitamin D in the Metabolic Syndrome. Nutrients 2021, 13, 830. [Google Scholar] [CrossRef] [PubMed]
- Maki, K.C.; Rubin, M.R.; Wong, L.G.; McManus, J.F.; Jensen, C.D.; Marshall, J.W.; Lawless, A. Serum 25-hydroxyvitamin D is independently associated with high-density lipoprotein cholesterol and the metabolic syndrome in men and women. J. Clin. Lipidol. 2009, 3, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Prasad, P.; Kochhar, A. Interplay of vitamin D and metabolic syndrome: A review. Diabetes Metab. Syndr. 2016, 10, 105–112. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Controls | Cases | p-Value | |
|---|---|---|---|
| n (f/m) | 135 (83/52) | 84 (43/41) | 0.16 * |
| Age, y | 37.4 (15.1) | 35.5 (15.7) | 0.55 |
| Height, m | 1.70 (0.14) | 1.70 (0.15) | 0.32 |
| Body Mass, kg | 75.3 (23.6) | 99.8 (27.6) | <0.01 |
| BMI, kg/m2 | 26.0 (6.0) | 33.9 (8.6) | <0.01 |
| BMI Classifications | <0.01 | ||
| Underweight (≤18.5 kg/m2), n (%) | 2 (1.5) | 0 | |
| Healthy Weight (18.5–24.9 kg/m2), n (%) | 52 (38.5) | 8 (9.5) | |
| Overweight (25.0–29.9 kg/m2), n (%) | 57 (42.2) | 8 (9.5) | |
| Obese (30.0–39.9 kg/m2), n (%) | 21 (15.6) | 49 (58.3) | |
| Severe Obesity (≥40.0 kg/m2), n (%) | 3 (2.2) | 19 (22.6) | |
| Systolic Blood Pressure, mmHg | 123 (19) | 138 (16) | <0.01 |
| Diastolic Blood Pressure, mmHg | 72 (12) | 78 (10) | <0.01 |
| Cholesterol, mg/dL | 184 (43) | 193 (45) | 0.27 |
| Triglycerides, mg/dL | 83.0 (46.5) | 168 (132) | <0.01 |
| HDL, mg/dL | 56.0 (21.8) | 43.0 (130) | <0.01 |
| LDL, mg/dL | 103 (49) | 103 (43) | 0.46 |
| Cholesterol/HDL-C Ratio | 3.05 (1.30) | 4.20 (1.40) | <0.01 |
| Non-HDLC, mg/dL | 124 (51) | 140 (40) | <0.01 |
| HbA1c, % | 5.20 (0.50) | 5.50 (0.40) | <0.01 |
| HbA1c Classification | <0.01 | ||
| Normal (<5.7%), n (%) | 119 (88.2) | 60 (71.4) | |
| Prediabetic (5.7–6.4%), n (%) | 15 (11.1) | 17 (20.2) | |
| Diabetic (>6.4%), n (%) | 1 (0.7) | 7 (8.3) | |
| Estimated Fasting Glucose, mg/dL | 103 (14) | 111 (11) | <0.01 |
| Vitamin D Status | 0.06 | ||
| Deficient, n (%) | 35 (25.9) | 34 (40.5) | |
| Insufficient, n (%) | 49 (36.3) | 28 (33.3) | |
| Sufficient, n (%) | 51 (37.8) | 22 (26.2) | |
| Season of 25(OH)D Assessment | 0.54 | ||
| Fall, n (%) | 33 (24.4) | 24 (28.6) | |
| Winter, n (%) | 29 (21.5) | 21 (25.0) | |
| Spring, n (%) | 34 (25.2) | 22 (26.2) | |
| Summer, n (%) | 39 (28.9) | 17 (20.2) |
| Serum 25(OH)D (ng/mL) | p-Value * | ||
|---|---|---|---|
| BMI | 0.26 | ||
| <30 kg/m2 (n = 127) | 26.0 (16.1) | ||
| ≥30 kg/m2 (n = 92) | 24.0 (15.8) | ||
| Triglycerides | 0.03 | ||
| <150 mg/dL (n = 156) | 26.5 (17.5) | ||
| ≥150 mg/dL (n = 63) | 23.6 (12.7) | ||
| HDL | 0.02 | ||
| males ≥ 40 and females ≥ 50 mg/dL (n = 154) | 25.7 (17.3) | ||
| males < 40 and females < 50 mg/dL (n = 65) | 25.0 (13.2) | ||
| Blood pressure | 0.11 | ||
| SBP < 130 and DBP < 85 mmHg (n = 107) | 27.4 (17.4) | ||
| SBP ≥ 130 or DBP ≥ 85 mmHg (n = 112) | 23.5 (14.9) | ||
| Estimated fasting glucose | 0.13 | ||
| <100 mg/dL (n = 73) | 28.2 (13.3) | ||
| ≥100 mg/dL (n = 146) | 23.8 (16.0) | ||
| Number of MetSy Components | Vitamin D Status | Row p-Value | ||
|---|---|---|---|---|
| Deficient | Insufficient | Sufficient | ||
| n = 69 | n = 77 | n = 73 | ||
| 0, n = 22 (row %) | 3 (13.6) | 7 (31.8) | 12 (54.6) | 0.06 |
| (column %) | (4.4) | (9.1) | (16.4) | |
| 1, n = 61 (row %) | 15 (24.6) | 24 (39.3) | 22 (36.1) | 0.33 |
| (column %) | (21.7) | (31.2) | (30.1) | |
| 2, n = 52 (row %) | 17 (32.7) | 18 (34.6) | 17 (32.7) | 0.98 |
| (column %) | (24.6) | (23.4) | (23.3) | |
| 3, n = 37 (row %) | 16 (43.2) | 9 (24.3) | 12 (32.4) | 0.37 |
| (column %) | (23.2) | (11.7) | (16.4) | |
| 4, n = 33 (row %) | 13 (39.4) | 13 (39.4) | 7 (21.2) | 0.34 |
| (column %) | (18.8) | (16.9) | (9.6) | |
| 5, n = 14 (row %) | 5 (35.7) | 6 (42.9) | 3 (21.4) | 0.61 |
| (column %) | (7.3) | (7.8) | (4.1) | |
| Column p-Value | <0.01 | <0.01 | <0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.; Mantor, A.; Price, H.; Kaeding, C.C.; Magnussen, R.A.; Flanigan, D.C.; Barker, T. Serum 25-Hydroxyvitamin D Is Decreased with Metabolic Syndrome Following Anterior Cruciate Ligament Reconstruction. Nutrients 2025, 17, 2410. https://doi.org/10.3390/nu17152410
Bae S, Mantor A, Price H, Kaeding CC, Magnussen RA, Flanigan DC, Barker T. Serum 25-Hydroxyvitamin D Is Decreased with Metabolic Syndrome Following Anterior Cruciate Ligament Reconstruction. Nutrients. 2025; 17(15):2410. https://doi.org/10.3390/nu17152410
Chicago/Turabian StyleBae, Sonu, Anthony Mantor, Hayden Price, Christopher C. Kaeding, Robert A. Magnussen, David C. Flanigan, and Tyler Barker. 2025. "Serum 25-Hydroxyvitamin D Is Decreased with Metabolic Syndrome Following Anterior Cruciate Ligament Reconstruction" Nutrients 17, no. 15: 2410. https://doi.org/10.3390/nu17152410
APA StyleBae, S., Mantor, A., Price, H., Kaeding, C. C., Magnussen, R. A., Flanigan, D. C., & Barker, T. (2025). Serum 25-Hydroxyvitamin D Is Decreased with Metabolic Syndrome Following Anterior Cruciate Ligament Reconstruction. Nutrients, 17(15), 2410. https://doi.org/10.3390/nu17152410