
Mediterranean Diet Compliance Is Related with Lower Prevalence of Perceived Stress and Poor Sleep Quality in University Students: A Cross-Sectional Study in Greece

 ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Methods
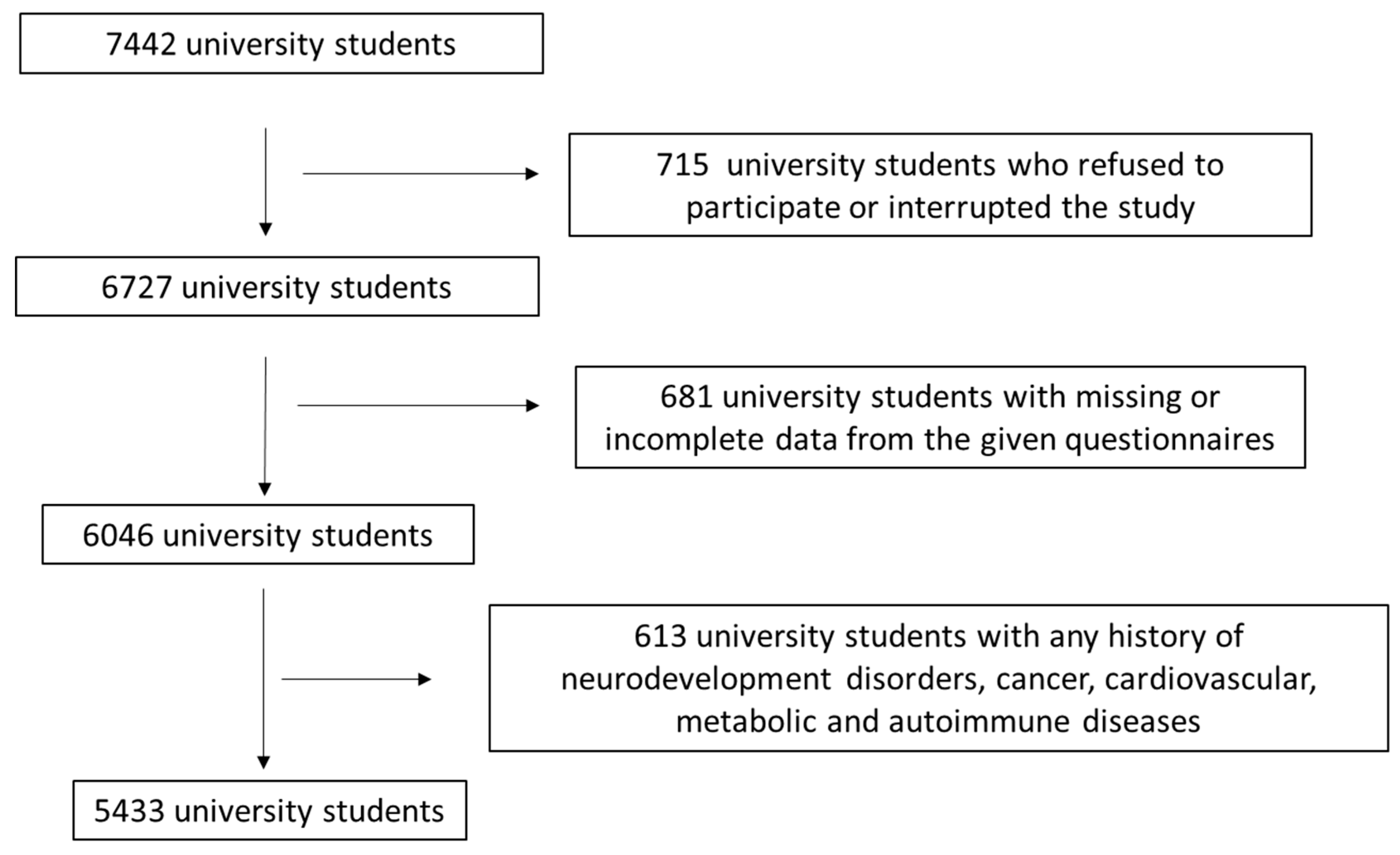
2.1. Study Population
2.2. Assessment of Sociodemographic and Anthropometric Factors
2.3. Evaluation and Lifestyle Factors
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Study Population
3.2. Association of MD Adherence with Sociodemographic, Anthropometric and Lifestyle Factors
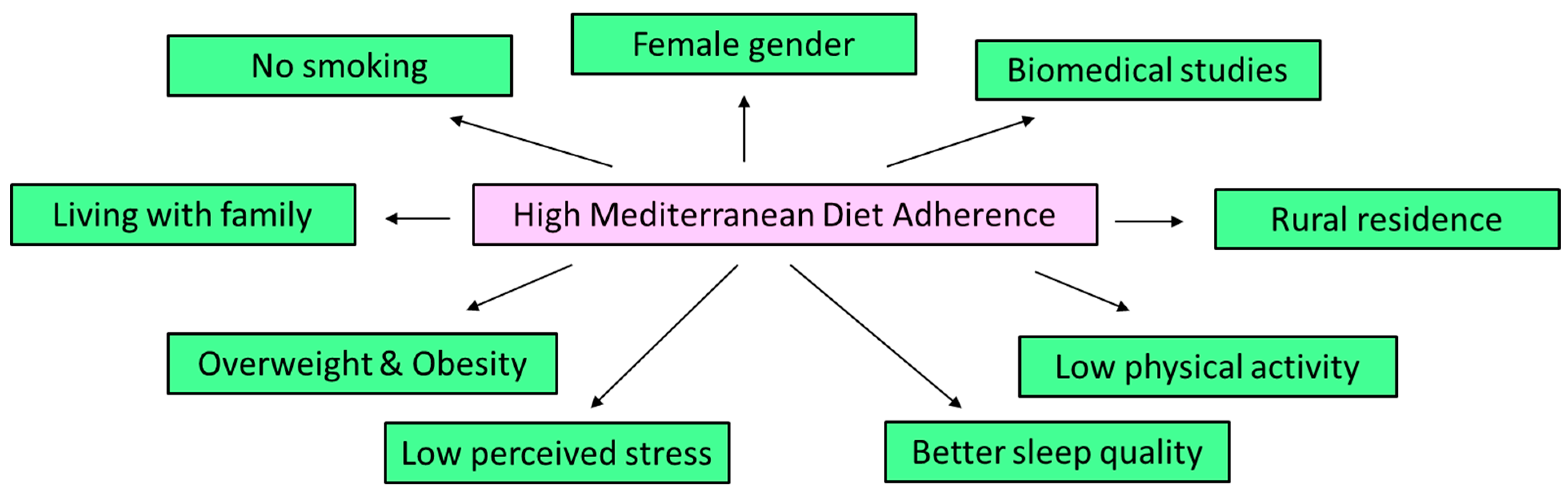
3.3. Multivariate Binary Logistic Regression Analysis for MD Adherence of the Study Population
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean diet: An update of the clinical trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean diet and cardiovascular health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Russo, G.L.; Siani, A.; Fogliano, V.; Geleijnse, J.M.; Giacco, R.; Giampaoli, S.; Iacoviello, L.; Kromhout, D.; Lionetti, L.; Naska, A.; et al. The Mediterranean diet from past to future: Key concepts from the second “Ancel Keys” International Seminar. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and metabolic syndrome: An updated systematic review. Rev. Endocr. Metab. Disord. 2013, 14, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Hashash, J.G.; Elkins, J.; Lewis, J.D.; Binion, D.G. AGA Clinical Practice Update on Diet and Nutritional Therapies in Patients With Inflammatory Bowel Disease: Expert Review. Gastroenterology 2024, 166, 521–532. [Google Scholar] [CrossRef]
- Maruca, A.; Catalano, R.; Bagetta, D.; Mesiti, F.; Ambrosio, F.A.; Romeo, I.; Moraca, F.; Rocca, R.; Ortuso, F.; Artese, A.; et al. The Mediterranean Diet as source of bioactive compounds with multi-targeting anti-cancer profile. Eur. J. Med. Chem. 2019, 181, 111579. [Google Scholar] [CrossRef]
- Itsiopoulos, C.; Mayr, H.L.; Thomas, C.J. The anti-inflammatory effects of a Mediterranean diet: A review. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 415–422. [Google Scholar] [CrossRef]
- Fernandes, J.; Fialho, M.; Santos, R.; Peixoto-Plácido, C.; Madeira, T.; Sousa-Santos, N.; Virgolino, A.; Santos, O.; Vaz Carneiro, A. Is olive oil good for you? A systematic review and meta-analysis on anti-inflammatory benefits from regular dietary intake. Nutrition 2020, 69, 110559. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health benefits of the Mediterranean diet: Metabolic and molecular mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef]
- Poulios, E.; Koukounari, S.; Psara, E.; Vasios, G.K.; Sakarikou, C.; Giaginis, C. Anti-obesity properties of phytochemicals: Highlighting their molecular mechanisms against obesity. Curr. Med. Chem. 2024, 31, 25–61. [Google Scholar] [CrossRef]
- Li, H.; Qi, J.; Li, L. Phytochemicals as potential candidates to combat obesity via adipose non-shivering thermogenesis. Pharmacol. Res. 2019, 147, 104393. [Google Scholar] [CrossRef] [PubMed]
- Borah, A.K.; Sharma, P.; Singh, A.; Kalita, K.J.; Saha, S.; Chandra Borah, J. Adipose and non-adipose perspectives of plant derived natural compounds for mitigation of obesity. J. Ethnopharmacol. 2021, 280, 114410. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Toral, M.; Morales-Domínguez, Z.; Granado-Alcón, M.D.C.; Díaz-Milanés, D.; Andrés-Villas, M. Mediterranean diet, psychological adjustment and health perception in university students: The mediating effect of healthy and unhealthy food groups. Nutrients 2021, 13, 3769. [Google Scholar] [CrossRef]
- Antonopoulou, M.; Mantzorou, M.; Serdari, A.; Bonotis, K.; Vasios, G.; Pavlidou, E.; Trifonos, C.; Vadikolias, K.; Petridis, D.; Giaginis, C. Evaluating Mediterranean diet adherence in university student populations: Does this dietary pattern affect students’ academic performance and mental health? Int. J. Health Plan. Manag. 2020, 35, 5–21. [Google Scholar] [CrossRef]
- Alfaro-González, S.; Garrido-Miguel, M.; Pascual-Morena, C.; Pozuelo-Carrascosa, D.P.; Fernández-Rodríguez, R.; Martínez-Hortelano, J.A.; Mesas, A.E.; Martínez-Vizcaíno, V. The Association Between Adherence to the Mediterranean Diet and Depression and Anxiety Symptoms in University Students: The Mediating Role of Lean Mass and the Muscle Strength Index. Nutrients 2025, 17, 346. [Google Scholar] [CrossRef]
- López-Olivares, M.; Mohatar-Barba, M.; Fernández-Gómez, E.; Enrique-Mirón, C. Mediterranean diet and the emotional well-being of students of the Campus of Melilla (University of Granada). Nutrients 2020, 12, 1826. [Google Scholar] [CrossRef] [PubMed]
- Tomás-Gallego, G.; Dalmau-Torres, J.M.; Jiménez-Boraita, R.; Ortuño-Sierra, J.; Gargallo-Ibort, E. Adherence to the Mediterranean diet in Spanish university students: Association with lifestyle habits, mental and emotional well-being. Nutrients 2025, 17, 698. [Google Scholar] [CrossRef]
- Lo Moro, G.; Corezzi, M.; Bert, F.; Buda, A.; Gualano, M.R.; Siliquini, R. Mental health and adherence to Mediterranean diet among university students: An Italian cross-sectional study. J. Am. Coll. Health 2023, 71, 2451–2461. [Google Scholar] [CrossRef]
- Lutin, E.; De Raedt, W.; Steyaert, J.; Van Hoof, C.; Evers, K. Exploring the perception of stress in childhood and early adolescence. J. Exp. Child Psychol. 2023, 228, 105604. [Google Scholar] [CrossRef]
- Johnson, M.D.; Krahn, H.J.; Galambos, N.L. Perceived stress trajectories from age 25 to 50 years. Int. J. Behav. Dev. 2023, 47, 233–242. [Google Scholar] [CrossRef]
- Commodari, E.; Di Nuovo, S. Perception of stress in aging: The role of environmental variables and appraisal of the life experiences on psychological stress. Neurol. Psychiatry Brain Res. 2019, 34, 28–33. [Google Scholar] [CrossRef]
- Kuang, S.; Wen, X.; Li, C.; Yan, S.; Li, H. Perceived stress and health outcomes among Chinese university students: The chain mediating role of repetitive negative thinking and trait forgiveness. J. Health Psychol. 2025, 13591053251317322. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, O.S.; Sayed, H.A.l.; Rabei, S.; Hegazy, N. Perceived stress and anxiety among medical students at Helwan University: A cross-sectional study. J. Public Health Res. 2024, 13, 22799036241227891. [Google Scholar] [CrossRef]
- La Fauci, V.; Venuto, R.; Genovese, C.; Squeri, R.; La Spada, G.; Pappalardo, R.; Alessi, V. Study-related stress, perceived stress and quality of life among healthcare university students. Clin. Ter. 2023, 174, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Alduais, F.; Samara, A.I.; Al-Jalabneh, H.M.; Alduais, A.; Alfadda, H.; Alaudan, R. Examining Perceived Stress and Coping Strategies of University Students during COVID-19: A Cross-Sectional Study in Jordan. Int. J. Environ. Res. Public Health 2022, 19, 9154. [Google Scholar] [CrossRef]
- Alsaleem, M.A.; Alsaleem, S.A.; Shehri, S.A.; Awadalla, N.J.; Mirdad, T.M.; Abbag, F.I.; Mahfouz, A.A. Prevalence and correlates of university students’ perceived stress in southwestern Saudi Arabia. Medicine 2021, 100, e27295. [Google Scholar] [CrossRef]
- Kyung, C.A.; Hye, L.K.; Mi, C.C.; Yi, C.J. Factors affecting the quality of sleep in young adults. Res. Community Public Health Nurs. 2021, 32, 497–505. [Google Scholar] [CrossRef]
- Arab, A.; Karimi, E.; Garaulet, M.; Scheer, F.A.J.L. Dietary patterns and insomnia symptoms: A systematic review and meta-analysis. Sleep Med. Rev. 2024, 75, 101936. [Google Scholar] [CrossRef]
- Nelson, K.L.; Davis, J.E.; Corbett, C.F. Sleep quality: An evolutionary concept analysis. Nurs. Forum. 2022, 7, 144–151. [Google Scholar] [CrossRef]
- Koffel, E.; Ancoli-Israel, S.; Zee, P.; Dzierzewski, J.M. Sleep health and aging: Recommendations for promoting healthy sleep among older adults: A National Sleep Foundation report. Sleep Health 2023, 9, 821–824. [Google Scholar] [CrossRef]
- Mansolf, M.; Blackwell, C.K.; Chandran, A.; Colicino, E.; Geiger, S.; Harold, G.; McEvoy, C.; Santos, H.P., Jr.; Sherlock, P.R.; Bose, S.; et al. Caregiver perceived stress and child sleep health: An item-level individual participant data meta-analysis. J. Child Fam. Stud. 2023, 32, 2558–2572. [Google Scholar] [CrossRef] [PubMed]
- McHugh, J.E.; Lawlor, B.A. Perceived stress mediates the relationship between emotional loneliness and sleep quality over time in older adults. Br. J. Health Psychol. 2013, 18, 546–555. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, L.; Liu, Y.; Zhang, S. Effects of perceived stress on college students’ sleep quality: A moderated chain mediation model. BMC Psychol. 2024, 12, 476. [Google Scholar] [CrossRef] [PubMed]
- Tadros, M.; Newby, J.M.; Li, S.; Werner-Seidler, A. A systematic review and meta-analysis of psychological treatments to improve sleep quality in university students. PLoS ONE 2025, 20, e0317125. [Google Scholar] [CrossRef] [PubMed]
- Nakie, G.; Takelle, G.M.; Rtbey, G.; Andualem, F.; Tinsae, T.; Kassa, M.A.; Tadesse, G.; Fentahun, S.; Wassie, Y.A.; Segon, T.; et al. Sleep quality and associated factors among university students in Africa: A systematic review and meta-analysis study. Front. Psychiatry 2024, 15, 1370757. [Google Scholar] [CrossRef]
- Ordóñez, Y.; Saavedra-Clarke, S.; Reyes-García, S.; Crovetto, M.; Valladares, M.; Espinoza, V.; Machuca-Barria, C.; Cresp-Barria, M.; Durán-Agüero, S. Diet and sleep quality in chilean university students. Int. J. Adolesc. Med. Health 2024, 36, 441–448. [Google Scholar] [CrossRef]
- Ünal, G.; Özenoğlu, A. Association of Mediterranean diet with sleep quality, depression, anxiety, stress, and body mass index in university students: A cross-sectional study. Nutr. Health 2024, 2601060231207666. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Granada-López, J.M.; Martínez-Abadía, B.; Echániz-Serrano, E.; Antón-Solanas, I.; Jerue, B.A. The association between diet and sleep quality among Spanish university students. Nutrients 2022, 14, 3291. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report: 2006: Working Together for Health. Available online: https://www.who.int/publications/i/item/9241563176 (accessed on 12 March 2025).
- James, W.P.T. WHO Recognition of the Global Obesity Epidemic. Int. J. Obes. 2008, 32, S120–S126. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro Santiago, P.H.; Nielsen, T.; Smithers, L.G.; Roberts, R.; Jamieson, L. Measuring tress in Australia: Validation of the Perceived Stress Scale (PSS-14) in a national sample. Health Qual. Life Outcomes 2020, 18, 100. [Google Scholar] [CrossRef]
- Salahuddin, M.; Maru, T.T.; Kumalo, A.; Pandi-Perumal, S.R.; Bahammam, A.S.; Manzar, M.D. Validation of the Pittsburgh Sleep Quality Index in community dwelling Ethiopian adults. Health Qual. Life Outcomes 2017, 15, 58. [Google Scholar] [CrossRef]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The reliability of the Mediterranean Diet Quality Index (KIDMED) questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- El Mikkawi, H.; El Khoury, C.; Rizk, R. Adherence to the Mediterranean diet and mental health among university students in Lebanon. Appl. Food Res. 2024, 4, 100435. [Google Scholar] [CrossRef]
- Cheema, S.; Maisonneuve, P.; Abraham, A.; Chaabna, K.; Tom, A.; Ibrahim, H.; Mushannen, T.; Yousuf, W.; Lowenfels, A.B.; Mamtani, R. Factors associated with perceived stress in Middle Eastern university students. J. Am. Coll. Health 2022, 70, 2462–2469. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Berg-Beckhoff, G. Nutritional Correlates of Perceived Stress among University Students in Egypt. Int. J. Environ. Res. Public Health 2015, 12, 14164–14176. [Google Scholar] [CrossRef]
- Chacón-Cuberos, R.; Zurita-Ortega, F.; Olmedo-Moreno, E.M.; Castro-Sánchez, M. Relationship between Academic Stress, Physical Activity and Diet in University Students of Education. Behav. Sci. 2019, 9, 59. [Google Scholar] [CrossRef]
- Abdallah, A.R.; Gabr, H.M. Depression, anxiety and stress among first year medical students in an Egyptian public university. Int. J. Res. Med. Sci. 2014, 2, 11–19. [Google Scholar]
- Naja, F.; Hasan, H.; Khadem, S.H.; Buanq, M.A.; Al-Mulla, H.K.; Aljassmi, A.K.; Faris, M.E. Adherence to the Mediterranean diet and its association with sleep quality and chronotype among youth: A cross-sectional study. Front. Nutr. 2022, 8, 805955. [Google Scholar] [CrossRef]
- Fallah, M.; Aminianfar, A.; Esmaillzadeh, A. Mediterranean diet adherence and sleep pattern: A systematic review of observational studies. BMC Nutr. 2024, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- El-Ali, Z.; Hebert, J.R.; Wirth, M.D.; Mitri, R. Association between the dietary inflammatory index and sleep quality among Lebanese university students. Sleep Sci. 2024, 17, e235–e243. [Google Scholar] [CrossRef]
- Arab, A.; Lempesis, I.G.; Garaulet, M.; Scheer, F.A.J.L. Sleep and the Mediterranean diet: A systematic review and meta-analysis. Sleep Med. Rev. 2025, 80, 102071. [Google Scholar] [CrossRef]
- Patel, A.; Cheung, J. The effect of mediterranean diet and chrononutrition on sleep quality: A scoping review. Nutr. J. 2025, 24, 31. [Google Scholar] [CrossRef] [PubMed]
- Różańska, D. The Mediterranean diet, the DASH diet, and the MIND diet in relation to sleep duration and quality: A narrative review. Nutrients 2024, 16, 4191. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fan, H.; Ren, Z.; Liu, X.; Niu, X. Sleep disorder, Mediterranean diet, and all-cause and cause-specific mortality: A prospective cohort study. BMC Public Health 2023, 23, 904. [Google Scholar] [CrossRef]
- Deligiannidou, G.E.; Philippou, E.; Vasiari, E.; de Andrade, V.L.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Jorge, R.; Dimitrova, D.; Ruskovska, T.; et al. Exploring the Relationship between Mediterranean Diet Adherence and Subjective Well-Being among Greek and Cypriot Adults. Nutrients 2024, 16, 1238. [Google Scholar] [CrossRef]
- López-Gil, J.F.; García-Hermoso, A. Adherence to the Mediterranean diet and subjective well-being among Chilean children. Appetite 2022, 172, 105974. [Google Scholar] [CrossRef]
- Andrade, V.; Jorge, R.; García-Conesa, M.T.; Philippou, E.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Maksimova, V.; Smilkov, K.; Ackova, D.G.; et al. Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients 2020, 12, 3837. [Google Scholar] [CrossRef]
- Mateo-Orcajada, A.; Abenza-Cano, L.; Molina-Morote, J.M.; Vaquero-Cristóbal, R. The influence of physical activity, adherence to Mediterranean diet, and weight status on the psychological well-being of adolescents. BMC Psychol. 2024, 12, 410. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics (n = 5433) | MD Adherence | |||
|---|---|---|---|---|
| Low 2589 (47.6%) | Moderate 1873 (34.5%) | High 971 (17.9%) | p-Value | |
| Age (mean ± SD; years) | 21.5 ± 2.5 | 21.3 ± 2.4 | 21.2 ± 2.3 | p = 0.2674 |
| Gender (n, %) | p = 0.0001 | |||
| Male | 1367 (52.8%) | 926 (49.4%) | 383 (39.4%) | |
| Female | 1222 (47.2%) | 947 (50.6%) | 588 (60.6%) | |
| Nationality (n, %) | p = 0.0832 | |||
| Greek | 2069 (79.9%) | 1578 (84.3%) | 696 (71.7%) | |
| Other | 520 (20.1%) | 295 (15.7%) | 275 (28.3%) | |
| Type of residence (n, %) | p < 0.0001 | |||
| Urban | 1811 (70.0%) | 1192 (63.6%) | 330 (34.0%) | |
| Rural | 778 (30.0%) | 680 (36.4%) | 641 (66.0%) | |
| Family economic status | p = 0.1582 | |||
| Low | 1434 (55.4%) | 577 (30.8%) | 360 (37.1%) | |
| Medium | 715 (27.6%) | 920 (49.1%) | 383 (39.4%) | |
| High | 440 (17.0%) | 376 (20.1%) | 228 (23.5%) | |
| Living status (n, %) | p < 0.0001 | |||
| Living with family | 916 (35.4%) | 1226 (65.5%) | 779 (80.2%) | |
| Living alone | 1673 (64.2%) | 647 (34.5%) | 192 (19.8%) | |
| Parents marital status | p < 0.0001 | |||
| Not divorced | 1510 (58.3%) | 1312 (70.0%) | 783 (80.6%) | |
| Divorced | 1079 (41.7%) | 561 (30.0%) | 188 (19.4%) | |
| Smoking status | p < 0.0001 | |||
| Non-smokers | 1221 (47.2%) | 1323 (70.6%) | 748 (77.0%) | |
| Regular smokers | 1368 (52.8%) | 550 (29.4%) | 223 (23.0%) | |
| Type of Studies | p = 0.0001 | |||
| Biomedical studies | 818 (31.6%) | 976 (52.1%) | 600 (61.8%) | |
| Other studies | 1771 (68.4%) | 897 (47.9%) | 371 (38.2%) | |
| Academic performance | p = 0.0052 | |||
| Good | 1545 (60.0%) | 449 (24.0%) | 249 (25.6%) | |
| Very good | 841 (32.5%) | 1023 (54.6%) | 181 (18.7%) | |
| Excellent | 203 (7.8%) | 401 (21.4%) | 541 (55.7%) | |
| Employment status | p = 0.0287 | |||
| Not employee | 1682 (65.0%) | 1375 (73.1%) | 630 (67.3%) | |
| Employee | 907 (35.0%) | 498 (26.6%) | 269 (27.7%) | |
| Physical activity (n, %) | p = 0.0045 | |||
| Low | 2038 (78.7%) | 346 (18.5%) | 183 (18.8%) | |
| Medium | 397 (15.3%) | 1318 (70.4%) | 124 (13.8%) | |
| High | 154 (6.0%) | 209 (11.2%) | 664 (68.4%) | |
| BMI (n, %) | p < 0.0001 | |||
| Normal weight | 2033 (78.5%) | 1416 (75.6%) | 619 (63.8%) | |
| Overweight | 337 (13.0%) | 325 (17.3%) | 180 (18.5%) | |
| Obese | 219 (8.5%) | 132 (7.1%) | 172 (17.7%) | |
| Perceived stress (n, %) | p < 0.0001 | |||
| Low | 1444 (57.4%) | 629 (33.6%) | 196 (20.2%) | |
| Moderate | 706 (27.3%) | 1012 (54.0%) | 673 (69.3%) | |
| High | 395 (15.3%) | 232 (12.4%) | 102 (10.5%) | |
| Sleep Quality (n, %) | p < 0.0001 | |||
| Adequate | 1530 (59.1%) | 1471 (78.5%) | 768 (79.1%) | |
| Inadequate | 1059 (40.9%) | 402 (21.5%) | 203 (20.9%) | |
| Characteristics | MD Adherence (Low vs. Moderate and High) | |
|---|---|---|
| OR * (95% CI **) | p-Value | |
| Age (Over/Below mean value) | 1.12 (0.21–2.23) | p = 0.4918 |
| Gender (Male/Female) | 0.70 (0.59–0.95) | p = 0.0022 |
| Nationality (Greek/Other) | 1.12 (0.32–1.91) | p = 0.5032 |
| Type of residence (Urban/Rural) | 0.81 (0.62–1.01) | p = 0.0091 |
| Family economic status (Low/Medium and High) | 0.85 (0.31–1.43) | p = 0.2019 |
| Living status (Living alone/Living with family) | 0.73 (0.62–0.90) | p = 0.0092 |
| Parents marital status (Divorced/No divorced) | 0.98 (0.29–1.78) | p = 0.3419 |
| Smoking status (Regular smokers/No smokers) | 1.15 (0.93–1.26) | p = 0.0005 |
| Type of Studies (Biomedical studies/Other studies) | 0.78 (0.59–0.97) | p = 0.0188 |
| Academic performance (Good/Very good and Excellent) | 0.88 (0.31–1.39) | p = 0.0809 |
| Employment status (Employee/No employee) | 1.13 (0.56–1.98) | p = 0.4019 |
| BMI (Overweight and obese/Normal weight) | 2.07 (1.92–2.25) | p = 0.0076 |
| Physical activity (Low/Medium and High) | 1.73 (1.58–1.97) | p = 0.0081 |
| Perceived stress (Moderate and High/Low) | 2.21 (1.99–2.47) | p = 0.0037 |
| Sleep Quality (Inadequate/Adequate) | 2.32 (2.09–2.54) | p = 0.0028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dakanalis, A.; Papadimitriou, K.; Alexatou, O.; Deligiannidou, G.-E.; Pappa, M.; Papadopoulou, S.K.; Louka, A.; Paschodimas, G.; Mentzelou, M.; Giaginis, C. Mediterranean Diet Compliance Is Related with Lower Prevalence of Perceived Stress and Poor Sleep Quality in University Students: A Cross-Sectional Study in Greece. Nutrients 2025, 17, 2174. https://doi.org/10.3390/nu17132174
Dakanalis A, Papadimitriou K, Alexatou O, Deligiannidou G-E, Pappa M, Papadopoulou SK, Louka A, Paschodimas G, Mentzelou M, Giaginis C. Mediterranean Diet Compliance Is Related with Lower Prevalence of Perceived Stress and Poor Sleep Quality in University Students: A Cross-Sectional Study in Greece. Nutrients. 2025; 17(13):2174. https://doi.org/10.3390/nu17132174
Chicago/Turabian StyleDakanalis, Antonios, Konstantinos Papadimitriou, Olga Alexatou, Georgia-Eirini Deligiannidou, Myrsini Pappa, Sousana K. Papadopoulou, Aikaterini Louka, Georgios Paschodimas, Maria Mentzelou, and Constantinos Giaginis. 2025. "Mediterranean Diet Compliance Is Related with Lower Prevalence of Perceived Stress and Poor Sleep Quality in University Students: A Cross-Sectional Study in Greece" Nutrients 17, no. 13: 2174. https://doi.org/10.3390/nu17132174
APA StyleDakanalis, A., Papadimitriou, K., Alexatou, O., Deligiannidou, G.-E., Pappa, M., Papadopoulou, S. K., Louka, A., Paschodimas, G., Mentzelou, M., & Giaginis, C. (2025). Mediterranean Diet Compliance Is Related with Lower Prevalence of Perceived Stress and Poor Sleep Quality in University Students: A Cross-Sectional Study in Greece. Nutrients, 17(13), 2174. https://doi.org/10.3390/nu17132174