
Gender-, Age-, and Region-Specific Associations Between Obesity and Nutrition/Health Knowledge, Dietary Diversity, and Physical Activity in Chinese School-Age Students: A Cross-Sectional Study

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Obesity
2.3. Nutrition and Health Knowledge and Physical Activity Survey
2.4. DDS and PA Scoring Criteria
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Correlation of Nutritional Literacy, DDS, PA, and BMI
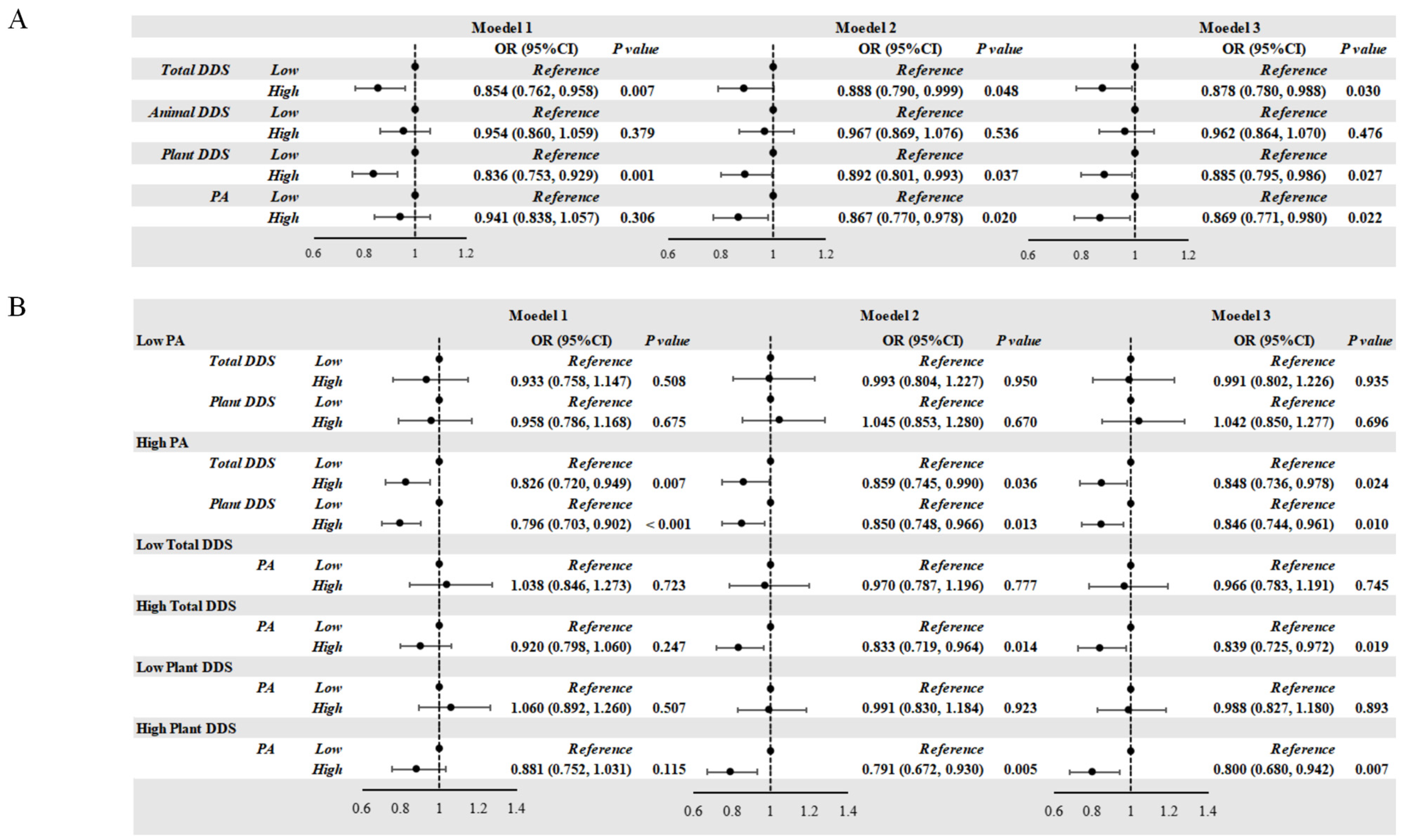
3.3. Association of DDS and PA with the Risk of Obesity
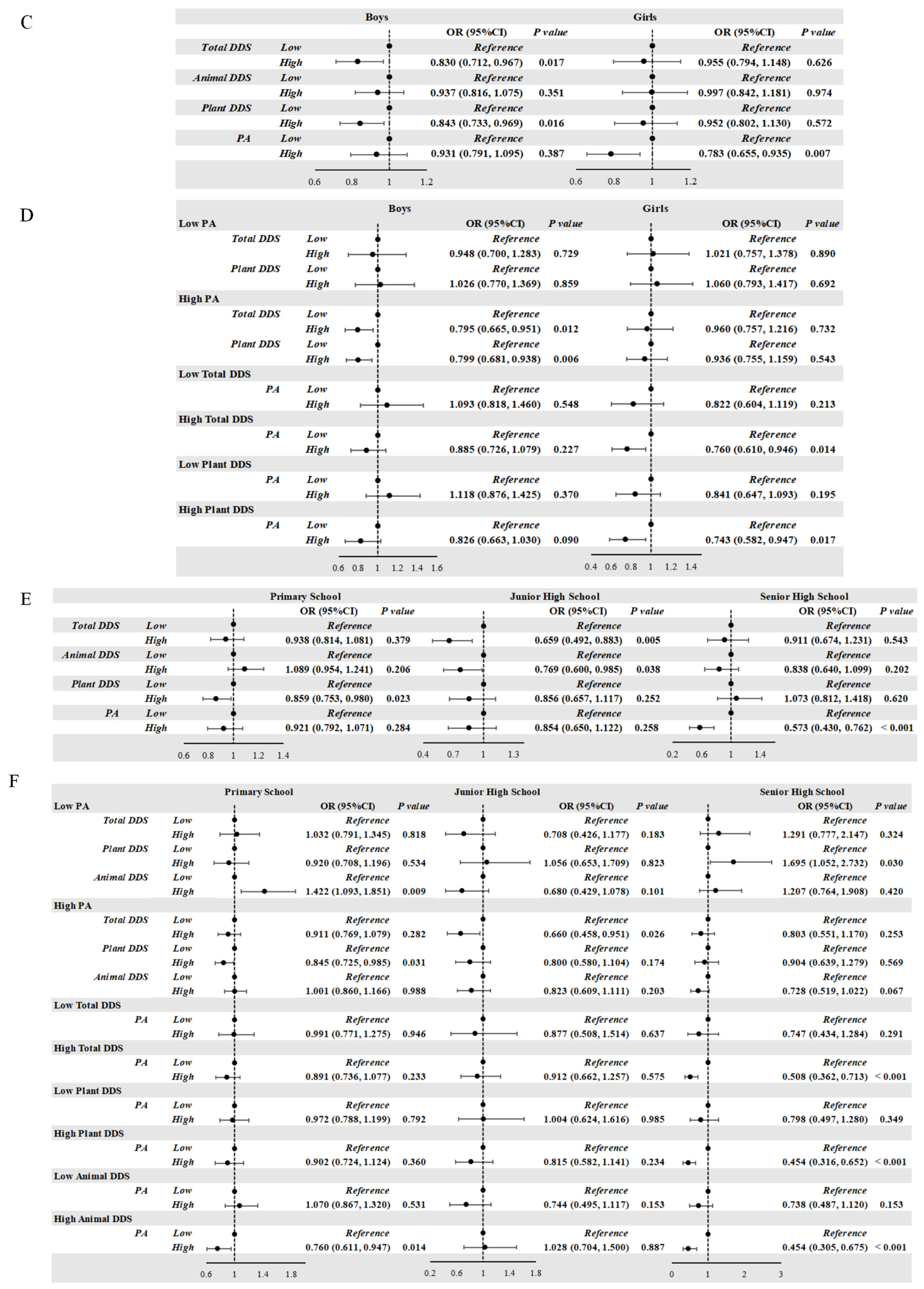
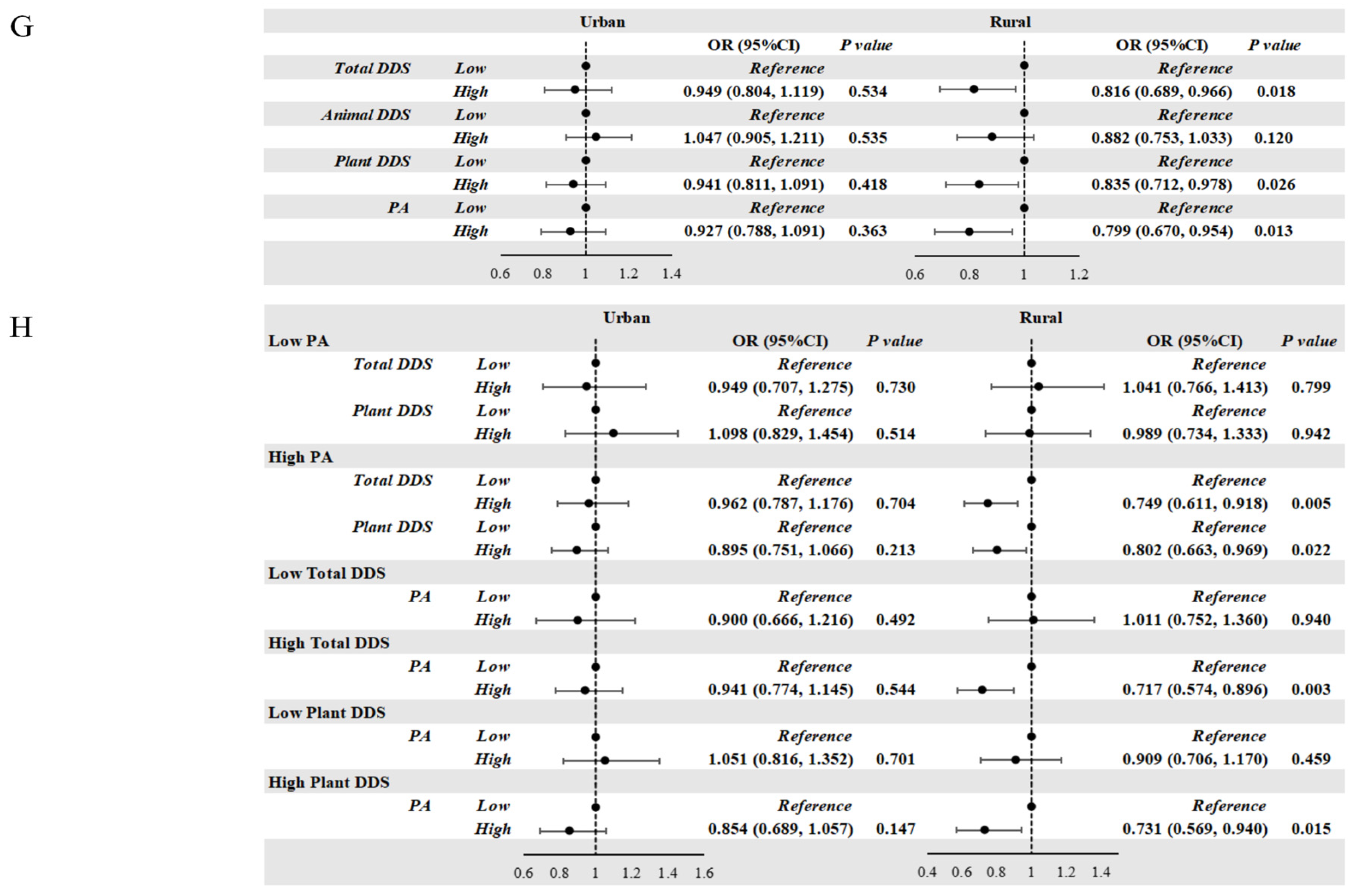
3.4. Association of DDS and PA with the Risk of Obesity According to Grade, Gender, and Residential Area
3.5. Association of DDS and PA with the Risk of Obesity According to the Combination of Grade, Gender, and Residential Area
3.6. Association of Nutritional Literacy and the Risk of Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PA | Physical Activity |
| DDS | Dietary Diversity Scores |
| WHO | World Health Organization |
| AHA | American Heart Association |
| BMI | Body Mass Index |
References
- Ma, G.-S.; Li, Y.-P.; Hu, X.-Q.; Cui, Z.-H.; Yang, X.-G.; Chen, C.-M. Report on childhood obesity in China (2). Verification of BMI classification reference for overweight and obesity in Chinese children and adolescents. Biomed. Environ. Sci. 2006, 19, 1–7. [Google Scholar] [PubMed]
- GBD 2021 Adolescent BMI Collaborators. Global, regional, and national prevalence of child and adolescent overweight and obesity, 1990-2021, with forecasts to 2050: A forecasting study for the Global Burden of Disease Study 2021. Lancet 2025, 405, 785–812. [Google Scholar] [CrossRef]
- Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 2024, 403, 1027–1050. [CrossRef] [PubMed]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Ndoadoumgue, A.L.; et al. Global, regional, and country estimates of metabolic syndrome burden in children and adolescents in 2020: A systematic review and modelling analysis. Lancet Child. Adolesc. Health 2022, 6, 158–170. [Google Scholar] [CrossRef]
- Wang, S.; Dong, Y.H.; Wang, Z.H.; Zou, Z.Y.; Ma, J. [Trends in overweight and obesity among Chinese children of 7–18 years old during 1985–2014]. Zhonghua Yu Fang Yi Xue Za Zhi 2017, 51, 300–305. [Google Scholar]
- Panera, N.; Mandato, C.; Crudele, A.; Bertrando, S.; Vajro, P.; Alisi, A. Genetics, epigenetics and transgenerational transmission of obesity in children. Front. Endocrinol. 2022, 13, 1006008. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Ullah, R.; Wang, J.-B.; Fu, J.-F. Trends of obesity and overweight among children and adolescents in China. World J. Pediatr. 2023, 19, 1115–1126. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- D’antonio, G.; Sansone, V.; Postiglione, M.; Battista, G.; Gallè, F.; Pelullo, C.P.; Di Giuseppe, G. Risky Behaviors for Non-Communicable Diseases: Italian Adolescents’ Food Habits and Physical Activity. Nutrients 2024, 16, 4162. [Google Scholar] [CrossRef]
- Cn, C. Eight Key Recommendations from Dietary Guidelines for Chinese Residents. 2022. Available online: https://en.chinacdc.cn/health_topics/nutrition_health/202206/t20220616_259702.html (accessed on 16 June 2022).
- de Oliveira Otto, M.; Anderson, C.A.M.; Dearborn, J.L.; Ferranti, E.P.; Mozaffarian, D.; Rao, G.; Wylie-Rosett, J.; Lichtenstein, A.H. Correction to: Dietary Diversity: Implications for Obesity Prevention in Adult Populations: A Science Advisory From the American Heart Association. Circulation 2018, 138, e712. [Google Scholar] [CrossRef] [PubMed]
- Pojednic, R.; D’Arpino, E.; Halliday, I.; Bantham, A. The Benefits of Physical Activity for People with Obesity, Independent of Weight Loss: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4981. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.M.; Peluso, J.; Stone, N.N.; Gow, K.; Baerg, J. Food for Thought: The Impact of a Nutritional Toolkit on Well-being in Children. J. Pediatr. Surg. 2025, 60, 162185. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.K.; Sullivan, D.K.; Ellerbeck, E.F.; Gajewski, B.J.; Gibbs, H.D. Nutrition literacy predicts adherence to healthy/unhealthy diet patterns in adults with a nutrition-related chronic condition. Public Health Nutr. 2019, 22, 2157–2169. [Google Scholar] [CrossRef]
- Yuan, C.; Dong, Y.; Chen, H.; Ma, L.; Jia, L.; Luo, J.; Liu, Q.; Hu, Y.; Ma, J.; Song, Y. Determinants of childhood obesity in China. Lancet Public Health 2024, 9, e1105–e1114. [Google Scholar] [CrossRef]
- O’Verger, E.; Le Port, A.; Borderon, A.; Bourbon, G.; Moursi, M.; Savy, M.; Mariotti, F.; Martin-Prevel, Y. Dietary Diversity Indicators and Their Associations with Dietary Adequacy and Health Outcomes: A Systematic Scoping Review. Adv. Nutr. 2021, 12, 1659–1672. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.; Ren, X.; Zhang, C.; Zhou, S.; Wang, Y.; Xu, J.; Liu, L.; Wang, Y.; Yuan, L. Association of Physical Activity and Dietary Diversity with Cognitive Function in the Elderly with Type 2 Diabetes Mellitus: Findings from a Cross-Sectional Study. J. Am. Nutr. Assoc. 2025, 44, 104–114. [Google Scholar] [CrossRef]
- Wisniewski, A.B.; Chernausek, S.D. Gender in childhood obesity: Family environment, hormones, and genes. Gend. Med. 2009, 6 (Suppl. 1), 76–85. [Google Scholar] [CrossRef]
- Garnett, S.P.; Högler, W.; Blades, B.; Baur, L.A.; Peat, J.; Lee, J.; Cowell, C.T. Relation between hormones and body composition, including bone, in prepubertal children. Am. J. Clin. Nutr. 2004, 80, 966–972. [Google Scholar] [CrossRef]
- Xie, B.; Chou, C.-P.; Spruijt-Metz, D.; Reynolds, K.; Clark, F.; Palmer, P.H.; Gallaher, P.; Sun, P.; Guo, Q.; Johnson, C.A. Weight perception and weight-related sociocultural and behavioral factors in Chinese adolescents. Prev. Med. 2006, 42, 229–234. [Google Scholar] [CrossRef]
- Keller, K.L.; Kling, S.M.R.; Fuchs, B.; Pearce, A.L.; Reigh, N.A.; Masterson, T.; Hickok, K. A Biopsychosocial Model of Sex Differences in Children’s Eating Behaviors. Nutrients 2019, 11, 682. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Wu, H.; Lee, T.; Wang, C.M.; Zhou, X.; Lu, Y.; Yuan, Z.; Maddock, J.E. Gender Differences in Home Environments Related to Childhood Obesity in Nanchang, China. Child. Obes. 2014, 10, 416–423. [Google Scholar] [CrossRef]
- Seum, T.; Meyrose, A.-K.; Rabel, M.; Schienkiewitz, A.; Ravens-Sieberer, U. Pathways of Parental Education on Children’s and Adolescent’s Body Mass Index: The Mediating Roles of Behavioral and Psychological Factors. Front. Public Health 2022, 10, 763789. [Google Scholar] [CrossRef]
- Tong, Z.; Zhang, H.; Yu, J.; Jia, X.; Hou, X.; Kong, Z. Spatial-temporal evolution of overweight and obesity among Chinese adolescents from 2016 to 2020. iScience 2024, 27, 108742. [Google Scholar] [CrossRef]
- Dong, Y.H.; Chen, L.; Liu, J.Y.; Ma, T.; Zhang, Y.; Chen, M.M.; Zhong, P.L.; Shi, D.; Hu, P.J.; Li, J.; et al. [Epidemiology and prediction of overweight and obesity among children and adolescents aged 7-18 years in China from 1985 to 2019]. Zhonghua Yu Fang Yi Xue Za Zhi 2023, 57, 11–19. [Google Scholar] [PubMed]
- Huang, Y.; Tian, X. Food accessibility, diversity of agricultural production and dietary pattern in rural China. Food Policy 2019, 84, 92–102. [Google Scholar] [CrossRef]
- Millward, D.J. Nutrition, infection and stunting: The roles of deficiencies of individual nutrients and foods, and of inflammation, as determinants of reduced linear growth of children. Nutr. Res. Rev. 2017, 30, 50–72. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.; Schoenmakers, I.; Laskey, M.A.; de Bono, S.; Ginty, F.; Goldberg, G.R. Nutrition and bone growth and development. Proc. Nutr. Soc. 2006, 65, 348–360. [Google Scholar] [CrossRef]
- Adegoke, O.; Huang, Y.; Fu, X.; Mora, S. Editorial: Nutrition in the Regulation of Muscle Development and Repair. Front. Physiol. 2022, 13, 853007. [Google Scholar] [CrossRef]
- López, L.F.M.; Llerena, J.L.G.; Rodríguez, J.A.V.; Guerrero, A.B.M.; Martínez, B.E.G.; Pérez, E.S.; Lomelí, M.L.-C. Dietary Modulation of the Immune System. Nutrients 2024, 16, 4363. [Google Scholar] [CrossRef]
- Das, J.K.; Salam, R.A.; Thornburg, K.L.; Prentice, A.M.; Campisi, S.; Lassi, Z.S.; Koletzko, B.; Bhutta, Z.A. Nutrition in adolescents: Physiology, metabolism, and nutritional needs. Ann. N. Y Acad. Sci. 2017, 1393, 21–33. [Google Scholar] [CrossRef]
- V P, N.P.; Joye, I.J. Dietary Fibre from Whole Grains and Their Benefits on Metabolic Health. Nutrients 2020, 12, 3045. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef] [PubMed]
- Jagiello, T.; Belcher, J.; Neelakandan, A.; Boyd, K.; Wuthrich, V.M. Academic Stress Interventions in High Schools: A Systematic Literature Review. Child. Psychiatry Hum. Dev. 2024; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Almaqhawi, A.; Albarqi, M. The effects of technology use on children’s physical activity: A cross-sectional study in the Eastern province of Saudi Arabia. J. Med. Life 2022, 15, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- E, Y.; Yang, J.; Shen, Y.; Quan, X. Physical Activity, Screen Time, and Academic Burden: A Cross-Sectional Analysis of Health among Chinese Adolescents. Int. J. Environ. Res. Public. Health 2023, 20, 4917. [Google Scholar] [CrossRef]
- Pereira, P.M.; Vicente, A.F. Meat nutritional composition and nutritive role in the human diet. Meat Sci. 2013, 93, 586–592. [Google Scholar] [CrossRef]
- Intiful, F.D.; Oddam, E.G.; Kretchy, I.; Quampah, J. Exploring the relationship between the big five personality characteristics and dietary habits among students in a Ghanaian University. BMC Psychol. 2019, 7, 1–7. [Google Scholar] [CrossRef]
- Mahmood, L.; Flores-Barrantes, P.; Moreno, L.A.; Manios, Y.; Gonzalez-Gil, E.M. The Influence of Parental Dietary Behaviors and Practices on Children’s Eating Habits. Nutrients 2021, 13, 1138. [Google Scholar] [CrossRef]
- Bahnfleth, C.; Cole, N.C.; Kingshipp, B.J.; Scinto-Madonich, S.; Butera, G.; Spahn, J. School-Based Strategies to Improve Acceptance of Healthier Foods and Dietary Patterns: A Rapid Review; USDA Nutrition Evidence Systematic Review: Alexandria, VA, USA, 2022. [Google Scholar]
- Kuwahara, M.; Eum, W. Effects of Childhood Nutrition Education from School and Family on Eating Habits of Japanese Adults. Nutrients 2022, 14, 2517. [Google Scholar] [CrossRef]
- Harris, J.L.; Bargh, J.A.; Brownell, K.D. Priming effects of television food advertising on eating behavior. Health Psychol. 2009, 28, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.; Braet, C.; Van Vlierberghe, L.; Mels, S. Loss of control over eating in overweight youngsters: The role of anxiety, depression and emotional eating. Eur. Eat. Disord. Rev. 2009, 17, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Lemon, S.C.; Pagoto, S.L.; Barton, B.A.; Lapane, K.L.; Goldberg, R.J. Personal and parental weight misperception and self-reported attempted weight loss in us children and adolescents, national health and nutrition examination survey, 2007–2008 and 2009–2010. Prev. Chronic Dis. 2014, 11, E132. [Google Scholar] [CrossRef] [PubMed]
- China Raises Government Subsidies for Basic Public Health Services. Available online: https://english.www.gov.cn/news/202307/12/content_WS64aea86ec6d0868f4e8ddb99.html (accessed on 12 July 2023).
- China Issues Guidelines for High-Quality Development of Disease Prevention, Control. Available online: https://english.www.gov.cn/policies/latestreleases/202312/27/content_WS658b5bdfc6d0868f4e8e289b.html (accessed on 27 December 2023).
- China to Integrate Student Health Education and All-Around Development. Available online: https://english.www.gov.cn/statecouncil/ministries/202109/05/content_WS6133f8f3c6d0df57f98dfb0e.html (accessed on 5 September 2021).

{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Obesity (n = 1681) | Control (n = 9604) | Total (n = 11,285) | p Value |
|---|---|---|---|---|
| Age (years) | 11.32 ± 3.28 | 12.91 ± 3.44 | 12.67 ± 3.46 | <0.001 |
| BMI (kg/m2) | 27.16 ± 4.67 | 18.65 ± 3.25 | 19.92 ± 4.63 | <0.001 |
| Gender, n (%) | <0.001 | |||
| Boys | 1052 (62.6) | 4582 (47.7) | 5634 (49.9) | |
| Girls | 629 (37.4) | 5022 (52.3) | 5651 (50.1) | |
| Residential area, n (%) | 0.005 | |||
| Urban | 932 (55.4) | 4965 (51.7) | 5897 (52.3) | |
| Rural | 749 (44.6) | 4639 (48.3) | 5388 (47.7) | |
| Living at school, n (%) | <0.001 | |||
| Yes | 217 (12.9) | 2281 (23.8) | 2498 (22.1) | |
| No | 1464 (87.1) | 7323 (76.2) | 8787 (77.9) | |
| Dining at school, n (%) | <0.001 | |||
| Yes | 801 (47.7) | 5895 (61.4) | 6696 (59.3) | |
| No | 880 (52.3) | 3709 (38.6) | 4589 (40.7) | |
| Cooking responsibility, n (%) | 0.189 | |||
| Father | 190 (11.3) | 1123 (11.7) | 1313 (11.6) | |
| Mother | 1030 (61.3) | 6073 (63.2) | 7103 (62.9) | |
| Grandparents | 419 (24.9) | 2214 (23.1) | 2633 (23.3) | |
| Others | 42 (2.5) | 194 (2.0) | 236 (2.1) | |
| Father’s education, n (%) | <0.001 | |||
| Primary school | 115 (6.8) | 489 (5.1) | 604 (5.4) | |
| Junior high school | 646 (38.4) | 4296 (44.7) | 4942 (43.8) | |
| High school | 461 (27.4) | 2590 (27.0) | 3051 (27.0) | |
| Junior college and above | 309 (18.4) | 1566 (16.3) | 1875 (16.6) | |
| Unknown | 150 (8.9) | 663 (6.9) | 813 (7.2) | |
| Mother’s education, n (%) | <0.001 | |||
| Primary school | 220 (13.1) | 1163 (12.1) | 1383 (12.3) | |
| Junior high school | 650 (38.7) | 4278 (44.5) | 4928 (43.7) | |
| High school | 355 (21.1) | 2035 (21.2) | 2390 (21.2) | |
| Junior college and above | 284 (16.9) | 1458 (15.2) | 1742 (15.4) | |
| Unknown | 172 (10.2) | 670 (7.0) | 842 (7.5) |
| Variables | Obesity (n = 1681) | Control (n = 9604) | Total (n = 11,285) | p Value |
|---|---|---|---|---|
| Dietary Intake (Times/Week) | ||||
| Cereals | 5.436 ± 2.262 | 5.627 ± 2.121 | 5.598 ± 2.144 | 0.001 |
| Vegetables | 5.430 ± 2.182 | 5.627 ± 2.020 | 5.598 ± 2.046 | 0.001 |
| Fruits | 5.124 ± 2.254 | 5.210 ± 2.172 | 5.197 ± 2.184 | 0.150 |
| Dairy | 4.805 ± 2.389 | 4.813 ± 2.334 | 4.812 ± 2.342 | 0.906 |
| Legumes | 3.899 ± 2.496 | 3.973 ± 2.463 | 3.962 ± 2.468 | 0.256 |
| Eggs | 4.891 ± 2.401 | 4.940 ± 2.342 | 4.933 ± 2.351 | 0.434 |
| Meat | 4.639 ± 2.257 | 4.679 ± 2.212 | 4.673 ± 2.219 | 0.492 |
| Whole grain | 4.540 ± 2.411 | 4.554 ± 2.325 | 4.552 ± 2.337 | 0.825 |
| Sea foods | 2.792 ± 2.496 | 2.716 ± 2.393 | 2.728 ± 2.409 | 0.247 |
| DDS (points) | ||||
| Total DDS | 13.256 ± 3.190 | 13.438 ± 3.187 | 13.411 ± 3.188 | 0.032 |
| Animal DDS | 5.569 ± 1.711 | 5.588 ± 1.666 | 5.585 ± 1.673 | 0.666 |
| Plant DDS | 7.688 ± 1.895 | 7.850 ± 1.886 | 7.826 ± 1.888 | 0.001 |
| PA (points) | 2.233 ± 1.005 | 2.251 ± 1.036 | 2.236 ± 1.010 | 0.514 |
| Total nutritional literacy (points) | 77.53 ± 16.71 | 74.75 ± 15.59 | 75.17 ± 15.79 | <0.001 |
| Variables | Obesity | Control | p Value | ||
|---|---|---|---|---|---|
| Boys (n = 1052) | Girls (n = 629) | Boys (n = 4582) | Girls (n = 5022) | ||
| Dietary intakes (times/week) | |||||
| Cereals | 5.554 ± 2.200 | 5.240 ± 2.351 a | 5.777 ± 2.044 b | 5.490 ± 2.181 a,b | <0.001 |
| Vegetables | 5.435 ± 2.182 | 5.422 ± 2.184 | 5.619 ± 2.017 b | 5.635 ± 2.022 b | 0.004 |
| Fruits | 5.130 ± 2.244 | 5.114 ± 2.271 | 5.182 ± 2.200 | 5.234 ± 2.146 | 0.313 |
| Dairy | 4.890 ± 2.374 | 4.664 ± 2.409 | 4.987 ± 2.320 | 4.654 ± 2.336 a | <0.001 |
| Legumes | 4.021 ± 2.491 | 3.694 ± 2.493 a | 4.180 ± 2.458 | 3.784 ± 2.453 a | <0.001 |
| Eggs | 4.940 ± 2.377 | 4.809 ± 2.441 | 5.099 ± 2.294 b | 4.795 ± 2.377 a | <0.001 |
| Meat | 4.939 ± 2.185 | 4.137 ± 2.288 a | 4.934 ± 2.149 | 4.446 ± 2.243 a,b | <0.001 |
| Whole grain | 4.594 ± 2.412 | 4.451 ± 2.407 | 4.649 ± 2.320 | 4.468 ± 2.326 a | 0.001 |
| Sea foods | 2.919 ± 2.564 | 2.580 ± 2.363 a | 2.867 ± 2.471 | 2.579 ± 2.312 a | <0.001 |
| DDS (points) | |||||
| Total DDS | 13.446 ± 3.208 | 12.940 ± 3.135 a | 13.703 ± 3.172 b | 13.195 ± 3.182 a | <0.001 |
| Animal DDS | 5.696 ± 1.685 | 5.356 ± 1.734 a | 5.756 ± 1.643 | 5.434 ± 1.673 a | <0.001 |
| Plant DDS | 7.750 ± 1.921 | 7.583 ± 1.846 | 7.947 ± 1.887 b | 7.761 ± 1.882 a,b | <0.001 |
| PA (points) | 2.384 ± 1.051 | 2.029 ± 0.972 a | 2.432 ± 1.047 | 2.052 ± 0.929 a | <0.001 |
| Total nutritional literacy (points) | 76.04 ± 17.15 | 80.04 ± 15.63 a | 74.10 ± 16.40 b | 75.34 ± 14.78 a,b | <0.001 |
| Variables | Obesity | Control | p Value | ||
|---|---|---|---|---|---|
| Urban (n = 932) | Rural (n = 749) | Urban (n = 4965) | Rural (n = 4639) | ||
| Dietary intakes (times/week) | |||||
| Cereals | 5.378 ± 2.276 | 5.509 ± 2.244 | 5.563 ± 2.149 a | 5.695 ± 2.090 a,b | <0.001 |
| Vegetables | 5.519 ± 2.177 | 5.320 ± 2.185 b | 5.725 ± 1.942 a | 5.523 ± 2.095 a,b | <0.001 |
| Fruits | 5.343 ± 2.192 | 4.852 ± 2.301 b | 5.306 ± 2.098 | 5.107 ± 2.244 a,b | <0.001 |
| Dairy | 4.831 ± 2.430 | 4.774 ± 2.339 | 4.939 ± 2.291 | 4.678 ± 2.372 b | <0.001 |
| Legumes | 3.951 ± 2.506 | 3.833 ± 2.483 | 4.023 ± 2.438 | 3.919 ± 2.489 | 0.088 |
| Eggs | 4.939 ± 2.395 | 4.831 ± 2.410 | 4.905 ± 2.323 | 4.978 ± 2.363 | 0.278 |
| Meat | 4.761 ± 2.236 | 4.486 ± 2.275 b | 4.814 ± 2.172 | 4.535 ± 2.245 b | <0.001 |
| Whole grain | 4.620 ± 2.387 | 4.441 ± 2.437 | 4.585 ± 2.308 | 4.521 ± 2.342 | 0.230 |
| Sea foods | 2.948 ± 2.554 | 2.598 ± 2.409 b | 2.752 ± 2.365 a | 2.678 ± 2.423 | 0.006 |
| DDS (points) | |||||
| Total DDS | 13.437 ± 3.168 | 13.032 ± 3.204 b | 13.578 ± 3.057 | 13.288 ± 3.314 a,b | <0.001 |
| Animal DDS | 5.652 ± 1.724 | 5.465 ± 1.690 b | 5.661 ± 1.615 | 5.510 ± 1.716 b | <0.001 |
| Plant DDS | 7.784 ± 1.891 | 7.567 ± 1.894 b | 7.917 ± 1.817 a | 7.778 ± 1.955 a,b | <0.001 |
| PA (points) | 2.255 ± 1.036 | 2.246 ± 1.037 | 2.180 ± 0.992 a | 2.290 ± 1.015 b | <0.001 |
| Total nutritional literacy (points) | 77.93 ± 15.71 | 77.04 ± 17.87 | 75.44 ± 14.67 a | 74.01 ± 16.48 a,b | <0.001 |
| Variables | Obesity | Control | p Value | ||||
|---|---|---|---|---|---|---|---|
| Primary School (n = 1141) | Junior High School (n = 303) | Senior High School (n = 237) | Primary (n = 4441) | Junior High School (n = 2700) | Senior High School (n = 2463) | ||
| Dietary intake (times/week) | |||||||
| Cereals | 5.046 ± 2.418 | 6.353 ± 1.476 a | 6.146 ± 1.755 a | 5.022 ± 2.367 | 6.314 ± 1.561 a | 5.963 ± 1.868 a,b | <0.001 |
| Vegetables | 5.218 ± 2.301 | 6.041 ± 1.731 a | 5.669 ± 1.932 a,b | 5.368 ± 2.170 c | 6.027 ± 1.726 a | 5.657 ± 1.963 a,b | <0.001 |
| Fruits | 5.144 ± 2.274 | 5.337 ± 2.100 | 4.755 ± 2.313 a,b | 5.227 ± 2.171 | 5.458 ± 2.028 a | 4.906 ± 2.289 a,b | <0.001 |
| Dairy | 4.770 ± 2.431 | 5.117 ± 2.250 a | 4.580 ± 2.330 b | 4.619 ± 2.408 | 5.221 ± 2.177 a | 4.714 ± 2.310 b | <0.001 |
| Legumes | 3.699 ± 2.542 | 4.554 ± 2.262 a | 4.023 ± 2.413 b | 3.613 ± 2.477 | 4.646 ± 2.322 a | 3.885 ± 2.438 a,b | <0.001 |
| Eggs | 4.845 ± 2.457 | 4.983 ± 2.302 | 4.994 ± 2.252 | 4.808 ± 2.413 | 5.120 ± 2.245 a | 4.982 ± 2.304 a,b | <0.001 |
| Meat | 4.360 ± 2.310 | 5.182 ± 2.067 a | 5.285 ± 1.963 a | 4.176 ± 2.263 c | 5.230 ± 2.029 a | 4.981 ± 2.110 a,b,c | <0.001 |
| Whole grain | 4.555 ± 2.418 | 4.508 ± 2.384 | 4.513 ± 2.418 | 4.527 ± 2.301 | 4.909 ± 2.258 a,c | 4.216 ± 2.385 a,b | <0.001 |
| Sea foods | 2.780 ± 2.472 | 3.030 ± 2.526 | 2.546 ± 2.556 b | 2.581 ± 2.307 c | 3.101 ± 2.463 a | 2.538 ± 2.421 b | <0.001 |
| DDS (points) | |||||||
| Total DDS | 12.972 ± 3.155 | 14.172 ± 3.153 a | 13.456 ± 3.176 a,b | 12.941 ± 3.093 | 14.344 ± 3.033 a | 13.339 ± 3.304 a,b | <0.001 |
| Animal DDS | 5.474 ± 1.714 | 5.898 ± 1.715 a | 5.603 ± 1.643 b | 5.364 ± 1.653 c | 5.954 ± 1.626 a | 5.589 ± 1.663 a,b | <0.001 |
| Plant DDS | 7.498 ± 1.909 | 8.274 ± 1.711 a | 7.852 ± 1.889 a,b | 7.577 ± 1.882 | 8.390 ± 1.707 a | 7.750 ± 1.958 a,b | <0.001 |
| PA (points) | 2.319 ± 1.046 | 2.165 ± 0.986 a | 2.034 ± 1.016 a | 2.316 ± 1.032 | 2.177 ± 0.974 a | 2.146 ± 0.977 a | <0.001 |
| Total nutritional literacy (points) | 82.25 ± 15.51 | 70.25 ± 14.76 a | 64.14 ± 13.81 a,b | 82.07 ± 14.30 | 71.00 ± 14.01 a | 65.66 ± 13.00 a,b | <0.001 |
| Grade | Region | Gender | n | OR 95%CI | p | OR 95%CI | p | OR 95%CI | p |
|---|---|---|---|---|---|---|---|---|---|
| High Total DDS (12–18) | High Plant DDS (8–10) | High PA (2–4) | |||||||
| Primary School | Urban | Total | 2876 | 0.972 (0.802, 1.178) | 0.770 | 0.876 (0.743, 1.045) | 0.141 | 1.005 (0.820, 1.233) | 0.959 |
| Boys | 1458 | 0.808 (0.626, 1.044) | 0.103 | 0.810 (0.640, 1.026) | 0.080 | 0.917 (0.693, 1.212) | 0.542 | ||
| Girls | 1418 | 1.167 (0.865, 1.574) | 0.311 | 0.950 (0.723, 1.248) | 0.712 | 1.027 (0.757, 1.392) | 0.864 | ||
| Rural | Total | 2706 | 0.932 (0.757, 1.147) | 0.507 | 0.863 (0.710, 1.049) | 0.138 | 0.911 (0.730, 1.136) | 0.409 | |
| Boys | 1357 | 0.969 (0.733, 1.281) | 0.825 | 0.788 (0.609, 1.021) | 0.072 | 1.240 (0.895, 1.718) | 0.196 | ||
| Girls | 1349 | 0.854 (0.623, 1.171) | 0.327 | 0.923 (0.681, 1.250) | 0.605 | 0.590 (0.430, 0.809) | 0.001 | ||
| Junior High School | Urban | Total | 1686 | 1.001 (0.648, 1.547) | 0.996 | 1.112 (0.769, 1.610) | 0.572 | 1.328 (0.934, 1.887) | 0.114 |
| Boys | 839 | 0.839 (0.478, 1.474) | 0.542 | 1.145 (0.707, 1.854) | 0.583 | 1.500 (0.906, 2.482) | 0.115 | ||
| Girls | 847 | 1.063 (0.516, 2.189) | 0.868 | 0.881 (0.482, 1.611) | 0.682 | 0.746 (0.428, 1.302) | 0.302 | ||
| Rural | Total | 1317 | 0.498 (0.334, 0.743) | 0.001 | 0.703 (0.479, 1.031) | 0.071 | 0.669 (0.445, 1.006) | 0.054 | |
| Boys | 643 | 0.572 (0.342, 0.958) | 0.034 | 0.750 (0.464, 1.213) | 0.241 | 0.449 (0.263, 0.769) | 0.004 | ||
| Girls | 674 | 0.377 (0.192, 0.737) | 0.004 | 0.652 (0.336, 1.268) | 0.208 | 0.740 (0.375, 1.460) | 0.385 | ||
| Senior High School | Urban | Total | 1335 | 1.116 (0.703, 1.771) | 0.640 | 1.356 (0.893, 2.061) | 0.153 | 0.561 (0.376, 0.836) | 0.004 |
| Boys | 661 | 0.830 (0.475, 1.452) | 0.514 | 1.113 (0.670, 1.850) | 0.680 | 0.465 (0.278, 0.776) | 0.003 | ||
| Girls | 674 | 1.507 (0.635, 3.574) | 0.352 | 1.646 (0.767, 3.529) | 0.201 | 0.425 (0.207, 0.874) | 0.020 | ||
| Rural | Total | 1365 | 0.894 (0.604, 1.324) | 0.557 | 0.983 (0.678, 1.426) | 0.929 | 0.802 (0.540, 1.191) | 0.275 | |
| Boys | 676 | 0.822 (0.493, 1.373) | 0.454 | 0.905 (0.563, 1.455) | 0.681 | 0.600 (0.357, 1.009) | 0.054 | ||
| Girls | 689 | 0.849 (0.445, 1.620) | 0.620 | 1.079 (0.576, 2.023) | 0.813 | 0.852 (0.447, 1.625) | 0.627 | ||
| Group | n | OR 95%CI | p |
|---|---|---|---|
| All | 11,285 | 1.087 (0.979, 1.207) | 0.117 |
| Primary School (85–100 points vs. 0–84 points) | 5582 | 1.125 (0.986, 1.282) | 0.079 |
| Junior High School (75–100 points vs. 0–74 points) | 3003 | 1.021 (0.804, 1.297) | 0.866 |
| Senior High School (68–100 points vs. 0–67 points) | 2700 | 0.886 (0.676, 1.160) | 0.378 |
| Grade | Region | Gender | n | OR 95%CI | p |
|---|---|---|---|---|---|
| Primary School (85–100 points vs. 0–84 points) | Urban | Total | 2876 | 0.953 (0.798, 1.139) | 0.599 |
| Boys | 1458 | 1.028 (0.811, 1.302) | 0.819 | ||
| Girls | 1418 | 0.887 (0.673, 1.169) | 0.394 | ||
| Rural | Total | 2706 | 1.365 (1.121, 1.662) | 0.002 | |
| Boys | 1357 | 1.026 (0.793, 1.328) | 0.845 | ||
| Girls | 1349 | 2.167 (1.571, 2.989) | <0.001 | ||
| Junior High School (75–100 points vs. 0–74 points) | Urban | Total | 1686 | 1.097 (0.804, 1.499) | 0.559 |
| Boys | 839 | 1.271 (0.865, 1.866) | 0.222 | ||
| Girls | 847 | 0.835 (0.477, 1.461) | 0.528 | ||
| Rural | Total | 1317 | 0.898 (0.614, 1.313) | 0.580 | |
| Boys | 643 | 0.846 (0.525, 1.361) | 0.489 | ||
| Girls | 674 | 1.012 (0.525, 1.950) | 0.971 | ||
| Senior High School (68–100 points vs. 0–67 points) | Urban | Total | 1335 | 0.801 (0.541, 1.185) | 0.267 |
| Boys | 661 | 0.722 (0.448, 1.164) | 0.181 | ||
| Girls | 674 | 0.995 (0.486, 2.038) | 0.990 | ||
| Rural | Total | 1365 | 0.984 (0.677, 1.429) | 0.932 | |
| Boys | 676 | 1.091 (0.676, 1.758) | 0.722 | ||
| Girls | 689 | 0.992 (0.531, 1.854) | 0.981 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, X.; Liu, Y.; Wang, X.; Li, R.; Guo, X.; Zhao, S.; Yan, R.; Zhang, C.; Zhou, S.; Yuan, L.; et al. Gender-, Age-, and Region-Specific Associations Between Obesity and Nutrition/Health Knowledge, Dietary Diversity, and Physical Activity in Chinese School-Age Students: A Cross-Sectional Study. Nutrients 2025, 17, 2214. https://doi.org/10.3390/nu17132214
Ren X, Liu Y, Wang X, Li R, Guo X, Zhao S, Yan R, Zhang C, Zhou S, Yuan L, et al. Gender-, Age-, and Region-Specific Associations Between Obesity and Nutrition/Health Knowledge, Dietary Diversity, and Physical Activity in Chinese School-Age Students: A Cross-Sectional Study. Nutrients. 2025; 17(13):2214. https://doi.org/10.3390/nu17132214
Chicago/Turabian StyleRen, Xiuwen, Yu Liu, Xixiang Wang, Ronghua Li, Xiaoxiao Guo, Suhua Zhao, Rui Yan, Chi Zhang, Shaobo Zhou, Linhong Yuan, and et al. 2025. "Gender-, Age-, and Region-Specific Associations Between Obesity and Nutrition/Health Knowledge, Dietary Diversity, and Physical Activity in Chinese School-Age Students: A Cross-Sectional Study" Nutrients 17, no. 13: 2214. https://doi.org/10.3390/nu17132214
APA StyleRen, X., Liu, Y., Wang, X., Li, R., Guo, X., Zhao, S., Yan, R., Zhang, C., Zhou, S., Yuan, L., & Li, W. (2025). Gender-, Age-, and Region-Specific Associations Between Obesity and Nutrition/Health Knowledge, Dietary Diversity, and Physical Activity in Chinese School-Age Students: A Cross-Sectional Study. Nutrients, 17(13), 2214. https://doi.org/10.3390/nu17132214