
Assessing Plant-Based Diets in Taiwan Using a Harmonized Food Description-Incorporated Framework

Abstract
1. Introduction
2. Materials and Methods
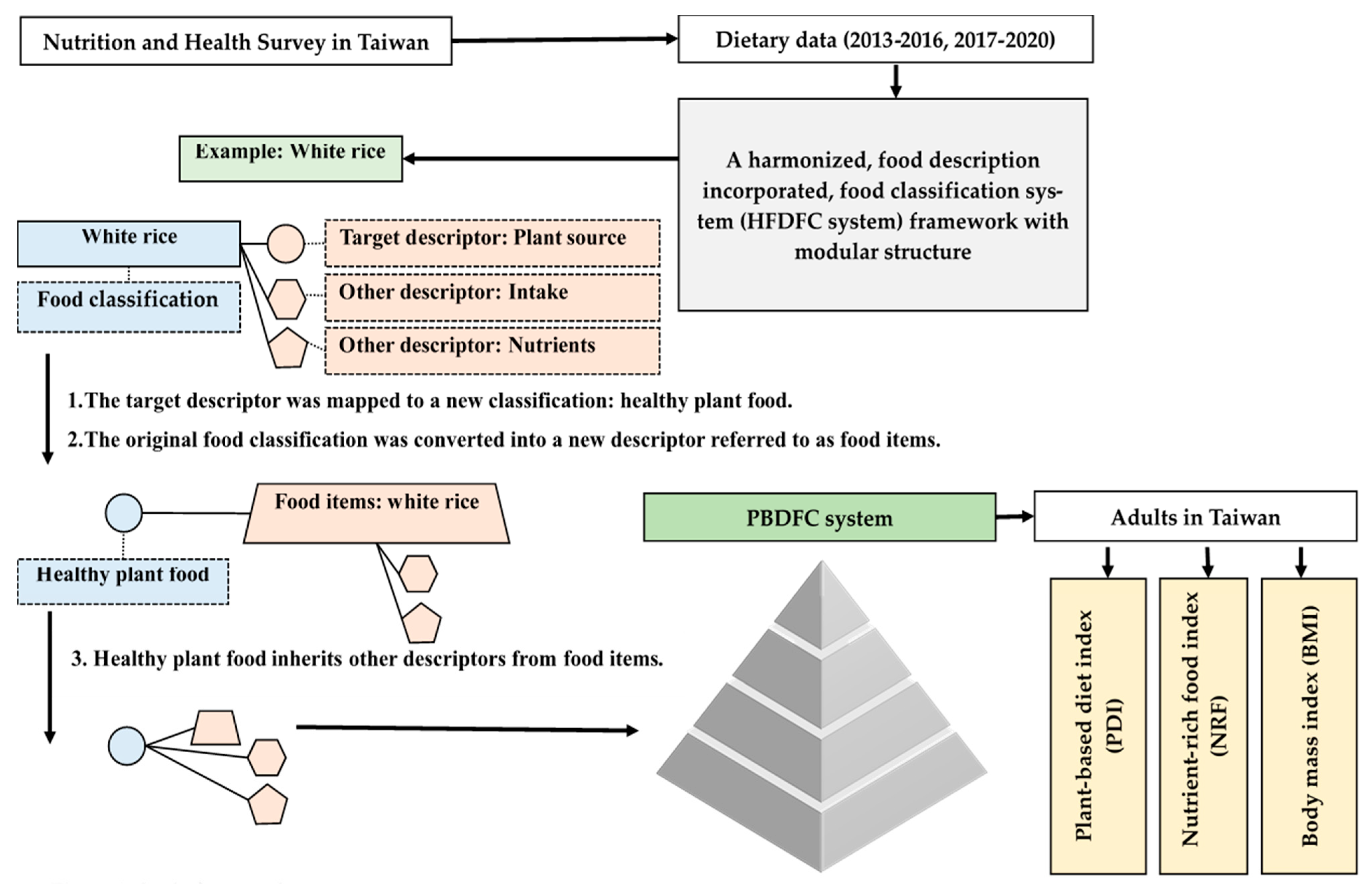
2.1. HFDFC System
2.2. Research Framework
2.3. Plant-Based Dietary Index
2.4. Nutrition-Rich Food Index
2.5. Statistical Analysis
3. Results
3.1. Food Classification Framework and Scoring Criteria for PDI and NRF132
3.2. Distribution of Plant-Based Diet Indices, Nutritional Quality, and BMI Across Age Groups
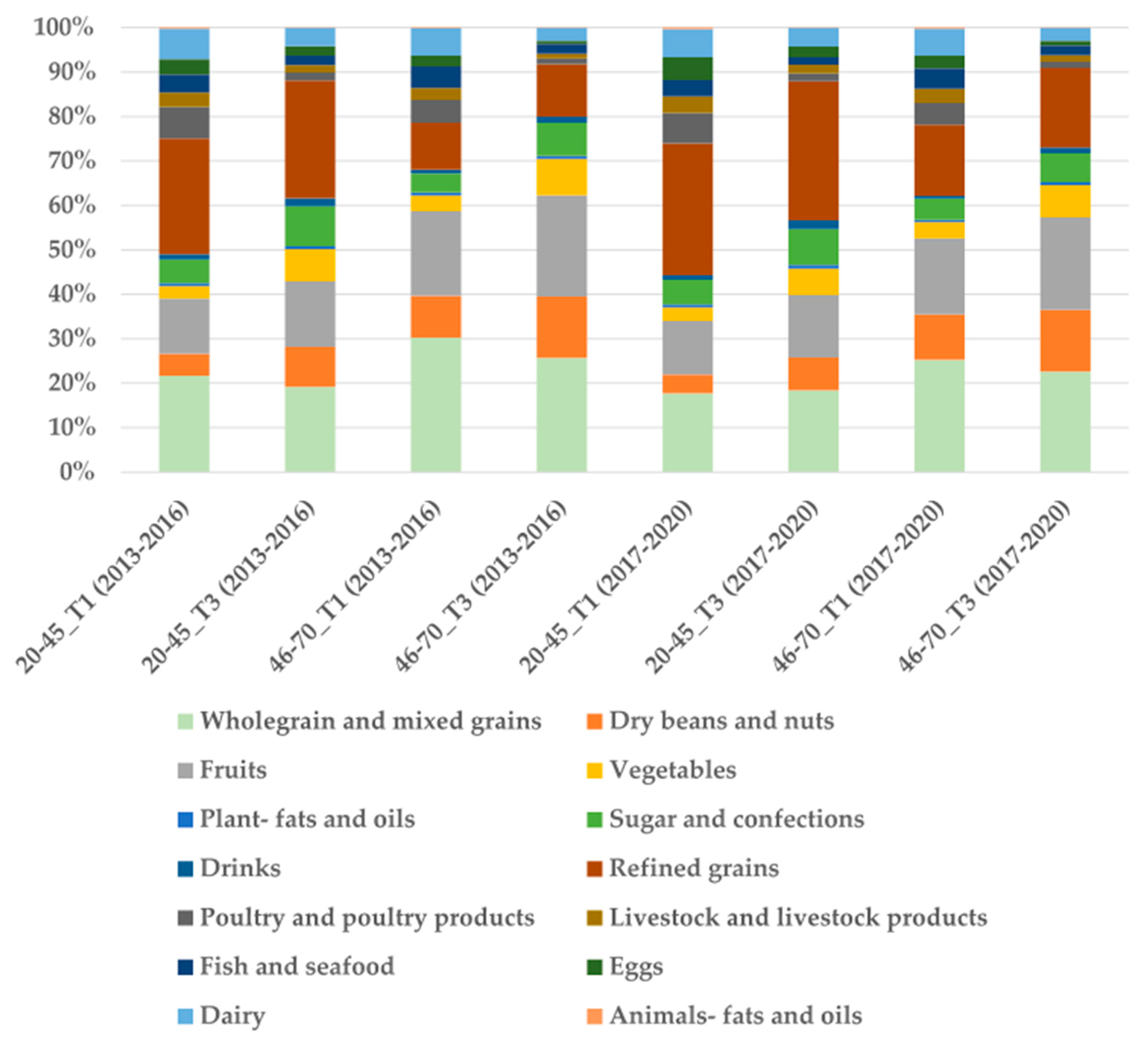
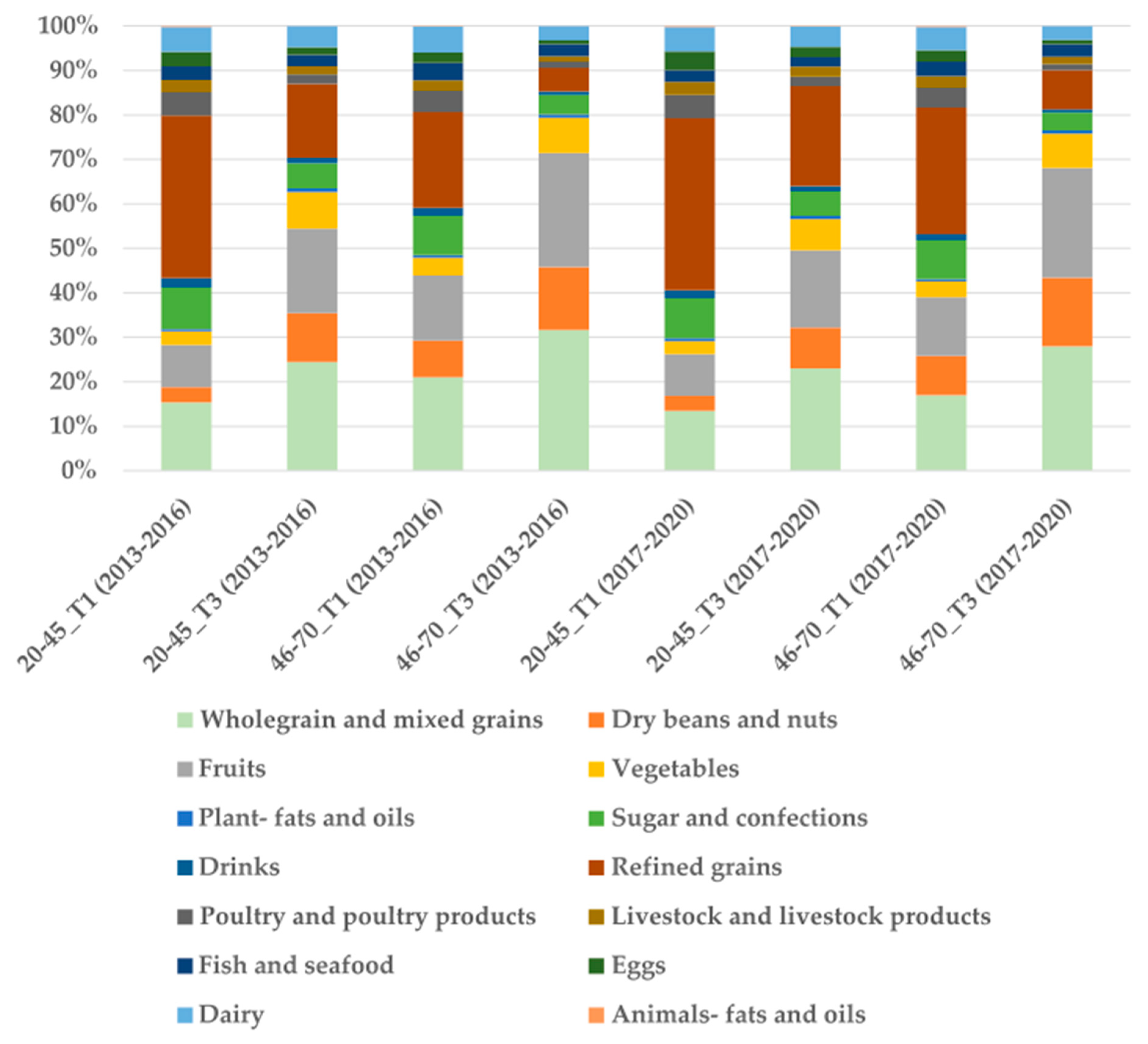
3.3. Changes in Food Intake Composition Across Plant-Based Diet Index Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sadler, C.R.; Grassby, T.; Hart, K.; Raats, M.; Sokolović, M.; Timotijevic, L. Processed food classification: Conceptualisation and challenges. Trends Food Sci. Technol. 2021, 112, 149–162. [Google Scholar]
- Crino, M.; Barakat, T.; Trevena, H.; Neal, B. Systematic Review and Comparison of Classification Frameworks Describing the Degree of Food Processing. Nutr. Food Technol. 2017, 3, 138. [Google Scholar]
- Monteiro, C.; Cannon, G.; Levy, R.B.; Claro, R.; Moubarac, J.-C.; Martins, A.P.; Louzada, M.L.; Baraldi, L.; Canella, D. The big issue for nutrition, disease, health, well-being. World Nutr. 2012, 3, 527–569. [Google Scholar]
- Moubarac, J.-C.; Parra, D.C.; Cannon, G.; Monteiro, C.A. Food Classification Systems Based on Food Processing: Significance and Implications for Policies and Actions: A Systematic Literature Review and Assessment. Curr. Obes. Rep. 2014, 3, 256–272. [Google Scholar]
- Durazzo, A.; Lucarini, M. Food Composition and Dedicated Databases: Key Tools for Human Health and Public Nutrition (2nd Edition). Nutrients 2025, 17, 1119. [Google Scholar] [CrossRef]
- Ireland, J.D.; Møller, A. Review of International Food Classification and Description. J. Food Compos. Anal. 2000, 13, 529–538. [Google Scholar]
- Karageorgou, D.; Castor, L.L.; de Quadros, V.P.; de Sousa, R.F.; Holmes, B.A.; Ioannidou, S.; Mozaffarian, D.; Micha, R. Harmonising dietary datasets for global surveillance: Methods and findings from the Global Dietary Database. Public Health Nutr. 2024, 27, e47. [Google Scholar] [PubMed]
- Ardizzone, M.; Binaglia, M.; Cottrill, B.; Cugier, J.; Ferreira, L.; Ruiz, J.Á.G.; Innocenti, M.; Ioannidou, S.; Puente, S.L.; Merten, C.; et al. Animal dietary exposure: Overview of current approaches used at EFSA. EFSA J. 2019, 17, e05896. [Google Scholar] [PubMed]
- Chiu, S.-Y.; Lin, H.-T.; Ho, W.-C.; Lin, M.-H.; Chen, P.-C.; Huang, H.-Y. Application of food description to the food classification system: Evidence of risk assessment from Taiwan as Acrylamide of grain products. J. Food Drug Anal. 2018, 26, 1312–1319. [Google Scholar]
- Auclair, O.; Burgos, S.A. Protein consumption in Canadian habitual diets: Usual intake, inadequacy, and the contribution of animal- and plant-based foods to nutrient intakes. Appl. Physiol. Nutr. Metab. 2021, 46, 501–510. [Google Scholar]
- Bassin, S.R.; De Carvalho, J.F.; Gulati, M. A Review of Plant-Based Diets for Obesity Management. Endocr. Pract. 2024, 30, 779–789. [Google Scholar] [PubMed]
- Carey, C.N.; Paquette, M.; Sahye-Pudaruth, S.; Dadvar, A.; Dinh, D.; Khodabandehlou, K.; Liang, F.; Mishra, E.; Sidhu, M.; Brown, R.; et al. The Environmental Sustainability of Plant-Based Dietary Patterns: A Scoping Review. J. Nutr. 2023, 153, 857–869. [Google Scholar]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B.; et al. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar]
- Acosta, P.F.C.; Landon, O.A.; Ribau, Z.J.; Haines, J.; Ma, D.W.L.; Duncan, A.M.; on behalf of the Guelph Family Health Study. Plant-Based Dietary Indices in Relation to Nutrient and Food Group Intakes in Preschool-Aged Children. Nutrients 2023, 15, 4617. [Google Scholar] [PubMed]
- Schorr, K.A.; Agayn, V.; de Groot, L.C.; Slagboom, P.E.; Beekman, M. A plant-based diet index to study the relation between diet and disease risk among adults: A narrative review. J. Nutr. Health Aging 2024, 28, 100272. [Google Scholar]
- Rosenfeld, R.M.; Juszczak, H.M.; Wong, M.A. Scoping review of the association of plant-based diet quality with health outcomes. Front. Nutr. 2023, 10, 1211535. [Google Scholar]
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar]
- Strid, A.; Johansson, I.; Bianchi, M.; Sonesson, U.; Hallström, E.; Lindahl, B.; Winkvist, A. Diets benefiting health and climate relate to longevity in northern Sweden. Am. J. Clin. Nutr. 2021, 114, 515–529. [Google Scholar]
- Van Kernebeek, H.; Oosting, S.; Feskens, E.; Gerber, P.; De Boer, I. The effect of nutritional quality on comparing environmental impacts of human diets. J. Clean. Prod. 2014, 73, 88–99. [Google Scholar]
- Chiu, S.-Y.; Lin, H.-T.; Lin, M.-H.; Ho, W.-C.; Chen, P.-C.; Huang, H.-Y. The Integration of Recipes with a Standardizable Food Description FACET for Cadmium Exposure Risk Assessment. Int. J. Environ. Res. Public Health 2019, 16, 4825. [Google Scholar]
- Wang, Y.B.; Page, A.J.; Gill, T.K.; Melaku, Y.A. The association between diet quality, plant-based diets, systemic inflammation, and mortality risk: Findings from NHANES. Eur. J. Nutr. 2023, 62, 2723–2737. [Google Scholar] [PubMed]
- Liang, F.; Fu, J.; Turner-McGrievy, G.; Wang, Y.; Qiu, N.; Ding, K.; Zeng, J.; Moore, J.B.; Li, R. Association of Body Mass Index and Plant-Based Diet with Cognitive Impairment among Older Chinese Adults: A Prospective, Nationwide Cohort Study. Nutrients 2022, 14, 3132. [Google Scholar] [CrossRef]
- Li, L.; Liu, C.; Xia, T.; Li, H.; Yang, J.; Pu, M.; Zhang, S.; Ma, Y.; Zhang, T.; Sung, W.-W. Association between plant-based dietary index and gallstone disease: A cross sectional study from NHANES. PLoS ONE 2024, 19, e0305822. [Google Scholar]
- Drewnowski, A. Defining nutrient density: Development and validation of the nutrient rich foods index. J. Am. Coll. Nutr. 2009, 28, 421S–426S. [Google Scholar]
- Health Promotion Administration. Dietary Reference Intakes in Taiwan-Version 8; Health Promotion Administration: Taipei, Taiwan, 2022. [Google Scholar]
- Wang, S.; Li, W.; Li, S.; Tu, H.; Jia, J.; Zhao, W.; Xu, A.; Xu, W.; Tsai, M.K.; Chu, D.T.-W.; et al. Association between plant-based dietary pattern and biological aging trajectory in a large prospective cohort. BMC Med. 2023, 21, 310. [Google Scholar]
- Zhou, L.; Zhang, R.; Yang, H.; Zhang, S.; Zhang, Y.; Li, H.; Chen, Y.; Maimaitiyiming, M.; Lin, J.; Ma, Y.; et al. Association of plant-based diets with total and cause-specific mortality across socioeconomic deprivation level: A large prospective cohort. Eur. J. Nutr. 2024, 63, 835–846. [Google Scholar] [PubMed]
- Peng, C.-J.; Liu, M.-Y.; Ho, C.-H. Anthropometric data analysis and norm establishment on 2013–2016 Nutrition and Health Survey in Taiwan-(I) height, weight and BMI. Nutr. Sci. J. 2023, 47, 109–124. [Google Scholar]
- Kent, G.; Kehoe, L.; Flynn, A.; Walton, J. Plant-based diets: A review of the definitions and nutritional role in the adult diet. Proc. Nutr. Soc. 2022, 81, 62–74. [Google Scholar]
- Satija, A.; Malik, V.; Rimm, E.B.; Sacks, F.; Willett, W.; Hu, F.B. Changes in intake of plant-based diets and weight change: Results from 3 prospective cohort studies. Am. J. Clin. Nutr. 2019, 110, 574–582. [Google Scholar]
- Zamani, B.; Daneshzad, E.; Siassi, F.; Guilani, B.; Bellissimo, N.; Azadbakht, L. Association of plant-based dietary patterns with psychological profile and obesity in Iranian women. Clin. Nutr. 2020, 39, 1799–1808. [Google Scholar]
- EFSA. The Food Classification and Description System FoodEx 2 (Revision 2); EFSA Supporting Publications: Parma, Italy, 2015; Volume 12, p. 804E. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HFDFC Classification | PBDFC Classification | OPDI | HPDI | LhPDI | RDA of NRF132 | Note | ||
|---|---|---|---|---|---|---|---|---|
| Nutrients | Male | Female | ||||||
| Wholegrain and mixed grains | Healthy plant foods | + | + | − | Fiber | 24 g | 20 g | Encourage nutrients |
| Dry beans and nuts | + | + | − | Protein | 70 g | 60 g | ||
| Fruits | + | + | − | Vitiman A | 600 µg | 500 µg | ||
| Vegetables | + | + | − | Vitiman C | 100 mg | 100 mg | ||
| Plant-fats and oils | + | + | − | Vitiman E | 12 mg | 12 mg | ||
| Sugar and confections | Less healthy foods | + | − | + | Ca | 1000 mg | 1000 mg | |
| Drinks | + | − | + | Iron | 15 mg | 10 mg | ||
| Refined grains; | + | − | + | Potassium | 2800 mg | 2500 mg | ||
| Poultry and poultry products | Animal foods | − | − | − | Magnesium | 360 mg | 310 mg | |
| Livestock and livestock products | − | − | − | Zinc | 15 mg | 12 mg | ||
| Fish and seafood | − | − | − | B1 | 1.2 mg | 0.9 mg | ||
| Eggs | − | − | − | B2 | 1.3 mg | 1.0 mg | ||
| Dairy | − | − | − | B12 | 2.4 µg | 2.4 µg | ||
| Animals-fats and oils | − | − | − | Saturated fat | 2300 mg | 1800 mg | Limit nutrients | |
| Na | 2300 mg | 2300 mg | ||||||
| Survey Period | Age Groups | N | OPDI | HPDI | LhPDI | BMI | Nrf_Ec132 |
|---|---|---|---|---|---|---|---|
| Mean (SD) | Median | ||||||
| 2013–2016 | 20–45 | 1865 | 43.48 (5.84) | 42.5 (6.33) | 45.07 (7.49) | 22.06 (3.85) | 20.78 |
| 46–70 | 2577 | 45.1 (5.61) | 47.92 (6.37) | 43.49 (6.91) | 24.8 (2.75) | 24.39 | |
| 2017–2020 | 20–45 | 1897 | 42.77 (5.64) | 41.51 (6.11) | 45.18 (7.01) | 22.91 (4.58) | 18.62 |
| 46–70 | 3107 | 44.83 (5.74) | 46.85 (6.39) | 43.11 (6.74) | 24.98 (3.29) | 24.63 | |
| 2013–2016 | 2017–2020 | ||||||
|---|---|---|---|---|---|---|---|
| Age: 20–45 | Variables | T1 (n = 582) | T3 (n = 911) | p Value | T1 (n = 555) | T3 (n = 853) | p Value |
| O-PDI | BMI | 21.79 | 22.22 | 0.0301 * | 22.76 | 23.10 | 0.1827 |
| Nrf_Ec132 | 17.35 | 24.61 | <0.0001 + | 13.59 | 22.44 | <0.0001 + | |
| H-PDI | BMI | 22.21 | 21.89 | 0.1273 | 23.17 | 22.77 | 0.1188 |
| Nrf_Ec132 | 18.16 | 22.96 | 0.0036 + | 13.98 | 21.77 | <0.0001 + | |
| Lh-PDI | BMI | 22.22 | 21.95 | 0.1887 | 23.31 | 22.39 | 0.0002 * |
| Nrf_Ec132 | 25.17 | 15.03 | <0.0001 + | 24.88 | 12.31 | <0.0001 + | |
| Age: 46–70 | Variables | T1 (n = 870) | T3 (n = 1052) | p value | T1 (n = 894) | T3 (n = 1393) | p value |
| O-PDI | BMI | 24.96 | 24.55 | 0.0010 * | 25.07 | 24.87 | 0.1771 |
| Nrf_Ec132 | 20.55 | 26.71 | <0.0001 + | 18.65 | 29.51 | <0.0001 + | |
| H-PDI | BMI | 25.06 | 24.64 | 0.0021 * | 25.18 | 24.82 | 0.0147 * |
| Nrf_Ec132 | 22.02 | 26.16 | 0.0558 + | 21.21 | 26.98 | 0.0002 + | |
| Lh-PDI | BMI | 24.91 | 24.68 | 0.0787 | 24.82 | 25.11 | 0.0403 * |
| Nrf_Ec132 | 29.06 | 17.02 | <0.0001 + | 30.09 | 17.63 | <0.0001 + | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Y.-S.; Lin, M.-H.; Chen, F.-J.; Chiu, S.-Y. Assessing Plant-Based Diets in Taiwan Using a Harmonized Food Description-Incorporated Framework. Nutrients 2025, 17, 2268. https://doi.org/10.3390/nu17142268
Wei Y-S, Lin M-H, Chen F-J, Chiu S-Y. Assessing Plant-Based Diets in Taiwan Using a Harmonized Food Description-Incorporated Framework. Nutrients. 2025; 17(14):2268. https://doi.org/10.3390/nu17142268
Chicago/Turabian StyleWei, Yu-Syuan, Ming-Hua Lin, Fu-Jun Chen, and She-Yu Chiu. 2025. "Assessing Plant-Based Diets in Taiwan Using a Harmonized Food Description-Incorporated Framework" Nutrients 17, no. 14: 2268. https://doi.org/10.3390/nu17142268
APA StyleWei, Y.-S., Lin, M.-H., Chen, F.-J., & Chiu, S.-Y. (2025). Assessing Plant-Based Diets in Taiwan Using a Harmonized Food Description-Incorporated Framework. Nutrients, 17(14), 2268. https://doi.org/10.3390/nu17142268