
Decoding Health Professionals’ Attitudes and Perceptions Towards Plant-Based Nutrition: A Narrative Review



Abstract
1. Introduction
1.1. Plant-Based Diets
1.2. Benefits of Plant-Based Diets
1.3. Theoretical Domains Framework (TDF)
2. Materials and Methods
2.1. Research Question
2.2. Literature Search
2.3. Eligibility Criteria
2.4. Data Profiling and Synthesis of Results
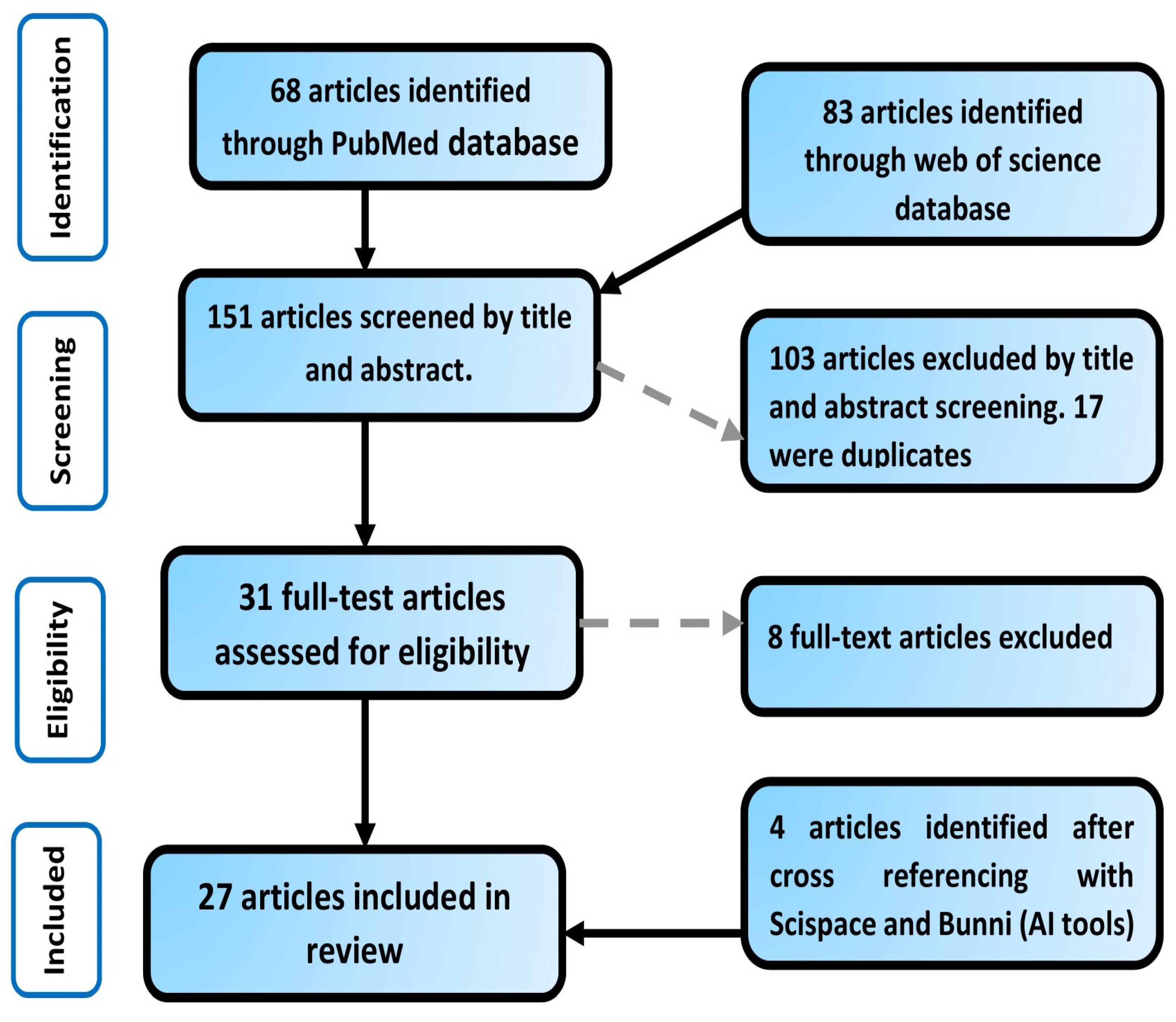
2.5. Article Search and Selection
3. Results
3.1. General Overview of Included Studies
3.2. General Overview of Health Professionals’ Attitudes and Perceptions
3.3. Factors Influencing Health Professionals’ Attitudes and Perceptions Towards Plant-Based Diets
3.3.1. Knowledge
3.3.2. Education and Training
3.3.3. Evidence-Based Guidelines
3.3.4. Multidisciplinary Collaboration
3.3.5. Personal Experience and Interest
3.3.6. Educational Resources
3.3.7. Lack of Time
3.3.8. Safety and Compliance Challenges
3.3.9. Lack of Confidence in Patient Capabilities
4. Subgroup Analysis of Barriers and Enablers by Professional Category
5. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PBD | Plant-based diet |
| TDF | Theoretical Domains Framework |
| NIH | National Institute of Health |
| CDC | Center for Disease Control and Prevention |
| FAO | Food and Agriculture Organization |
| AICR | American Institute for Cancer Research |
| DASH | Dietary Approaches to Stop Hypertension |
| MD | Mediterranean diet |
References
- Regestein, Q.R. The big, bad obesity pandemic. Menopause 2018, 25, 129–132. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health [NIH]. Available online: https://www.niddk.nih.gov/health-information/health-statistics/overweight-obesity (accessed on 1 February 2024).
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- Helmchen, L.A.; Henderson, R.M. Changes in the distribution of body mass index of white US men, 1890–2000. Ann. Hum. Biol. 2004, 31, 174–181. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Health, United States, 2021: Data Brief [No. 456]. 2023. Available online: https://www.cdc.gov/nchs/products/databriefs/db456.htm (accessed on 1 February 2024).
- Ward, Z.J.; Bleich, S.N.; Long, M.W.; Gortmaker, S.L. Association of body mass index with health care expenditures in the United States by age and sex. PLoS ONE 2021, 16, e0247307. [Google Scholar] [CrossRef]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Meldrum, D.R.; Morris, M.A.; Gambone, J.C. Obesity pandemic: Causes, consequences, and solutions-but do we have the will? Fertil. Steril. 2017, 107, 833–839. [Google Scholar] [CrossRef]
- World Cancer Research Fund. Summary of the Third Expert Report: Diet, Nutrition, Physical Activity and Cancer. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 1 February 2024).
- Romanello, M.; Di Napoli, C.; Drummond, P.; Green, C.; Kennard, H.; Lampard, P.; Scamman, D.; Arnell, N.; Ayeb-Karlsson, S.; Ford, L.B.; et al. The 2022 report of the Lancet Countdown on health and climate change: Health at the mercy of fossil fuels. Lancet 2022, 400, 1619–1654. [Google Scholar] [CrossRef]
- Viroli, G.; Kalmpourtzidou, A.; Cena, H. Exploring Benefits and Barriers of Plant-Based Diets: Health, Environmental Impact, Food Accessibility and Acceptability. Nutrients 2023, 15, 4723. [Google Scholar] [CrossRef]
- Searchinger, T.; Waite, R.; Hanson, C.; Ranganathan, J.; Dumas, P.; Matthews, E.; Klirs, C. Creating a Sustainable Food Future: A Menu of Solutions to Feed Nearly 10 Billion People by 2050. Final Report. 2019. Available online: https://research.wri.org/sites/default/files/2019-07/creating-sustainable-food-future_2_5.pdf (accessed on 1 February 2024).
- The Rockefeller Foundation. Available online: https://www.rockefellerfoundation.org/report/true-cost-of-food-measuring-what-matters-to-transform-the-u-s-food-system/ (accessed on 28 March 2024).
- Food and Agriculture Organization. The State of Food and Agriculture 2021: A Report on the Future of Food. 2021. Available online: https://www.fao.org/3/ca6640en/ca6640en.pdf (accessed on 28 March 2024).
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6, e000534. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Nishi, S.K.; Khan, T.A.; Braunstein, C.R.; Glenn, A.J.; Mejia, S.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Jenkins, D.J.A.; et al. Portfolio Dietary Pattern and Cardiovascular Disease: A Systematic Review and Meta-analysis of Controlled Trials. Prog. Cardiovasc. Dis. 2018, 61, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association Between Plant-Based Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2019, 179, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. FastStats: Deaths. Available online: https://www.cdc.gov/nchs/fastats/deaths.htm (accessed on 1 February 2024).
- Springmann, M.; Wiebe, K.; Mason-D’Croz, D.; Sulser, T.B.; Rayner, M.; Scarborough, P. Health and nutritional aspects of sustainable diet strategies and their association with environmental impacts: A global modelling analysis with country-level detail. Lancet Planet. Health 2018, 2, e451–e461. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Drewnowski, A.; Finley, J.; Hess, J.M.; Ingram, J.; Miller, G.; Peters, C. Toward Healthy Diets from Sustainable Food Systems. Curr. Dev. Nutr. 2020, 4, nzaa083. [Google Scholar] [CrossRef]
- Kraak, V.I.; Consavage Stanley, K. An economic lens for sustainable dietary guidelines. Lancet Planet. Health 2023, 7, e350–e351. [Google Scholar] [CrossRef]
- Consavage Stanley, K.; Hedrick, V.E.; Serrano, E.; Holz, A.; Kraak, V.I. US Adults’ Perceptions, Beliefs, and Behaviors towards Plant-Rich Dietary Patterns and Practices: International Food Information Council Food and Health Survey Insights, 2012–2022. Nutrients 2023, 15, 4990. [Google Scholar] [CrossRef]
- Koutras, Y.; Chrysostomou, S.; Poulimeneas, D.; Yannakoulia, M. Examining the associations between a posteriori dietary patterns and obesity indexes: Systematic review of observational studies. Nutr. Health 2022, 28, 149–162. [Google Scholar] [CrossRef]
- Spencer, E.A.; Appleby, P.N.; Davey, G.K.; Key, T.J. Diet and body mass index in 38000 EPIC-Oxford meat-eaters, fish-eaters, vegetarians and vegans. Int. J. Obes. 2003, 27, 728–734. [Google Scholar] [CrossRef]
- Jarvis, S.E.; Nguyen, M.; Malik, V.S. Association between adherence to plant-based dietary patterns and obesity risk: A systematic review of prospective cohort studies. Appl. Physiol. Nutr. Metab. 2022, 47, 1115–1133. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.Y.; Huang, C.C.; Hu, F.B.; Chavarro, J.E. Vegetarian Diets and Weight Reduction: A Meta-Analysis of Randomized Controlled Trials. J. Gen. Intern. Med. 2016, 31, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Klementova, M.; Thieme, L.; Haluzik, M.; Pavlovicova, R.; Hill, M.; Pelikanova, T.; Kahleova, H. A Plant-Based Meal Increases Gastrointestinal Hormones and Satiety More Than an Energy- and Macronutrient-Matched Processed-Meat Meal in T2D, Obese, and Healthy Men: A Three-Group Randomized Crossover Study. Nutrients 2019, 11, 157. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- Craig, W.J.; Mangels, A.R. American Dietetic Association Position of the American Dietetic Association: Vegetarian diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef]
- American Institute for Cancer Research. What Is a Plant-Based Diet? AICR’s Take. 2023. Available online: https://www.aicr.org/resources/blog/what-is-a-plant-based-diet-aicrs-take/ (accessed on 1 February 2024).
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. 2020–2025 Dietary Guidelines for Americans. 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed on 1 February 2024).
- Nielsen. Plant-Based Food Options Are Sprouting: Growth for Retailers. 2018. Available online: https://www.nielsen.com/us/en/insights/article/2018/plant-based-food-options-are-sprouting-growth-for-retailers/ (accessed on 1 February 2024).
- Reinhart, R. Snapshot: Few Americans Are Vegetarian or Vegan. Gallup. 2019. Available online: https://news.gallup.com/poll/238328/snapshot-few-americans-vegetarian-vegan.aspx (accessed on 1 February 2024).
- Lee, V.; McKay, T.; Ardern, C.I. Awareness and perception of plant-based diets for the treatment and management of type 2 diabetes in a community education clinic: A pilot study. J. Nutr. Metab. 2015, 2015, 236234. [Google Scholar] [CrossRef]
- Lea, E.J.; Crawford, D.; Worsley, A. Public views of the benefits and barriers to the consumption of a plant-based diet. Eur. J. Clin. Nutr. 2006, 60, 828–837. [Google Scholar] [CrossRef]
- Morton, K.F.; Pantalos, D.C.; Ziegler, C.; Patel, P.D. Whole-Foods, Plant-Based Diet Perceptions of Medical Trainees Compared to Their Patients: A Cross-Sectional Pilot Study. Am. J. Lifestyle Med. 2021, 16, 318–333. [Google Scholar] [CrossRef]
- Willet, W.C.; Stampfer, M.J. Current evidence on healthy eating. Annu. Rev. Public Health 2013, 34, 77–95. [Google Scholar] [CrossRef]
- Kent, G.; Kehoe, L.; Flynn, A.; Walton, J. Plant-based diets: A review of the definitions and nutritional role in the adult diet. Proc. Nutr. Soc. 2022, 81, 62–74. [Google Scholar] [CrossRef]
- Laine, J.E.; Huybrechts, I.; Gunter, M.J.; Ferrari, P.; Weiderpass, E.; Tsilidis, K.; Aune, D.; Schulze, M.B.; Bergmann, M.; Temme, E.H.M.; et al. Co-benefits from sustainable dietary shifts for population and environmental health: An assessment from a large European cohort study. Lancet Planet. Health 2021, 5, e786–e796. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension [DASH] diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ Clin. Res. Ed. 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Marczak, L.; O’Rourke, K.; Shepard, D. When and why people die in the United States, 1990–2013. Jama 2016, 315, 241. [Google Scholar] [CrossRef]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10 (Suppl. S4), S275–S283. [Google Scholar] [CrossRef]
- Springmann, M.; Godfray, H.C.; Rayner, M.; Scarborough, P. Analysis and valuation of the health and climate change cobenefits of dietary change. Proc. Natl. Acad. Sci. USA 2016, 113, 4146–4151. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A.; “Psychological Theory” Group. Making psychological theory useful for implementing evidence based practice: A consensus approach. Qual. Saf. Health Care 2005, 14, 26–33. [Google Scholar] [CrossRef]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef]
- French, S.D.; Green, S.E.; O’Connor, D.A.; McKenzie, J.E.; Francis, J.J.; Michie, S.; Buchbinder, R.; Schattner, P.; Spike, N.; Grimshaw, J.M. Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implement. Sci. 2012, 7, 38. [Google Scholar] [CrossRef]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- SciSpace. Chat with PDF. SciSpace. 18 April 2024. Available online: https://scispace.com/chat-pdf (accessed on 16 June 2024).
- Bunni AI. Bunni: Chat to Your PDF Documents—Summarize and Ask Questions. 18 April 2024. Available online: https://bunni.ai/ (accessed on 16 June 2024).
- Stanford, J.; Zuck, M.; Stefoska-Needham, A.; Charlton, K.; Lambert, K. Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians. Nutrients 2022, 14, 216. [Google Scholar] [CrossRef]
- Hughes, G.J.; Kress, K.S.; Armbrecht, E.S.; Mukherjea, R.; Mattfeldt-Beman, M. Initial investigation of dietitian perception of plant-based protein quality. Food Sci. Nutr. 2014, 2, 371–379. [Google Scholar] [CrossRef]
- Moutou, K.E.; England, C.; Gutteridge, C.; Toumpakari, Z.; McArdle, P.D.; Papadaki, A. Exploring dietitians’ practice and views of giving advice on dietary patterns to patients with type 2 diabetes mellitus: A qualitative study. J. Hum. Nutr. Diet. 2022, 35, 179–190. [Google Scholar] [CrossRef]
- Hawkins, I.W.; Mangels, A.R.; Goldman, R.; Wood, R.J. Dietetics Program Directors in the United States Support Teaching Vegetarian and Vegan Nutrition and Half Connect Vegetarian and Vegan Diets to Environmental Impact. Front. Nutr. 2019, 6, 123. [Google Scholar] [CrossRef]
- Mayr, H.L.; Kostjasyn, S.P.; Campbell, K.L.; Palmer, M.; Hickman, I.J. Investigating Whether the Mediterranean Dietary Pattern Is Integrated in Routine Dietetic Practice for Management of Chronic Conditions: A National Survey of Dietitians. Nutrients 2020, 12, 3395. [Google Scholar] [CrossRef]
- Asher, K.E.; Doucet, S.; Luke, A. Registered dietitians’ perceptions and use of the plant-based recommendations in the 2019 Canada’s Food Guide. J. Hum. Nutr. Diet. 2021, 34, 715–723. [Google Scholar] [CrossRef]
- Saintila, J.; Calizaya-Milla, Y.E.; Javier-Aliaga, D.J. Knowledge of Vegetarian and Nonvegetarian Peruvian Dietitians about Vegetarianism at Different Stages of Life. Nutr. Metab. Insights 2021, 14, 1178638821997123. [Google Scholar] [CrossRef]
- Janse Van Rensburg, L.M.; Wiles, N.L. The opinion of KwaZulu-Natal dietitians regarding the use of a whole-foods plant-based diet in the management of non-communicable diseases. South Afr. J. Clin. Nutr. 2021, 34, 60–64. [Google Scholar] [CrossRef]
- Duncan, K.H.; Bergman, E. Knowledge and attitudes of registered dietitians concerning vegetarian diets. Nutr. Res. 1999, 19, 1741–1748. [Google Scholar] [CrossRef]
- Betz, M.V.; Nemec, K.B.; Zisman, A.L. Plant-based Diets in Kidney Disease: Nephrology Professionals’ Perspective. J. Ren. Nutr. 2022, 32, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Fuller, S.J.; Hill, K.M. Attitudes toward veganism in eating disorder professionals. BJPsych Bull. 2022, 46, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Bettinelli, M.E.; Bezze, E.; Morasca, L.; Plevani, L.; Sorrentino, G.; Morniroli, D.; Giannì, M.L.; Mosca, F. Knowledge of Health Professionals Regarding Vegetarian Diets from Pregnancy to Adolescence: An Observational Study. Nutrients 2019, 11, 1149. [Google Scholar] [CrossRef]
- Mayr, H.L.; Kelly, J.T.; Macdonald, G.A.; Russell, A.W.; Hickman, I.J. Clinician Perspectives of Barriers and Enablers to Implementing the Mediterranean Dietary Pattern in Routine Care for Coronary Heart Disease and Type 2 Diabetes: A Qualitative Interview Study. J. Acad. Nutr. Diet. 2022, 122, 1263–1282. [Google Scholar] [CrossRef]
- Meulenbroeks, D.; Versmissen, I.; Prins, N.; Jonkers, D.; Gubbels, J.; Scheepers, H. Care by Midwives, Obstetricians, and Dietitians for Pregnant Women Following a Strict Plant-Based Diet: A Cross-Sectional Study. Nutrients 2021, 13, 2394. [Google Scholar] [CrossRef]
- Mayr, H.L.; Kelly, J.T.; Macdonald, G.A.; Hickman, I.J. ‘Focus on diet quality’: A qualitative study of clinicians’ perspectives of use of the Mediterranean dietary pattern for non-alcoholic fatty liver disease. Br. J. Nutr. 2022, 128, 1220–1230. [Google Scholar] [CrossRef]
- Albertelli, T.; Carretier, E.; Loisel, A.; Moro, M.R.; Blanchet, C. Vegetarianism and eating disorders: The subjective experience of healthcare professionals. Appetite 2024, 193, 107136. [Google Scholar] [CrossRef]
- McHugh, P.; Smith, M.; Wright, N.; Bush, S.; Pullon, S. If You Don’t Eat Meat… You’ll Die. A Mixed-Method Survey of Health-Professionals’ Beliefs. Nutrients 2019, 11, 3028. [Google Scholar] [CrossRef]
- Olfert, M.D.; Wattick, R.A.; Hagedorn, R.L. Experiential Application of a Culinary Medicine Cultural Immersion Program for Health Professionals. J. Med. Educ. Curric. Dev. 2020, 7, 2382120520927396. [Google Scholar] [CrossRef]
- Hamiel, U.; Landau, N.; Eshel Fuhrer, A.; Shalem, T.; Goldman, M. The Knowledge and Attitudes of Pediatricians in Israel Towards Vegetarianism. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Lessem, A.; Gould, S.M.; Evans, J.; Dunemn, K. A whole-food plant-based experiential education program for health care providers results in personal and professional changes. J. Am. Assoc. Nurse Pract. 2020, 32, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Sentenach-Carbo, A.; Batlle, C.; Franquesa, M.; García-Fernandez, E.; Rico, L.; Shamirian-Pulido, L.; Pérez, M.; Deu-Valenzuela, E.; Ardite, E.; Funtikova, A.N.; et al. Adherence Of Spanish Primary Physicians And Clinical Practise To The Mediterranean Diet. Eur. J. Clin. Nutr. 2019, 72 (Suppl. S1), 92–98. [Google Scholar] [CrossRef]
- Estell, M.; Hughes, J.; Grafenauer, S. Plant protein and plant-based meat alternatives: Consumer and nutrition professional attitudes and perceptions. Sustainability 2021, 13, 1478. [Google Scholar] [CrossRef]
- Aggarwal, M.; Singh Ospina, N.; Kazory, A.; Joseph, I.; Zaidi, Z.; Ataya, A.; Agito, M.; Bubb, M.; Hahn, P.; Sattari, M. The Mismatch of Nutrition and Lifestyle Beliefs and Actions Among Physicians: A Wake-Up Call. Am. J. Lifestyle Med. 2019, 14, 304–315. [Google Scholar] [CrossRef]
- Fresán, U.; Vidal-Carou, M.C.; Ramos-Truchero, G.; de Pipaon, M.S.; Moreno, L.A.; Salas-Salvadó, J. Knowledge, attitude, and patient advice on sustainable diets among Spanish health professionals. Front. Nutr. 2023, 10, 1182226. [Google Scholar] [CrossRef]
- Krause, A.J.; Williams, K.A., Sr. Understanding and Adopting Plant-Based Nutrition: A Survey of Medical Providers. Am. J. Lifestyle Med. 2017, 13, 312–318. [Google Scholar] [CrossRef]
- Harkin, N.; Johnston, E.; Mathews, T.; Guo, Y.; Schwartzbard, A.; Berger, J.; Gianos, E. Physicians’ Dietary Knowledge, Attitudes, and Counseling Practices: The Experience of a Single Health Care Center at Changing the Landscape for Dietary Education. Am. J. Lifestyle Med. 2018, 13, 292–300. [Google Scholar] [CrossRef]
- Boocock, R.C.; Lake, A.A.; Haste, A.; Moore, H.J. Clinicians’ perceived barriers and enablers to the dietary management of adults with type 2 diabetes in primary care: A systematic review. J. Hum. Nutr. Diet. 2021, 34, 1042–1052. [Google Scholar] [CrossRef]
- Williams, B.; Perillo, S.; Brown, T. What are the factors of organizational culture in health care settings that act as barriers to the implementation of evidence-based practice? A scoping review. Nurse Educ. Today 2015, 35, e34–e41. [Google Scholar] [CrossRef]
- Gray, M.; Joy, E.; Plath, D.; Webb, S.A. Implementing evidence-based practice: A review of the empirical research literature. Res. Soc. Work. Pract. 2013, 23, 157–166. [Google Scholar] [CrossRef]
- Soguel, L.; Vaucher, C.; Bengough, T.; Burnand, B.; Desroches, S. Knowledge Translation and Evidence-Based Practice: A Qualitative Study on Clinical Dietitians’ Perceptions and Practices in Switzerland. J. Acad. Nutr. Diet. 2019, 119, 1882–1889. [Google Scholar] [CrossRef] [PubMed]
- Byham-Gray, L.D.; Gilbride, J.A.; Dixon, L.B.; Stage, F.K. Evidence-based practice: What are dietitians’ perceptions, attitudes, and knowledge? J. Am. Diet. Assoc. 2005, 105, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Gianfrancesco, C.; Johnson, M. Exploring the provision of diabetes nutrition education by practice nurses in primary care settings. J. Hum. Nutr. Diet. 2020, 33, 263–273. [Google Scholar] [CrossRef]
- Smeets, R.G.M.; Kroese, M.E.A.L.; Ruwaard, D.; Hameleers, N.; Elissen, A.M.J. Person-centred and efficient care delivery for high-need, high-cost patients: Primary care professionals’ experiences. BMC Fam. Pract. 2020, 21, 106. [Google Scholar] [CrossRef]
- Frank, E.; Wright, E.H.; Serdula, M.K.; Elon, L.K.; Baldwin, G. Personal and professional nutrition-related practices of US female physicians. Am. J. Clin. Nutr. 2002, 75, 326–332. [Google Scholar] [CrossRef]
- Landry, M.J.; Ward, C.P.; Koh, L.M.; Gardner, C.D. The knowledge, attitudes, and perceptions towards a plant-based dietary pattern: A survey of obstetrician-gynecologists. Front. Nutr. 2024, 11, 1381132. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Lea, E.; Worsley, A. Benefits and barriers to the consumption of a vegetarian diet in Australia. Public Health Nutr. 2003, 6, 505–511. [Google Scholar] [CrossRef]
- Lea, E.; Worsley, A. The factors associated with the belief that vegetarian diets provide health benefits. Asia Pac. J. Clin. Nutr. 2003, 12, 296–303. [Google Scholar]
- Fehér, A.; Gazdecki, M.; Véha, M.; Szakály, M.; Szakály, Z. A Comprehensive Review of the Benefits of and the Barriers to the Switch to a Plant-Based Diet. Sustainability 2020, 12, 4136. [Google Scholar] [CrossRef]
- Graça, J.; Oliveira, A.; Calheiros, M.M. Meat, beyond the plate. Data-driven hypotheses for understanding consumer willingness to adopt a more plant-based diet. Appetite 2015, 90, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Mullee, A.; Vermeire, L.; Vanaelst, B.; Mullie, P.; Deriemaeker, P.; Leenaert, T.; De Henauw, S.; Dunne, A.; Gunter, M.J.; Clarys, P.; et al. Vegetarianism and meat consumption: A comparison of attitudes and beliefs between vegetarian, semi-vegetarian, and omnivorous subjects in Belgium. Appetite 2017, 114, 299–305. [Google Scholar] [CrossRef]
- Springmann, M.; Clark, M.; Mason-D’Croz, D.; Wiebe, K.; Bodirsky, B.L.; Lassaletta, L.; de Vries, W.; Vermeulen, S.J.; Herrero, M.; Carlson, K.M.; et al. Options for keeping the food system within environmental limits. Nature 2018, 562, 519–525. [Google Scholar] [CrossRef]
- Fresán, U.; Sabaté, J. Vegetarian Diets: Planetary Health and Its Alignment with Human Health. Adv. Nutr. 2019, 10 (Suppl. S4), S380–S388. [Google Scholar] [CrossRef]
- Hallström, E.; Carlsson-Kanyama, A.; Börjesson, P. Environmental impact of dietary change: A systematic review. J. Clean. Prod. 2015, 91, 1–11. [Google Scholar] [CrossRef]
- Vanham, D.; Hoekstra, A.Y.; Bidoglio, G. Potential water saving through changes in European diets. Environ. Int. 2013, 61, 45–56. [Google Scholar] [CrossRef]
- Catapan, S.C.; Nair, U.; Gray, L.; Cristina Marino Calvo, M.; Bird, D.; Janda, M.; Fatehi, F.; Menon, A.; Russell, A. Same goals, different challenges: A systematic review of perspectives of people with diabetes and healthcare professionals on Type 2 diabetes care. Diabet. Med. 2021, 38, e14625. [Google Scholar] [CrossRef]
- American College of Lifestyle Medicine. The Benefits of Plant-Based Nutrition. Available online: https://lifestylemedicine.org/articles/benefits-plant-based-nutrition/ (accessed on 16 June 2025).
- Tuso, P.J.; Ismail, M.H.; Ha, B.P.; Bartolotto, C. Nutritional update for physicians: Plant-based diets. Perm. J. 2013, 17, 61–66. [Google Scholar] [CrossRef]
- Kaiser Permanente. The Plant-Based Diet: A Healthier Way to Eat. Available online: https://healthy.kaiserpermanente.org/content/dam/kporg/final/documents/health-education-materials/instructions/plant-based-diet-hi-en.pdf (accessed on 16 June 2025).
- Physicians Committee for Responsible Medicine (PCRM). Available online: https://www.pcrm.org (accessed on 16 June 2025).
- Moreno, L.A.; Meyer, R.; Donovan, S.M.; Goulet, O.; Haines, J.; Kok, F.J.; Van’t Veer, P. Perspective: Striking a Balance between Planetary and Human Health-Is There a Path Forward? Adv. Nutr. 2022, 13, 355–375. [Google Scholar] [CrossRef]
- Folkvord, F.; Anschütz, D.; Geurts, M. Watching TV Cooking Programs: Effects on Actual Food Intake among Children. J. Nutr. Educ. Behav. 2020, 52, 3–9, Erratum in J. Nutr. Educ. Behav. 2023, 55, 165. [Google Scholar] [CrossRef] [PubMed]
- Pierce, B.; Bowden, B.; McCullagh, M.; Diehl, A.; Chissell, Z.; Rodriguez, R.; Berman, B.M.; D’Adamo, C.R. A Summer Health Program for African American High School Students in Baltimore, Maryland: Community Partnership for Integrative Health. Explore 2017, 13, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Onwezen, M.C.; Bouwman, E.P.; Reinders, M.J.; Dagevos, H. A systematic review on consumer acceptance of alternative proteins: Pulses, algae, insects, plant-based meat alternatives, and cultured meat. Appetite 2021, 159, 105058. [Google Scholar] [CrossRef] [PubMed]
- Orsini, F.; Gasperi, D.; Marchetti, L.; Piovene, C.; Draghetti, S.; Ramazzotti, S.; Bazzocchi, G.G.; Gianquinto, G. Exploring the production capacity of rooftop gardens [RTGs] in urban agriculture: The potential impact on food and nutrition security, biodiversity and other ecosystem services in the city of Bologna. Food Secur. 2014, 6, 781–792. [Google Scholar] [CrossRef]
- Davies, A.R. Toward a Sustainable Food System for the European Union: Insights from the Social Sciences. One Earth 2020, 3, 27–31. [Google Scholar] [CrossRef]

{kind=link}
| Dietary Pattern | Foods |
|---|---|
| Lacto-vegetarian diet | Includes dairy |
| Ovo-vegetarian diet | Includes eggs |
| Lacto-ovo vegetarian diet | Includes dairy and eggs |
| Pesco-vegetarian diet | Includes fish and seafood |
| Vegan diet | Excludes all meat and all animal products |
| Mediterranean diet | Based on fruits, vegetables, whole grains, legumes, moderate consumption of dairy and fish, and low consumption of meat and sweets |
| DASH diet | Based on vegetables, fruits, and whole grains; includes fat-free and low-fat dairy products, fish, poultry, beans, and nuts. |
| Author, Year | Country | Study Design | Population and Sample | Objective | Methodology | Key Findings |
|---|---|---|---|---|---|---|
| Stanford et al., 2022 [56] | Australia | Cross-sectional | N = 35 renal dietitians completed online surveys, and 11 participated in in-depth interviews | Explore perspectives of renal dietitians regarding PBDs for chronic kidney disease (CKD) management and evaluate their acceptability of a hypothetical plant-based dietary prescription | Exploratory Mixed methods: Short online questionnaire and in-depth semi-structured interview | Renal dietitians perceived PBDs as beneficial to patients with CKD. |
| Betz et al., 2022 [65] | USA | Cross-sectional | N = 382 dietitians (154 physicians, 62 nurse practitioners, 32 fellows, 13 physician assistants, and 14 other professionals) | Understand the perspectives of nephrology professionals towards the use of PBDs for the treatment of CKD | Online questionnaire based on a previous survey | Nephrology professionals believed PBDs were beneficial in the management of CKD, but dietitians were more likely to be aware of the benefits of PBDs than other professionals. |
| Fuller & Hill, 2022 [66] | UK | Cross-sectional | N = 116 specialist eating disorder professionals, 90 general mental health professionals, and 186 other professionals | Investigate attitudes of health care professionals towards veganism | Self-reported questionnaire based on general eating habits and ATvegan questionnaires | All had positive views of veganism, but general mental health professionals had more positive attitudes than eating disorder specialists and other professionals. |
| Bettinelli et al., 2019 [67] | Italy | Cross-sectional | 140 nurses,135 pediatric nurses, 60 midwives, 43 health care support workers, and 40 staff nurses | Assess knowledge of health care professionals regarding the adoption of vegetarian diets from pregnancy through adolescence | Online questionnaire developed for the study and pre-tested | Clinicians had a positive view of the Mediterranean diet (MD), though it was not routinely recommended due to limited knowledge, practice skills, and training |
| Hughes et al., 2014 [57] | USA | Cross-sectional | N = 136 dietitians, of whom 124 were registered dietitians | Assess dietitians’ perceptions of plant-based protein quality | Online questionnaire developed for the study and pre-tested | Dietitians had a positive attitude towards PBDs, but knowledge about plant-based protein quality was limited. |
| Moutou et al., 2021 [58] | UK | Cross-sectional | N = 12 registered dietitians | Explore dietitians’ views about advising on 5 dietary patterns (including MD and DASH diets) deemed effective for the management of type 2 diabetes | Semi-structured interviews with short demographic questionnaires developed for the study | Study participants considered the MD effective, but most had mixed responses about the DASH diet. |
| Mayr et al., 2022 [68] | Australia | Cross-sectional | N = 57 clinicians (21 nurses, 19 doctors, 13 dietitians, and 4 physiotherapists) | Explore multidisciplinary health care professionals’ perspectives on recommending the MD to patients with coronary heart disease and type 2 diabetes | Qualitative study with individual semi-structured interviews via telephone or face-to-face | The MD was not routinely recommended and clinicians had limited knowledge and practice skills regarding MD; barriers to recommending the MD were a lack of education and training and personal experience/interest. |
| Meulenbroeks et al., 2021 [69] | The Netherlands | Cross-sectional | N = 411 (121 midwives, 179 obstetricians, and 111 dietitians) | Evaluate self-reported knowledge and advice given by Dutch obstetric caregivers and dietitians to pregnant women following PBDs | Online questionnaire developed based on focus group interviews | Both obstetricians and midwives reported limited knowledge about strict PBDs. Only 38.7% of dietitians felt they had enough knowledge to advise pregnant women on strict PBDs. They believed that women following a strict PBD during pregnancy were at a higher risk of nutrient deficiencies. |
| Mayr et al., 2022 [70] | Australia | Cross-sectional | N = 14 (7 doctors, 3 nurses, 3 dietitians, and 1 exercise physiologist) | Assess multidisciplinary clinicians’ perspectives on whether the Mediterranean diet (MD) is recommended in routine management of non-alcoholic liver disease | Semi-structured individual phone and face-to-face interviews | The MD was seen as an evidence-based approach for enhancing diet quality, promoting weight loss, and reducing the risk of chronic co-morbidities. However, some doctors and nurses had limited knowledge of the specific literature supporting the benefits of following an MD. |
| Hawkins et al., 2019 [59] | USA | Cross- sectional | N = 205 nutrition and dietetics program directors | Investigate curricular practices in accredited dietetics programs and assess the prevalence and perceived importance of vegetarian and vegan nutrition instruction | Online questionnaire developed for the study and pre-tested | Over 90% of program directors agreed that vegetarian nutrition should be taught, while 87% agreed that vegan nutrition should be taught. Program directors in northeastern programs had higher percentages of agreement than those in southern programs. In addition, 51% and 49% of the programs teach vegetarian and vegan nutrition, respectively. |
| Albertelli et al., 2024 [71] | France | Cross- sectional | N = 18 (14 dietitians, 3 physicians specialized in nutrition, and 1 psychiatrist) | Investigate health care professionals’ subjective experience of vegetarianism in patients with eating disorders (EDs) | Qualitative study with remotely administered semi-structured interviews via videoconferences and telephone | Health professionals regarded vegetarianism as a restrictive approach and often linked it to eating disorders in patients. They were strongly opposed to veganism, citing the risk of severe nutritional deficiencies. |
| Mayr et al., 2020 [60] | Australia | Cross- sectional | N = 182 dietitians who had practiced with at least one of the relevant chronic disease patient groups | Evaluate the extent the MD is routinely recommended by dietitians to patients with chronic diseases | Online questionnaire based on TDF | Approximately 62%, 46%, and 39% of dietitians strongly agreed that there was enough evidence to support recommending MD to patients with CVD, type 2 diabetes, and non-alcoholic liver disease, respectively. Moreover, 48% strongly agreed that they were knowledgeable about the principles of MD, and 46% were confident in counseling patients about MD. |
| McHugh et al., 2019 [72] | New Zealand | Cross- sectional | N = 41 (20 doctors, 13 nurses, 7 pharmacists, and 1 osteopath) | Investigate whether health professionals have sufficient nutritional education for their roles in health education and promotion and whether their nutritional beliefs are consistent with the current literature | Mixed methods, including an online de novo questionnaire and one focus group | PBDs were generally viewed as beneficial to health but deemed complicated. Moreover, 43% of participants reported dissatisfaction with the amount of nutritional training received. |
| Olfert et al., 2020 [73] | USA | Descriptive case study | N = 29 health professionals, 15 currently practicing in cohort 1 and 14 aspiring health professionals in cohort 2 from various disciplines | Determine the effectiveness of culinary medicine and MD to enhance the nutritional knowledge, attitudes, and self-efficacy of current and aspiring (student) health professionals | Online questionnaire developed but influenced by evidence-based sources | At baseline, cohort 2 had higher attitude and knowledge scores. There was no significant difference in mean self-efficacy scores or mean MD adherence scores. |
| Hamiel et al., 2020 [74] | Israel | Cross- sectional | N = 270 pediatricians, 14.1% were following a vegetarian diet | Assess the knowledge and attitudes of pediatricians towards vegetarian diets | Online questionnaire based on a previously validated questionnaire | Pediatricians had knowledge gaps regarding vegetarian nutrition, and most did not have a positive attitude towards vegetarian diets. Knowledge was positively correlated with attitude. |
| Lessem et al., 2020 [75] | USA | Experiential education program | N = 30 (13 nurse practitioners, 14 registered nurses, and 3 physicians) | Increase knowledge and acceptance of whole-food plant-based (WFPB) diets and the likelihood of counseling patients about the diet among health care workers | Online questionnaires based on previously validated research | Pre-intervention average knowledge scores were 65.4%. Average self-efficacy scores for knowledge and counseling were 2.64 and 2.38 at baseline on a scale of 1 to 4. |
| Sentenach et al., 2019 [76] | Spain | Cross- sectional | N = 422 physicians (PREDIMED screener) and N = 212 physicians (knowledge/opinion survey) | Evaluate physicians’ knowledge/awareness of and adherence to an MD | Online questionnaire based on the PREDIMED MD screener previously used in the PREDIMED study | Most physicians did not adhere to the MD, but 70% considered themselves knowledgeable about the benefits of the MD, and 60% were willing to recommend it to patients. |
| Estell & Hughes, 2021 [77] | Australia | Cross- sectional | N = 660 (228 nutrition professionals) | Explore consumer and nutrition professional perceptions and attitudes to plant protein, including plant-based meat alternatives | Online questionnaire based on previous research | Over 80% of nutrition professionals agreed that following a PBD promoted good nutrition, and over 70% disagreed that it was hard to meet protein requirements while following a PBD. |
| Asher et al., 2021 [61] | Canada | Cross- sectional | N = 403 dietitians | Assess Canadian registered dietitians’ attitudes and behaviors towards the new food guidelines’ increased plant-based recommendations | The online questionnaire developed for the study and pre-tested | Over 80% of dietitians considered the food guide’s recommendation to choose plant-based protein foods as evidence-based. Most had a positive view of the new guidelines, and 58.7% were more likely to encourage their clients to select plant-based protein options. |
| Aggarwal et al., 2019 [78] | USA | Cross- sectional | N = 303 physicians from departments of cardiology and general medicine | Assess nutrition and exercise knowledge and personal health behaviors of physicians | Online questionnaire based on validated surveys | Less than 25% of the physicians in the study followed the facets of MD. |
| Saintila et al., 2021 [62] | Peru | Cross- Sectional | N = 179 registered dietitians (72 vegetarians and 107 non-vegetarians) | Compare the level of knowledge of vegetarian and non-vegetarian Peruvian dietitians regarding vegetarianism | Online questionnaire based on the recommendations of the current dietary guidelines | Vegetarian dietitians were more knowledgeable about the risks and benefits associated with vegetarian diets. |
| Janse et al., 2021 [63] | South Africa | Cross- Sectional | N = 101 dietitians (45 government employed and 48 in private practice) | Assess whether dietitians in South Africa would use a whole-foods plant-based diet (WFPBD) to address chronic diseases | Online questionnaire based on validated surveys | A significant number of dietitians reported inadequate university training surrounding PBDs, albeit a significant number of them were confident about prescribing PBDs to clients. |
| Duncan & Bergman, 1999 [64] | USA | Cross- sectional | N = 183 registered dietitians from Vermont, Nebraska, and Washington | Investigate what registered dietitians know about the safety, adequacy, and health benefits of vegetarian diets | Paper questionnaire sent by mail | Average knowledge and attitude scores were greater for registered dietitians who were currently or had previously followed a vegetarian diet. Overall knowledge scores varied between states. |
| Fresan et al., 2023 [79] | Spain | Cross- Sectional | N = 2545 health professionals (550 dietitian-nutritionists, 1139 nurses, 427 physicians and 346 pharmacists, and 83 others) | Assess knowledge and attitudes regarding sustainable diets among health professionals in Spain | Online questionnaire developed for the study | Approximately 21.5% of respondents had not previously heard about sustainable diets, and 32.4% acknowledged their limited knowledge about the subject. Most when presented with information about sustainable diets considered it important to promote them. |
| Krause et al., 2019 [80] | USA | Cross- Sectional | N = 64 (12 residents,6 fellows, 46 physician attendings) | Assess medical providers’ knowledge of plant-based nutrition and their willingness to recommend it to patients | Online questionnaire developed for the study | Approximately 33% of respondents were willing to recommend PBDs, while the majority (51%) responded with maybe. Only 28% were willing to adopt PBDs, and 25% were willing to try it for 6 months or more. |
| Lee et al., 2015 [37] | Canada | Cross- Sectional | N = 98 patients and 25 health care providers | Assess awareness, barriers, and promoters of plant-based diet use for the management of type 2 diabetes for the development of an educational program | Two sets of questionnaires for patients and health care providers were developed for the study | Approximately 72% of health care providers reported knowledge of PBDs for the management of type 2, while the majority of patients (89%) had not heard of using PBDs to treat/manage type 2 diabetes. Less than 50% of respondents were aware of the benefits of PBDs regarding other chronic conditions. |
| Harkin et al., 2018 [81] | USA | Cross- Sectional | N = 236 (140 physicians and 96 cardiologists) | Assess basic nutritional knowledge, attitudes, and practices of physicians | Online questionnaire based on validated surveys | Nutrition knowledge was average, with only 13.5% feeling sufficiently trained to discuss nutrition with their patients. Physicians most commonly recommended the MD (55.1%), followed by the DASH diet (38.2%), to their patients. |
| Theme | TDF Domains | Enablers | Barriers |
| Knowledge |
|
|
|
| Education and training |
|
|
|
| Evidence-based guidelines |
|
|
|
| Multi-disciplinary collaboration |
|
|
|
| Personal experience and interest |
|
|
|
| Educational resources for both patients and health professionals |
|
|
|
| Lack of time |
|
|
|
| Safety and compliance challenges |
|
|
|
| Lack of confidence in patient capabilities |
|
|
|
| Category | Physicians/Clinicians | Dietitians/Nutritionists |
|---|---|---|
| Barriers | Limited nutritional education, training, and practical skills at degree and professional levels | Patient resistance/culture |
| Time constraints | Limited resources | |
| Lack of clear clinical practice guidelines and lack of knowledge of guidelines | Time constraints | |
| Uncertainty about scientific evidence or the benefits of PBDs | Lack of patient education and monitoring resources | |
| Limited resources | ||
| Perception that diet counseling is not their responsibility | ||
| Worry about overall health/fear of patient injury/risk of deficiency | ||
| Limited dietary knowledge exchange within and across multidisciplinary teams | ||
| Lack of diet-specific educational support | ||
| Low perceived patient acceptability | ||
| Low self-efficacy | ||
| Financial disincentives | ||
| Enablers | Patient interest in PBDs | Professional development |
| Evidence-based support for PBD benefits | Patient interest in PBDs | |
| Professional development | Personal history of following a PBD | |
| Institutional initiatives promoting preventive care | Knowledge sharing from expert dietitians | |
| Interest in lifestyle medicine | ||
| Beliefs about consequences | ||
| Personal history of following a PBD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sempa, J.; Brenes, P.; Whitehair, K.; Hobbs, L.; Kidd, T. Decoding Health Professionals’ Attitudes and Perceptions Towards Plant-Based Nutrition: A Narrative Review. Nutrients 2025, 17, 2095. https://doi.org/10.3390/nu17132095
Sempa J, Brenes P, Whitehair K, Hobbs L, Kidd T. Decoding Health Professionals’ Attitudes and Perceptions Towards Plant-Based Nutrition: A Narrative Review. Nutrients. 2025; 17(13):2095. https://doi.org/10.3390/nu17132095
Chicago/Turabian StyleSempa, Judith, Priscilla Brenes, Kelly Whitehair, Lonnie Hobbs, and Tandalayo Kidd. 2025. "Decoding Health Professionals’ Attitudes and Perceptions Towards Plant-Based Nutrition: A Narrative Review" Nutrients 17, no. 13: 2095. https://doi.org/10.3390/nu17132095
APA StyleSempa, J., Brenes, P., Whitehair, K., Hobbs, L., & Kidd, T. (2025). Decoding Health Professionals’ Attitudes and Perceptions Towards Plant-Based Nutrition: A Narrative Review. Nutrients, 17(13), 2095. https://doi.org/10.3390/nu17132095