
The Effects of Creatine Monohydrate Supplementation on Recovery from Eccentric Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial Considering Sex and Age Differences
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
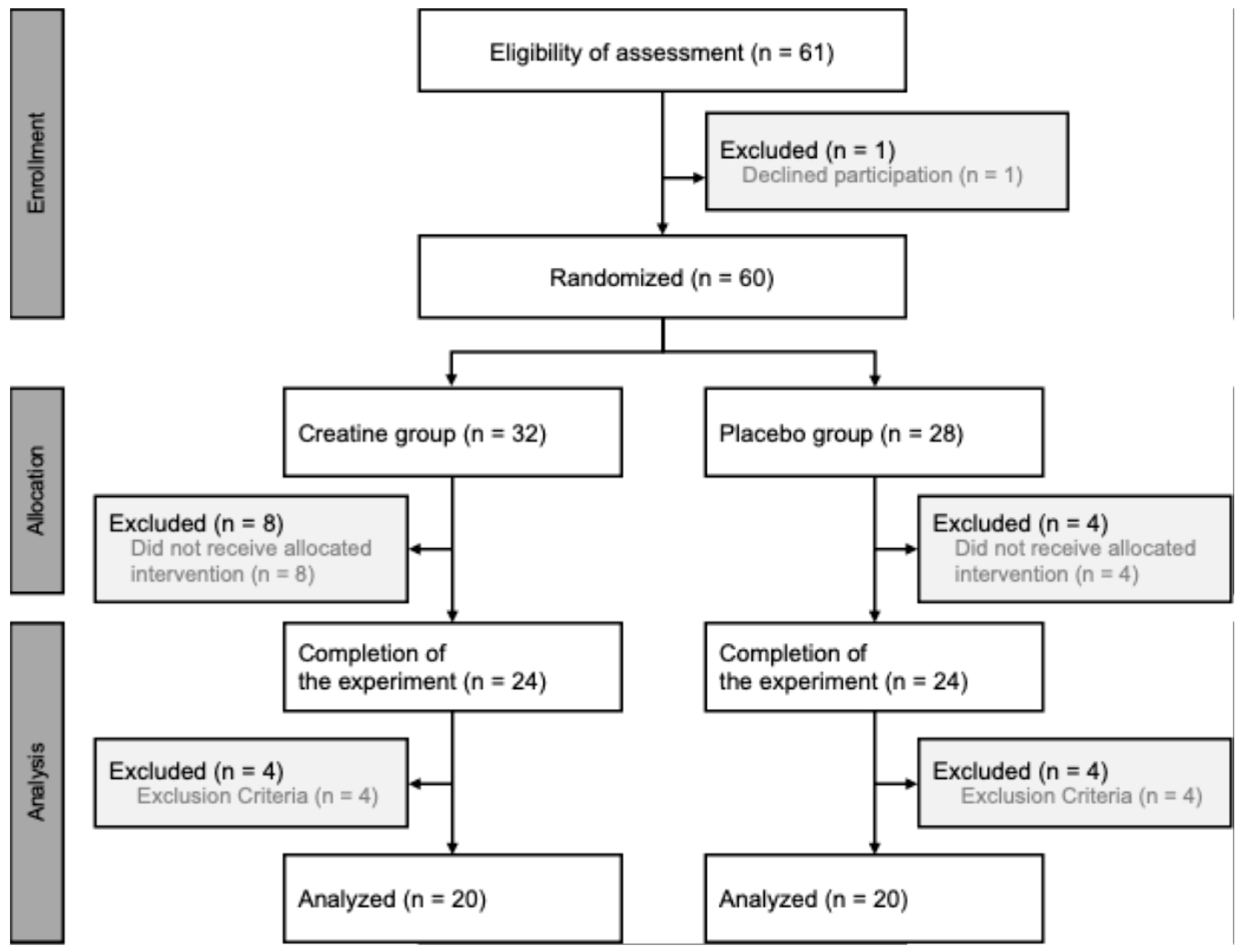
2.1. Participants
2.2. Experimental Design
2.3. Body Composition
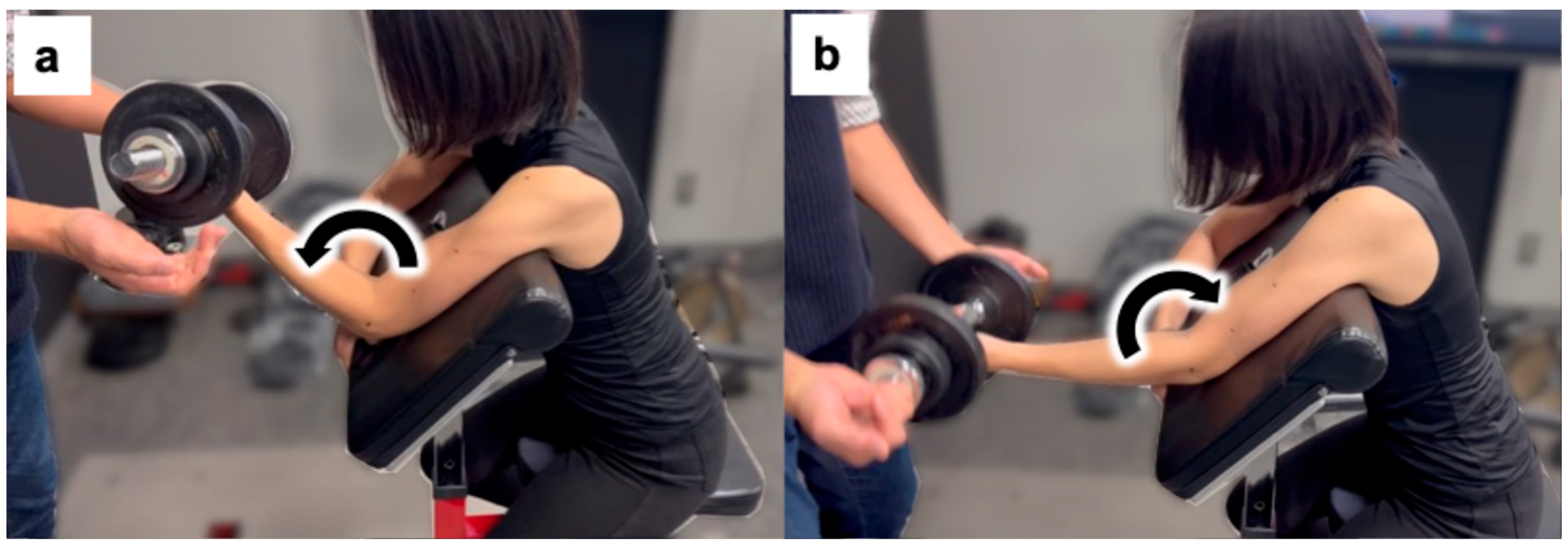
2.4. Eccentric Exercise
2.5. Maximum Voluntary Contraction Evaluation
2.6. Active Range of Motion
2.7. Subjective Evaluation
2.8. Circumference
2.9. Muscle Shear Modulus
2.10. Statistical Analysis
3. Results
3.1. Baseline Values
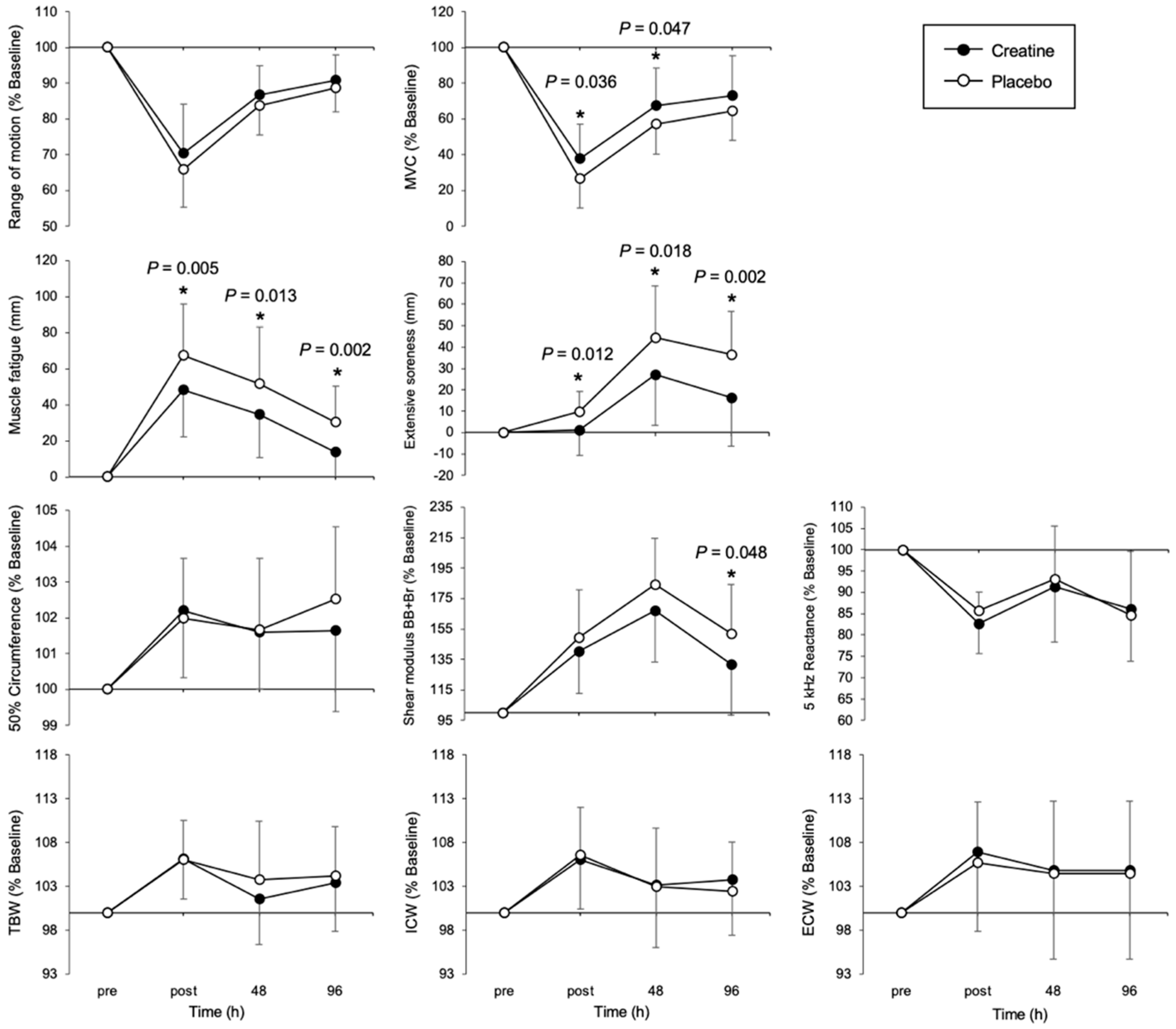
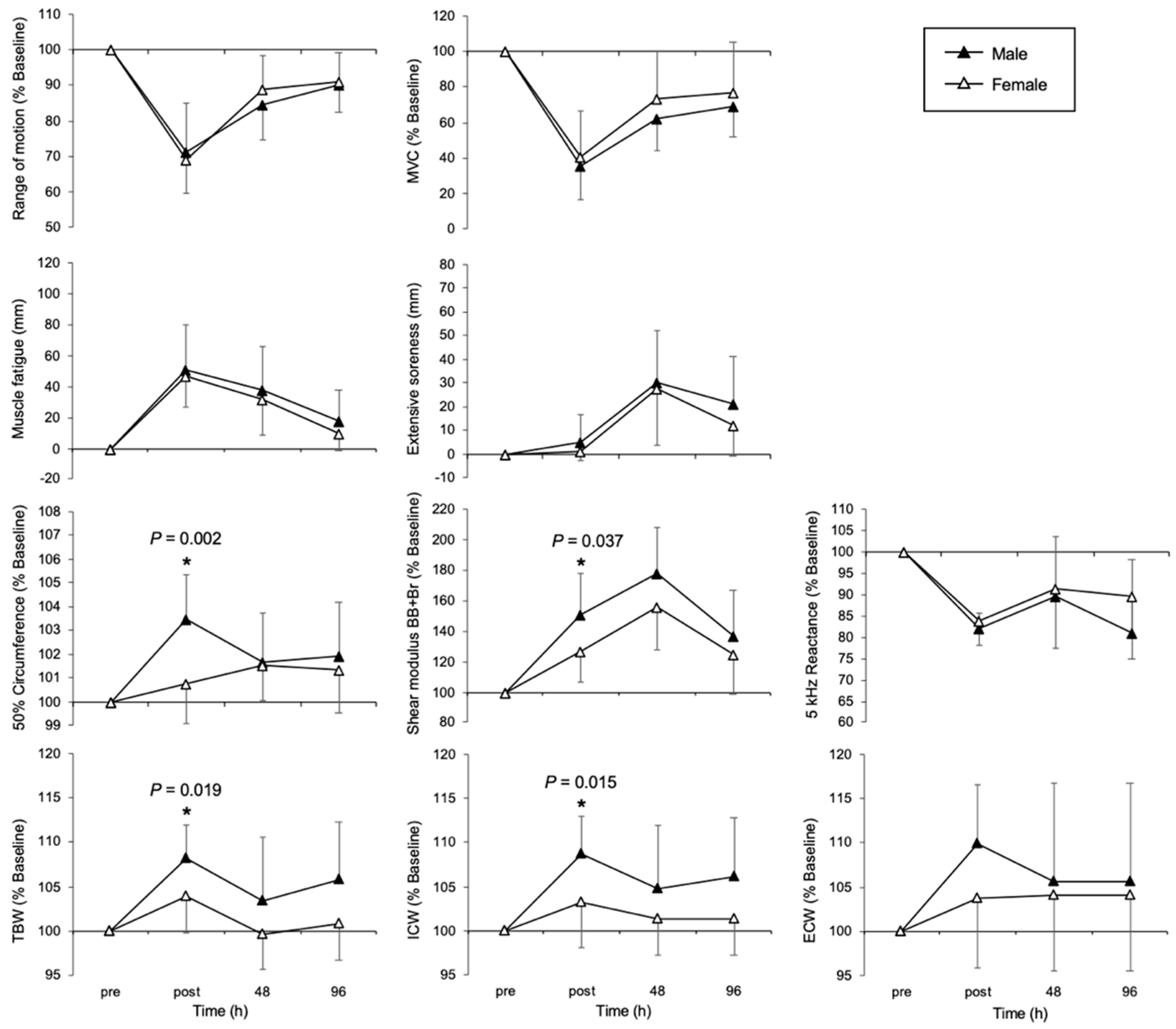
3.2. Temporal Changes in Each Muscle Damage Indicator
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CrM | Creatine monohydrate |
| EIMD | Exercise-induced muscle damage |
| MVC | Maximal voluntary contraction |
| ROM | Range of motion |
| CRE | Creatine supplementation group |
| PLA | Placebo group |
| BB | Biceps brachii muscle |
| Br | Brachialis muscle |
| SDs | Standard deviations |
| Xc | Reactance |
| PhA | Phase angle |
| TBW | Total body water |
| ECW | Extracellular water |
| ICW | Intracellular water |
References
- Yamaguchi, S.; Suzuki, K.; Inami, T.; Kanda, K.; Hanye, Z.; Okada, J. Changes in Urinary Titin N-Terminal Fragment Concentration after Concentric and Eccentric Exercise. J. Sports Sci. Med. 2020, 19, 121–129. [Google Scholar] [PubMed]
- Clarkson, P.M.; Sayers, S.P. Etiology of Exercise-Induced Muscle Damage. Can. J. Appl. Physiol. 1999, 24, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Connolly, D.A.J.; Sayers, S.P.; McHugh, M.P. Treatment and Prevention of Delayed Onset Muscle Soreness. J. Strength Cond. Res. 2003, 17, 197–208. [Google Scholar] [CrossRef]
- Casey, A.; Greenhaff, P.L. Does Dietary Creatine Supplementation Play a Role in Skeletal Muscle Metabolism and Performance? Am. J. Clin. Nutr. 2000, 72, 607S–617S. [Google Scholar] [CrossRef] [PubMed]
- Yokota, Y.; Yamada, S.; Yamamoto, D.; Kato, K.; Morito, A.; Takaoka, A. Creatine Supplementation Alleviates Fatigue after Exercise through Anti-Inflammatory Action in Skeletal Muscle and Brain. Nutraceuticals 2023, 3, 234–249. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Inami, T.; Ishida, H.; Morito, A.; Yamada, S.; Nagata, N.; Murayama, M. The Effect of Prior Creatine Intake for 28 Days on Accelerated Recovery from Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients 2024, 16, 896. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A. Sex Differences in Exercise Metabolism and the Role of 17-Beta Estradiol. Med. Sci. Sports Exerc. 2008, 40, 648–654. [Google Scholar] [CrossRef]
- Enns, D.L.; Tiidus, P.M. The Influence of Estrogen on Skeletal Muscle. Sports Med. 2010, 40, 41–58. [Google Scholar] [CrossRef]
- Dreyer, H.C.; Volpi, E. Role of Protein and Amino Acids in the Pathophysiology and Treatment of Sarcopenia. J. Am. Coll. Nutr. 2005, 24, 140S–145S. [Google Scholar] [CrossRef]
- Lexell, J. Human Aging, Muscle Mass, and Fiber Type Composition. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 11–16. [Google Scholar] [CrossRef]
- Faulkner, J.A.; Brooks, S.V.; Zerba, E. Muscle Atrophy and Weakness with Aging: Contraction-Induced Injury as an Underlying Mechanism. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Hyatt, H.W.; Powers, S.K. The Role of Calpains in Skeletal Muscle Remodeling with Exercise and Inactivity-Induced Atrophy. Int. J. Sports Med. 2020, 41, 994–1008. [Google Scholar] [CrossRef]
- Peake, J.M.; Neubauer, O.; Della Gatta, P.A.; Nosaka, K. Muscle Damage and Inflammation during Recovery from Exercise. J. Appl. Physiol. 2017, 122, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, T.; Genovesi, F.; Nemmer, M.; Carling, C.; Alberti, G.; Howatson, G. Nutritional Interventions for Reducing the Signs and Symptoms of Exercise-Induced Muscle Damage and Accelerate Recovery in Athletes: Current Knowledge, Practical Application and Future Perspectives. Eur. J. Appl. Physiol. 2020, 120, 1965–1996. [Google Scholar] [CrossRef]
- Alfieri, R.R.; Bonelli, M.A.; Cavazzoni, A.; Brigotti, M.; Fumarola, C.; Sestili, P.; Mozzoni, P.; De Palma, G.; Mutti, A.; Carnicelli, D.; et al. Creatine as a Compatible Osmolyte in Muscle Cells Exposed to Hypertonic Stress. J. Physiol. 2006, 576, 391–401. [Google Scholar] [CrossRef]
- Guerrero, M.L.; Beron, J.; Spindler, B.; Groscurth, P.; Wallimann, T.; Verrey, F. Metabolic Support of Na+ Pump in Apically Permeabilized A6 Kidney Cell Epithelia: Role of Creatine Kinase. Am. J. Physiol. 1997, 272, C697–C706. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.H.; Huang, T.; Xiao, J.W.; Gu, R.C.; Ouyang, J.; Wu, G.; Liao, H. Estrogen Signaling Effects on Muscle-Specific Immune Responses through Controlling the Recruitment and Function of Macrophages and T Cells. Skelet. Muscle 2019, 9, 20. [Google Scholar] [CrossRef]
- Nosaka, K.; Newton, M. Repeated Eccentric Exercise Bouts Do Not Exacerbate Muscle Damage and Repair. J. Strength Cond. Res. 2002, 16, 117–122. [Google Scholar]
- Yamaguchi, S.; Inami, T.; Ishida, H.; Nagata, N.; Murayama, M.; Morito, A.; Yamada, S.; Kohtake, N. Bioimpedance Analysis for Identifying New Indicators of Exercise-Induced Muscle Damage. Sci. Rep. 2024, 14, 15299. [Google Scholar] [CrossRef]
- Inami, T.; Yamaguchi, S.; Ishida, H.; Kohtake, N.; Morito, A.; Yamada, S.; Shimomasuda, M.; Haramoto, M.; Nagata, N.; Murayama, M. Changes in Muscle Shear Modulus and Urinary Titin N-Terminal Fragment after Eccentric Exercise. J. Sports Sci. Med. 2022, 21, 536–544. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Suzuki, K.; Kanda, K.; Inami, T.; Okada, J. Changes in Urinary Titin N-Terminal Fragments as a Biomarker of Exercise-Induced Muscle Damage in the Repeated Bout Effect. J. Sci. Med. Sport 2020, 23, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Clarkson, P.M. Changes in Indicators of Inflammation after Eccentric Exercise of the Elbow Flexors. Med. Sci. Sports Exerc. 1996, 28, 953–961. [Google Scholar] [CrossRef]
- Cooke, M.B.; Rybalka, E.; Williams, A.D.; Cribb, P.J.; Hayes, A. Creatine Supplementation Enhances Muscle Force Recovery after Eccentrically-Induced Muscle Damage in Healthy Individuals. J. Int. Soc. Sports Nutr. 2009, 6, 13. [Google Scholar] [CrossRef]
- Northeast, B.; Clifford, T. The Effect of Creatine Supplementation on Markers of Exercise-Induced Muscle Damage: A Systematic Review and Meta-Analysis of Human Intervention Trials. Int. J. Sport. Nutr. Exerc. Metab. 2021, 31, 276–291. [Google Scholar] [CrossRef]
- Doma, K.; Ramachandran, A.K.; Boullosa, D.; Connor, J. The Paradoxical Effect of Creatine Monohydrate on Muscle Damage Markers: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 1623–1645. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Newton, M.; Sacco, P. Delayed-Onset Muscle Soreness Does Not Reflect the Magnitude of Eccentric Exercise-Induced Muscle Damage. Scand. J. Med. Sci. Sports 2002, 12, 337–346. [Google Scholar] [CrossRef]
- Santos, R.V.T.; Bassit, R.A.; Caperuto, E.C.; Costa Rosa, L.F.B.P. The Effect of Creatine Supplementation upon Inflammatory and Muscle Soreness Markers after a 30 km Race. Life Sci. 2004, 75, 1917–1924. [Google Scholar] [CrossRef] [PubMed]
- Hotta, K.; Behnke, B.J.; Masamoto, K.; Shimotsu, R.; Onodera, N.; Yamaguchi, A.; Poole, D.C.; Kano, Y. Microvascular Permeability of Skeletal Muscle after Eccentric Contraction-Induced Muscle Injury: In Vivo Imaging Using Two-Photon Laser Scanning Microscopy. J. Appl. Physiol. 2018, 125, 369–380. [Google Scholar] [CrossRef]
- Lawler, J.M.; Barnes, W.S.; Wu, G.; Song, W.; Demaree, S. Direct Antioxidant Properties of Creatine. Biochem. Biophys. Res. Commun. 2002, 290, 47–52. [Google Scholar] [CrossRef]
- Bär, P.R.; Amelink, G.J. Protection against Muscle Damage Exerted by Oestrogen: Hormonal or Antioxidant Action? Biochem. Soc. Trans. 1997, 25, 50–54. [Google Scholar] [CrossRef]
- Huang, H.; Guo, J.; Chen, Q.; Chen, X.; Yang, Y.; Zhang, W.; Liu, Y.; Chen, X.; Yang, D. The Synergistic Effects of Vitamin D and Estradiol Deficiency on Metabolic Syndrome in Chinese Postmenopausal Women. Menopause 2019, 26, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Cabre, H.E.; Gould, L.M.; Redman, L.M.; Smith-Ryan, A.E. Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review. Metabolites 2024, 14, 347. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Qiu, B.; Li, R.; Han, Y.; Petersen, C.; Liu, S.; Zhang, Y.; Liu, C.; Candow, D.G.; Del Coso, J. Effects of Creatine Supplementation and Resistance Training on Muscle Strength Gains in Adults <50 Years of Age: A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 3665. [Google Scholar] [CrossRef] [PubMed]
- Green, A.L.; Hultman, E.; Macdonald, I.A.; Sewell, D.A.; Greenhaff, P.L. Carbohydrate Ingestion Augments Skeletal Muscle Creatine Accumulation during Creatine Supplementation in Humans. Am. J. Physiol. 1996, 271, E821–E826. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Levene | t-test | ||||||
|---|---|---|---|---|---|---|---|
| PLA | CRE | F-Value | p-Value | t-Value | p-Value | t-Test | |
| Age (years) | 26.8 ± 8.4 | 25.1 ± 7.1 | 0.566 | 0.456 | 0.865 | 0.392 | n.s. |
| Body mass (kg) | 60.0 ± 12.0 | 59.1 ± 8.6 | 1.866 | 0.180 | 0.417 | 0.679 | n.s. |
| Body fat (%) | 26.0 ± 6.4 | 23.0 ± 7.9 | 1.480 | 0.232 | 0.761 | 0.451 | n.s. |
| SMM (kg) | 27.0 ± 5.9 | 24.7 ± 5.3 | 0.061 | 0.806 | 1.217 | 0.231 | n.s. |
| ROM (deg) | 124.1 ± 7.0 | 123.8 ± 6.7 | 1.133 | 0.717 | 0.121 | 0.904 | n.s. |
| MVC (kgf) | 15.1 ± 5.0 | 15.2 ± 4.1 | 1.114 | 0.292 | −0.057 | 0.955 | n.s. |
| CIR (cm) | 25.5 ± 3.4 | 25.4 ± 2.4 | 1.935 | 0.173 | 0.102 | 0.919 | n.s. |
| SOR (mm) | 0.0 ± 0.0 | 0.0 ± 0.0 | − | − | − | − | n.s. |
| MF (mm) | 0.0 ± 0.0 | 0.0 ± 0.0 | − | − | − | − | n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, S.; Inami, T.; Nishioka, T.; Morito, A.; Ishiyama, K.; Murayama, M. The Effects of Creatine Monohydrate Supplementation on Recovery from Eccentric Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial Considering Sex and Age Differences. Nutrients 2025, 17, 1772. https://doi.org/10.3390/nu17111772
Yamaguchi S, Inami T, Nishioka T, Morito A, Ishiyama K, Murayama M. The Effects of Creatine Monohydrate Supplementation on Recovery from Eccentric Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial Considering Sex and Age Differences. Nutrients. 2025; 17(11):1772. https://doi.org/10.3390/nu17111772
Chicago/Turabian StyleYamaguchi, Shota, Takayuki Inami, Takuya Nishioka, Akihisa Morito, Kaho Ishiyama, and Mitsuyoshi Murayama. 2025. "The Effects of Creatine Monohydrate Supplementation on Recovery from Eccentric Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial Considering Sex and Age Differences" Nutrients 17, no. 11: 1772. https://doi.org/10.3390/nu17111772
APA StyleYamaguchi, S., Inami, T., Nishioka, T., Morito, A., Ishiyama, K., & Murayama, M. (2025). The Effects of Creatine Monohydrate Supplementation on Recovery from Eccentric Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial Considering Sex and Age Differences. Nutrients, 17(11), 1772. https://doi.org/10.3390/nu17111772