
Impact of Isomaltulose on Glycemic Response in Diabetic and Healthy Populations: A Meta-Analysis



Abstract
1. Introduction

2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Outcomes and Quality Assessment
2.6. Statistical Analysis
3. Results
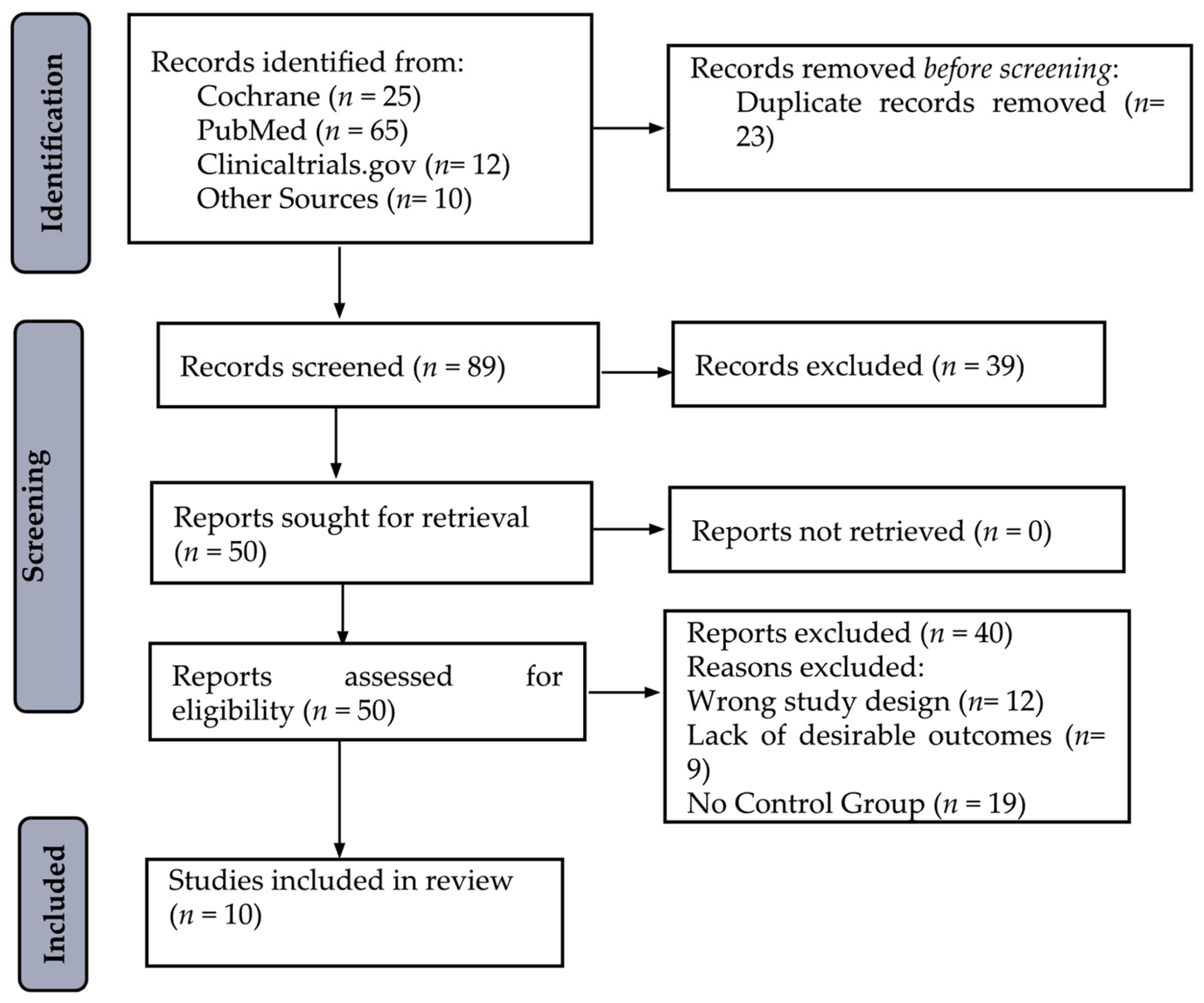
3.1. Search Results
3.2. Study Characteristics
3.3. Glycemic Response at 60 min Post-Meal
3.4. Subgroup Analysis
3.5. Sensitivity Analysis
3.6. Risk of Bias Assessment

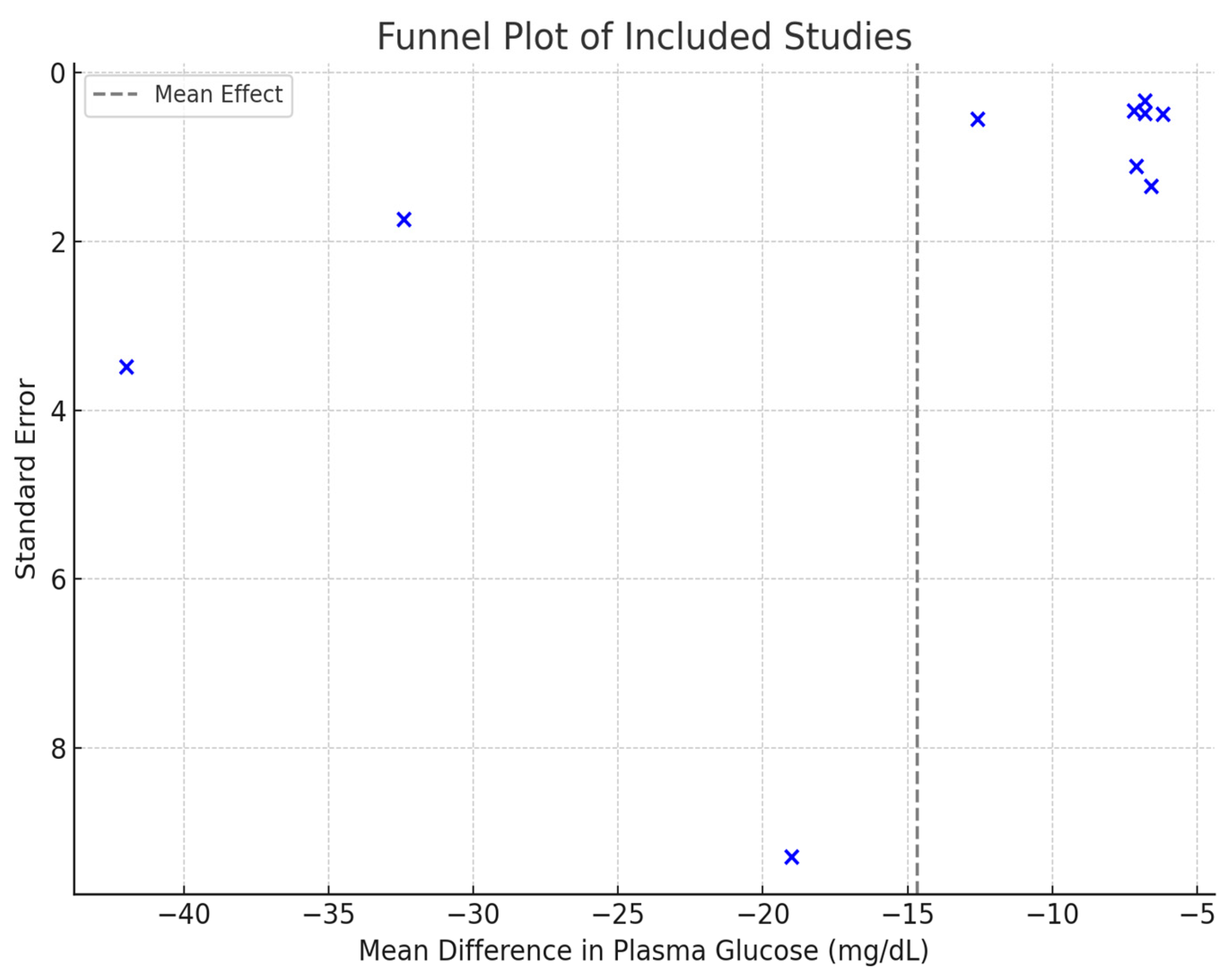
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hershon, K.S.; Hirsch, B.R.; Odugbesan, O. Importance of postprandial glucose in relation to A1C and cardiovascular disease. Clin. Diabetes 2019, 37, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S. Diabetes: From research to clinical practice. In Diabetes: From Research to Clinical Practice; Springer: Berlin/Heidelberg, Germany, 2020; Volume 4, pp. 1–5. [Google Scholar]
- Keyhani-Nejad, F.; Irmler, M.; Isken, F.; Wirth, E.K.; Beckers, J.; Birkenfeld, A.L.; Pfeiffer, A.F. Nutritional strategy to prevent fatty liver and insulin resistance independent of obesity by reducing glucose-dependent insulinotropic polypeptide responses in mice. Diabetologia 2015, 58, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Keyhani-Nejad, F.; Kemper, M.; Schueler, R.; Pivovarova, O.; Rudovich, N.; Pfeiffer, A.F. Effects of palatinose and sucrose intake on glucose metabolism and incretin secretion in subjects with type 2 diabetes. Diabetes Care 2016, 39, e38–e39. [Google Scholar] [CrossRef] [PubMed]
- Lina, B.; Jonker, D.; Kozianowski, G. Isomaltulose (Palatinose®): A review of biological and toxicological studies. Food Chem. Toxicol. 2002, 40, 1375–1381. [Google Scholar] [CrossRef]
- De Oliva-Neto, P.; Menão, P.T. Isomaltulose production from sucrose by Protaminobacter rubrum immobilized in calcium alginate. Bioresour. Technol. 2009, 100, 4252–4256. [Google Scholar] [CrossRef]
- Livesey, G. Carbohydrate Digestion, Absorption, and Fiber. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Kawai, K.; Yoshikawa, H.; Murayama, Y.; Okuda, Y.; Yamashita, K. Usefulness of palatinose as a caloric sweetener for diabetic patients. Horm. Metab. Res. 1989, 21, 338–340. [Google Scholar] [CrossRef]
- Holub, I.; Gostner, A.; Theis, S.; Nosek, L.; Kudlich, T.; Melcher, R.; Scheppach, W. Novel findings on the metabolic effects of the low glycaemic carbohydrate isomaltulose (Palatinose™). Br. J. Nutr. 2010, 103, 1730–1737. [Google Scholar] [CrossRef]
- Keller, J.; Kahlhöfer, J.; Peter, A.; Bosy-Westphal, A. Effects of low versus high glycemic index sugar-sweetened beverages on postprandial vasodilatation and inactivity-induced impairment of glucose metabolism in healthy men. Nutrients 2016, 8, 802. [Google Scholar] [CrossRef]
- Tan, W.S.K.; Tan, S.-Y.; Henry, C.J. Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose. Nutrients 2017, 9, 347. [Google Scholar] [CrossRef]
- Xie, J.; Li, J.; Qin, Q.; Ning, H.; Long, Z.; Gao, Y.; Yu, Y.; Han, Z.; Wang, F.; Wang, M. Effect of isomaltulose on glycemic and insulinemic responses: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2022, 13, 1901–1913. [Google Scholar] [CrossRef]
- Maresch, C.C.; Petry, S.F.; Theis, S.; Bosy-Westphal, A.; Linn, T. Low glycemic index prototype isomaltulose—Update of clinical trials. Nutrients 2017, 9, 381. [Google Scholar] [CrossRef] [PubMed]
- Fels, L.; Ruf, F.; Bunzel, M. Quantification of isomaltulose in food products by using heteronuclear single quantum coherence NMR-experiments. Front. Nutr. 2022, 9, 928102. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Schäfer, S.M.; Kabisch, S.; Csanalosi, M.; Schuppelius, B.; Kemper, M.; Markova, M.; Meyer, N.M.T.; Pivovarova-Ramich, O.; Keyhani-Nejad, F. Implication of sugar, protein and incretins in excessive glucagon secretion in type 2 diabetes after mixed meals. Clin. Nutr. 2023, 42, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Sokołowska, E.; Sadowska, A.; Sawicka, D.; Kotulska-Bąblińska, I.; Car, H. A head-to-head comparison review of biological and toxicological studies of isomaltulose, d-tagatose, and trehalose on glycemic control. Crit. Rev. Food Sci. Nutr. 2022, 62, 5679–5704. [Google Scholar] [CrossRef]
- Sawale, P.D.; Shendurse, A.M.; Mohan, M.S.; Patil, G. Isomaltulose (palatinose)—An emerging carbohydrate. Food Biosci. 2017, 18, 46–52. [Google Scholar] [CrossRef]
- Von Rymon Lipinski, G.W. 10—Reduced-calorie sweeteners and caloric alternatives. In Optimising Sweet Taste in Foods; Spillane, W.J., Ed.; Woodhead Publishing: Cambridge, UK, 2006; pp. 252–280. [Google Scholar]
- Kordowski, A.; Künstner, A.; Schweitzer, L.; Theis, S.; Schröder, T.; Busch, H.; Sina, C.; Smollich, M. Palatinose™ (isomaltulose) and prebiotic inulin-type fructans have beneficial effects on glycemic response and gut microbiota composition in healthy volunteers—A real-life, retrospective study of a cohort that participated in a digital nutrition program. Front. Nutr. 2022, 9, 829933. [Google Scholar] [CrossRef]
- Pfeiffer, A.F.; Keyhani-Nejad, F. High glycemic index metabolic damage–a pivotal role of GIP and GLP-1. Trends Endocrinol. Metab. 2018, 29, 289–299. [Google Scholar] [CrossRef]
- Hermansen, K.; Mortensen, L.S.; Hermansen, M.L. Combining insulins with oral antidiabetic agents: Effect on hyperglycemic control, markers of cardiovascular risk and disease. Vasc. Health Risk. Manag. 2008, 4, 561–574. [Google Scholar] [CrossRef]
- Sabarathinam, S. A glycemic diet improves the understanding of glycemic control in diabetes patients during their follow-up. Future Sci. OA 2023, 9, fso843. [Google Scholar] [CrossRef]
- Surat Komindr, M. Impact of isomaltulose and sucrose based breakfasts on postprandial substrate oxidation and glycemic/insulinemic changes in type-2 diabetes mellitus subjects. J. Med. Assoc. Thai 2016, 99, 282–289. [Google Scholar]
- Ang, M.; Linn, T. Comparison of the effects of slowly and rapidly absorbed carbohydrates on postprandial glucose metabolism in type 2 diabetes mellitus patients: A randomized trial123. Am. J. Clin. Nutr. 2014, 100, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Okuda, Y.; Yamashita, K. Changes in blood glucose and insulin after an oral palatinose administration in normal subjects. Endocrinol. Jpn. 1985, 32, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Amano, T.; Katayama, S.; Okamoto, Y.; Otsuka, J.; Fujii, N.; Kenny, G.P.; Nishiyasu, T.; Enoki, Y.; Maejima, D. Comparisons of isomaltulose, sucrose, and mixture of glucose and fructose ingestions on postexercise hydration state in young men. Eur. J. Nutr. 2021, 60, 4519–4529. [Google Scholar] [CrossRef]
- Mills, B.M.; Keesing, C.T.; Haszard, J.J.; Venn, B.J. The effect on satiety of ingesting isosweet and isoenergetic sucrose- and isomaltulose-sweetened beverages: A randomised crossover trial. Br. J. Nutr. 2020, 124, 225–231. [Google Scholar] [CrossRef]
- Lee, H.W.; Bi, X.; Henry, C.J. Comparative evaluation of minerals content of common green leafy vegetables consumed by the Asian populations in Singapore. J. Food Compos. Anal. 2024, 125, 105787. [Google Scholar] [CrossRef]
- McCarthy, O.M.; Christensen, M.B.; Tawfik, S.; Kristensen, K.B.; Hartmann, B.; Holst, J.J.; Schmidt, S.; Nørgaard, K.; Bracken, R.M. Metabolic and Hormonal Responses to Isomaltulose Ingestion Before or During Sustained Submaximal Exercise in Adults with Type 1 Diabetes Using Automated Insulin Delivery Systems. Nutrients 2024, 16, 4098. [Google Scholar] [CrossRef]
- Fujiwara, T.; Naomoto, Y.; Motoki, T.; Shigemitsu, K.; Shirakawa, Y.; Yamatsuji, T.; Kataoka, M.; Haisa, M.; Fujiwara, T.; Egi, M. Effects of a novel palatinose based enteral formula (MHN-01) carbohydrate-adjusted fluid diet in improving the metabolism of carbohydrates and lipids in patients with esophageal cancer complicated by diabetes mellitus. J. Surg. Res. 2007, 138, 231–240. [Google Scholar] [CrossRef]
- Vanschoonbeek, K.; Lansink, M.; Van Laere, K.; Senden, J.; Verdijk, L.; Van Loon, L. Slowly digestible carbohydrate sources can be used to attenuate the postprandial glycemic response to the ingestion of diabetes-specific enteral formulas. Diabetes Educ. 2009, 35, 631–640. [Google Scholar] [CrossRef]
- Banks, J.; Amspoker, A.B.; Vaughan, E.M.; Woodard, L.; Naik, A.D. Ascertainment of minimal clinically important differences in the diabetes distress scale–17: A secondary analysis of a randomized clinical trial. JAMA Netw. Open 2023, 6, e2342950. [Google Scholar] [CrossRef]
- Mateo-Gallego, R.; Pérez-Calahorra, S.; Lamiquiz-Moneo, I.; Marco-Benedí, V.; Bea, A.M.; Fumanal, A.J.; Prieto-Martín, A.; Laclaustra, M.; Cenarro, A.; Civeira, F. Effect of an alcohol-free beer enriched with isomaltulose and a resistant dextrin on insulin resistance in diabetic patients with overweight or obesity. Clin. Nutr. 2020, 39, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Häberer, D.; Thibault, L.; Langhans, W.; Geary, N. Beneficial effects on glucose metabolism of chronic feeding of isomaltulose versus sucrose in rats. Ann. Nutr. Metab. 2009, 54, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Takeda, E.; Yamanaka-Okumura, H.; Taketani, Y.; Inagaki, N.; Hosokawa, M.; Shide, K.; Maegawa, H.; Kondo, K.; Kawasaki, E.; Shinozaki, S. Effect of nutritional counseling and long term isomaltulose based liquid formula (MHN-01) intake on metabolic syndrome. J. Clin. Biochem. Nutr. 2015, 57, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Koshinaka, K.; Ando, R.; Sato, A. Short-term replacement of starch with isomaltulose enhances both insulin-dependent and-independent glucose uptake in rat skeletal muscle. J. Clin. Biochem. Nutr. 2018, 63, 113–122. [Google Scholar] [CrossRef]
- De Souza, W.F.C.; Almeida, F.L.C.; de Castro, R.J.S.; Sato, H.H. Isomaltulose: From origin to application and its beneficial properties—A bibliometric approach. Food Res. Int. 2022, 155. [Google Scholar] [CrossRef]
- Gerontiti, E.; Shalit, A.; Stefanaki, K.; Kazakou, P.; Karagiannakis, D.S.; Peppa, M.; Psaltopoulou, T.; Paschou, S.A. The role of low glycemic index and load diets in medical nutrition therapy for type 2 diabetes: An update. Hormones 2024, 23, 655–665. [Google Scholar] [CrossRef]
- Zhang, J.; Sonnenburg, D.; Tricò, D.; Kabisch, S.; Mari, A.; Theis, S.; Kemper, M.; Pivovarova-Ramich, O.; Rohn, S.; Pfeiffer, A.F.H. Isomaltulose Enhances GLP-1 and PYY Secretion to a Mixed Meal in People With or Without Type 2 Diabetes as Compared to Saccharose. Mol. Nutr. Food Res. 2024, 68, 2300086. [Google Scholar] [CrossRef]
- Shyam, S.; Ramadas, A.; Chang, S.K. Isomaltulose: Recent evidence for health benefits. J. Funct. Foods 2018, 48, 173–178. [Google Scholar] [CrossRef]
- Takeda, E.; Arai, H.; Yamamoto, H.; Okumura, H.; Taketani, Y. Control of oxidative stress and metabolic homeostasis by the suppression of postprandial hyperglycemia. J. Med. Investig. 2005, 52, 259–265. [Google Scholar] [CrossRef]
- Tudurí, E.; Soriano, S.; Almagro, L.; Montanya, E.; Alonso-Magdalena, P.; Nadal, Á.; Quesada, I. The pancreatic β-cell in ageing: Implications in age-related diabetes. Ageing Res. Rev. 2022, 80, 101674. [Google Scholar] [CrossRef]
- Leow, M. The Glycaemic Effect of Isomaltulose Consumption in Healthy Participants; Singapore Institute Of Food And Biotechnology Innovation: Singapore, 2017.
- West, D.J.; Morton, R.D.; Stephens, J.W.; Bain, S.C.; Kilduff, L.P.; Luzio, S.; Still, R.; Bracken, R.M. Isomaltulose improves postexercise glycemia by reducing CHO oxidation in T1DM. Med. Sci. Sports Exerc. 2011, 43, 204–210. [Google Scholar] [CrossRef] [PubMed]
- van Can, J.G.; van Loon, L.J.; Brouns, F.; Blaak, E.E. Reduced glycaemic and insulinaemic responses following trehalose and isomaltulose ingestion: Implications for postprandial substrate use in impaired glucose-tolerant subjects. Br. J. Nutr. 2012, 108, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Giuntini, E.B.; Sardá, F.A.H.; de Menezes, E.W. The effects of soluble dietary fibers on glycemic response: An overview and futures perspectives. Foods 2022, 11, 3934. [Google Scholar] [CrossRef] [PubMed]
- Keyhani-Nejad, F.; Yanez, R.L.B.; Kemper, M.; Schueler, R.; Pivovarova-Ramich, O.; Rudovich, N.; Pfeiffer, A.F. Endogenously released GIP reduces and GLP-1 increases hepatic insulin extraction. Peptides 2020, 125, 170231. [Google Scholar] [CrossRef]
- Brunner, S.; Holub, I.; Theis, S.; Gostner, A.; Melcher, R.; Wolf, P.; Amann-Gassner, U.; Scheppach, W.; Hauner, H. Metabolic effects of replacing sucrose by isomaltulose in subjects with type 2 diabetes: A randomized double-blind trial. Diabetes Care 2012, 35, 1249–1251. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Year | Population Type | Population Age (mean) | Sample Size | Gender | Washout Period | Mean BMI (kg/m2) | |
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| Kawai, 1985 [26] | Healthy | 23 | 8 | 4 | 4 | 2 days | 19.7 |
| Kawai, 1989 [8] | Healthy | 23.1 | 10 | 5 | 5 | 2 days | 19.5 |
| Tan et al., 2017 [11] | Healthy | 21–49 | 40 | Mixed | Mixed | 2 days | 24 |
| Lee, 2024 [29] | Healthy | 21–60 | 65 | 65 | 0 | 14 days | 22–27 |
| Amano et al., 2021 [27] | Healthy | 24 | 10 | 10 | 0 | 7 days | 22.5 |
| Mills et al., 2020 [28] | Healthy | 30 | 77 | Mixed | Mixed | 14 days | 24 |
| Komindr, 2016 [23] | T2DM | 49.64 | 11 | 0 | 11 | 10 h | 27.81 |
| Ang, 2014 [24] | T2DM | 53.7 | 11 | 5 | 6 | 14 days | 31.6 |
| Kordowski et al., 2022 [19] | T2DM | 42.9 | 117 | Mixed | Mixed | 14 days | 28.7 ± 6.7 |
| McCarthy et al., 2024 [30] | T1DM | 47 ± 16 | 8 | 3 | 5 | 10 days | 27.5 ± 3.8 |
| Study Design | Region | Population Type | Intervention Method | Intervention | Control | Refs. |
|---|---|---|---|---|---|---|
| CS | Japan | Healthy | Ingesting sugars dissolved in 150 mL water over 2–3 min after an overnight fast | Isomaltulose (50 g) | Sucrose (50 g) | [26] |
| CS | Japan | Healthy | Ingesting sugars dissolved in 150 mL water within 2–3 min after an overnight fast | Isomaltulose (50 g) | Sucrose (50 g) | [8] |
| Randomized CS | Japan | Healthy | Ingesting 10% isomaltulose or sucrose drink before exercise in a hot environment | Isomaltulose (10%) | Sucrose (10%) | [27] |
| Randomized CS | New Zealand | Healthy | Ingesting sucrose or isomaltulose drink after standard lunch, followed by satiety assessment | Isomaltulose (50 g) | Sucrose (50 g) | [28] |
| SB Randomized CS | Singapore | Healthy | Ingesting different sucrose: isomaltulose ratios over 9 test sessions | Various sucrose:isomaltulose ratios | Standard glucose solution | [29] |
| SB Randomized CS | Singapore | Healthy | Ingesting sucrose or isomaltulose drink (50 g carbohydrate) | isomaltulose (50 g) | Sucrose (50 g) | [11] |
| DB Randomized CS | Germany | T2DM | Ingesting sugars dissolved in 200 mL water within 5 min after an overnight fast | Isomaltulose | Sucrose | [24] |
| RCS | Germany | T2DM | Digital nutrition program with 14-day continuous glucose monitoring | Isomaltulose-sweetened meals | Sucrose-sweetened meals | [19] |
| DB Randomized CS | Thailand | T2DM | Breakfast meal with cooked rice, fried boiled egg with tamarind sauce, Chinese cabbage plus minced pork soup, hot cocoa drink | 51% Isomaltulose | Sucrose | [23] |
| Randomized CS | Denmark | T1DM | Ingesting isomaltulose before or during exercise, glucose and insulin levels measured | Isomaltulose (0.75 g/kg BMI) | Sucrose | [30] |
| Group 1: Isomaltulose | Group 1: Sucrose (Control) | Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| Study of Subgroup | Mean (mg/dL) | SD (mg/dL) | Total | Mean (mg/dL) | SD (mg/dL) | Total | Weight | IV, Fixed, 95% CI (mg/dL) |
| Ang et al. [24] | 104.4 | 1.8 | 11 | 117 | 1.8 | 11 | 15.70% | −12.6 (−14.10, −11.10) |
| Lee [29] | 24.5 | 3.9 | 65 | 30.7 | 4.5 | 65 | 17.00% | −6.20 (−7.65, −4.75) |
| Kawai et al., 1985 [26] | 110.9 | 4.9 | 8 | 143.3 | 8.8 | 8 | 0.70% | −32.40 (−39.38, −25.42) |
| Kawai et al., 1989 [8] | 195 | 11 | 10 | 237 | 12 | 10 | 0.30% | −42.00 (−52.09, −31.91) |
| Komindr et al. [23] | 87.18 | 30.78 | 11 | 106.18 | 26.24 | 11 | 0.10% | −19.00 (−42.90, 4.90) |
| Kordowski et al. [19] | 28.4 | 3.6 | 117 | 35.2 | 4.5 | 117 | 32.60% | −6.80 (−7.84, −5.76) |
| Tan [11] | 22.9 | 3.2 | 50 | 30.1 | 4.8 | 50 | 13.90% | −7.20 (−8.80, −5.60) |
| McCarthy et al. [30] | 27.5 | 3.8 | 8 | 34.1 | 4.9 | 8 | 1.90% | −6.60 (−10.90, −2.30) |
| Mills et al. [28] | 24 | 4.2 | 77 | 30.8 | 5.6 | 77 | 14.50% | −6.80 (−8.36, −5.24) |
| Amano et al. [27] | 122.5 | 3.5 | 10 | 29.6 | 4.1 | 10 | 3.20% | −7.10 (−10.44, −3.76) |
| Total | 367 | 367 | 100% | −7.99 (−8.58, −7.39) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Gu, F.; Wu, J. Impact of Isomaltulose on Glycemic Response in Diabetic and Healthy Populations: A Meta-Analysis. Nutrients 2025, 17, 1940. https://doi.org/10.3390/nu17111940
Chen Z, Gu F, Wu J. Impact of Isomaltulose on Glycemic Response in Diabetic and Healthy Populations: A Meta-Analysis. Nutrients. 2025; 17(11):1940. https://doi.org/10.3390/nu17111940
Chicago/Turabian StyleChen, Zhaojie, Fangting Gu, and Jianyong Wu. 2025. "Impact of Isomaltulose on Glycemic Response in Diabetic and Healthy Populations: A Meta-Analysis" Nutrients 17, no. 11: 1940. https://doi.org/10.3390/nu17111940
APA StyleChen, Z., Gu, F., & Wu, J. (2025). Impact of Isomaltulose on Glycemic Response in Diabetic and Healthy Populations: A Meta-Analysis. Nutrients, 17(11), 1940. https://doi.org/10.3390/nu17111940