
Nutritional Deficiencies and Management in Tuberculosis: Pharmacotherapeutic and Clinical Implications

 ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Current Pharmacotherapy Guidelines in Tuberculosis
2.1. First-Line Antituberculosis Drugs
2.2. Second-Line and Newer Drugs for Drug-Resistant TB
2.3. Prophylaxis and Pharmacological Considerations in Special Populations
3. Nutritional Status and Tuberculosis
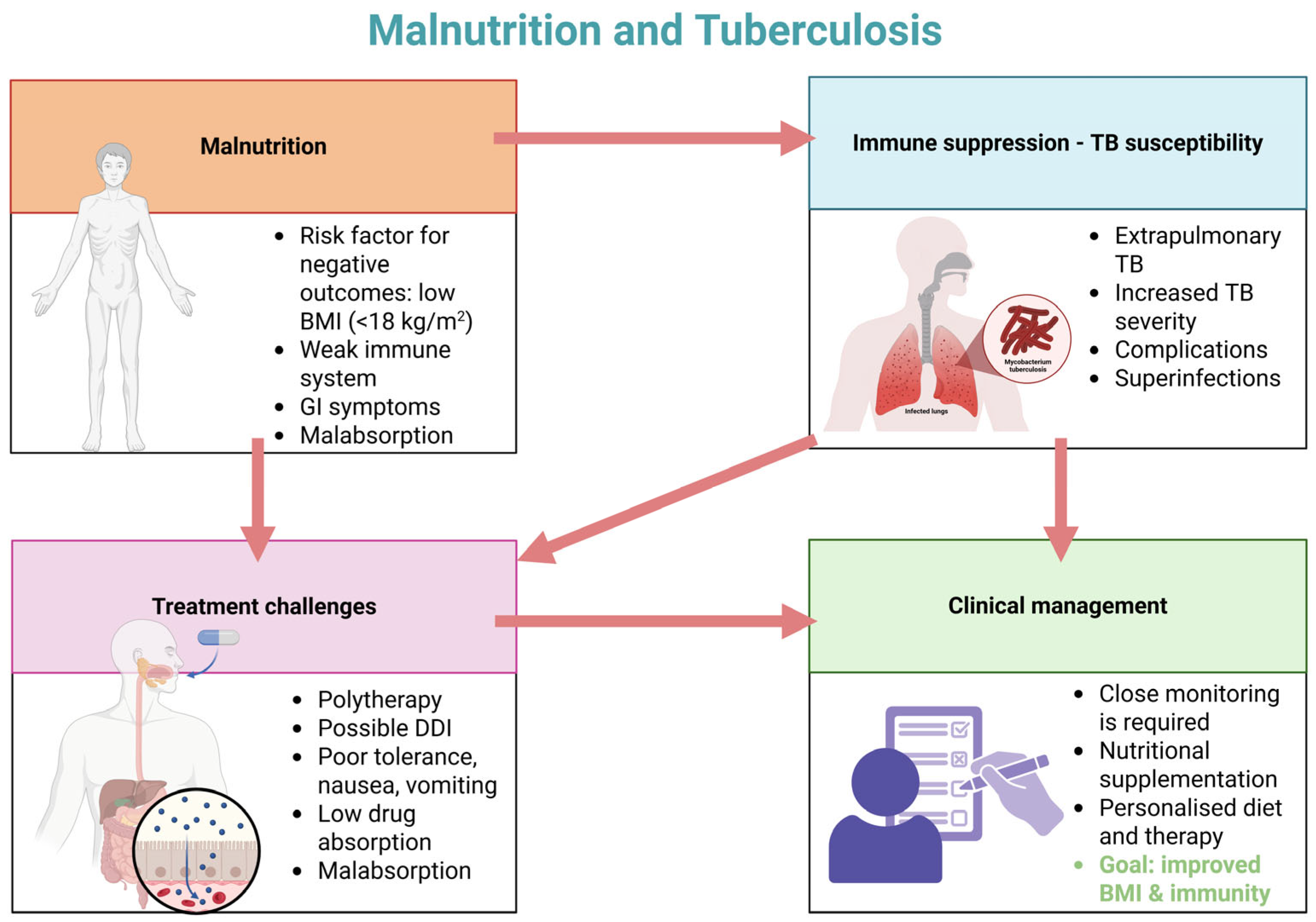
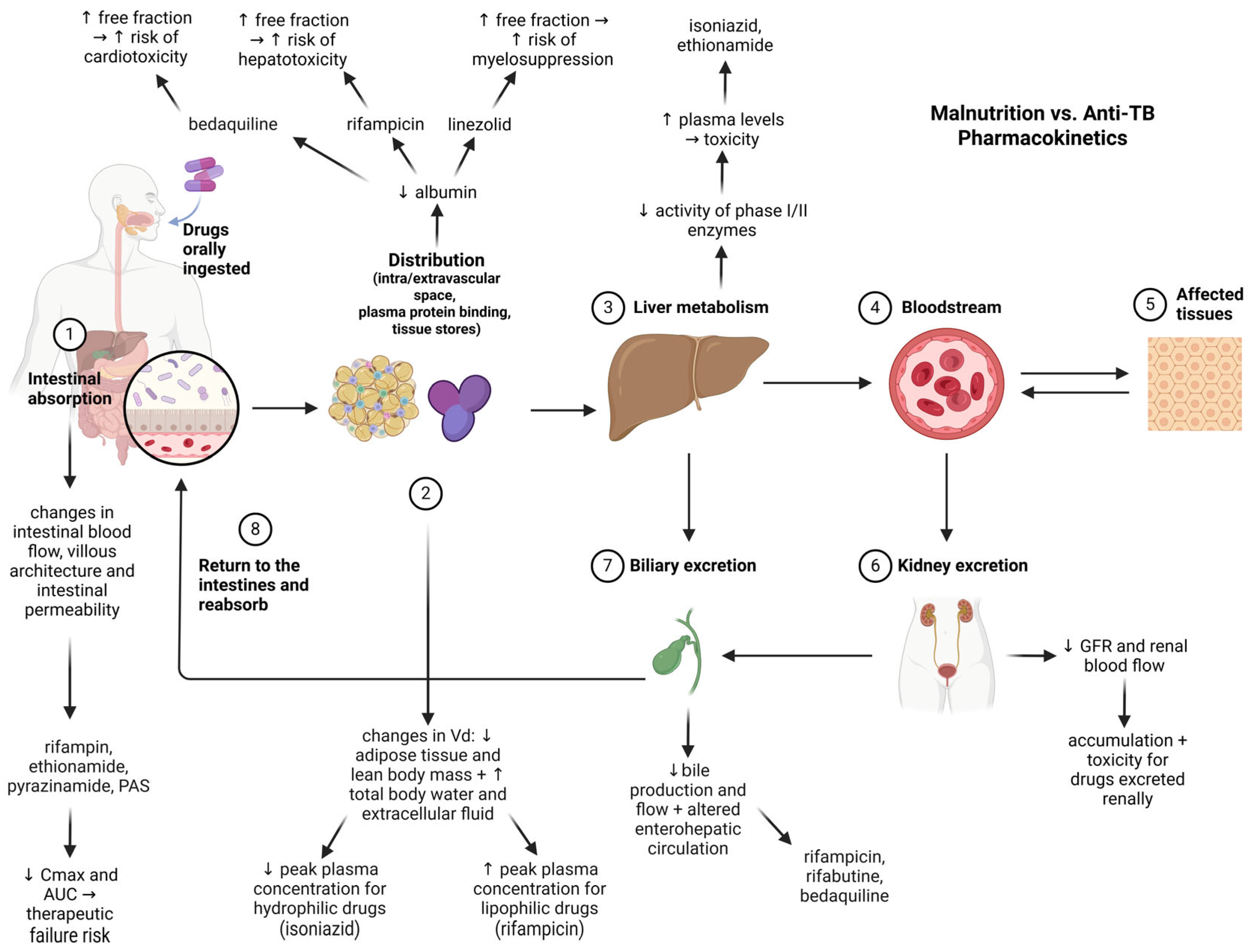
3.1. Malnutrition, TB Risk, and Impact on Pharmacotherapy
3.2. The Effect of TB Infection on Nutritional Status and Common Nutritional Deficiencies in TB Patients
4. Deficiencies Induced by Anti-TB Drugs and Drug-Nutrient Interactions
4.1. Drug-Induced Nutritional Deficiencies
4.2. Drug–Food Interactions in Tuberculosis Therapy
5. Nutritional Management of Tuberculosis Patients
6. Integrating Nutritional Management with Pharmacotherapy in TB Care
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barberis, I.; Bragazzi, N.L.; Galluzzo, L.; Martini, M. The history of tuberculosis: From the first historical records to the isolation of Koch’s bacillus. J. Prev. Med. Hyg. 2017, 58, E9–E12. [Google Scholar] [PubMed]
- World Health Organization Global Tuberculosis Report 2024. Available online: https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2024/tb-disease-burden/1-1-tb-incidence (accessed on 10 April 2025).
- Mondoni, M.; Centanni, S.; Sotgiu, G. New perspectives on difficult-to-treat tuberculosis based on old therapeutic approaches. Int. J. Infect. Dis. 2020, 92, S91–S99. [Google Scholar] [CrossRef] [PubMed]
- da Costa, C.; Benn, C.S.; Nyirenda, T.; Mpabalwani, E.; Grewal, H.M.S.; Ahmed, R.; Kapata, N.; Nyasulu, P.S.; Maeurer, M.; Hui, D.S.; et al. Perspectives on development and advancement of new tuberculosis vaccines. Int. J. Infect. Dis. 2024, 141, 106987. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Monde, N.; Munyeme, M.; Chongwe, G.; Wensman, J.J.; Zulu, M.; Siziya, S.; Tembo, R.; Siame, K.K.; Shambaba, O.; Malama, S. First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia. Antibiotics 2023, 12, 166. [Google Scholar] [CrossRef]
- Chin, K.L.; Anibarro, L.; Chang, Z.Y.; Palasuberniam, P.; Mustapha, Z.A.; Sarmiento, M.E.; Acosta, A. Impacts of MDR/XDR-TB on the global tuberculosis epidemic: Challenges and opportunities. Curr. Res. Microb. Sci. 2024, 7, 100295. [Google Scholar] [CrossRef]
- Mancuso, G.; Midiri, A.; De Gaetano, S.; Ponzo, E.; Biondo, C. Tackling Drug-Resistant Tuberculosis: New Challenges from the Old Pathogen Mycobacterium tuberculosis. Microorganisms 2023, 11, 2277. [Google Scholar] [CrossRef]
- Maison, D.P. Tuberculosis pathophysiology and anti-VEGF intervention. J. Clin. Tuberc. Other Mycobact. Dis. 2022, 27, 100300. [Google Scholar] [CrossRef]
- Huang, L.; Nazarova, E.V.; Russell, D.G. Mycobacterium tuberculosis: Bacterial Fitness within the Host Macrophage. Microbiol. Spectr. 2019, 7, 127–138. [Google Scholar] [CrossRef]
- CDC Clinical Symptoms of Tuberculosis. Available online: https://www.cdc.gov/tb/hcp/clinical-signs-and-symptoms/index.html (accessed on 12 April 2025).
- Naghavi, M.; Vollset, S.E.; Ikuta, K.S.; Swetschinski, L.R.; Gray, A.P.; Wool, E.E.; Robles Aguilar, G.; Mestrovic, T.; Smith, G.; Han, C.; et al. Global burden of bacterial antimicrobial resistance 1990–2021: A systematic analysis with forecasts to 2050. Lancet 2024, 404, 1199–1226. [Google Scholar] [CrossRef]
- Méndez López, L.F.; González Llerena, J.L.; Vázquez Rodríguez, J.A.; Medellín Guerrero, A.B.; González Martínez, B.E.; Solís Pérez, E.; López-Cabanillas Lomelí, M. Dietary Modulation of the Immune System. Nutrients 2024, 16, 4363. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’ambrosio, L.; Migliori, G.B. Tuberculosis Treatment and Drug Regimens. Cold Spring Harb. Perspect. Med. 2015, 5, a017822. [Google Scholar] [CrossRef] [PubMed]
- Mencarini, J.; Spinicci, M.; Zammarchi, L.; Bartoloni, A. Tuberculosis in the European Region. Curr. Trop. Med. Rep. 2023, 10, 88–93. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Consolidated Operational Handbook on Tuberculosis. Module 4: Treatment and Care; World Health Organization: Geneva, Switzerland, 2025. [Google Scholar]
- Unissa, A.N.; Subbian, S.; Hanna, L.E.; Selvakumar, N. Overview on mechanisms of isoniazid action and resistance in Mycobacterium tuberculosis. Infect. Genet. Evol. 2016, 45, 474–492. [Google Scholar] [CrossRef]
- Pang, Y.; Lu, J.; Wang, Y.; Song, Y.; Wang, S.; Zhao, Y. Study of the Rifampin Monoresistance Mechanism in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2013, 57, 893–900. [Google Scholar] [CrossRef]
- Gopal, P.; Grüber, G.; Dartois, V.; Dick, T. Pharmacological and Molecular Mechanisms Behind the Sterilizing Activity of Pyrazinamide. Trends Pharmacol. Sci. 2019, 40, 930–940. [Google Scholar] [CrossRef]
- Zhu, C.; Liu, Y.; Hu, L.; Yang, M.; He, Z.-G. Molecular mechanism of the synergistic activity of ethambutol and isoniazid against Mycobacterium tuberculosis. J. Biol. Chem. 2018, 293, 16741–16750. [Google Scholar] [CrossRef]
- Sekaggya-Wiltshire, C.; von Braun, A.; Scherrer, A.U.; Manabe, Y.C.; Buzibye, A.; Muller, D.; Ledergerber, B.; Gutteck, U.; Corti, N.; Kambugu, A.; et al. Anti-TB drug concentrations and drug-associated toxicities among TB/HIV-coinfected patients. J. Antimicrob. Chemother. 2017, 72, 1172–1177. [Google Scholar] [CrossRef]
- Bakare, A.A.; Moses, V.Y.; Beckely, C.T.; Oluyemi, T.I.; Ogunfeitimi, G.O.; Adelaja, A.A.; Ayorinde, G.T.; Gbadebo, A.M.; Fagbenro, O.S.; Ogunsuyi, O.I.; et al. The first-line antituberculosis drugs, and their fixed-dose combination induced abnormal sperm morphology and histological lesions in the testicular cells of male mice. Front. Cell Dev. Biol. 2022, 10, 1023413. [Google Scholar] [CrossRef]
- Valadares, R.M.C.; Carvalho, W.d.S.; Miranda, S.S.d. Association of adverse drug reaction to anti-tuberculosis medication with quality of life in patients in a tertiary referral hospital. Rev. Soc. Bras. Med. Trop. 2020, 53, e20190207. [Google Scholar] [CrossRef]
- Mase, S.R.; Chorba, T. Treatment of Drug-Resistant Tuberculosis. Clin. Chest Med. 2019, 40, 775–795. [Google Scholar] [CrossRef] [PubMed]
- Liebenberg, D.; Gordhan, B.G.; Kana, B.D. Drug resistant tuberculosis: Implications for transmission, diagnosis, and disease management. Front. Cell. Infect. Microbiol. 2022, 12, 943545. [Google Scholar] [CrossRef] [PubMed]
- Grigoryan, Z.; McPherson, R.; Harutyunyan, T.; Truzyan, N.; Sahakyan, S. Factors Influencing Treatment Adherence Among Drug-Sensitive Tuberculosis (DS-TB) Patients in Armenia: A Qualitative Study. Patient Prefer. Adherence 2022, 16, 2399–2408. [Google Scholar] [CrossRef]
- Rusu, R.; Ababei, D.; Macadan, I.; Ciobîcă, A.; Paraschiv, M.; Bild, W.; Moraru, A.; Nicolae, C.; Bild, V. Factors that influence treatment adherence—Realities, controversies, perspectives. Farmacia 2023, 71, 638–647. [Google Scholar] [CrossRef]
- Jiang, W. Addressing the adherence challenge in tuberculosis treatment: More than digital technologies. Lancet Glob. Health 2023, 11, e634–e635. [Google Scholar] [CrossRef]
- Appiah, M.A.; Arthur, J.A.; Gborgblorvor, D.; Asampong, E.; Kye-Duodu, G.; Kamau, E.M.; Dako-Gyeke, P. Barriers to tuberculosis treatment adherence in high-burden tuberculosis settings in Ashanti region, Ghana: A qualitative study from patient’s perspective. BMC Public Health 2023, 23, 1317. [Google Scholar] [CrossRef]
- Walker, T.M.; Watson, J.A.; Moore, D.A.J.; Frick, M.; Jamrozik, E. Tuberculosis preventive therapy: Scientific and ethical considerations for trials of ultra-short regimens. Lancet Infect. Dis. 2025. [Google Scholar] [CrossRef]
- Graciaa, D.S.; Schechter, M.C.; Fetalvero, K.B.; Cranmer, L.M.; Kempker, R.R.; Castro, K.G. Updated considerations in the diagnosis and management of tuberculosis infection and disease: Integrating the latest evidence-based strategies. Expert Rev. Anti-Infect. Ther. 2023, 21, 595–616. [Google Scholar] [CrossRef]
- Suárez, I.; Rauschning, D.; Schüller, C.; Hagemeier, A.; Stecher, M.; Lehmann, C.; Schommers, P.; Schlabe, S.; Vehreschild, J.-J.; Koll, C.; et al. Incidence and risk factors for HIV-tuberculosis coinfection in the Cologne–Bonn region: A retrospective cohort study. Infection 2024, 52, 1439–1448. [Google Scholar] [CrossRef]
- Navasardyan, I.; Miwalian, R.; Petrosyan, A.; Yeganyan, S.; Venketaraman, V. HIV–TB Coinfection: Current Therapeutic Approaches and Drug Interactions. Viruses 2024, 16, 321. [Google Scholar] [CrossRef]
- Hîncu, S.; Apetroaei, M.-M.; Ștefan, G.; Fâcă, A.I.; Arsene, A.L.; Mahler, B.; Drăgănescu, D.; Tăerel, A.-E.; Stancu, E.; Hîncu, L.; et al. Drug–Drug Interactions in Nosocomial Infections: An Updated Review for Clinicians. Pharmaceutics 2024, 16, 1137. [Google Scholar] [CrossRef] [PubMed]
- Nhandara, R.B.C.; Ayele, B.T.; Sigwadhi, L.N.; Ozougwu, L.U.N.; Nyasulu, P.S. Determinants of adherence to clinic appointments among tuberculosis and HIV co-infected individuals attending care at Helen Joseph Hospital, Johannesburg, South Africa. Pan Afr. Med. J. 2020, 37, 118. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, P.; Saravanan, N.; Bethunaickan, R.; Tripathy, S. Malnutrition: Modulator of Immune Responses in Tuberculosis. Front. Immunol. 2017, 8, 1316. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ortega, E.F.; Meydani, S.N.; Adkins, Y.; Stephensen, C.B.; Thompson, B.; Zwickey, H. Nutrition, Immunosenescence, and Infectious Disease: An Overview of the Scientific Evidence on Micronutrients and on Modulation of the Gut Microbiota. Adv. Nutr. 2022, 13, S1–S26. [Google Scholar] [CrossRef]
- Morales, F.; Montserrat-de la Paz, S.; Leon, M.J.; Rivero-Pino, F. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children’s Health Status: A Literature Review. Nutrients 2023, 16, 1. [Google Scholar] [CrossRef]
- Fan, Y.; Yao, Q.; Liu, Y.; Jia, T.; Zhang, J.; Jiang, E. Underlying Causes and Co-existence of Malnutrition and Infections: An Exceedingly Common Death Risk in Cancer. Front. Nutr. 2022, 9, 814095. [Google Scholar] [CrossRef]
- Mendes, Y.C.; Dourado, A.L.L.; de Oliveira, P.V.; Rezende, A.d.O.; Sales, A.C.d.S.; de Sousa, G.P.; Pereira, E.d.A.; Sousa, E.L.C.; Lindoso, M.C.C.M.; Júnior, R.d.M.R.; et al. Nutritional Factors and Food and Nutrition Insecurity in Patients with Tuberculosis. Nutrients 2025, 17, 878. [Google Scholar] [CrossRef]
- Spanakis, M.; Patelarou, E.; Patelarou, A. Drug-Food Interactions with a Focus on Mediterranean Diet. Appl. Sci. 2022, 12, 10207. [Google Scholar] [CrossRef]
- Marinescu, S.C.; Apetroaei, M.-M.; Nedea, M.I.; Arsene, A.L.; Velescu, B.Ș.; Hîncu, S.; Stancu, E.; Pop, A.L.; Drăgănescu, D.; Udeanu, D.I. Dietary Influence on Drug Efficacy: A Comprehensive Review of Ketogenic Diet–Pharmacotherapy Interactions. Nutrients 2024, 16, 1213. [Google Scholar] [CrossRef]
- D’Alessandro, C.; Benedetti, A.; Di Paolo, A.; Giannese, D.; Cupisti, A. Interactions between Food and Drugs, and Nutritional Status in Renal Patients: A Narrative Review. Nutrients 2022, 14, 212. [Google Scholar] [CrossRef]
- Nisbett, N. Malnutrition as more-than-food: Understanding failings in the broader infrastructures of nurture. Child. Geogr. 2023, 21, 883–897. [Google Scholar] [CrossRef]
- Liana, Y.A.; Ndendya, J.Z.; Shaban, N. The nutritional nexus: Modeling the impact of malnutrition on TB transmission. Sci. Afr. 2025, 27, e02516. [Google Scholar] [CrossRef]
- World Health Organization. Tuberculosis and Malnutrition; World Health Organization: Copenhagen, Denmark, 2024. [Google Scholar]
- Ibrahim, M.K.; Zambruni, M.; Melby, C.L.; Melby, P.C. Impact of Childhood Malnutrition on Host Defense and Infection. Clin. Microbiol. Rev. 2017, 30, 919–971. [Google Scholar] [CrossRef] [PubMed]
- Raczyńska, A.; Leszczyńska, T.; Skotnicki, P.; Koronowicz, A. The Impact of Immunomodulatory Components Used in Clinical Nutrition—A Narrative Review. Nutrients 2025, 17, 752. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Redondo-Flórez, L.; Beltrán-Velasco, A.I.; Martín-Rodríguez, A.; Martínez-Guardado, I.; Navarro-Jiménez, E.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. The Role of Adipokines in Health and Disease. Biomedicines 2023, 11, 1290. [Google Scholar] [CrossRef]
- Hemat Jouy, S.; Mohan, S.; Scichilone, G.; Mostafa, A.; Mahmoud, A.M. Adipokines in the Crosstalk between Adipose Tissues and Other Organs: Implications in Cardiometabolic Diseases. Biomedicines 2024, 12, 2129. [Google Scholar] [CrossRef]
- Foolchand, A.; Ghazi, T.; Chuturgoon, A.A. Malnutrition and Dietary Habits Alter the Immune System Which May Consequently Influence SARS-CoV-2 Virulence: A Review. Int. J. Mol. Sci. 2022, 23, 2654. [Google Scholar] [CrossRef]
- Zhang, Y.; Kutateladze, T.G. Diet and the epigenome. Nat. Commun. 2018, 9, 3375. [Google Scholar] [CrossRef]
- Alwarawrah, Y.; Kiernan, K.; MacIver, N.J. Changes in Nutritional Status Impact Immune Cell Metabolism and Function. Front. Immunol. 2018, 9, 1055. [Google Scholar] [CrossRef]
- Cohen, S.; Danzaki, K.; MacIver, N.J. Nutritional effects on T-cell immunometabolism. Eur. J. Immunol. 2017, 47, 225–235. [Google Scholar] [CrossRef]
- Collins, N. Dietary Regulation of Memory T Cells. Int. J. Mol. Sci. 2020, 21, 4363. [Google Scholar] [CrossRef] [PubMed]
- Noor, Z.; Hasan, M.M.; Gazi, M.A.; Hossaini, F.; Haque, N.M.S.; Palit, P.; Fahim, S.M.; Das, S.; Mahfuz, M.; Marie, C.; et al. Immune modulation by nutritional intervention in malnourished children: Identifying the phenotypic distribution and functional responses of peripheral blood mononuclear cells. Scand. J. Immunol. 2023, 98, e13302. [Google Scholar] [CrossRef] [PubMed]
- Peroni, D.G.; Hufnagl, K.; Comberiati, P.; Roth-Walter, F. Lack of iron, zinc, and vitamins as a contributor to the etiology of atopic diseases. Front. Nutr. 2023, 9, 1032481. [Google Scholar] [CrossRef] [PubMed]
- Roth-Walter, F.; Berni Canani, R.; O’Mahony, L.; Peroni, D.; Sokolowska, M.; Vassilopoulou, E.; Venter, C. Nutrition in chronic inflammatory conditions: Bypassing the mucosal block for micronutrients. Allergy 2024, 79, 353–383. [Google Scholar] [CrossRef]
- Wang, R.; Lan, C.; Benlagha, K.; Camara, N.O.S.; Miller, H.; Kubo, M.; Heegaard, S.; Lee, P.; Yang, L.; Forsman, H.; et al. The interaction of innate immune and adaptive immune system. MedComm 2024, 5, e714. [Google Scholar] [CrossRef]
- Heggi, M.T.; Nour El-Din, H.T.; Morsy, D.I.; Abdelaziz, N.I.; Attia, A.S. Microbial evasion of the complement system: A continuous and evolving story. Front. Immunol. 2024, 14, 1281096. [Google Scholar] [CrossRef]
- França, T.; Ishikawa, L.; Zorzella-Pezavento, S.; Chiuso-Minicucci, F.; da Cunha, M.; Sartori, A. Impact of malnutrition on immunity and infection. J. Venom. Anim. Toxins Incl. Trop. Dis. 2009, 15, 374–390. [Google Scholar] [CrossRef]
- Savino, W.; Durães, J.; Maldonado-Galdeano, C.; Perdigon, G.; Mendes-da-Cruz, D.A.; Cuervo, P. Thymus, undernutrition, and infection: Approaching cellular and molecular interactions. Front. Nutr. 2022, 9, 948488. [Google Scholar] [CrossRef]
- de Meis, J.; Aurélio Farias-de-Oliveira, D.; Nunes Panzenhagen, P.H.; Maran, N.; Villa-Verde, D.M.S.; Morrot, A.; Savino, W. Thymus Atrophy and Double-Positive Escape Are Common Features in Infectious Diseases. J. Parasitol. Res. 2012, 2012, 574020. [Google Scholar] [CrossRef]
- Rytter, M.J.H.; Kolte, L.; Briend, A.; Friis, H.; Christensen, V.B. The Immune System in Children with Malnutrition—A Systematic Review. PLoS ONE 2014, 9, e105017. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A Review of Micronutrients and the Immune System–Working in Harmony to Reduce the Risk of Infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [PubMed]
- Bono, M.; Tejon, G.; Flores-Santibañez, F.; Fernandez, D.; Rosemblatt, M.; Sauma, D. Retinoic Acid as a Modulator of T Cell Immunity. Nutrients 2016, 8, 349. [Google Scholar] [CrossRef] [PubMed]
- Gürbüz, M.; Aktaç, Ş. Understanding the role of vitamin A and its precursors in the immune system. Nutr. Clin. Métabolisme 2022, 36, 89–98. [Google Scholar] [CrossRef]
- Ross, A.C.; Chen, Q.; Ma, Y. Vitamin A and Retinoic Acid in the Regulation of B-Cell Development and Antibody Production; Elsevier: Amsterdam, The Netherlands, 2011; pp. 103–126. [Google Scholar]
- Munteanu, C.; Schwartz, B. The relationship between nutrition and the immune system. Front. Nutr. 2022, 9, 1082500. [Google Scholar] [CrossRef]
- Schimmer, S.; Sridhar, V.; Satan, Z.; Grebe, A.; Saad, M.; Wagner, B.; Kahlert, N.; Werner, T.; Richter, D.; Dittmer, U.; et al. Iron improves the antiviral activity of NK cells. Front. Immunol. 2025, 15, 1526197. [Google Scholar] [CrossRef]
- Lan, L.; Feng, Z.; Liu, X.; Zhang, B. The roles of essential trace elements in T cell biology. J. Cell. Mol. Med. 2024, 28, e18390. [Google Scholar] [CrossRef]
- Frawley, E.R.; Fang, F.C. The ins and outs of bacterial iron metabolism. Mol. Microbiol. 2014, 93, 609–616. [Google Scholar] [CrossRef]
- Kulik, L.; Maywald, M.; Kloubert, V.; Wessels, I.; Rink, L. Zinc deficiency drives Th17 polarization and promotes loss of Treg cell function. J. Nutr. Biochem. 2019, 63, 11–18. [Google Scholar] [CrossRef]
- Tourkochristou, E.; Triantos, C.; Mouzaki, A. The Influence of Nutritional Factors on Immunological Outcomes. Front. Immunol. 2021, 12, 665968. [Google Scholar] [CrossRef]
- Cheng, F.; Peng, G.; Lu, Y.; Wang, K.; Ju, Q.; Ju, Y.; Ouyang, M. Relationship between copper and immunity: The potential role of copper in tumor immunity. Front. Oncol. 2022, 12, 1019153. [Google Scholar] [CrossRef]
- Franco, J.V.; Bongaerts, B.; Metzendorf, M.-I.; Risso, A.; Guo, Y.; Peña Silva, L.; Boeckmann, M.; Schlesinger, S.; Damen, J.A.; Richter, B.; et al. Undernutrition as a risk factor for tuberculosis disease. Cochrane Database Syst. Rev. 2024, 2025, CD015890. [Google Scholar] [CrossRef]
- Irawan, G.C.; Margawati, A.; Rosidi, A. Underweight increases the risk of pulmonary tuberculosis in adult. Universa Med. 2017, 36, 4. [Google Scholar] [CrossRef]
- Choi, H.; Yoo, J.E.; Han, K.; Choi, W.; Rhee, S.Y.; Lee, H.; Shin, D.W. Body Mass Index, Diabetes, and Risk of Tuberculosis: A Retrospective Cohort Study. Front. Nutr. 2021, 8, 739766. [Google Scholar] [CrossRef]
- Kumar, N.P.; Nancy, A.P.; Moideen, K.; Menon, P.A.; Banurekha, V.V.; Nair, D.; Nott, S.; Babu, S. Low body mass index is associated with diminished plasma cytokines and chemokines in both active and latent tuberculosis. Front. Nutr. 2023, 10, 1194682. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Zhang, Y.; Liu, Q.; Ding, X.; Kong, W.; Zhu, L.; Lu, W. Association of BMI, diabetes, and risk of tuberculosis: A population-based prospective cohort. Int. J. Infect. Dis. 2021, 109, 168–173. [Google Scholar] [CrossRef]
- Cho, S.H.; Lee, H.; Kwon, H.; Shin, D.W.; Joh, H.-K.; Han, K.; Park, J.H.; Cho, B. Association of underweight status with the risk of tuberculosis: A nationwide population-based cohort study. Sci. Rep. 2022, 12, 16207. [Google Scholar] [CrossRef]
- Park, J.; Yoon, J.H.; Ki, H.K.; Eun, Y.; Han, K.; Kim, H. Association of duration of undernutrition with occurrence of tuberculosis. BMC Public Health 2022, 22, 2392. [Google Scholar] [CrossRef]
- Verrest, L.; Wilthagen, E.A.; Beijnen, J.H.; Huitema, A.D.R.; Dorlo, T.P.C. Influence of Malnutrition on the Pharmacokinetics of Drugs Used in the Treatment of Poverty-Related Diseases: A Systematic Review. Clin. Pharmacokinet. 2021, 60, 1149–1169. [Google Scholar] [CrossRef]
- Vonasek, B.J.; Radtke, K.K.; Vaz, P.; Buck, W.C.; Chabala, C.; McCollum, E.D.; Marcy, O.; Fitzgerald, E.; Kondwani, A.; Garcia-Prats, A.J. Tuberculosis in children with severe acute malnutrition. Expert Rev. Respir. Med. 2022, 16, 273–284. [Google Scholar] [CrossRef]
- Seneadza, N.A.H.; Antwi, S.; Yang, H.; Enimil, A.; Dompreh, A.; Wiesner, L.; Peloquin, C.A.; Lartey, M.; Lauzardo, M.; Kwara, A. Effect of malnutrition on the pharmacokinetics of anti-TB drugs in Ghanaian children. Int. J. Tuberc. Lung Dis. 2021, 25, 36–42. [Google Scholar] [CrossRef]
- Petermann, Y.J.; Said, B.; Cathignol, A.E.; Sariko, M.L.; Thoma, Y.; Mpagama, S.G.; Csajka, C.; Guidi, M. State of the art of real-life concentration monitoring of rifampicin and its implementation contextualized in resource-limited settings: The Tanzanian case. JAC-Antimicrobial Resist. 2024, 6, dlae182. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.; Kelley, K.D. Linezolid-Induced Myelosuppression. Ann. Intern. Med. Clin. Cases 2024, 3, e240263. [Google Scholar] [CrossRef]
- Ramappa, V.; Aithal, G.P. Hepatotoxicity Related to Anti-tuberculosis Drugs: Mechanisms and Management. J. Clin. Exp. Hepatol. 2013, 3, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Reshetnyak, V.I.; Maev, I.V. Mechanism for development of malnutrition in primary biliary cholangitis. World J. Meta-Analysis 2022, 10, 81–98. [Google Scholar] [CrossRef]
- Zhuang, L.; Yang, L.; Li, L.; Ye, Z.; Gong, W. Mycobacterium tuberculosis: Immune response, biomarkers, and therapeutic intervention. MedComm 2024, 5, e419. [Google Scholar] [CrossRef]
- Stewart, P.; Patel, S.; Comer, A.; Muneer, S.; Nawaz, U.; Quann, V.; Bansal, M.; Venketaraman, V. Role of B Cells in Mycobacterium Tuberculosis Infection. Vaccines 2023, 11, 955. [Google Scholar] [CrossRef]
- Sia, J.K.; Rengarajan, J. Immunology of Mycobacterium tuberculosis Infections. Microbiol. Spectr. 2019, 7, 10-1128. [Google Scholar] [CrossRef]
- Baazim, H.; Antonio-Herrera, L.; Bergthaler, A. The interplay of immunology and cachexia in infection and cancer. Nat. Rev. Immunol. 2022, 22, 309–321. [Google Scholar] [CrossRef]
- Ding, Y.; Raterink, R.-J.; Marín-Juez, R.; Veneman, W.J.; Egbers, K.; van den Eeden, S.; Haks, M.C.; Joosten, S.A.; Ottenhoff, T.H.M.; Harms, A.C.; et al. Tuberculosis causes highly conserved metabolic changes in human patients, mycobacteria-infected mice and zebrafish larvae. Sci. Rep. 2020, 10, 11635. [Google Scholar] [CrossRef]
- Yen, Y.-F.; Tung, F.-I.; Ho, B.-L.; Lai, Y.-J. Underweight increases the risk of early death in tuberculosis patients. Br. J. Nutr. 2017, 118, 1052–1060. [Google Scholar] [CrossRef]
- Min, J.; Kim, J.S.; Kim, H.W.; Ko, Y.; Oh, J.Y.; Jeong, Y.-J.; Lee, E.H.; Yang, B.; Lee, K.M.; Ahn, J.H.; et al. Effects of underweight and overweight on mortality in patients with pulmonary tuberculosis. Front. Public Health 2023, 11, 1236099. [Google Scholar] [CrossRef]
- Chakhaia, T.; Blumberg, H.M.; Kempker, R.R.; Luo, R.; Dzidzikashvili, N.; Chincharauli, M.; Tukvadze, N.; Avaliani, Z.; Stauber, C.; Magee, M.J. Lack of weight gain and increased mortality during and after treatment among adults with drug-resistant tuberculosis: A retrospective cohort study in Georgia, 2009–2020. ERJ Open Res. 2025; early view. [Google Scholar] [CrossRef]
- Yen, Y.-F.; Chuang, P.-H.; Yen, M.-Y.; Lin, S.-Y.; Chuang, P.; Yuan, M.-J.; Ho, B.-L.; Chou, P.; Deng, C.-Y. Association of Body Mass Index With Tuberculosis Mortality. Medicine 2016, 95, e2300. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Ponnuraja, C.; Gupte, N.; Prakash Babu, S.; Cox, S.R.; Sarkar, S.; Mave, V.; Paradkar, M.; Cintron, C.; Govindarajan, S.; et al. Impact of Undernutrition on Tuberculosis Treatment Outcomes in India: A Multicenter, Prospective, Cohort Analysis. Clin. Infect. Dis. 2023, 76, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Kornfeld, H.; Sahukar, S.B.; Procter-Gray, E.; Kumar, N.P.; West, K.; Kane, K.; Natarajan, M.; Li, W.; Babu, S.; Viswanathan, V. Impact of Diabetes and Low Body Mass Index on Tuberculosis Treatment Outcomes. Clin. Infect. Dis. 2020, 71, e392–e398. [Google Scholar] [CrossRef]
- Bhargava, A.; Chatterjee, M.; Jain, Y.; Chatterjee, B.; Kataria, A.; Bhargava, M.; Kataria, R.; D’Souza, R.; Jain, R.; Benedetti, A.; et al. Nutritional Status of Adult Patients with Pulmonary Tuberculosis in Rural Central India and Its Association with Mortality. PLoS ONE 2013, 8, e77979. [Google Scholar] [CrossRef]
- Birlie, A.; Tesfaw, G.; Dejene, T.; Woldemichael, K. Time to Death and Associated Factors among Tuberculosis Patients in Dangila Woreda, Northwest Ethiopia. PLoS ONE 2015, 10, e0144244. [Google Scholar] [CrossRef]
- Howard, N.C.; Khader, S.A. Immunometabolism during Mycobacterium tuberculosis Infection. Trends Microbiol. 2020, 28, 832–850. [Google Scholar] [CrossRef]
- Shi, L.; Salamon, H.; Eugenin, E.A.; Pine, R.; Cooper, A.; Gennaro, M.L. Infection with Mycobacterium tuberculosis induces the Warburg effect in mouse lungs. Sci. Rep. 2015, 5, 18176. [Google Scholar] [CrossRef]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg Effect: The Metabolic Requirements of Cell Proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef]
- Abhimanyu; Longlax, S.C.; Nishiguchi, T.; Ladki, M.; Sheikh, D.; Martinez, A.L.; Mace, E.M.; Grimm, S.L.; Caldwell, T.; Portillo Varela, A.; et al. TCA metabolism regulates DNA hypermethylation in LPS and Mycobacterium tuberculosis –induced immune tolerance. Proc. Natl. Acad. Sci. USA 2024, 121, e2404841121. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.; Son, H.; Baek, J.-H. Tricarboxylic Acid (TCA) Cycle Intermediates: Regulators of Immune Responses. Life 2021, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Mamadapur, V.K.; Nagaraju, S.; Prabhu, M.M. Comparative Study of Vitamin D Levels in Newly Diagnosed Tuberculosis and a Normal Population. Medicina 2024, 60, 685. [Google Scholar] [CrossRef] [PubMed]
- Pareek, M.; Innes, J.; Sridhar, S.; Grass, L.; Connell, D.; Woltmann, G.; Wiselka, M.; Martineau, A.R.; Kon, O.M.; Dedicoat, M.; et al. Vitamin D deficiency and TB disease phenotype. Thorax 2015, 70, 1171–1180. [Google Scholar] [CrossRef]
- Al-Jaberi, F.A.H.; Crone, C.G.; Lindenstrøm, T.; Arildsen, N.S.; Lindeløv, E.S.; Aagaard, L.; Gravesen, E.; Mortensen, R.; Andersen, A.B.; Olgaard, K.; et al. Reduced vitamin D-induced cathelicidin production and killing of Mycobacterium tuberculosis in macrophages from a patient with a non-functional vitamin D receptor: A case report. Front. Immunol. 2022, 13, 1038960. [Google Scholar] [CrossRef]
- Chung, C.; Silwal, P.; Kim, I.; Modlin, R.L.; Jo, E.-K. Vitamin D-Cathelicidin Axis: At the Crossroads between Protective Immunity and Pathological Inflammation during Infection. Immune Netw. 2020, 20, e12. [Google Scholar] [CrossRef]
- Gough, M.E.; Graviss, E.A.; May, E.E. The dynamic immunomodulatory effects of vitamin D 3 during Mycobacterium infection. Innate Immun. 2017, 23, 506–523. [Google Scholar] [CrossRef]
- DiNardo, A.R.; Rajapakshe, K.; Nishiguchi, T.; Grimm, S.L.; Mtetwa, G.; Dlamini, Q.; Kahari, J.; Mahapatra, S.; Kay, A.; Maphalala, G.; et al. DNA hypermethylation during tuberculosis dampens host immune responsiveness. J. Clin. Investig. 2020, 130, 3113–3123. [Google Scholar] [CrossRef]
- Sharma, G.; Upadhyay, S.; Srilalitha, M.; Nandicoori, V.K.; Khosla, S. The interaction of mycobacterial protein Rv2966c with host chromatin is mediated through non-CpG methylation and histone H3/H4 binding. Nucleic Acids Res. 2015, 43, 3922–3937. [Google Scholar] [CrossRef]
- Kumar, N.P.; Moideen, K.; Banurekha, V.V.; Nair, D.; Babu, S. Plasma Proinflammatory Cytokines Are Markers of Disease Severity and Bacterial Burden in Pulmonary Tuberculosis. Open Forum Infect. Dis. 2019, 6, ofz257. [Google Scholar] [CrossRef]
- Langhans, W.; Hrupka, B.J. Cytokines and Appetite; Springer: Boston, MA, USA, 2003; pp. 167–209. [Google Scholar]
- Pourhassan, M.; Babel, N.; Sieske, L.; Westhoff, T.H.; Wirth, R. Inflammatory cytokines and appetite in older hospitalized patients. Appetite 2021, 166, 105470. [Google Scholar] [CrossRef] [PubMed]
- Costamagna, D.; Costelli, P.; Sampaolesi, M.; Penna, F. Role of Inflammation in Muscle Homeostasis and Myogenesis. Mediat. Inflamm. 2015, 2015, 805172. [Google Scholar] [CrossRef] [PubMed]
- Nizamani, P.; Afridi, H.I.; Kazi, T.G.; Talpur, F.N.; Baig, J.A. Essential trace elemental levels (zinc, iron and copper) in the biological samples of smoker referent and pulmonary tuberculosis patients. Toxicol. Rep. 2019, 6, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Shey-Njila, O.; Hikal, A.F.; Gupta, T.; Sakamoto, K.; Yahyaoui Azami, H.; Watford, W.T.; Quinn, F.D.; Karls, R.K. CtpB Facilitates Mycobacterium tuberculosis Growth in Copper-Limited Niches. Int. J. Mol. Sci. 2022, 23, 5713. [Google Scholar] [CrossRef]
- Zheng, Y.; Chen, H.; Zhang, C.; Hu, D.; Zhao, F.; Piao, W.; Li, S.; Liang, D.; Luo, Z.; Fan, Y.; et al. A community-based cross-sectional study of dietary composition and associated factors among tuberculosis patients in China. Sci. Rep. 2024, 14, 2676. [Google Scholar] [CrossRef]
- Ren, Z.; Zhao, F.; Chen, H.; Hu, D.; Yu, W.; Xu, X.; Lin, D.; Luo, F.; Fan, Y.; Wang, H.; et al. Nutritional intakes and associated factors among tuberculosis patients: A cross-sectional study in China. BMC Infect. Dis. 2019, 19, 907. [Google Scholar] [CrossRef]
- Tugra Ozer, N. The Vicious Cycle of Malnutrition and Tuberculosis: A Narrative Review. J. Clin. Pract. Res. 2024, 46, 444–448. [Google Scholar] [CrossRef]
- Oh, J.; Choi, R.; Park, H.-D.; Lee, H.; Jeong, B.-H.; Park, H.Y.; Jeon, K.; Kwon, O.J.; Koh, W.-J.; Lee, S.-Y. Evaluation of vitamin status in patients with pulmonary tuberculosis. J. Infect. 2017, 74, 272–280. [Google Scholar] [CrossRef]
- Muzembo, B.A.; Mbendi, N.C.; Ngatu, N.R.; Suzuki, T.; Wada, K.; Ikeda, S. Serum selenium levels in tuberculosis patients: A systematic review and meta-analysis. J. Trace Elem. Med. Biol. 2018, 50, 257–262. [Google Scholar] [CrossRef]
- Keflie, T.S.; Samuel, A.; Woldegiorgis, A.Z.; Mihret, A.; Abebe, M.; Biesalski, H.K. Vitamin A and zinc deficiencies among tuberculosis patients in Ethiopia. J. Clin. Tuberc. Other Mycobact. Dis. 2018, 12, 27–33. [Google Scholar] [CrossRef]
- Gebremicael, G.; Alemayehu, M.; Sileshi, M.; Geto, Z.; Gebreegziabxier, A.; Tefera, H.; Ashenafi, N.; Tadese, C.; Wolde, M.; Kassa, D. The serum concentration of vitamin B12 as a biomarker of therapeutic response in tuberculosis patients with and without human immunodeficiency virus (HIV) infection. Int. J. Gen. Med. 2019, 12, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.-P.; Li, R.; Wang, L.-J.; Tang, F.; Li, H.-M. Clinical relevance of vitamin B12 level and vitamin B12 metabolic gene variation in pulmonary tuberculosis. Front. Immunol. 2022, 13, 947897. [Google Scholar] [CrossRef] [PubMed]
- Cioboata, R.; Nicolosu, D.; Balasoiu, A.-T.; Balteanu, M.A.; Zlatian, O.M.; Osman, A.; Biciusca, V.; Tieranu, E.-N.; Mogos, G.F.R.; Ghenea, A.E. Vitamin C and Tuberculosis: Examining the Relationship Between Antioxidant Defense and Disease Severity—Preliminary Findings from a Southwestern Romanian Study. J. Clin. Med. 2024, 13, 6715. [Google Scholar] [CrossRef] [PubMed]
- Cioboata, R.; Balteanu, M.A.; Zlatian, O.M.; Vlasceanu, S.G.; Driga, M.V.P.; Mitroi, D.M.; Catana, O.M.; Buciu, C.I.; Camen, G.; Mirea, A.A. Impact of vitamin C deficiency on imaging patterns and ventilatory function in pulmonary tuberculosis. Front. Med. 2025, 12, 1554723. [Google Scholar] [CrossRef]
- Albors-Vaquer, A.; Rizvi, A.; Matzapetakis, M.; Lamosa, P.; Coelho, A.V.; Patel, A.B.; Mande, S.C.; Gaddam, S.; Pineda-Lucena, A.; Banerjee, S.; et al. Active and prospective latent tuberculosis are associated with different metabolomic profiles: Clinical potential for the identification of rapid and non-invasive biomarkers. Emerg. Microbes Infect. 2020, 9, 1131–1139. [Google Scholar] [CrossRef]
- Li, Y.; Yao, C.; Ji, P.; Wang, H.; Wang, S.; Wang, Y.; Cheng, Q.; Xia, L.; Chen, Y. Plasma dynamic metabolomics during anti-tuberculosis treatment identifies an amino acid panel with diagnostic potential. LabMed Discov. 2025, 2, 100059. [Google Scholar] [CrossRef]
- Vrieling, F.; Ronacher, K.; Kleynhans, L.; van den Akker, E.; Walzl, G.; Ottenhoff, T.H.M.; Joosten, S.A. Patients with Concurrent Tuberculosis and Diabetes Have a Pro-Atherogenic Plasma Lipid Profile. EBioMedicine 2018, 32, 192–200. [Google Scholar] [CrossRef]
- Yi, W.-J.; Han, Y.-S.; Wei, L.-L.; Shi, L.-Y.; Huang, H.; Jiang, T.-T.; Li, Z.-B.; Chen, J.; Hu, Y.-T.; Tu, H.-H.; et al. l-Histidine, arachidonic acid, biliverdin, and l-cysteine-glutathione disulfide as potential biomarkers for cured pulmonary tuberculosis. Biomed. Pharmacother. 2019, 116, 108980. [Google Scholar] [CrossRef]
- Collins, J.M.; Siddiqa, A.; Jones, D.P.; Liu, K.; Kempker, R.R.; Nizam, A.; Shah, N.S.; Ismail, N.; Ouma, S.G.; Tukvadze, N.; et al. Tryptophan catabolism reflects disease activity in human tuberculosis. JCI Insight 2020, 5, e137131. [Google Scholar] [CrossRef]
- Gautam, U.S.; Foreman, T.W.; Bucsan, A.N.; Veatch, A.V.; Alvarez, X.; Adekambi, T.; Golden, N.A.; Gentry, K.M.; Doyle-Meyers, L.A.; Russell-Lodrigue, K.E.; et al. In vivo inhibition of tryptophan catabolism reorganizes the tuberculoma and augments immune-mediated control of Mycobacterium tuberculosis. Proc. Natl. Acad. Sci. USA 2018, 115, E62–E71. [Google Scholar] [CrossRef]
- Felípez, L.; Sentongo, T.A. Drug-Induced Nutrient Deficiencies. Pediatr. Clin. N. Am. 2009, 56, 1211–1224. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J.; Pontefract, S.K. Adverse drug reactions. Clin. Med. 2016, 16, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Prescott, J.D.; Drake, V.J.; Stevens, J.F. Medications and Micronutrients: Identifying Clinically Relevant Interactions and Addressing Nutritional Needs. J. Pharm. Technol. 2018, 34, 216–230. [Google Scholar] [CrossRef] [PubMed]
- Mohn, E.; Kern, H.; Saltzman, E.; Mitmesser, S.; McKay, D. Evidence of Drug–Nutrient Interactions with Chronic Use of Commonly Prescribed Medications: An Update. Pharmaceutics 2018, 10, 36. [Google Scholar] [CrossRef]
- Sankar, J.; Chauhan, A.; Singh, R.; Mahajan, D. Isoniazid-historical development, metabolism associated toxicity and a perspective on its pharmacological improvement. Front. Pharmacol. 2024, 15, 1441147. [Google Scholar] [CrossRef]
- Nabity, S.A.; Mponda, K.; Gutreuter, S.; Surie, D.; Zimba, S.B.; Chisuwo, L.; Moffitt, A.; Williams, A.M.; Sharma, A.J.; Marshall, R.E.; et al. Isoniazid-associated pellagra during mass scale-up of tuberculosis preventive therapy: A case-control study. Lancet Glob. Health 2022, 10, e705–e714. [Google Scholar] [CrossRef]
- Naik, A.L. Effect of DOTS Treatment on Vitamin D Levels in Pulmonary Tuberculosis. J. Clin. Diagn. Res. 2017, 11, BC18–BC22. [Google Scholar] [CrossRef]
- Torres-Fernandez, D.; de Pazos Azpeitia, B.; Gijon Mediavilla, M.; Lopez-Roa, P.; Epalza, C.; Grasa Lozano, C.D.; Blazquez-Gamero, D. Severe Rifampicin-induced Vitamin K Deficiency Coagulopathy in a Child. Pediatr. Infect. Dis. J. 2020, 39, 833–834. [Google Scholar] [CrossRef]
- Leung, C.; Warner, J.; Harris, M.; Nourse, C. Symptomatic Hypocalcemia Secondary to Rifampicin-induced Hypovitaminosis D. Pediatr. Infect. Dis. J. 2016, 35, 822–823. [Google Scholar] [CrossRef]
- Gopal, P.; Nartey, W.; Ragunathan, P.; Sarathy, J.; Kaya, F.; Yee, M.; Setzer, C.; Manimekalai, M.S.S.; Dartois, V.; Grüber, G.; et al. Pyrazinoic Acid Inhibits Mycobacterial Coenzyme A Biosynthesis by Binding to Aspartate Decarboxylase PanD. ACS Infect. Dis. 2017, 3, 807–819. [Google Scholar] [CrossRef]
- Kim, J.; Ahn, S.J. Risk Factors of Optic Neuropathy in Ethambutol Users: Interaction with Isoniazid and Other Associated Conditions of Toxic Optic Neuropathy. Toxics 2024, 12, 549. [Google Scholar] [CrossRef]
- Patel, J.; Patel, C.; Shah, A.; Shah, P.; Pandya, S.; Sojitra, B. Ethambutol-Induced Optic Neuritis and Vision Loss: A Case Report. Cureus 2024, 16, e64873. [Google Scholar] [CrossRef] [PubMed]
- Godad, A.; Ansari, A.; Bhatia, N.; Ali, A.; Zine, S.; Doshi, G. Drug nutraceutical interactions. In Industrial Application of Functional Foods, Ingredients and Nutraceuticals; Elsevier: Amsterdam, The Netherlands, 2023; pp. 663–723. [Google Scholar]
- Gupta, Y.; Shah, I. Ethionamide-induced Pellagra. J. Trop. Pediatr. 2015, 61, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Shvets, O.M.; Shevchenko, O.S.; Todoriko, L.D.; Tovazhnyanska, O.L.; Dubynska, O.I.; Ostrovskyi, M.M.; Makoyda, I.Y.; Yeremenchuk, I.V. Changes of vitamins B1, B12 as predicting factors of peripheral polyneuropathy in pulmonary tuberculosis patients. Arch. Balk. Med. Union 2020, 55, 113–120. [Google Scholar] [CrossRef]
- Kenreigh, C.; Vazquez, J.A.; Arnold, A.; Swanson, R.; Biswas, P.; Bassetti, M. Safety of long-term use of linezolid: Results of an open-label study. Ther. Clin. Risk Manag. 2016, 12, 1347–1354. [Google Scholar] [CrossRef]
- Campbell, R.E.; Chen, C.H.; Edelstein, C.L. Overview of Antibiotic-Induced Nephrotoxicity. Kidney Int. Rep. 2023, 8, 2211–2225. [Google Scholar] [CrossRef]
- Szeto, W.; Garcia-Buitrago, M.T.; Abbo, L.; Rosenblatt, J.D.; Moshiree, B.; Morris, M.I. Clofazimine Enteropathy: A Rare and Underrecognized Complication of Mycobacterial Therapy. Open Forum Infect. Dis. 2016, 3, ofw004. [Google Scholar] [CrossRef]
- Chong, R.Q.; Gelissen, I.; Chaar, B.; Penm, J.; Cheung, J.M.; Harnett, J.E. Do medicines commonly used by older adults impact their nutrient status? Explor. Res. Clin. Soc. Pharm. 2021, 3, 100067. [Google Scholar] [CrossRef]
- Chan, L. Drug-Nutrient Interactions. J. Parenter. Enter. Nutr. 2013, 37, 450–459. [Google Scholar] [CrossRef]
- Court, R.; Centner, C.M.; Chirehwa, M.; Wiesner, L.; Denti, P.; de Vries, N.; Harding, J.; Gumbo, T.; Maartens, G.; McIlleron, H. Neuropsychiatric toxicity and cycloserine concentrations during treatment for multidrug-resistant tuberculosis. Int. J. Infect. Dis. 2021, 105, 688–694. [Google Scholar] [CrossRef]
- Mergenhagen, K.A.; Wattengel, B.A.; Skelly, M.K.; Clark, C.M.; Russo, T.A. Fact versus Fiction: A Review of the Evidence behind Alcohol and Antibiotic Interactions. Antimicrob. Agents Chemother. 2020, 64, e02167-19. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, K.; Claus, S.P.; Lindon, J.C.; Holmes, E.; Everett, J.R.; Nicholson, J.K.; Coen, M. Pharmacometabonomic Characterization of Xenobiotic and Endogenous Metabolic Phenotypes That Account for Inter-individual Variation in Isoniazid-Induced Toxicological Response. J. Proteome Res. 2012, 11, 4630–4642. [Google Scholar] [CrossRef] [PubMed]
- Walden, D.M.; Khotimchenko, M.; Hou, H.; Chakravarty, K.; Varshney, J. Effects of Magnesium, Calcium, and Aluminum Chelation on Fluoroquinolone Absorption Rate and Bioavailability: A Computational Study. Pharmaceutics 2021, 13, 594. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.K.H.; Chandrasekaran, V.; Kumar, A.K.; Kawaskar, M.; Lavanya, J.; Swaminathan, S.; Ramachandran, G. Food significantly reduces plasma concentrations of first-line anti-tuberculosis drugs. Indian J. Med. Res. 2017, 145, 530–535. [Google Scholar] [CrossRef]
- Bushra, R.; Aslam, N.; Khan, A. Food Drug Interactions. Oman Med. J. 2011, 26, 77–83. [Google Scholar] [CrossRef]
- KANEKO, T.; ISHIGATSUBO, Y. Isoniazid and Food Interactions: —Fish, Cheese, and Wine. Intern. Med. 2005, 44, 1120–1121. [Google Scholar] [CrossRef]
- Umut, G.; Dernek, B.; Kucukparlak, I.; Aydin, T.; Karamustafalioglu, N.; Kesiktas, F.N. Acute psychotic attack under isoniazid treatment: A case report. Dusunen Adam J. Psychiatry Neurol. Sci. 2016, 38, 379–381. [Google Scholar] [CrossRef]
- Rumore, M.M.; Roth, M.; Orfanos, A. Dietary Tyramine Restriction for Hospitalized Patients on Linezolid. Nutr. Clin. Pract. 2010, 25, 265–269. [Google Scholar] [CrossRef]
- Won, C.S.; Oberlies, N.H.; Paine, M.F. Mechanisms underlying food–drug interactions: Inhibition of intestinal metabolism and transport. Pharmacol. Ther. 2012, 136, 186–201. [Google Scholar] [CrossRef]
- Aðalbjörnsson, B.V.; Ramel, A. Food-Drug Interaction in Older Adults; Springer: Cham, Switzerland, 2021; pp. 249–259. [Google Scholar]
- Boullata, J.I.; Hudson, L.M. Drug–Nutrient Interactions: A Broad View with Implications for Practice. J. Acad. Nutr. Diet. 2012, 112, 506–517. [Google Scholar] [CrossRef]
- Gunturu, S.G.; Dharmarajan, T.S. Drug–Nutrient Interactions. In Geriatric Gastroenterology; Springer International Publishing: Cham, Switzerland, 2021; pp. 381–408. [Google Scholar]
- World Health Organization. Guideline: Nutritional Care and Support for Patients with Tuberculosis; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Module 1: Prevention—Infection prevention and control. In WHO Operational Handbook on Tuberculosis; WHO: Geneva, Switzerland, 2023; ISBN 978-92-4-007815-4. [Google Scholar]
- Amagon, K.I.; Awodele, O.; Akindele, A.J. Methionine and vitamin B-complex ameliorate antitubercular drugs-induced toxicity in exposed patients. Pharmacol. Res. Perspect. 2017, 5, e00360. [Google Scholar] [CrossRef] [PubMed]
- Ockenga, J.; Fuhse, K.; Chatterjee, S.; Malykh, R.; Rippin, H.; Pirlich, M.; Yedilbayev, A.; Wickramasinghe, K.; Barazzoni, R. Tuberculosis and malnutrition: The European perspective. Clin. Nutr. 2023, 42, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Bhargava, M.; Carwile, M.E.; Dauphinais, M.R.; Tisile, P.; Cintron, C.; Locks, L.M.; Hauser, J.; Oliver, M.; Heysell, S.K.; et al. A roadmap for integrating nutritional assessment, counselling, and support into the care of people with tuberculosis. Lancet Glob. Health 2025, 13, e967–e973. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A.; Bhargava, M.; Meher, A.; Teja, G.S.; Velayutham, B.; Watson, B.; Benedetti, A.; Barik, G.; Singh, V.P.; Singh, D.; et al. Nutritional support for adult patients with microbiologically confirmed pulmonary tuberculosis: Outcomes in a programmatic cohort nested within the RATIONS trial in Jharkhand, India. Lancet Glob. Health 2023, 11, e1402–e1411. [Google Scholar] [CrossRef]
- Singh, A.K.; Siddhanta, A.; Goswami, L. Improving tuberculosis treatment success rate through nutrition supplements and counselling: Findings from a pilot intervention in India. Clin. Epidemiol. Glob. Health 2021, 11, 100782. [Google Scholar] [CrossRef]
- Sayem, M.A.; Hossain, M.G.; Ahmed, T.; Hossain, K.; Saud, Z.A. Effect of Nutritional Support on Treatment of Multi-Drug Resistant Tuberculosis in Rajshahi Division, Bangladesh. J. Tuberc. Res. 2020, 08, 223–236. [Google Scholar] [CrossRef]
- Shah, V.; Murugan, Y.; Patel, S.S.; Trivedi, N.S.; Pithadiya, D.; Makwana, N.; Parmar, D. Nutritional Supplementation in Tuberculosis Treatment: A Mixed Methods Study of Clinical Outcomes and Patient Perceptions in Jamnagar, India. Cureus 2024, 16, e70300. [Google Scholar] [CrossRef]
- Kouhpayeh, H. Different diets and their effect on tuberculosis prevention in HIV patients. J. Fam. Med. Prim. Care 2022, 11, 1369–1376. [Google Scholar] [CrossRef]
- Engoru, S.; Bajunirwe, F.; Izudi, J. Malnutrition and unsuccessful tuberculosis treatment among people with multi-drug resistant tuberculosis in Uganda: A retrospective analysis. J. Clin. Tuberc. Other Mycobact. Dis. 2024, 37, 100477. [Google Scholar] [CrossRef]
- Dlatu, N.; Faye, L.M.; Apalata, T. Outcomes of Treating Tuberculosis Patients with Drug-Resistant Tuberculosis, Human Immunodeficiency Virus, and Nutritional Status: The Combined Impact of Triple Challenges in Rural Eastern Cape. Int. J. Environ. Res. Public Health 2025, 22, 319. [Google Scholar] [CrossRef]
- Bhargava, A.; Bhargava, M.; Velayutham, B.; Thiruvengadam, K.; Watson, B.; Kulkarni, B.; Singh, M.; Dayal, R.; Pathak, R.R.; Mitra, A.; et al. The RATIONS (Reducing Activation of Tuberculosis by Improvement of Nutritional Status) study: A cluster randomised trial of nutritional support (food rations) to reduce TB incidence in household contacts of patients with microbiologically confirmed pulmon. BMJ Open 2021, 11, e047210. [Google Scholar] [CrossRef]
- Yang, Y.; Cai, J.; Wang, X.; Zhao, K.; Lei, Z.; Han, W.; Yin, X.; Yan, K.; Hu, Y.; Zhang, B.; et al. Nutritional supplementation during tuberculosis treatment to improve clinical symptoms: A double-blinded placebo-controlled randomized trial. Food Funct. 2025, 16, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Benzekri, N.A.; Sambou, J.F.; Tamba, I.T.; Diatta, J.P.; Sall, I.; Cisse, O.; Thiam, M.; Bassene, G.; Badji, N.M.; Faye, K.; et al. Nutrition support for HIV-TB co-infected adults in Senegal, West Africa: A randomized pilot implementation study. PLoS ONE 2019, 14, e0219118. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.U.; Khan, F.U.; Aqeel, M.T.; Hayat, K.; Chang, J.; Rehman, A.u.; Fang, Y. A randomized controlled trial to evaluate the impact of pharmacist-led clinical interventions on the health-related quality of life among TB patients. Front. Pharmacol. 2023, 14, 1171985. [Google Scholar] [CrossRef] [PubMed]
- Campos-Pardos, E.; Uranga, S.; Picó, A.; Gómez, A.B.; Gonzalo-Asensio, J. Dependency on host vitamin B12 has shaped Mycobacterium tuberculosis Complex evolution. Nat. Commun. 2024, 15, 2161. [Google Scholar] [CrossRef]
- Bistrian, B.R. Nutritional Assessment. In Goldman’s Cecil Medicine; Elsevier: Amsterdam, The Netherlands, 2012; pp. 1384–1388. [Google Scholar]
- Ramakrishnan, U.; Casanova, I.G. Nutrition epidemiology for developing countries. In Public Health in Developing Countries; Woodhead Publishing Limited: Sawston, UK; pp. 25–49.
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef]
- Butnaru, T.; Mihaltan, F.; Constantin, A. Quality of life of romanian patients with sensitive and drug-resistant tuberculosis during and after treatment. Farmacia 2024, 72, 675–687. [Google Scholar] [CrossRef]
- Ramos, J.P.; Vieira, M.; Pimentel, C.; Argel, M.; Barbosa, P.; Duarte, R. Building bridges: Multidisciplinary teams in tuberculosis prevention and care. Breathe 2023, 19, 230092. [Google Scholar] [CrossRef]
- Myburgh, H.; Baloyi, D.; Loveday, M.; Meehan, S.-A.; Osman, M.; Wademan, D.; Hesseling, A.; Hoddinott, G. A scoping review of patient-centred tuberculosis care interventions: Gaps and opportunities. PLoS Glob. Public Health 2023, 3, e0001357. [Google Scholar] [CrossRef]
- Wagnew, F.; Gray, D.; Tsheten, T.; Kelly, M.; Clements, A.C.A.; Alene, K.A. Effectiveness of nutritional support to improve treatment adherence in patients with tuberculosis: A systematic review. Nutr. Rev. 2024, 82, 1216–1225. [Google Scholar] [CrossRef]
- Xu, L.; Wang, J.; Zhao, S.; Zhang, J.; Xiong, K.; Cai, J.; Wang, Q.; Lin, S.; Ma, Y.; Ma, A. Increased vegetable and fruit intake is associated with reduced failure rate of tuberculosis treatment: A hospital-based cohort study in China. Br. J. Nutr. 2021, 125, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Saqlain, M.; Tanveer, M.; Blebil, A.Q.; Dujaili, J.A.; Hasan, S.S. The impact of clinical pharmacist services on patient health outcomes in Pakistan: A systematic review. BMC Health Serv. Res. 2021, 21, 859. [Google Scholar] [CrossRef] [PubMed]
- Awad, K.; Jaam, M.; Awaisu, A.; Stewart, D.; Rathore, H.A.; Abdul Hadi, M. Impact of pharmaceutical care interventions in improving clinical outcomes among patients with pulmonary tuberculosis: A systematic review. J. Pharm. Policy Pract. 2024, 17, 2305770. [Google Scholar] [CrossRef] [PubMed]
- Ihm, S.H.; Kim, K.-I.; Lee, K.J.; Won, J.W.; Na, J.O.; Rha, S.-W.; Kim, H.-L.; Kim, S.-H.; Shin, J. Interventions for Adherence Improvement in the Primary Prevention of Cardiovascular Diseases: Expert Consensus Statement. Korean Circ. J. 2022, 52, 1. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Design and Population Characteristics | BMI Categories Analysed | Outcome Measured | Confounders Adjusted For | Key Findings | Limitations | Reference |
|---|---|---|---|---|---|---|
| Case–control study, Central Java, Indonesia, 2016; 57 adults aged 19–63 years (19 TB cases, 38 controls); 52.6% female | <18.5 (underweight), 18.5–24.9 (normal), >25 (overweight) | TB incidence (based on AFB and chest X-ray) | Energy, protein, vitamins A/C/selenium intake, smoking, income, education, DM history | BMI <18.5: OR 6.0 (95% CI 1.32–27.18); underweight most influential risk factor | Small sample (n = 57), recall bias (FFQ), no biochemical validation of nutrients or albumin, limited generalizability | [77] |
| Retrospective cohort, South Korea, 2009–2018; 10,087,903 adults from national screening; age ≥20, 52% male | <18.5, 18.5–22.9 (ref), 23.0–24.9, 25.0–29.9, ≥30 kg/m2 (Asia-Pacific criteria); stratified by DM status | TB incidence (RID registration); 7.3-year follow-up | Age, sex, smoking, alcohol, physical activity, income, hypertension, dyslipidemia | Underweight: aHR 2.21 (2.14–2.28) in non-DM; aHR 3.24 (2.95–3.56) in DM; stronger effect in age <65, smokers, drinkers | BMI measured once; Korean population; possible diagnostic miscoding; no latent TB or clinical progression data | [78] |
| Cross-sectional study, India, 2023; 253 PTB (127 LBMI, 126 NBMI) and 176 LTB (71 LBMI, 105 NBMI); age 18–65; HIV and DM excluded | <18.5 (LBMI), 18.5–24.9 (NBMI) | Immune markers in TB and LTB | HIV, DM excluded; no adjustment for others | LBMI associated with ↓ IFNγ, IL-2, TNFα, IL-12, IL-6, CXCL9, CXCL10 (in PTB and LTB); ↑ IL-10, TGFβ; impaired immunity may ↑ TB susceptibility | Cross-sectional (no causality), no TB incidence data, no adjustment for SES or lifestyle, gender imbalance in PTB | [79] |
| Prospective cohort, Eastern China, 2013–2021; 27,807 adults; median age 50; ~50% female | ≤24 vs. >24 kg/m2; BMI as continuous variable also analysed | TB incidence (confirmed via national registry) | Age, sex, BMI, smoking, alcohol, BCG vaccination, diabetes | Lower BMI ↑ TB risk: per 1 unit ↓ BMI, aHR 0.84 (0.77–0.91); BMI ≤ 24 + diabetes → aHR 2.68 (1.32–5.43); BMI > 24 neutralised DM risk | BMI only at baseline; no HIV data; diabetes self-reported; Jiangsu-only registry—possible missed TB if moved away | [80] |
| Prospective cohort, South Korea, 2010–2017; 11,135,332 adults ≥20 y from NHIS screening database; 69.3% of underweight were female; mean age underweight 40.8 y | <18.5 (underweight), 18.5–22.9 (normal), 23.0–24.9 (overweight), ≥25 (obese); underweight further split: 17.0–18.4, 16.0–16.9, <16.0 | TB incidence (national registry) | Age, sex, smoking, alcohol, exercise, income, hypertension, diabetes, dyslipidemia | BMI <18.5 → aHR 2.08 (2.02–2.15); mild thinness aHR 1.98, moderate 2.50, severe 2.83 vs. normal; log-linear inverse BMI–TB risk | TB type not stratified; only baseline BMI; generalizability limited to high-income settings; underweight may reflect other risks | [81] |
| Retrospective cohort, South Korea, 2006–2017; 2,396,434 adults; 7.27-year median follow-up; ~22% female in underweight group, younger population | BMI <18.5 (underweight); 0 to 4 accumulated episodes of underweight across 4 years | TB incidence (new diagnosis based on national registry) | Age, sex, diabetes, hypertension, dyslipidemia; stratified by sex, age, WC | TB risk ↑ with more years underweight: aHR 3.33 (3.00–3.84) for 4× underweight vs. 0×; stronger in women and those <65 years | BMI not consecutive; no HIV data; body composition not analyzed; mostly Korean subjects; no severe underweight (<16) subgroup analyzed | [82] |
| Study Design and Population Characteristics | BMI Categories Analysed | Mortality Outcome | Key Findings | Confounders Adjusted For | Adherence Support | Limitations | Reference |
|---|---|---|---|---|---|---|---|
| Retrospective cohort, Taiwan, 2012–2014; 2410 adults with TB; age ≥ 18, mean age 64.5 years, 67.1% men | <18.5 (underweight), 18.5–24.9 (normal), ≥25 (overweight) | TB-specific and non-TB-specific mortality during treatment; early (<8 weeks) and late (>8 weeks); mortality: Underweight 24.2%, Normal 14.0%, Overweight 10.4% | Underweight ↑ all-cause mortality (AHR 1.57, CI 1.26–1.95), TB-specific (AHR 1.85, CI 1.03–3.33), non-TB-specific (AHR 1.52, CI 1.19–1.95); strongest effect in first 8 weeks: TB-specific AHR 2.23 (CI 1.09–4.59), non-TB-specific AHR 1.81 (CI 1.29–2.55) | Age, sex, education, marital status, unemployment, smoking, alcohol, diabetes, ESRD, malignancy, AFB smear, TB culture, CXR findings, DOT, extrapulmonary TB | Yes—DOTS (Directly Observed Treatment Short-Course) program applied to most | BMI self-reported, only baseline value; retrospective design; some clinical data not collected (e.g., IV drug use); limited generalizability beyond Taiwan | [95] |
| Prospective cohort, Korea, 2019–2020; 9721 patients with pulmonary TB; mean age 61.8 years, 36.5% female | Underweight < 18.5, Normal 18.5–22.9, Overweight ≥ 23 (Asian cut-offs) | All-cause, TB-related, non-TB-related mortality during anti-TB treatment; underweight mortality 19.3%, normal 10.0%, overweight 8.2% | Underweight ↑ mortality: all-cause aOR 1.95 (1.67–2.27), TB-related aOR 2.06 (1.55–2.74); Overweight protective (e.g., TB-related death aOR 0.69, 95% CI 0.48–0.99) | Age, sex, smoking, heavy alcohol, comorbidities (e.g., diabetes, heart/lung/kidney/liver disease, malignancy) | Yes—PPM program with TB nurse monitoring until treatment end | No inflammatory biomarkers; generalizability limited (low HIV prevalence, high-income country); BMI only at baseline | [96] |
| Retrospective cohort, Georgia, 2009–2020; 720 adults with M/XDR-TB; median age 35.5 (IQR: 26.5–49.0), 68.8% male | <18.5 (low), 18.5–24.9 (normal), ≥25 (high); BMI change during first 3–6 months categorized as negative, no change, positive | All-cause mortality during and after treatment; 16 died during (2.2%), 50 post-treatment (6.9%) | No BMI gain in low BMI group ↑ post-TB mortality (aHR 4.99, CI 1.25–19.94); weight loss in normal BMI ↑ mortality during treatment (aHR 5.25, CI 1.31–21.10) | Age, gender, year of treatment initiation, baseline sputum smear, chest X-ray cavitation | Yes—DOT program (directly observed therapy) | 34.8% excluded for missing BMI follow-up; no data on severity biomarkers or treatment regimens; retrospective design limits causality | [97] |
| Retrospective cohort, Taipei, Taiwan, 2011–2012; 1608 adults with TB; age 18–112 (mean 64.6), 67.5% male | <18.5 (underweight), 18.5–24.9 (normal), ≥25 (overweight) | TB-specific, non-TB-specific, and all-cause mortality during treatment; underweight death rate 24.4%, normal 14.2%, overweight 10.3% | Underweight ↑ all-cause mortality (AOR 1.66, CI 1.21–2.30), TB-specific (AOR 2.14, CI 1.18–3.89), non-TB-specific (AOR 1.58, CI 1.11–2.25); effect only in males: TB-specific AOR 2.37 (CI 1.19–4.72) | Age, sex, education, unemployment, AFB smear, pleural effusion, ESRD, malignancy | Not mentioned | BMI only at baseline; 25.7% TB diagnosed clinically, possible overdiagnosis; retrospective design; missing info (e.g., IV drug use) | [98] |
| Prospective cohort, India, 2015–2019; 2931 adults with drug-sensitive pulmonary TB from 5 academic sites; age >18; 70.8% male | <16, 16–16.99, 17–18.49, 18.5–22.99 (ref), ≥23; also premorbid BMI (same cut-offs); BMI change after 2 months | All-cause mortality; part of composite outcome (death, treatment failure, relapse); 3.4% died | BMI < 16 at treatment start: aIRR 2.05 (1.42–2.98); premorbid BMI < 16: aIRR 2.20 (1.16–3.94); unchanged/decreased BMI after 2 months: aIRR 5.16 (1.51–17.65); severe stunting: aIRR 1.52 (1.00–2.24) | Age, sex, symptom duration, sputum smear grade, smoking, alcohol use disorder, diabetes, HIV status | Not mentioned; no objective adherence measurement | Self-reported premorbid weight (recall bias); no adherence data; variable diabetes definitions; possible residual confounding; limited generalizability outside India | [99] |
| Prospective cohort, India (Chennai), 2014–2018; 389 adults with drug-sensitive pulmonary TB, aged 25–60; 256 with diabetes, 133 with normal glucose tolerance | BMI < 18.5 vs. ≥18.5; HbA1c < 8.0% vs. ≥8.0% used for subgrouping; 4 groups: BMIlo/A1clo, BMIlo/A1chi, BMIhi/A1clo, BMIhi/A1chi | All-cause mortality and treatment failure (composite outcome); BMIlo/A1clo had worst outcomes | BMI < 18.5 strongest predictor of failure/death: aOR 4.99 (1.77–11.36); paradoxical protective effect of DM with HbA1c ≥ 8.0 in underweight: aOR 1.48 (0.42–5.19); VAI > 5.0: OR 13.5 (1.4–135.0) in underweight | Age, sex, income, height, smoking, alcohol use | Yes—Treatment under national TB program (not directly measured) | Small subgroups; adherence not objectively assessed; no detailed nutrition data; no vitamin A or insulin resistance markers; population-specific metabolic effects may not generalize | [100] |
| Retrospective cohort, India, 2004–2009; 1695 adults with pulmonary TB, rural setting; median age 38, 68% men | <16 (severe), 16–16.99 (moderate), 17–18.49 (mild), 18.5–24.9 (normal); continuous BMI also used | TB-related mortality during treatment; 60 deaths among 1179 treated (5.1%) | BMI < 16 → 2-fold ↑ TB death risk; BMI 13 → aOR 3.9 (CI 1.7–8.3); each 1 unit ↑ BMI → aOR 0.78 (CI 0.68–0.90); effect stronger in men | Age, sex, weight, height, smear status, HIV status, treatment history | Daily self-administered therapy at low cost; counselling; DOT not mentioned | Retrospective; no data on disease extent or adherence; some missing heights; limited generalizability; chronic undernutrition prevalent | [101] |
| Retrospective cohort, Ethiopia, 2008–2012; 810 adult TB patients; mean age 32.4, 61% EPTB, 18.3% HIV+ | Body weight < 35 kg vs. ≥35 kg (BMI not used) | All-cause mortality during treatment; 60 deaths (7.4%), 56.7% in intensive phase | Weight < 35 kg → AHR 3.90 (CI 1.63–9.33); age and HIV status also significant predictors | Age, sex, type of TB, HIV status, ART use | Yes—DOTS program in all clinics | Body weight not BMI; limited data on comorbidities and MDR-TB; retrospective design; possible underreporting of causes | [102] |
| Nutrient | Clinical Impact | Aetiology and Mechanisms | Reference |
|---|---|---|---|
| Energy (Calories) | Weight loss, fatigue, decreased physical function | Elevated basal metabolic rate; reduced appetite; nutrient malabsorption | [119,120] |
| Protein | Muscle wasting, impaired immunity, delayed recovery | Increased catabolism due to systemic inflammation; anorexia leading to reduced intake; anabolic block, where dietary protein is used more for energy than for tissue synthesis | [121,122,123] |
| Copper | Anaemia, neutropenia, impaired immune response, neurological symptoms | Host macrophages increase copper concentration in phagosomes to combat M. tuberculosis; the bacterium counters by upregulating copper efflux pumps (e.g., CtpV) and metallothioneins (e.g., MymT), leading to disrupted host copper homeostasis and potential systemic deficiency | [119,120] |
| Iron | Anaemia, reduced oxygen transport | Anaemia of chronic disease due to inflammation; iron sequestration; decreased absorption | [119,124] |
| Selenium | Weakened antioxidant defence, increased oxidative damage | Reduced intake; increased utilisation during oxidative stress | [125] |
| Vitamin A | Impaired mucosal immunity, increased infection risk | Decreased intake, malabsorption, increased urinary loss, and the acute phase response reducing serum levels | [124,126,127] |
| Vitamin B12 | Megaloblastic anaemia, peripheral neuropathy, cognitive disturbances, fatigue | Reduced dietary intake due to anorexia; malabsorption from gastrointestinal involvement | [127,128] |
| Vitamin C | Impaired collagen synthesis, delayed wound healing | Increased oxidative stress depletes stores; reduced intake due to anorexia | [129,130] |
| Vitamin D | Compromised macrophage function, increased susceptibility to infection, increased risk of disseminated TB | Limited sun exposure, decreased dietary intake, and inflammation-induced sequestration; reduced innate immunity and antimicrobial peptide synthesis; associated with more severe TB phenotypes and extrapulmonary disease in vitamin D-deficient individuals | [124] |
| Vitamin E | Reduced antioxidant capacity, increased cellular damage | Enhanced oxidative stress from chronic inflammation; decreased dietary intake | [124] |
| Zinc | Impaired immune response, delayed wound healing | Redistribution during acute phase response; decreased intake; increased losses | [119,126] |
| Alanine | Impaired energy metabolism; muscle wasting; fatigue and reduced exercise tolerance | Catabolised by Mtb as a nitrogen and carbon source; restored after TB therapy due to reduced Mtb demand; restored host protein metabolism | [131,132] |
| Glutamine | Suppressed immune response; increased oxidative stress; higher risk of secondary infections | Used by both Mtb (nitrogen source) and host immune cells (ATP and cytokines); restored after TB therapy | [131,132] |
| Histidine | Anaemia and fatigue; impaired antioxidant capacity; altered inflammation regulation | Used in host immune response; altered in wasting syndrome; restored after TB therapy due to restored protein metabolism and reduced inflammatory burden | [133,134] |
| Lysine | Reduced wound healing capacity; impaired immune response; muscle catabolism and weight loss | Rapidly metabolised as a nitrogen donor for Mtb | [131] |
| Tryptophan | Depression, mood disturbances, sleep disorders; immunosuppression via kynurenine pathway activation | Catabolised to kynurenine via IDO1; suppresses T-cell proliferation; restored after TB therapy due to Reduced IDO1 activity; immune reactivation | [135,136] |
| Drug | Nutritional Deficiency | Mechanism | Reference |
|---|---|---|---|
| Isoniazid | Vitamin B6 | isoniazid binds to pyridoxal 5′-phosphate (active form of vitamin B6) → inactivation → depletion → impairs neurotransmitter synthesis (GABA) → risk: peripheral neuropathy and seizures | [141] |
| Vitamin B3 | isoniazid inhibits tryptophan → niacin conversion by interfering with vitamin B6-dependent enzymes + directly disrupts intracellular niacin synthesis → pellagra | [142] | |
| Vitamin D | impairs 25-hydroxylation → impaired vitamin D action | [143] | |
| Rifampicin | Vitamin K | very rare, possibly by disrupting the vitamin K cycle | [144] |
| Vitamin D | rifampin induces P450 → accelerates vitamin D metabolization into inactive forms → reduces circulating levels of 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D → deficiency | [145] | |
| Pyrazinamide | Coenzyme A | pyrazinoic acid inhibits the aspartate decarboxylase (needed for β-alanine biosynthesis, precursor of vitamin B5 → disrupts coenzyme A synthesis | [146] |
| Ethambutol | Zinc | ethambutol chelates zinc → reduced absorption and increased urinary excretion → to zinc deficiency → optic neuropathy. | [147] |
| Copper | ethambutol binds to copper → deficiency → altered mitochondrial function and oxidative phosphorylation → optic nerve damage. | [148] | |
| Vitamin B1 | prolonged use → decreased vitamin B1 levels → optic neuropathy. | [147] | |
| Vitamin E | prolonged use → decreased vitamin E levels → optic neuropathy | [147] | |
| Cycloserine | Vitamin B6 | cycloserine forms an inactive covalently bound complex with pyridoxal 5′-phosphate → a functional vitamin B6 deficiency → anaemia and peripheral neuropathy | [149] |
| Ethionamide | Vitamin B6 | rare, neurotoxic effects | [150] |
| Linezolid | Vitamins B1, B9, B12 | prolonged use → deficiencies → peripheral neuropathy and haematological abnormalities | [151,152] |
| Aminoglycosides | Magnesium, calcium, potassium | renal tubular dysfunction → increased excretion of magnesium and calcium | [153] |
| Clofazimine | Vitamins A, D, E, K, B9, B12 | causes crystal-storing histiocytosis → damages the intestinal mucosa → villous blunting, inflammation, and loss of absorptive surface area → impaired absorption of vitamins A, D, E, K, B9, B12 | [154] |
| Nutrient/Food | Drug | Mechanism | Reference |
|---|---|---|---|
| Alcohol | cycloserine | neurotoxicity risk: seizures and psychosis | [157] |
| isoniazid, ethionamide, PAS, pyrazinamide, rifampin, ethionamide | hepatotoxicity: additive effects on hepatic metabolism | [158] | |
| Caffeine (coffee, tea, cola, chocolate) | isoniazid | central nervous system stimulation; isoniazid inhibits the metabolism of caffeine; heightened side effects: restlessness, insomnia, increased heart rate | [159] |
| Dairy products, iron supplements | fluoroquinolones | reduced absorption: calcium, magnesium, aluminium, and iron can bind to fluoroquinolones, forming insoluble complexes | [160] |
| Food | isoniazid, rifampicin | notable reductions in drug exposures and peak concentrations, a delay in reaching peak drug concentrations | [161] |
| bedaquiline, cycloserine, ethionamide, delamanid, PAS, pretomanid | improved gastrointestinal tolerance | [162] | |
| Histamine-rich foods (certain fish like tuna, mackerel, salmon) | isoniazid | DAO inhibition; histamine accumulation: flushing, hypotension, gastrointestinal discomfort. | [163] |
| Tyramine-rich foods (aged cheeses, cured meats, soy products, red wine) | isoniazid | MAO inhibition; elevated tyramine levels, resulting in headache, flushing, palpitations, and hypertension | [164] |
| linezolid | Hypertensive crisis risk: hypertensive crises. | [165] |
| Study Design and Population Characteristics | Nutritional Intervention | Impact on Outcome | Reference |
|---|---|---|---|
| Cluster randomized trial, Jharkhand (India); ~2800 adult TB patients and ~11,200 household contacts (HHCs); 2-year follow-up | Index patients: monthly food basket (1200 kcal, 52 g protein/day), multivitamins; HHCs in intervention arm: 750 kcal, 23 g protein/day + multivitamins; both groups received nutritional counselling | Primary: reduction in TB incidence among HHCs; Secondary: improved nutritional status, reduced infections and mortality, improved treatment adherence and performance status in patients; final outcomes pending trial completion | [182] |
| Double-blind placebo-controlled RCT, China (Weifang); 329 adults (aged 18–80) with pulmonary TB + prediabetes or diabetes; 6-month follow-up | Daily nutrition package (112 kcal, 9.1 g protein, macro + 13 vitamins/minerals incl. A, B1, B2, B6, B12, C, D, E, folate, niacin, iron, Ca, Zn); vs. placebo (same calories, 3 g protein, no micronutrients) | ↓ Chest pain, expectoration, and anaemia; ↑ haemoglobin, albumin, lymphocyte count; no overall sputum conversion benefit, but faster in non-cavitary TB; no significant weight change; no major adverse effects | [183] |
| Randomized pilot implementation study, Senegal (Ziguinchor and Bignona); 26 HIV-TB co-infected adults; 6-month follow-up; median age 46 y; 50% female | Monthly food basket (local cowpeas, rice, oil, milk: ~1200 kcal/day) or RUTF (Plumpy’Nut, ~1000 kcal/day); both arms 6 months; adherence, food security, and clinical outcomes tracked | 100% TB treatment completion; all smear-negative at end; ↑ CD4 (207 → 321), ↑ Hb (10.2 → 12.8), ↑ weight (50 → 55 kg), ↑ BMI (17.3 → 19.3); ↓ food insecurity (92% → 73%); adherence to ART and TB >95% in both arms; food basket more acceptable/shared | [184] |
| Single-blinded RCT, Pakistan (PIMS TB centre), 2020–2021; 426 adult TB patients; 213 intervention, 213 control; follow-up at 3 and 6 months | Pharmacist-led patient-centred care: individualised counselling, printed materials on nutrition and drug use, lifestyle education, medication management, SMS and phone reminders; all patients continued standard TB therapy | EQ-5D utility score ↑ from 0.40 to 0.89 (vs. 0.42 to 0.78 in control); significant improvement in HRQoL domains (mobility, self-care, activities, pain, anxiety); ↑ patient satisfaction and adherence indicators | [185] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fâcă, A.I.; Udeanu, D.I.; Arsene, A.L.; Mahler, B.; Drăgănescu, D.; Apetroaei, M.-M. Nutritional Deficiencies and Management in Tuberculosis: Pharmacotherapeutic and Clinical Implications. Nutrients 2025, 17, 1878. https://doi.org/10.3390/nu17111878
Fâcă AI, Udeanu DI, Arsene AL, Mahler B, Drăgănescu D, Apetroaei M-M. Nutritional Deficiencies and Management in Tuberculosis: Pharmacotherapeutic and Clinical Implications. Nutrients. 2025; 17(11):1878. https://doi.org/10.3390/nu17111878
Chicago/Turabian StyleFâcă, Anca Ionela, Denisa Ioana Udeanu, Andreea Letiția Arsene, Beatrice Mahler, Doina Drăgănescu, and Miruna-Maria Apetroaei. 2025. "Nutritional Deficiencies and Management in Tuberculosis: Pharmacotherapeutic and Clinical Implications" Nutrients 17, no. 11: 1878. https://doi.org/10.3390/nu17111878
APA StyleFâcă, A. I., Udeanu, D. I., Arsene, A. L., Mahler, B., Drăgănescu, D., & Apetroaei, M.-M. (2025). Nutritional Deficiencies and Management in Tuberculosis: Pharmacotherapeutic and Clinical Implications. Nutrients, 17(11), 1878. https://doi.org/10.3390/nu17111878