
Exploring the Dietary Patterns and Health Behaviours of Centenarians in Ourense (Spain): Adherence to the Southern European Atlantic Diet

 ,
,  ,
,  ,
,  ,
,  and
and 
Highlights
- Centenarians from Ourense follow a seasonal, homegrown diet rooted in the Southern European Atlantic Diet.
- Strong social ties and active rural routines support healthy and prolonged longevity.
- Industriousness is a central trait that promotes related factors like physical activity, sleep regulation and self-sufficient food production.
- Longevity arises from interactions between nutrition, lifestyle and personality traits.
- Self-sufficiency and food-sharing culture contribute to a balanced and sustainable diet.
Abstract

1. Introduction
2. Materials and Methods
2.1. Design, Participants and Selection Criteria
- Inclusion Criteria: Individuals aged 100 years or older having lived most of their life (more than 50%) in the province of Ourense. In cases of cognitive decline, individuals with a suitable informant available for an interview; a suitable informant is defined as a family member or caregiver (formal or informal) who knows the participant’s life history in detail.
- Exclusion Criteria: Refusal to participate in the questionnaire.
2.2. Variables and Instruments
- Longevity calculations (for the province and each municipality): To minimise the impact of major demographic phenomena such as declining birth rates and migration, two indices have been used: (A) the Centenarian Index (CI), defined as the ratio of centenarians to individuals over 90 years old; and (B) the Longevity Index (LI), defined as the proportion of individuals over 90 years old relative to those over 65. These data were calculated based on figures from the Galician Institute of Statistics (Instituto Galego de Estatística, IGE).
- Socio-demographic variables: Age, sex, residence, marital status, number of children, level of education, and type of housing.
- Environmental variables: altitude: Classified as low (0–300 m), medium (300–600 m), or high (>600 m), annual average temperature and precipitation; UNESCO heritage area status: Protected or non-protected (data obtained from the National Geographic Institute and the Ministry for Ecological Transition); exposure to radon in the primary residence, defined as the place where the individual has lived the longest, and classified into Zones I, II, and III (based on information from the Ministry of Health); thermal soil presence in the area; and exposure to thermal waters in the primary residence.
- Longevity-related dimensions: Body Mass Index (BMI); family history; diet (questions adapted from the Food Quality Survey of the Elderly and the Survey on Dietary Habits of the Adult Galician Population, 2007); current health status (self-reported health and number of medications taken); sleep quality (questions adapted from the Pittsburgh Sleep Quality Index and the Oviedo Sleep Questionnaire); physical activity (based on the Global Physical Activity Questionnaire-GPAQ); intellectual activity; perceived stress (adapted questions from the Spanish version of the Perceived Stress Scale (PSS) [42]; occupational/employment dimension; perceived social support (questions adapted from the MOS Social Support Survey and the Duke-UNC Functional Social Support Questionnaire); Resilience (questions adapted from the Connor-Davidson Resilience Scale); personality traits (questions adapted from the NEO-PI-R test); spirituality (questions adapted from the Meaning in Life Scale; marital satisfaction (question taken from the Relationship Assessment Scale (RAS) by Hendrick [43]; life satisfaction (questions adapted from the Satisfaction with Life Scale—SWLS); self-perception of longevity (ad hoc questions to explore individuals’ attributions regarding their own longevity).
2.3. Procedure
- The heads of each public Primary Care service in the province of Ourense and/or their nursing coordinators were contacted. The study was presented to them, and they were invited to participate as collaborating researchers. These individuals then contacted the General Practitioners and nurses within their respective services, who, being familiar with the patients under their care, initially informed the centenarians about the project. If a centenarian expressed interest in taking part, the General Practitioner or nurse provided them with the contact details of the principal research team or, if preferred, offered to have the principal research team initiate contact. For institutionalised centenarians, the same procedure was followed through the Primary Care General Practitioner and/or nurse, or through the medical or nursing staff of the institution, if they were the designated professionals. These professionals contacted the centenarian and/or a family member and followed the same protocol.
- A member of the research team either received a phone call from the participant/family member or made the call (in cases where this was the preferred method) to explain the objective of the study, its methodology, and what participation would entail.
- For those who ultimately agreed to participate, an appointment was scheduled. The meeting location was either the health centre, a community facility, or the participant’s home. One of the interviewers, a member of the research team, provided detailed in-person information and handed the participant the study information sheet (Section S2) and the informed consent form (Section S3); if the participant agreed, the interview was conducted. Each interview lasted approximately 60 min.
- If the participant did not meet the required cognitive conditions, the procedure was discussed with their legal representative, who could either act as the informant or designate another person for that role.
- Data collection was carried out using a questionnaire (Section S4), which consisted of a semi-structured interview combining open-ended, closed, and mixed-format questions. Each item began with an open question to allow the participant to share their perspective, followed by a set of predefined response options. This questionnaire was developed ad hoc, adapting items from validated instruments used to explore the various dimensions of interest (Section S1), and based on tools found in the relevant literature, such as the Chinese Longitudinal Healthy Longevity Survey Biomarkers Cohort (HLSBC) [44] and the Newcastle 85+ Study [45], adapted to our cultural context.
2.4. Data Analysis
- Quantitative Analysis: Quantitative variables were expressed as a mean and standard deviation when they followed a normal distribution, or as a median and interquartile range if they were non-Gaussian. Normality tests included the Kolmogorov–Smirnov and Shapiro–Wilk tests. A descriptive statistical analysis of the variables was carried out. Multivariate analysis and logistic regression were also conducted to identify which variables acted as independent factors associated with healthy longevity.
- Qualitative Analysis: A thematic qualitative analysis was carried out using a mixed categorisation approach (both pre-established and inductive), with the aim of identifying emerging factors not previously reported in the available literature, which might arise from the accounts of centenarians or their informants.
2.5. Ethical Considerations
3. Results and Discussion
3.1. Location of the Study Sample
3.2. Sociodemographic, Clinical, and Functional Characteristics of the Sample
3.3. Nutrition: Dietary Analysis
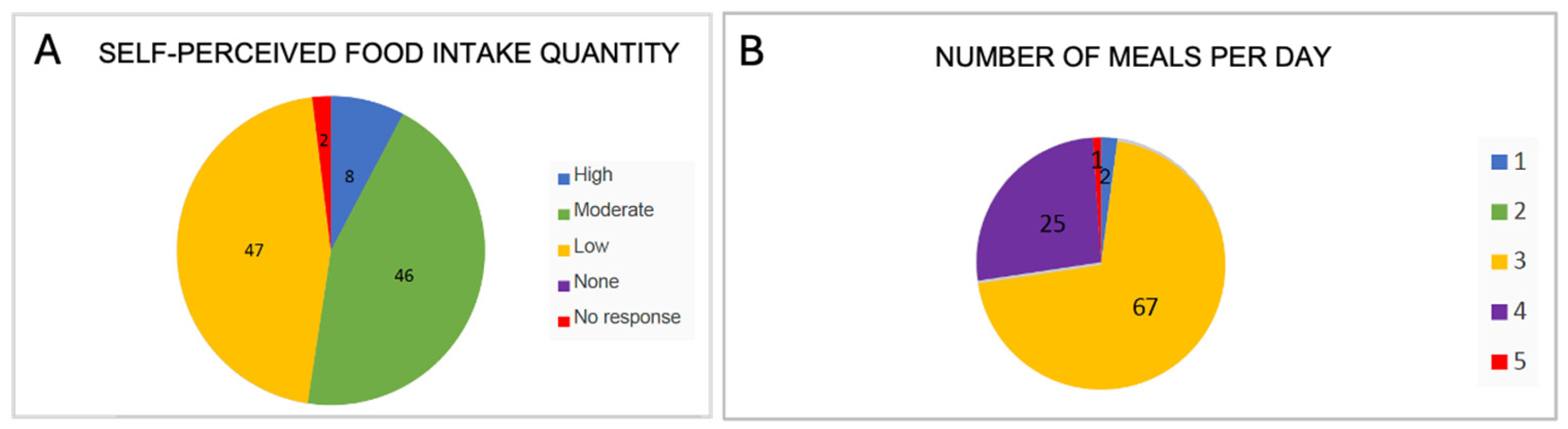
3.3.1. Amount of Food Consumed per Day and Number of Meals per Day
3.3.2. Consumption of Greens, Vegetables, Legumes Fruits
3.3.3. Meat and Fish Consumption
3.3.4. Consumption of Sweets, Bread, and Potatoes
3.3.5. Consumption of Salt, Milk, Cheese, and Cottage Cheese
3.3.6. Consumption of Wine and Distilled Beverages
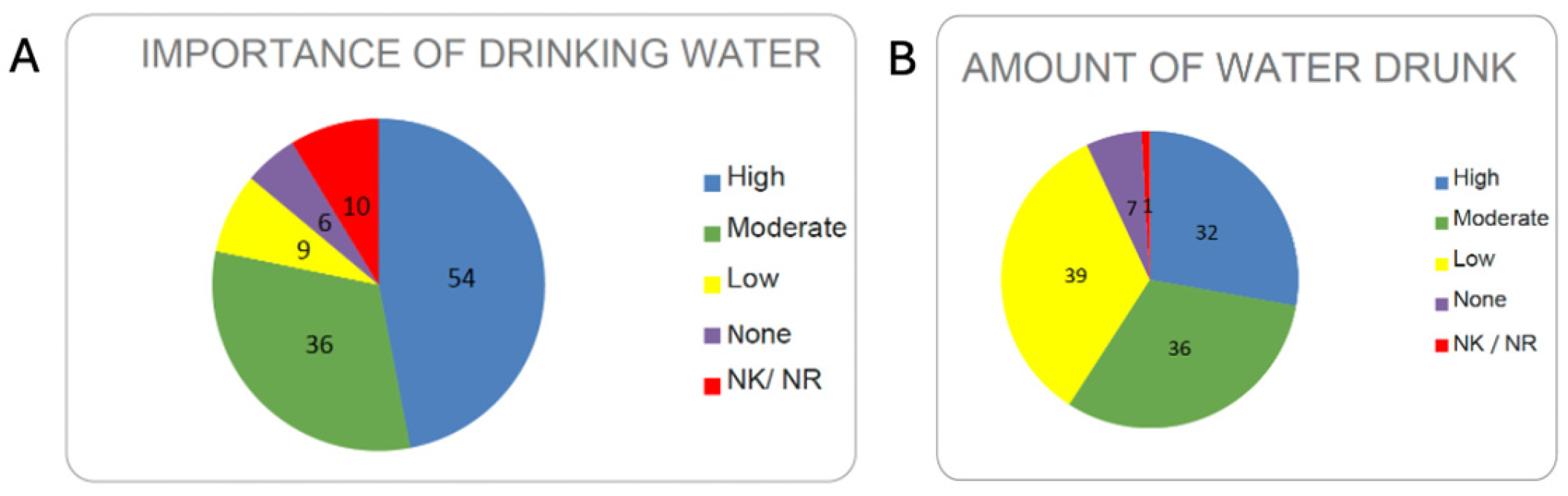
3.3.7. Importance of Drinking Water
3.4. Assessment of Longevity Determinants Beyond Nutritional Aspects [47]
3.5. Relationship Between Each Variable and Cognitive Impairment
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CI | Centenarian Index |
| CVD | Cardiovascular Disease |
| DASH | Dietary Approaches to Stop Hypertension |
| LI | Longevity Index |
| M/F | Male/Female |
| NECS | New England Centenarian Study |
| PSS | Perceived Stress Scale |
| PUFA | Polyunsaturated Fatty Acids |
| RAS | Relationship Assessment Scale |
| SEAD | Southern European Atlantic Diet |
| SPSS | Statistical Package for Social Sciences |
| SWLS | Satisfaction with Life Scale |
| UPF | Ultra-Processed Food |
| GPAQ | Global Physical Activity Questionnaire |
References
- Dakic, T.; Jevdjovic, T.; Vujovic, P.; Mladenovic, A. The Less We Eat, the Longer We Live: Can Caloric Restriction Help Us Become Centenarians? Int. J. Mol. Sci. 2022, 23, 6546. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, P.; Perls, T.T. The Genetics of Extreme Longevity: Lessons from the New England Centenarian Study. Front. Genet. 2012, 3, 277. [Google Scholar] [CrossRef] [PubMed]
- Boccardi, M.; Boccardi, V. Psychological Wellbeing and Healthy Aging: Focus on Telomeres. Geriatrics 2019, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Ljungquist, B.; Berg, S.; Lanke, J.; McClearn, G.E.; Pedersen, N.L. The Effect of Genetic Factors for Longevity: A Comparison of Identical and Fraternal Twins in the Swedish Twin Registry. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53A, M441–M446. [Google Scholar] [CrossRef]
- Royston, K.J.; Tollefsbol, T.O. The Epigenetic Impact of Cruciferous Vegetables on Cancer Prevention. Curr. Pharmacol. Rep. 2015, 1, 46–51. [Google Scholar] [CrossRef]
- Brooks-Wilson, A.R. Genetics of Healthy Aging and Longevity. Hum. Genet. 2013, 132, 1323–1338. [Google Scholar] [CrossRef]
- Komaki, S.; Nagata, M.; Arai, E.; Otomo, R.; Ono, K.; Abe, Y.; Ohmomo, H.; Umekage, S.; Shinozaki, N.O.; Hachiya, T.; et al. Epigenetic Profile of Japanese Supercentenarians: A Cross-Sectional Study. Lancet Healthy Longev. 2023, 4, e83–e90. [Google Scholar] [CrossRef]
- Coppedè, F.; Franzago, M.; Giardina, E.; Nigro, C.L.; Matullo, G.; Moltrasio, C.; Nacmias, B.; Pileggi, S.; Sirchia, S.M.; Stoccoro, A.; et al. A Perspective on Diet, Epigenetics and Complex Diseases: Where Is the Field Headed Next? Epigenomics 2022, 14, 1281–1304. [Google Scholar] [CrossRef]
- Morris, B.J.; Willcox, B.J.; Donlon, T.A. Genetic and Epigenetic Regulation of Human Aging and Longevity. Biochim. Biophys. Acta BBA—Mol. Basis Dis. 2019, 1865, 1718–1744. [Google Scholar] [CrossRef]
- Yu, Z.; Zhang, F.; Xu, C.; Wang, Y. Association between Circulating Antioxidants and Longevity: Insight from Mendelian Randomization Study. BioMed Res. Int. 2022, 2022, 4012603. [Google Scholar] [CrossRef]
- Elkashty, O.A.; Tran, S.D. Sulforaphane as a Promising Natural Molecule for Cancer Prevention and Treatment. Curr. Med. Sci. 2021, 41, 250–269. [Google Scholar] [CrossRef] [PubMed]
- Bernkopf, D.B.; Daum, G.; Brückner, M.; Behrens, J. Sulforaphane Inhibits Growth and Blocks Wnt/β-Catenin Signaling of Colorectal Cancer Cells. Oncotarget 2018, 9, 33982–33994. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; He, F.; Wu, C.; Li, P.; Li, N.; Deng, J.; Zhu, G.; Ren, W.; Peng, Y. Betaine in Inflammation: Mechanistic Aspects and Applications. Front. Immunol. 2018, 9, 1070. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, A.P.; Levchenko, A. Epigenetics as a Mediator of Plasticity in Cancer. Science 2023, 379, eaaw3835. [Google Scholar] [CrossRef]
- El-Seweidy, M.M.; Ali, S.I.; Elsweify, S.E.; Ali, A.A.; Mashhour, M.M. Omega3 Fatty Acids Intake Versus Diclofenac in Osteoarthritis Induced in Experimental Rats. Funct. Foods Health Dis. 2017, 7, 291. [Google Scholar] [CrossRef]
- Bowen, K.J.; Harris, W.S.; Kris-Etherton, P.M. Omega-3 Fatty Acids and Cardiovascular Disease: Are There Benefits? Curr. Treat. Options Cardiovasc. Med. 2016, 18, 69. [Google Scholar] [CrossRef]
- Biagi, E.; Franceschi, C.; Rampelli, S.; Severgnini, M.; Ostan, R.; Turroni, S.; Consolandi, C.; Quercia, S.; Scurti, M.; Monti, D.; et al. Gut Microbiota and Extreme Longevity. Curr. Biol. 2016, 26, 1480–1485. [Google Scholar] [CrossRef]
- Tafaro, L.; Cicconetti, P.; Baratta, A.; Brukner, N.; Ettorre, E.; Marigliano, V.; Cacciafesta, M. Sleep Quality of Centenarians: Cognitive and Survival Implications. Arch. Gerontol. Geriatr. 2007, 44, 385–389. [Google Scholar] [CrossRef]
- Aiello, A.; Accardi, G.; Ali, S.; Caruso, C.; Chen, M.; Vivo, I.; Ligotti, M.; Scapagnini, G.; Davinelli, S.; Candore, G. Possible Association of Telomere Length with Sleep Duration. A Preliminary Pilot Study in a Sicilian Cohort with Centenarians. Transl. Med. UniSa 2021, 24, 24–29. [Google Scholar] [CrossRef]
- Demakakos, P.; Nazroo, J.; Breeze, E.; Marmot, M. Socioeconomic Status and Health: The Role of Subjective Social Status. Soc. Sci. Med. 2008, 67, 330–340. [Google Scholar] [CrossRef]
- Packard, C.J.; Bezlyak, V.; McLean, J.S.; Batty, G.D.; Ford, I.; Burns, H.; Cavanagh, J.; Deans, K.A.; Henderson, M.; McGinty, A.; et al. Early Life Socioeconomic Adversity Is Associated in Adult Life with Chronic Inflammation, Carotid Atherosclerosis, Poorer Lung Function and Decreased Cognitive Performance: A Cross-Sectional, Population-Based Study. BMC Public Health 2011, 11, 42. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, Z.; Jagger, C.; Chiu, C.-T.; Ofstedal, M.B.; Rojo, F.; Saito, Y. Spirituality, Religiosity, Aging and Health in Global Perspective: A Review. SSM—Popul. Health 2016, 2, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Tafaro, L.; Tombolillo, M.T.; Brükner, N.; Troisi, G.; Cicconetti, P.; Motta, M.; Cardillo, E.; Bennati, E.; Marigliano, V. Stress in Centenarians. Arch. Gerontol. Geriatr. 2009, 48, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.M.; De Caro, F.; Funk, R.H.W.; Schiavo, L.; Gonnella, J.; Boccia, G.; Capunzo, M. Extreme Longevity: Analysis of the Direct or Indirect Influence of Environmental Factors on Old, Nonagenarians, and Centenarians in Cilento, Italy. Int. J. Environ. Res. Public. Health 2022, 19, 1589. [Google Scholar] [CrossRef]
- Buettner, D.; Skemp, S. Blue Zones: Lessons from the World’s Longest Lived. Am. J. Lifestyle Med. 2016, 10, 318–321. [Google Scholar] [CrossRef]
- Willcox, B.J.; Willcox, D.C.; Todoriki, H.; Fujiyoshi, A.; Yano, K.; He, Q.; Curb, J.D.; Suzuki, M. Caloric Restriction, the Traditional Okinawan Diet, and Healthy Aging. Ann. N. Y. Acad. Sci. 2007, 1114, 434–455. [Google Scholar] [CrossRef]
- Garagnani, P.; Bacalini, M.G.; Pirazzini, C.; Gori, D.; Giuliani, C.; Mari, D.; Di Blasio, A.M.; Gentilini, D.; Vitale, G.; Collino, S.; et al. Methylation of ELOVL2 Gene as a New Epigenetic Marker of Age. Aging Cell 2012, 11, 1132–1134. [Google Scholar] [CrossRef]
- Ministerio de Agricultura, Pesca y Alimentación Informe Del Consumo Alimentario en España 2022. Available online: https://www.mapa.gob.es/eu/alimentacion/temas/consumo-tendencias/informe-consumo-2022-baja-res_tcm35-655390.pdf (accessed on 26 June 2025).
- Mendoza, K.; Smith-Warner, S.A.; Rossato, S.L.; Khandpur, N.; Manson, J.E.; Qi, L.; Rimm, E.B.; Mukamal, K.J.; Willett, W.C.; Wang, M.; et al. Ultra-Processed Foods and Cardiovascular Disease: Analysis of Three Large US Prospective Cohorts and a Systematic Review and Meta-Analysis of Prospective Cohort Studies. Lancet Reg. Health—Am. 2024, 37, 100859. [Google Scholar] [CrossRef]
- Kliemann, N.; Al Nahas, A.; Vamos, E.P.; Touvier, M.; Kesse-Guyot, E.; Gunter, M.J.; Millett, C.; Huybrechts, I. Ultra-Processed Foods and Cancer Risk: From Global Food Systems to Individual Exposures and Mechanisms. Br. J. Cancer 2022, 127, 14–20. [Google Scholar] [CrossRef]
- Vivanco, P.G.; Taboada, P.; Coelho, A. The Southern European Atlantic Diet and Its Supplements: The Chemical Bases of Its Anticancer Properties. Nutrients 2023, 15, 4274. [Google Scholar] [CrossRef]
- Instituto Universitario de Ciencias de la Salud. Universidad de A Coruña Encuesta Sobre Los Hábitos Alimentarios de La Población Adulta Gallega. Available online: https://www.sergas.es/cas/Publicaciones/Docs/SaludPublica/PDF-2153-es.pdf (accessed on 26 June 2025).
- Pes, G.M.; Tolu, F.; Dore, M.P.; Sechi, G.P.; Errigo, A.; Canelada, A.; Poulain, M. Male Longevity in Sardinia, a Review of Historical Sources Supporting a Causal Link with Dietary Factors. Eur. J. Clin. Nutr. 2015, 69, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillón, P.; Oliveira, A.; Lopes, C.; López-García, E.; Rodríguez-Artalejo, F. The Southern European Atlantic Diet Is Associated with Lower Concentrations of Markers of Coronary Risk. Atherosclerosis 2013, 226, 502–509. [Google Scholar] [CrossRef] [PubMed]
- GALIAT Galicia Alimentación Atlántica DIETA ATLÁNTICA GALLEGA Productos Autóctonos Beneficiosos Para La Salud. Available online: https://galiat6mas7.com/es/categorias.php?var1=Proyecto&nar1=820&var2=Introducci%F3n&nar2=820&vez=1&metatitle= (accessed on 26 June 2025).
- Calvo-Malvar, M.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Leis, R.; Gude, F. Effects of a Community-Based Behavioral Intervention with a Traditional Atlantic Diet on Cardiometabolic Risk Markers: A Cluster Randomized Controlled Trial (“The GALIAT Study”). Nutrients 2021, 13, 1211. [Google Scholar] [CrossRef]
- Carballo-Casla, A.; Ortolá, R.; García-Esquinas, E.; Oliveira, A.; Sotos-Prieto, M.; Lopes, C.; Lopez-Garcia, E.; Rodríguez-Artalejo, F. The Southern European Atlantic Diet and All-Cause Mortality in Older Adults. BMC Med. 2021, 19, 36. [Google Scholar] [CrossRef]
- Govindaraju, D.; Atzmon, G.; Barzilai, N. Genetics, Lifestyle and Longevity: Lessons from Centenarians. Appl. Transl. Genomics 2015, 4, 23–32. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística Número de Personas Centenarias En Ourense y Lugo.Ministerio de Economía y Hacienda. 2022. Available online: https://www.ine.es/jaxi/Datos.htm?path=/t20/e245/p04/provi/l0/&file=0ccaa003.px# (accessed on 26 June 2025).
- Pfeiffer, E. A Short Portable Mental Status Questionnaire for the Assessment of Organic Brain Deficit in Elderly Patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Harris, K.M.; Gaffey, A.E.; Schwartz, J.E.; Krantz, D.S.; Burg, M.M. The Perceived Stress Scale as a Measure of Stress: Decomposing Score Variance in Longitudinal Behavioral Medicine Studies. Ann. Behav. Med. 2023, 57, 846–854. [Google Scholar] [CrossRef]
- Hendrick, S.S. A generic measure of relationship satisfaction. J. Marriage Fam. 1988, 50, 93–98. [Google Scholar] [CrossRef]
- Lv, Y.; Mao, C.; Yin, Z.; Li, F.; Wu, X.; Shi, X. Healthy Ageing and Biomarkers Cohort Study (HABCS): A Cohort Profile. BMJ Open 2019, 9, e026513. [Google Scholar] [CrossRef]
- Collerton, J.; Barrass, K.; Bond, J.; Eccles, M.; Jagger, C.; James, O.; Martin-Ruiz, C.; Robinson, L.; Von Zglinicki, T.; Kirkwood, T. The Newcastle 85+ Study: Biological, Clinical and Psychosocial Factors Associated with Healthy Ageing: Study Protocol. BMC Geriatr. 2007, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Rafiei, H.; Ashrafizadeh, M.; Ahmadi, Z. MicroRNAs as Novel Targets of Sulforaphane in Cancer Therapy: The Beginning of a New Tale? Phytother. Res. 2020, 34, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Agricultura, Pesca y Alimentación Encuesta Sobre Superficies y Rendimientos Cultivos (ESYRCE). Available online: https://www.mapa.gob.es/dam/mapa/contenido/estadisticas/temas/estadisticas-agrarias/2.agricultura/1.-encuesta-sobre-superficies-y-rendimientos-de-cultivos--esyrce/2023/boletin20231.pdf (accessed on 26 June 2025).
- Asociación Ourensividad Estudio Del Fenómeno de Los Centenarios de Ourense. Available online: https://ourensividad.com/ourense-clave-para-la-longevidad-el-fenomeno-de-los-centenarios/ (accessed on 26 June 2025).
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Willcox, D.C.; Willcox, B.J.; Todoriki, H.; Suzuki, M. The Okinawan Diet: Health Implications of a Low-Calorie, Nutrient-Dense, Antioxidant-Rich Dietary Pattern Low in Glycemic Load. J. Am. Coll. Nutr. 2009, 28, 500S–516S. [Google Scholar] [CrossRef]
- Pes, G.M.; Dore, M.P.; Tsofliou, F.; Poulain, M. Diet and Longevity in the Blue Zones: A Set-and-Forget Issue? Maturitas 2022, 164, 31–37. [Google Scholar] [CrossRef]
- Fastame, M.C. Well-Being, Food Habits, and Lifestyle for Longevity. Preliminary Evidence from the Sardinian Centenarians and Long-Lived People of the Blue Zone. Psychol. Health Med. 2022, 27, 728–733. [Google Scholar] [CrossRef]
- Agabio, R.; Pisanu, C.; Minerba, L.; Gessa, G.L.; Franconi, F. Gender Differences among Sardinians with Alcohol Use Disorder. J. Clin. Med. 2021, 10, 4688. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Item | Ourense (303,450 Inhabitants) | Sardinia (56,000 Inhabitants) | Okinawa (1,285,000 Inhabitants) |
|---|---|---|---|
| Pork | Most consumed meat | Most consumed meat | Most consumed meat. All parts are eaten, including tendons and cartilage |
| Cheese | Yes, with quality labels. Cow | Yes, widely consumed. Sheep and goat | Little. Cow |
| Vegetables | Mainly brassica varieties | Smaller quantities. Diet predominantly animal-based | Yes, combined with other foods |
| Preferred fish type | Oily fish from the Atlantic Ocean | White fish from the Mediterranean Sea | Freshwater fish |
| Milk | Significant quantity. Cow | Significant, rich in arzanol | Significant |
| Wine | Very little | Moderate, consumed with meals | Little |
| Typical dish | Galician stew | Minestrone with onion, carrots, legumes, and fennel | Food combination: fish with pig liver, garlic, and carrot |
| Seaweed | Not consumed | Rarely consumed | Frequently consumed (Saccharina japonica) |
| Bread | Yes, with Protected Geographical Indication | Yes, served with meals. Very distinctive | No |
| Caloric restriction | No (2200–2700 kcal) | No (2200–2700 kcal) | Yes (1800–2200 kcal) |
| Cured meats | Chorizo | Plant-complemented cured meats. “Guanciale” | Rarely consumed |
| Type of fat | Extra virgin olive oil | Lard and pork fat until nutritional transition | Pork fat |
| Condiment | Paprika | Saba (grape syrup) | Turmeric |
| Other characteristic foods | Chestnuts | Mastic tree oil | Soya and tofu |
| Sugars | A Lot | Quite a Bit | A Little | None | Total |
|---|---|---|---|---|---|
| No Dementia | 10 | 11 | 25 | 1 | 47 |
| Dementia | 4 | 9 | 50 | 1 | 64 |
| Total | 14 | 20 | 75 | 2 | 111 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Vivanco, P.; Fernandez, R.; Meijide-Faílde, R.; Navarro-Pardo, E.; Conde, C.; de la Fuente, R.; Margusinos, C.; Rodríguez, A.; Canelada, A.; Taboada, P.; et al. Exploring the Dietary Patterns and Health Behaviours of Centenarians in Ourense (Spain): Adherence to the Southern European Atlantic Diet. Nutrients 2025, 17, 2231. https://doi.org/10.3390/nu17132231
García-Vivanco P, Fernandez R, Meijide-Faílde R, Navarro-Pardo E, Conde C, de la Fuente R, Margusinos C, Rodríguez A, Canelada A, Taboada P, et al. Exploring the Dietary Patterns and Health Behaviours of Centenarians in Ourense (Spain): Adherence to the Southern European Atlantic Diet. Nutrients. 2025; 17(13):2231. https://doi.org/10.3390/nu17132231
Chicago/Turabian StyleGarcía-Vivanco, Pablo, Roberto Fernandez, Rosa Meijide-Faílde, Esperanza Navarro-Pardo, Cristina Conde, Ricardo de la Fuente, Cristina Margusinos, Alberto Rodríguez, Ana Canelada, Pablo Taboada, and et al. 2025. "Exploring the Dietary Patterns and Health Behaviours of Centenarians in Ourense (Spain): Adherence to the Southern European Atlantic Diet" Nutrients 17, no. 13: 2231. https://doi.org/10.3390/nu17132231
APA StyleGarcía-Vivanco, P., Fernandez, R., Meijide-Faílde, R., Navarro-Pardo, E., Conde, C., de la Fuente, R., Margusinos, C., Rodríguez, A., Canelada, A., Taboada, P., Cepeda, A., & Coelho, A. (2025). Exploring the Dietary Patterns and Health Behaviours of Centenarians in Ourense (Spain): Adherence to the Southern European Atlantic Diet. Nutrients, 17(13), 2231. https://doi.org/10.3390/nu17132231