

Designing and Developing a Population/Literature-Based Westernized Diet Index (WDI) and Its Relevance for Cardiometabolic Health



Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
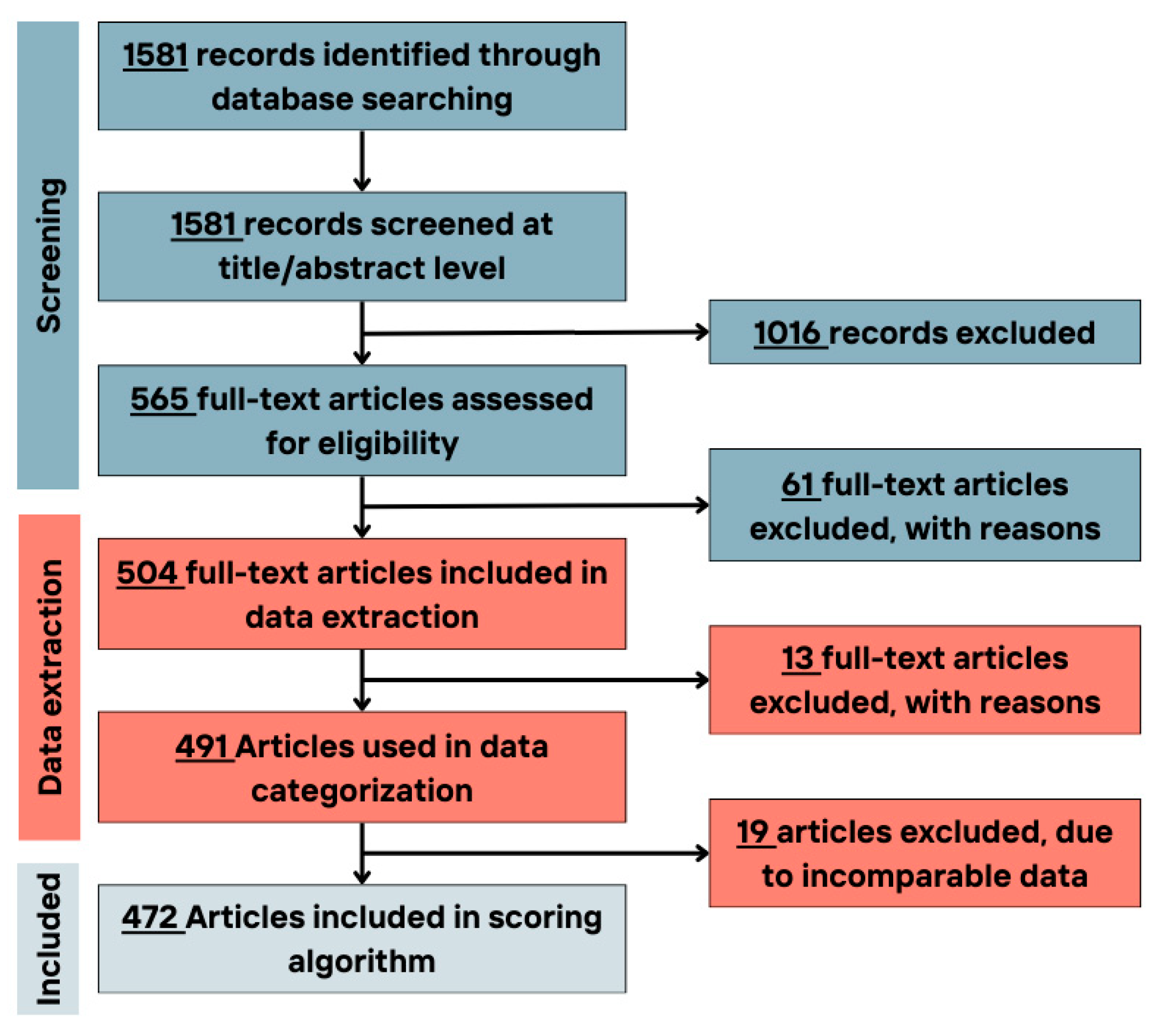
2.2. Literature Review and Selection
2.3. Search Strategy
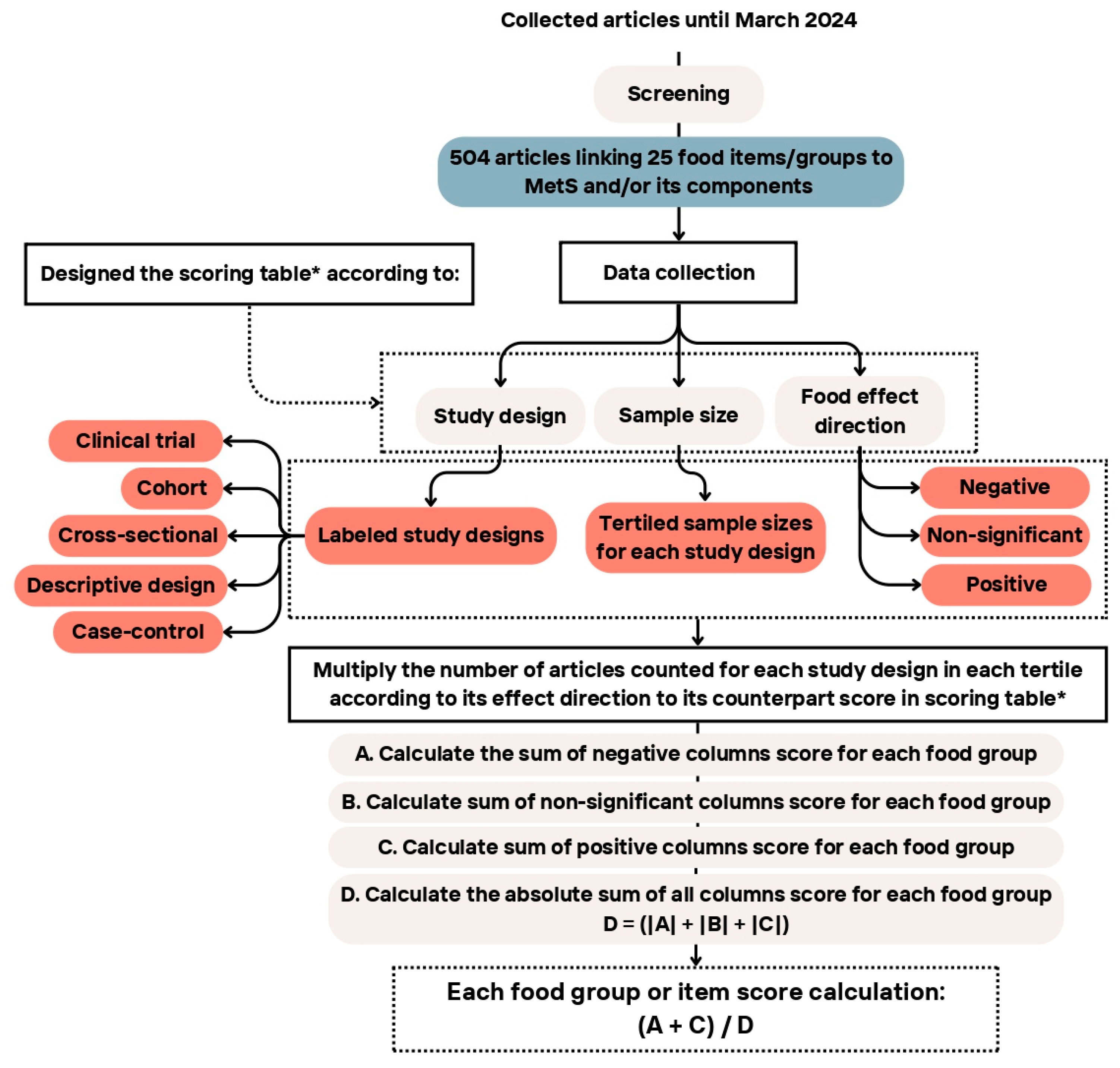
2.4. Data Extraction
2.5. Scoring Algorithm
2.6. MetS/Its Components and Score Calculation
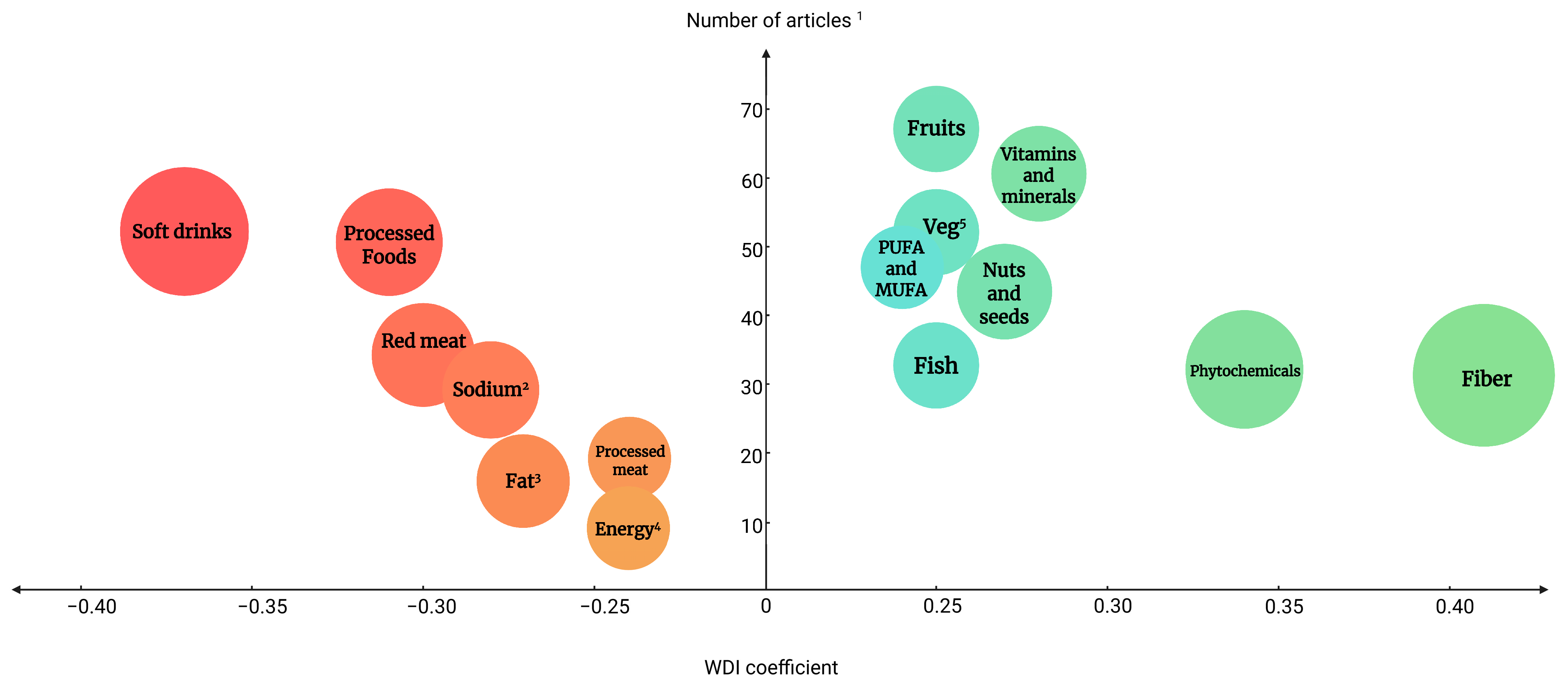
3. Results
4. Discussion
4.1. Negative Coefficients of the WDI
4.2. Positive Coefficients of the WDI
4.3. The WDI Compared to Other Indices
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kontis, V.; Mathers, C.D.; Rehm, J.; Stevens, G.A.; Shield, K.D.; Bonita, R.; Riley, L.M.; Poznyak, V.; Beaglehole, R.; Ezzati, M. Contribution of six risk factors to achieving the 25 × 25 non-communicable disease mortality reduction target: A modelling study. Lancet 2014, 384, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Noland, D.; Drisko, J.A.; Wagner, L. Integrative and Functional Medical Nutrition Therapy: Principles and Practices; Springer Nature: Berlin/Heidelberg, Germany, 2020; pp. 17–29. [Google Scholar]
- Boudreau, D.M.; Malone, D.C.; Raebel, M.A.; Fishman, P.A.; Nichols, G.A.; Feldstein, A.C.; Boscoe, A.N.; Ben-Joseph, R.H.; Magid, D.J.; Okamoto, L.J. Health care utilization and costs by metabolic syndrome risk factors. Met. Syndr. Rel. Dis. 2009, 7, 305–314. [Google Scholar] [CrossRef]
- Vollset, S.E.; Ababneh, H.S.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasian, M.; Abbastabar, H.; Al Magied, A.H.A.; ElHafeez, S.A.; Abdelkader, A. Burden of disease scenarios for 204 countries and territories, 2022–2050: A forecasting analysis for the global burden of disease study 2021. Lancet 2024, 403, 2204–2256. [Google Scholar] [CrossRef] [PubMed]
- Szypowska, A.; Zatońska, K.; Szuba, A.; Regulska-Ilow, B. Dietary inflammatory index (dii)(®) and metabolic syndrome in the selected population of polish adults: Results of the pure poland sub-study. Int J. Environ. Res. Public Health 2023, 20, 1056. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Cur. Hypert. Rep. 2018, 20, 1–8. [Google Scholar] [CrossRef]
- Okunogbe, A.; Nugent, R.; Spencer, G.; Powis, J.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for 161 countries. BMJ Global Health 2022, 7, e009773. [Google Scholar] [CrossRef]
- Ärnlöv, J.G.; Collaborators, R.F. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Jamali, Z.; Ayoobi, F.; Jalali, Z.; Bidaki, R.; Lotfi, M.A.; Esmaeili-Nadimi, A.; Khalili, P. Metabolic syndrome: A population-based study of prevalence and risk factors. Sci. Rep. 2024, 14, 3987. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B., Jr.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C., Jr.; Stone, N.J. Implications of recent clinical trials for the national cholesterol education program adult treatment panel iii guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef]
- Oggioni, C.; Lara, J.; Wells, J.; Soroka, K.; Siervo, M. Shifts in population dietary patterns and physical inactivity as determinants of global trends in the prevalence of diabetes: An ecological analysis. Nutr. Metab. Cardiovas. Dis. 2014, 24, 1105–1111. [Google Scholar] [CrossRef]
- Dai, C.; Sun, X.; Wu, L.; Chen, J.; Hu, X.; Ding, F.; Chen, W.; Lei, H.; Li, X. Associations between exposure to various air pollutants and risk of metabolic syndrome: A systematic review and meta-analysis. Int. Arch Occ. Environ. Healthy 2024, 97, 621–639. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.M.; Sakhvidi, M.J.Z.; Ashraf, S.; Dadvand, P.; Browning, M.H.; Alam, M.A.; Bell, M.L.; James, P.; Astell-Burt, T. Impact of green space and built environment on metabolic syndrome: A systematic review with meta-analysis. Sci. Total Environ. 2024, 23, 170977. [Google Scholar] [CrossRef] [PubMed]
- Cleven, L.; Krell-Roesch, J.; Schmidt, S.C.E.; Dziuba, A.; Bös, K.; Jekauc, D.; Woll, A. Longitudinal association between physical activity and the risk of incident metabolic syndrome in middle-aged adults in germany. Sci. Rep. 2022, 12, 19424. [Google Scholar] [CrossRef]
- Azzam, A. Is the world converging to a ‘western diet’? Public Health Nutr. 2021, 24, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Rakhra, V.; Galappaththy, S.L.; Bulchandani, S.; Cabandugama, P.K. Obesity and the western diet: How we got here. Mo. Med. 2020, 117, 536–538. [Google Scholar]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.-L.; Foka, A.J.; Ndoadoumgue, A.L. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals. Diab. Res. Clin. Pract. 2022, 188, 109924. [Google Scholar] [CrossRef]
- Database, G.D. Dietary Data by Country. 2016. Available online: https://globaldietarydatabase.org/our-data/data-visualizations/dietary-data-country (accessed on 13 July 2024).
- Bener, A.; Zirie, M.; Musallam, M.; Khader, Y.S.; Al-Hamaq, A.O. Prevalence of metabolic syndrome according to adult treatment panel iii and international diabetes federation criteria: A population-based study. Metab. Syndr. Rel. Dis. 2009, 7, 221–230. [Google Scholar] [CrossRef]
- Bhalwar, R. Metabolic syndrome: The indian public health perspective. Med. J. Armed For. India 2020, 76, 8–16. [Google Scholar] [CrossRef]
- Ali, N.; Taher, A.; Trisha, A.D.; Koley, N.J.; Fariha, K.A.; Islam, F. Prevalence of metabolic syndrome and its related factors in bangladeshi adults: A cross-sectional study. Endocrinol. Diabetes Metab. 2024, 7, e00491. [Google Scholar] [CrossRef]
- Ortiz-Rodríguez, M.A.; Bautista-Ortiz, L.F.; Villa, A.R.; Antúnez-Bautista, P.K.; Aldaz-Rodríguez, M.V.; Estrada-Luna, D.; Denova-Gutiérrez, E.; Camacho-Díaz, B.H.; Martínez-Salazar, M.F. Prevalence of metabolic syndrome among mexican adults. Metab. Syndr. Rel. Dis. 2022, 20, 264–272. [Google Scholar] [CrossRef]
- Mehata, S.; Shrestha, N.; Mehta, R.K.; Bista, B.; Pandey, A.R.; Mishra, S.R. Prevalence of the metabolic syndrome and its determinants among nepalese adults: Findings from a nationally representative cross-sectional study. Sci. Rep. 2018, 8, 14995. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nut. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef]
- Vahid, F.; Rahmani, D.; Davoodi, S.H. The correlation between serum inflammatory, antioxidant, glucose handling biomarkers, and dietary antioxidant index (dai) and the role of dai in obesity/overweight causation: Population-based case-control study. Int. J. Obes. 2021, 45, 2591–2599. [Google Scholar] [CrossRef] [PubMed]
- Vahid, F.; Rahmani, D.; Davoodi, S.H. Validation of dietary antioxidant index (dai) and investigating the relationship between dai and the odds of gastric cancer. Nutr. Metab. 2020, 17, 102. [Google Scholar] [CrossRef]
- Al Kudsee, K.; Vahid, F.; Bohn, T. High adherence to the mediterranean diet and alternative healthy eating index are associated with reduced odds of metabolic syndrome and its components in participants of the oriscav-lux2 study. Front. Nutr. 2022, 9, 1087985. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef]
- Chain, E.P.; Knutsen, H.K.; Alexander, J.; Barregård, L.; Bignami, M.; Brüschweiler, B.; Ceccatelli, S.; Cottrill, B.; Dinovi, M.; Edler, L. Risks for public health related to the presence of tetrodotoxin (ttx) and ttx analogues in marine bivalves and gastropods. Eur. Food Saf. Authority (EFSA) J. 2017, 15, e04752. [Google Scholar] [CrossRef]
- Kohl, C.; McIntosh, E.J.; Unger, S.; Haddaway, N.R.; Kecke, S.; Schiemann, J.; Wilhelm, R. Correction to: Online tools supporting the conduct and reporting of systematic reviews and systematic maps: A case study on cadima and review of existing tools. Environ. Evid. 2018, 7, 1. [Google Scholar] [CrossRef]
- Jowshan, M.R.; Rafraf, M.; Hashemi, A.H.; Hajjarzadeh, S.; Asghari-Jafarabadi, M.; Asghari, S. Association between healthy eating index-2015 scores and metabolic syndrome among iranian women: A cross-sectional study. BMC Womens Health 2024, 24, 30. [Google Scholar] [CrossRef]
- Alkerwi, A.; Vernier, C.; Crichton, G.E.; Sauvageot, N.; Shivappa, N.; Hébert, J.R. Cross-comparison of diet quality indices for predicting chronic disease risk: Findings from the observation of cardiovascular risk factors in luxembourg (oriscav-lux) study. Br. J. Nutr. 2015, 113, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Mehrdad, M.; Vahid, F.; Shivappa, N.; Hébert, J.R.; Fardaei, M.; Eftekhari, M.H. High dietary inflammatory index (dii) scores increase odds of overweight in adults with rs9939609 polymorphism of fto gene. Clin. Nutr. ESPEN 2021, 42, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. The role of sugar-sweetened beverages in the global epidemics of obesity and chronic diseases. Nature Rev. Endocrinol. 2022, 18, 205–218. [Google Scholar] [CrossRef]
- Gugliucci, A. Sugar and dyslipidemia: A double-hit, perfect storm. J. Clin. Med. 2023, 12, 5660. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Resolved: There is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes. Rev. 2013, 14, 606–619. [Google Scholar] [CrossRef]
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diab. Endocrinol. 2016, 4, 174–186. [Google Scholar] [CrossRef]
- Aminianfar, A.; Vahid, F.; Shayanfar, M.; Davoodi, S.H.; Mohammad-Shirazi, M.; Shivappa, N.; Sharifi, G.; Hebert, J.R.; Surkan, P.J.; Faghfoori, Z.; et al. The association between the dietary inflammatory index and glioma: A case-control study. Clin. Nutr. 2020, 39, 433–439. [Google Scholar] [CrossRef]
- Jha, P.; Flather, M.; Lonn, E.; Farkouh, M.; Yusuf, S. The antioxidant vitamins and cardiovascular disease: A critical review of epidemiologic and clinical trial data. Ann. Int. Med. 1995, 123, 860–872. [Google Scholar] [CrossRef]
- Aramburu, A.; Alvarado-Gamarra, G.; Cornejo, R.; Curi-Quinto, K.; Díaz-Parra, C.D.P.; Rojas-Limache, G.; Lanata, C.F. Ultra-processed foods consumption and health-related outcomes: A systematic review of randomized controlled trials. Front. Nutr. 2024, 11, 1421728. [Google Scholar] [CrossRef]
- Moubarac, J.C.; Martins, A.P.; Claro, R.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. Consumption of ultra-processed foods and likely impact on human health. Evidence from canada. Public Health Nutr. 2013, 16, 2240–2248. [Google Scholar] [CrossRef]
- Juul, F.N.P.; Martinez-Steele, E.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption among us adults from 2001 to 2018. Am. J. Clin. Nutr. 2022, 115, 211–221. [Google Scholar] [CrossRef]
- Slimani, N.; Deharveng, G.; Southgate, D.; Biessy, C.; Chajès, V.; Van Bakel, M.; Boutron-Ruault, M.; McTaggart, A.; Grioni, S.; Verkaik-Kloosterman, J. Contribution of highly industrially processed foods to the nutrient intakes and patterns of middle-aged populations in the european prospective investigation into cancer and nutrition study. Eur. J. Clin. Nutr. 2009, 63, S206–S250. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- Hess, J.M.; Comeau, M.E.; Casperson, S.; Slavin, J.L.; Johnson, G.H.; Messina, M.; Raatz, S.; Scheett, A.J.; Bodensteiner, A.; Palmer, D.G. Dietary guidelines meet nova: Developing a menu for a healthy dietary pattern using ultra-processed foods. J. Nutr. 2023, 153, 2472–2481. [Google Scholar] [CrossRef] [PubMed]
- Cacau, L.T.; Marcadenti, A.; Bersch-Ferreira, A.C.; Weber, B.; de Almeida, J.C.; Rodrigues, C.C.R.; Lotufo, P.A.; Bensenor, I.M.; Marchioni, D.M. The aha recommendations for a healthy diet and ultra-processed foods: Building a new diet quality index. Front. Nutr. 2022, 9, 804121. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.L. Rising consumption of meat and milk in developing countries has created a new food revolution. J. Nutr. 2003, 133, 3907s–3910s. [Google Scholar] [CrossRef]
- Milford, A.B.; Le Mouël, C.; Bodirsky, B.L.; Rolinski, S. Drivers of meat consumption. Appetite 2019, 141, 104313. [Google Scholar] [CrossRef]
- Rosegrant, M.W.; Agcaoili-Sombilla, M.C.; Perez, N.D. Global Food Projections to 2020: Implications for Investment; Diane Publishing: Collingdale, PA, USA, 1995; pp. 3–50. [Google Scholar]
- Farvid, M.S.; Sidahmed, E.; Spence, N.D.; Angua, K.M.; Rosner, B.A.; Barnett, J.B. Consumption of red meat and processed meat and cancer incidence: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 937–951. [Google Scholar] [CrossRef]
- Shi, W.; Huang, X.; Schooling, C.M.; Zhao, J.V. Red meat consumption, cardiovascular diseases, and diabetes: A systematic review and meta-analysis. Eur. Heart J. 2023, 44, 2626–2635. [Google Scholar] [CrossRef]
- McAfee, A.J.; McSorley, E.M.; Cuskelly, G.J.; Moss, B.W.; Wallace, J.M.; Bonham, M.P.; Fearon, A.M. Red meat consumption: An overview of the risks and benefits. Meat Sci. 2010, 84, 1–13. [Google Scholar] [CrossRef]
- Vahid, F.; Hoge, A.; Hebert, J.R.; Bohn, T. Association of diet quality indices with serum and metabolic biomarkers in participants of the oriscav-lux-2 study. Eur. J. Nutr. 2023, 62, 2063–2085. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Redondo-Flórez, L.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Global impacts of western diet and its effects on metabolism and health: A narrative review. Nutrients 2023, 15, 2749. [Google Scholar] [CrossRef]
- Beauchesne-Rondeau, E.; Gascon, A.; Bergeron, J.; Jacques, H. Plasma lipids and lipoproteins in hypercholesterolemic men fed a lipid-lowering diet containing lean beef, lean fish, or poultry. Am. J. Clin. Nutr. 2003, 77, 587–593. [Google Scholar] [CrossRef]
- García-Montero, C.; Fraile-Martínez, O.; Gómez-Lahoz, A.M.; Pekarek, L.; Castellanos, A.J.; Noguerales-Fraguas, F.; Coca, S.; Guijarro, L.G.; García-Honduvilla, N.; Asúnsolo, A. Nutritional components in western diet versus mediterranean diet at the gut microbiota–immune system interplay. Implications for health and disease. Nutrients 2021, 13, 699. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Wang, B.; Wen, L.; Wang, F.; Yu, H.; Chen, D.; Su, X.; Zhang, C. Effects of dietary fiber on human health. Food Sci. Hum. Wellness 2022, 11, 1–10. [Google Scholar] [CrossRef]
- Rumawas, M.E.; Dwyer, J.T.; McKeown, N.M.; Meigs, J.B.; Rogers, G.; Jacques, P.F. The development of the mediterranean-style dietary pattern score and its application to the american diet in the framingham offspring cohort. J. Nutr. 2009, 139, 1150–1156. [Google Scholar] [CrossRef]
- Guerriero, G.; Berni, R.; Muñoz-Sanchez, J.A.; Apone, F.; Abdel-Salam, E.M.; Qahtan, A.A.; Alatar, A.A.; Cantini, C.; Cai, G.; Hausman, J.F.; et al. Production of plant secondary metabolites: Examples, tips and suggestions for biotechnologists. Genes 2018, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.; Duthie, G. Plant secondary metabolites and gut health: The case for phenolic acids. Proc. Nutr. Soc. 2011, 70, 389–396. [Google Scholar] [CrossRef]
- Bohn, T.; Bonet, M.L.; Borel, P.; Keijer, J.; Landrier, J.-F.; Milisav, I.; Ribot, J.; Riso, P.; Winklhofer-Roob, B.; Sharoni, Y. Mechanistic aspects of carotenoid health benefits—Where are we now? Nutr. Res. Rev. 2021, 34, 276–302. [Google Scholar] [CrossRef]
- Wei, C.; Liu, L.; Liu, R.; Dai, W.; Cui, W.; Li, D. Association between the phytochemical index and overweight/obesity: A meta-analysis. Nutrients 2022, 14, 1429. [Google Scholar] [CrossRef]
- Moshfegh, A.; Goldman, J.; Cleveland, L. What we eat in america, nhanes 2001–2002: Usual nutrient intakes from food compared to dietary reference intakes. US Dep. Agric. Agric. Res. Serv. 2005, 1–56. [Google Scholar]
- Kant, A.K. Consumption of energy-dense, nutrient-poor foods by adult americans: Nutritional and health implications. The third national health and nutrition examination survey, 1988–1994. Am. J. Clin. Nutr. 2000, 72, 929–936. [Google Scholar] [CrossRef]
- Carrera-Bastos, P.; Fontes-Villalba, M.; O’Keefe, J.H.; Lindeberg, S.; Cordain, L. The western diet and lifestyle and diseases of civilization. Res. Rep. Clin. Cardiol. 2011, 2, 15–35. [Google Scholar] [CrossRef]
- Ames, B.N. Low micronutrient intake may accelerate the degenerative diseases of aging through allocation of scarce micronutrients by triage. Proc. Natl. Acad. Sci. USA 2006, 103, 17589–17594. [Google Scholar] [CrossRef]
- Alkerwi, A.; Sauvageot, N.; Nau, A.; Lair, M.-L.; Donneau, A.-F.; Albert, A.; Guillaume, M. Population compliance with national dietary recommendations and its determinants: Findings from the oriscav-lux study. Br. J. Nutr. 2012, 108, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: An updated systematic review and meta-analysis of cohort studies. J. Ac. Nutr. Diet. 2018, 118, 74–100.e11. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, M.; Vahid, F.; Devaux, Y.; Bohn, T. Biomarkers of food intake and their relevance to metabolic syndrome. Food Funct. 2024, 15, 7271–7304. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Provisional report of a who consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Balkau, B.; Charles, M.-A. Comment on the provisional report from the who consultation. Diabet. Med. 1999, 16, 1464–5491. [Google Scholar]
- National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (ncep) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel iii), Final Report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Bloomgarden, Z.T. American association of clinical endocrinologists (aace) consensus conference on the insulin resistance syndrome: 25–26 august 2002, washington, dc. Diabetes Care 2003, 26, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A consensus statement from the international diabetes federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Aspect | Inclusion | Exclusion |
|---|---|---|
| Study design | Original peer-reviewed research papers | Case reports, reviews, systematic reviews, meta-analyses, comments, congress reports, editorials, book chapters, retracted publication |
| MetS | Containing MetS and/or its components in the study | No MetS and/or its components |
| WD components | Containing at least one of the WD components | No food components |
| Evaluation | Link between WD components and MetS and/or its components. | Studies not containing at least a WD component and its effect on MetS and/or its components. |
| Population | All populations, all ages, infants (≤12 months), toddlers (>12–36 months), children (>36 months–10 years), adolescents (>10–18 years), adults (>18–65 years), elderly (>65–75 years), very elderly (>75 years) [30] | N/A |
| Region | The whole world | N/A |
| Time | 2001–Mar 2024 | N/A |
| Language | English (abstract and whole text) | Non-English (abstract and whole text) |
| Species | Human studies (both genders) | Animal studies, cellular models, and in vitro studies |
| Study Designs (StDs) | StDs Coding | StD Score | StD + T1 Score | StD + T2 Score | StD + T3 Score ^ | |
|---|---|---|---|---|---|---|
| Clinical trials | Randomized, blinded clinical trials | I | 10 | 11 | 12 | 13 |
| Randomized or blinded clinical trials | II | 9 | 10 | 11 | 12 | |
| Non-randomized and non-blinded clinical trials | III | 8 | 9 | 10 | 11 | |
| Cohort | IV | 7 | 8 | 9 | 10 | |
| Case-control | V | 6 | 7 | 8 | 9 | |
| Nested cross-sectional | VI | 5 | 6 | 7 | 8 | |
| Case-no case cross-sectional design | VII | 4 | 5 | 6 | 7 | |
| Descriptive designs | VIII | 3 | 4 | 5 | 6 | |
| Step | Explanation | Calculation Detail | Score | |
|---|---|---|---|---|
| 1 | Assigning the StD and tertile score to the cohort study ^ | StD score | 7 points | 7 + 3 = 10 points |
| Tertile score | 3 points | |||
| 2 | Increasing the effect of health outcomes in the final score (compared to the StD and tertile score) | StD and tertile score | 10 points | 10 × 3 = 30 points |
| Factoring fixed number * | 3 points | |||
| 3.1 | Allocating scores to MetS (if reported) | Half of the calculated score in Step 2 | 30 ÷ 2 = 15 points | |
| 3.2 | Allocating scores to each of the MetS components (if reported) | One-fifth of the calculated score from step 3.1 | 15 ÷ 5 = 3 points | |
| StD | Tertiles | MetS Positive ^ | FBG Negative * | DBP Non-Significant § |
|---|---|---|---|---|
| Cohort (7 points) | T1 (1 point) | (7 + 1) × 15 = 120 | −(7 + 1) × 3 = −24 | 24 ÷ 2 = 12 |
| Cohort (7 points) | T2 (2 points) | (7 + 2) × 15 = 135 | −(7 + 2) × 3 = −27 | 27 ÷ 2 = 13.5 |
| Cohort (7 points) | T3 (3 points) | (7 + 3) × 15 = 150 | −(7 + 3) × 3 = −30 | 30 ÷ 2 = 15 |
| Study Designs a | Tertiles b | MetS c Positive | MetS Inverse | MetS Non-Significant | BG d Positive | BG Inverse | BG Non-Significant | HDL e Positive | HDL Inverse | HDL Non-Significant | TG f Positive | TG Inverse | TG Non-Significant | WC g Positive | WC Inverse | WC Non-Significant | DBP h Positive | DBP Inverse | DBP Non-Significant | SBP i Positive | SBP Inverse | SBP Non-Significant |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | T1 | 1 j (214.5) k | - | - | - | 1 (−42.9) | 1 (42.9) | - | - | 2 (85.8) | 1 (42.9) | - | 1 (42.9) | - | - | 2 (85.8) | - | - | 1 (21.45) | - | - | 1 (21.45) |
| I | T2 | - | - | - | 1 (46.8) | - | 1 (46.8) | 1 (46.8) | - | 2 (93.6) | 2 (93.6) | 1 (−46.8) | - | - | - | 2 (93.6) | 1 (23.4) | 1 (23.4) | 1 (23.4) | - | 1 (23.4) | |
| I | T3 | 1 (253.5) | 1 (−254) | 2 (507) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| IV | T1 | - | - | 1 (120) | 1 (24) | - | 1 (24) | - | - | 3 (72) | 1 (24) | - | 2 (48) | - | - | 2 (48) | - | - | 2 (24) | - | - | 2 (24) |
| IV | T2 | 2 (270) | - | 5 (675) | 1 (27) | - | 3 (81) | - | - | 4 (108) | - | 1 (−27) | - | 2 (54) | - | 2 (54) | - | - | 3 (40.5) | - | - | 3 (40.5) |
| IV | T3 | 4 (600) | - | - | 2 (60) | 1 (−30) | 1 (30) | 2 (60) | 1 (−30) | 1 (30) | 2 (60) | - | 2 (60) | 2 (60) | 1 (−30) | 1 (30) | 1 (15) | - | 3 (45) | 1 (15) | - | 3 (45) |
| V | T1 | - | 2 (−41) | 8 (164) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| VI | T1 | 3 (216) | - | 37 (2664) | 1 (14.4) | 2 (−28.8) | 29 (417.6) | 1 (14.4) | - | 29 (417.6) | 5 (72) | 3 (−43.2) | 21 (302.4) | 10 (144) | 3 (−43.2) | 12 (172.8) | 5 (36) | 1 (−7.2) | 27 (194.4) | 3 (21.6) | - | 30 (216) |
| VI | T2 | 3 (252) | 2 (−168) | 6 (504) | - | 1 (−16.8) | 9 (151.2) | 1 (16.8) | - | 9 (151.2) | 1 (16.8) | 2 (−33.6) | 7 (117.6) | 4 (67.2) | - | 6 (100.8) | 1 (8.4) | 2 (−16.8) | 8 (67.2) | 1 (8.4) | 2 (−16.8) | 8 (67.2) |
| VI | T3 | 32 (3072) | 3 (−288) | 12 (1152) | 5 (96) | 2 (−38.4) | 5 (96) | 7 (134.4) | 2 (−38.4) | 5 (96) | 6 (115.2) | 4 (−76.8) | 4 (76.8) | 8 (153.6) | 1 (−19.2) | - | 7 (67.2) | 2 (−19.2) | 5 (48) | 7 (67.2) | 2 (−19.2) | 5 (48) |
| VII | T1 | - | - | - | 1 (10.5) | - | 2 (21) | - | 1 (−10.5) | 2 (21) | - | - | 3 (31.5) | 1 (10.5) | - | 2 (21) | 1 (5.25) | - | 2 (10.5) | 2 (10.5) | - | 1 (5.25) |
| VII | T3 | - | - | - | - | - | 1 (14.7) | - | - | 1 (14.7) | - | - | 1 (14.7) | - | - | 1 (14.7) | - | - | 1 (7.35) | - | 1 (7.35) | |
| VIII | T1 | 7 (252) | 1 (−36) | 1 (36) | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Total Sum | 5130 l | −935 m | 6414 n | 278.7 l | −156.9 m | 925.2 n | 272.4 l | −78.9 m | 1089.9 n | 424.5 l | −227.4 m | 693.9 n | 489.3 l | −92.4 m | 620.7 n | 155.3 l | −43.2 m | 481.8 n | 146.1 l | −36 m | 498.2 n | |
| Positive sum l | 6896.3 | |||||||||||||||||||||
| Inverse sum m | −1569.8 | |||||||||||||||||||||
| Positive and inverse sum (l+m) | 6896.3 + (−1569.8) = 5328 | |||||||||||||||||||||
| Non-significant sum n | 10,723.6 | |||||||||||||||||||||
| Absolute sum (positive sum (l) + |inverse sum| (m) + non-significant sum (n)) | 6896.3 + |−1569.3| + 10,723.7 = 19,189.3 | |||||||||||||||||||||
| Score (positive and inverse sum/absolute sum) | 5328 ÷ 19,189.2 = 0.2776 | |||||||||||||||||||||
| # | Foods ^ | Number of Articles | Positive Sum | Negative Sum | Non-Significant Sum | Total Weight | WDI Coefficient * |
|---|---|---|---|---|---|---|---|
| 1 | Calorie, energy | 9 | 93.5 | −452.7 | 954.2 | 1500.3 | −0.2395 |
| 2 | Fiber | 31 | 1911.9 | −138.9 | 2313.8 | 4364.6 | 0.4062 |
| 3 | Whole grains | 39 | 2549.7 | −1521 | 6142.5 | 10,213.2 | 0.1007 |
| 4 | Carbohydrates | 41 | 2037.2 | −1552.5 | 4698 | 8287.7 | 0.0584 |
| 5 | Refined grains | 33 | 735.9 | −2017.5 | 3660.8 | 6414.2 | −0.1998 |
| 6 | Legumes | 38 | 1515.3 | −375.6 | 4143.9 | 6034.8 | 0.1888 |
| 7 | Nuts and seeds | 44 | 3090.5 | −587.7 | 5759.9 | 9438 | 0.2652 |
| 8 | Oils | 25 | 1310.6 | −803.3 | 3567 | 5680.8 | 0.0893 |
| 9 | Hydrogenated fat | 16 | 388.8 | −1317.6 | 1690.8 | 3397.2 | −0.2734 |
| 10 | Soft drinks | 53 | 190.8 | −3769.2 | 5730.9 | 9690.9 | −0.3693 |
| 11 | Sodium | 29 | 520.8 | −1457.9 | 1386.6 | 3365.3 | −0.2784 |
| 12 | Coffee, tea, and water | 40 | 2522.6 | −1119 | 4801.1 | 8442.6 | 0.1662 |
| 13 | Protein | 37 | 1807.1 | −1216.7 | 4097.6 | 7121.3 | 0.0829 |
| 14 | Diet drinks | 8 | 96 | −280.8 | 999.6 | 1376.4 | −0.1343 |
| 15 | Alcohol | 21 | 453.6 | −1026 | 2058 | 3537.6 | −0.1618 |
| 16 | Supplements | 65 | 4563.3 | −968.6 | 10,671.2 | 16,203 | 0.2219 |
| 17 | Vitamins and minerals | 61 | 6896.3 | −1569.3 | 10,723.7 | 19,189.2 | 0.2776 |
| 18 | Secondary plant metabolites | 32 | 3938.4 | −766.8 | 4559.1 | 9264.3 | 0.34235 |
| 19 | Total fat | 42 | 1237.2 | −1590 | 4132.2 | 6959.4 | −0.0507 |
| 20 | Processed foods | 51 | 717 | −4829.4 | 7794.5 | 13340.9 | −0.3083 |
| 21 | Cholesterol, SFAs, and trans fat | 27 | 484.2 | −811.2 | 2965.5 | 4261 | −0.0767 |
| 22 | PUFA and MUFA | 47 | 3729.5 | −743.4 | 7943.1 | 12416 | 0.2405 |
| 23 | Sugar | 43 | 728.3 | −2044.5 | 4616.4 | 7389.2 | −0.1782 |
| 24 | Fruits | 67 | 3591.8 | −676.7 | 7435.8 | 11704.2 | 0.2491 |
| 25 | Vegetables | 53 | 4073.4 | −1009.7 | 7326.5 | 12409.5 | 0.2469 |
| 26 | Processed meat | 19 | 286.2 | −889.2 | 1287.9 | 2463.3 | −0.2448 |
| 27 | Red meat | 34 | 511.8 | −2338.2 | 3333.6 | 6183.6 | −0.2954 |
| 28 | White meat | 16 | 595.2 | −340.8 | 1046.7 | 1982.7 | 0.1283 |
| 29 | Fish | 33 | 1831.2 | −439.8 | 3300.5 | 5571.5 | 0.2497 |
| 30 | Dairy | 46 | 3609.5 | −1244.4 | 6510.2 | 11364 | 0.2081 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cifuentes, M.; Hejazi, Z.; Vahid, F.; Bohn, T. Designing and Developing a Population/Literature-Based Westernized Diet Index (WDI) and Its Relevance for Cardiometabolic Health. Nutrients 2025, 17, 2314. https://doi.org/10.3390/nu17142314
Cifuentes M, Hejazi Z, Vahid F, Bohn T. Designing and Developing a Population/Literature-Based Westernized Diet Index (WDI) and Its Relevance for Cardiometabolic Health. Nutrients. 2025; 17(14):2314. https://doi.org/10.3390/nu17142314
Chicago/Turabian StyleCifuentes, Miguel, Zahra Hejazi, Farhad Vahid, and Torsten Bohn. 2025. "Designing and Developing a Population/Literature-Based Westernized Diet Index (WDI) and Its Relevance for Cardiometabolic Health" Nutrients 17, no. 14: 2314. https://doi.org/10.3390/nu17142314
APA StyleCifuentes, M., Hejazi, Z., Vahid, F., & Bohn, T. (2025). Designing and Developing a Population/Literature-Based Westernized Diet Index (WDI) and Its Relevance for Cardiometabolic Health. Nutrients, 17(14), 2314. https://doi.org/10.3390/nu17142314