
Mediterranean Diet Outcomes Across the Mother–Milk–Infant Triad: A Narrative Review




Abstract
1. Introduction
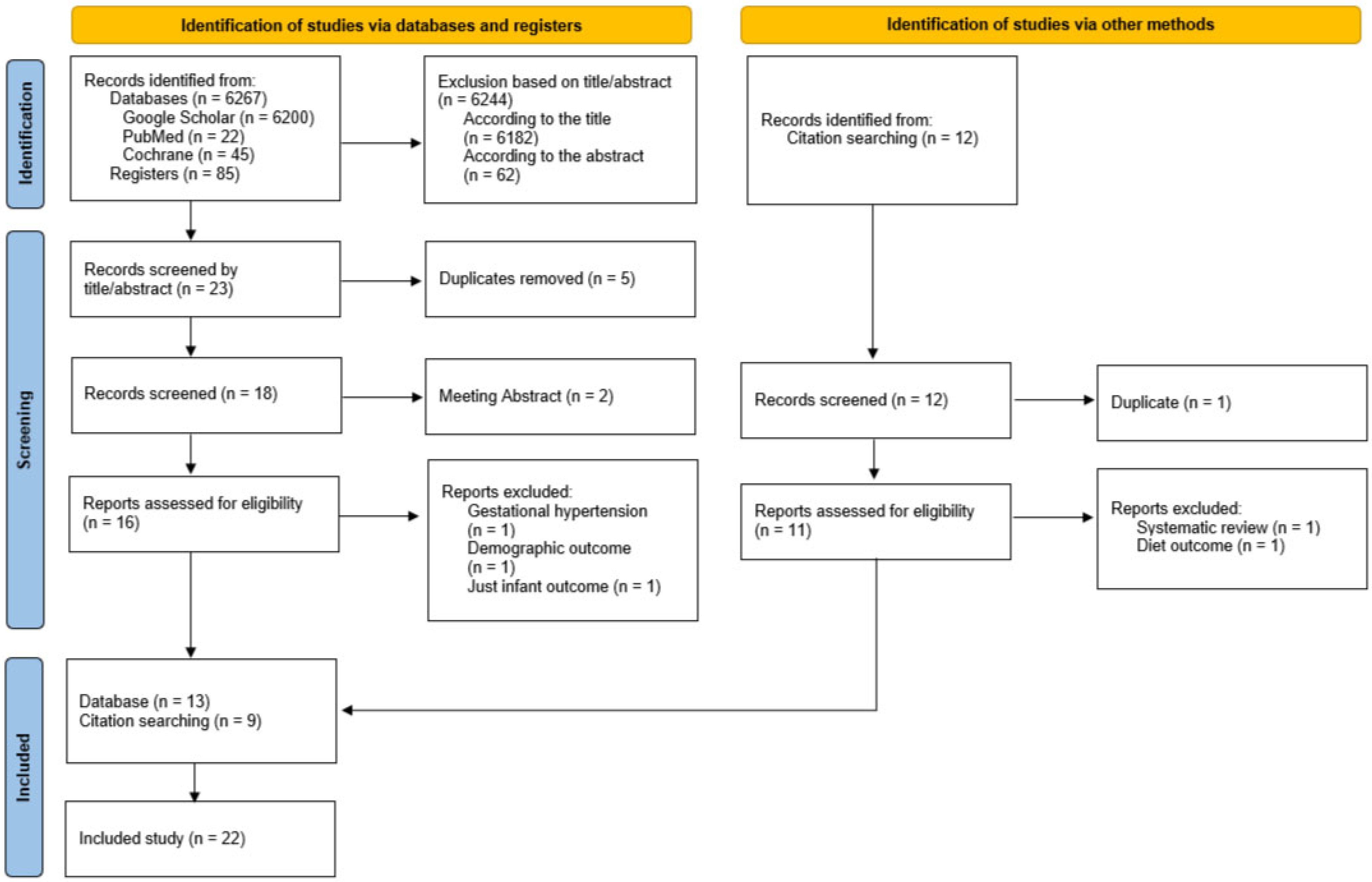
2. Materials and Methods
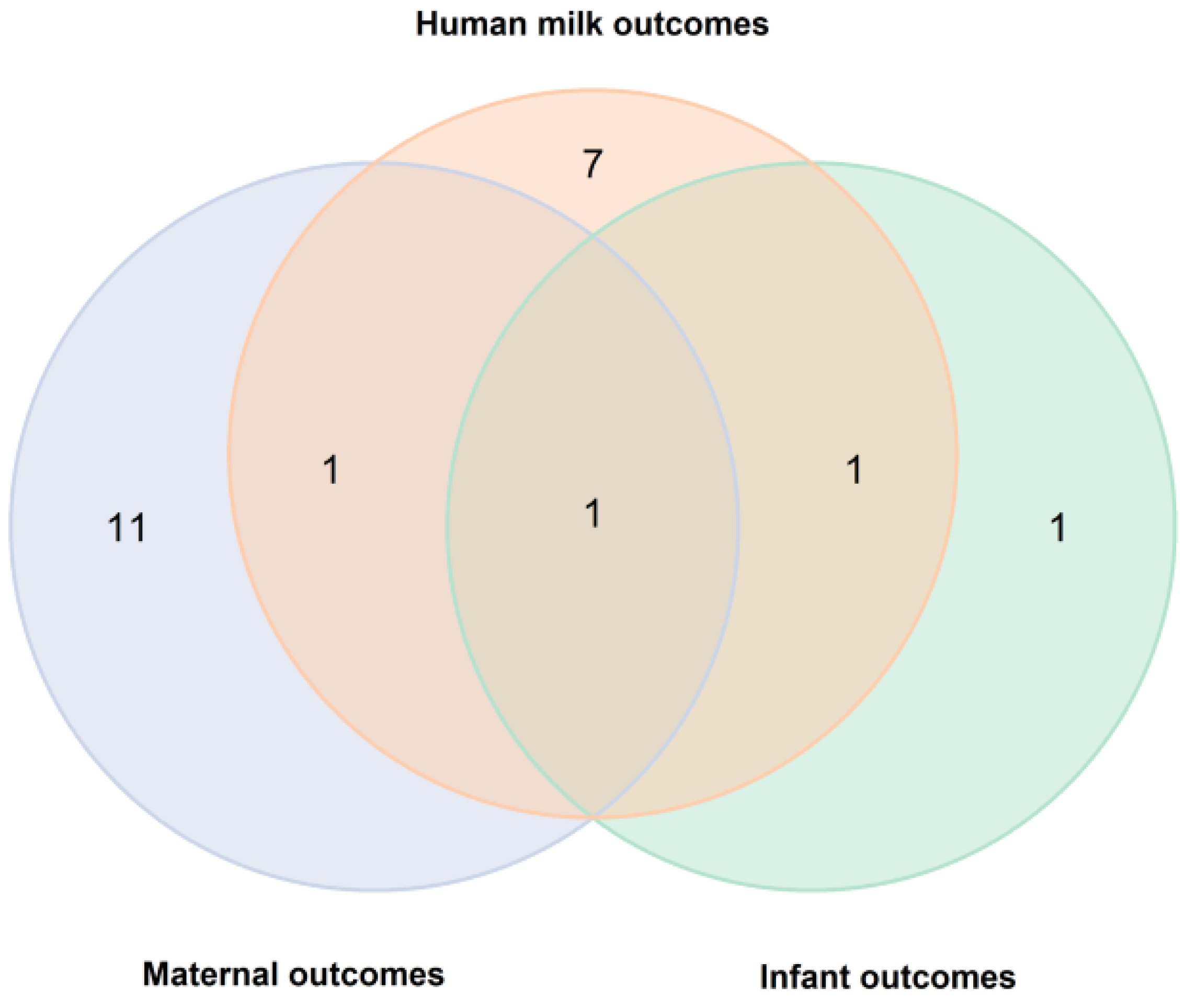
3. Results
3.1. Mediterranean Diet and Maternal Outcomes
3.1.1. Psychological Health and Well-Being
3.1.2. Anthropometry and Body Composition
3.1.3. Metabolic Outcome
3.2. Mediterranean Diet and Human Milk Outcomes
3.3. Mediterranean Diet and Infant Outcomes
4. Discussion
4.1. Maternal Mental Health and Well-Being
4.2. Maternal Anthropometric Outcomes
4.3. Maternal Metabolic Health
4.4. Human Milk Outcomes
4.5. Infant Outcomes
4.6. Methodological Aspects and Recommendations for Further Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AA | arachidonic acid |
| ALA | alpha-linolenic acid |
| aMED | alternate Mediterranean diet score |
| AP-Q | adherence to the healthy food pyramid |
| BIA | bioelectrical impedance analysis |
| BF | breastfeeding |
| BLOOM | breastmilk and the link to overweightness/obesity and maternal diet |
| BMI | body mass index |
| C | cholesterol |
| Ca | calcium |
| CRP | C-reactive protein |
| d | days |
| DASH | dietary approaches to stop hypertension |
| dBP | diastolic blood pressure |
| DHA | docosahexaenoic acid |
| DPA | docosapentaenoic acid |
| DPPH | 2,2-Diphenyl-1-picrylhydrazyl |
| DXA | dual-energy X-ray absorptiometry |
| EBF | exclusive breastfeeding |
| ELISA | enzyme-linked immunosorbent assay |
| EPA | eicosapentaenoic acid |
| EPDS | Edinburgh Postpartum Depression Scale |
| EPIC-ffq | European Prospective Investigation into Cancer and Nutrition Food Frequency Questionnaire |
| EVOO | extra-virgin olive oil |
| FA | fatty acid |
| Fe | iron |
| FFMI | fat-free mass index |
| FFQ | food frequency questionnaire |
| FG | fasting glucose |
| FM | fat mass |
| FMI | fat mass index |
| FRAP | ferric reducing antioxidant power |
| GC | gas chromatography |
| GDM | gestational diabetes |
| GWG | gestational weight gain |
| Hb1Ac | hemoglobin 1Ac (glycated hemoglobin) |
| Hbd | gestational weeks |
| HDL-C | high-density lipoprotein cholesterol |
| HEI | Healthy Eating Index |
| HM | human milk |
| HMOs | human milk oligosaccharides |
| HOMA-IR | homeostatic model assessment for insulin resistance |
| HPLC | high-performance liquid chromatography |
| ICP-MS | inductively coupled plasma mass spectrometry |
| IL | interleukin |
| IMI | Italian Mediterranean Index |
| K | potassium |
| LA | linoleic acid |
| LC-MS | liquid chromatography–mass spectrometry |
| LDL-C | low-density lipoprotein |
| LMD | Lebanese Mediterranean diet |
| LOT | Life Orientation Test |
| m | months |
| MED | Mediterranean diet |
| MEDAS | Mediterranean Diet adherence screener |
| Mg | magnesium |
| MetS | metabolic syndrome |
| MISC | mother and infant study cohort |
| MUFA | monounsaturated fatty acids |
| Na | sodium |
| NW | normal weight |
| OA | oleic acid |
| OW/OB | overweightness/obesity |
| P | phosphor |
| PPWR | postpartum weight retention |
| PSS | Perceived Stress Scale |
| PUFA | polyunsaturated fatty acids |
| RCT | randomized controlled trial |
| sBP | systolic blood pressure |
| Se | selenium |
| SFA | saturated fatty acids |
| TBARS | thiobarbituric acid reactive substances |
| TG | triglyceride |
| TNF-α | tumor necrosis factor α |
| UPLC-MS/MS | ultra-performance liquid chromatography–tandem mass spectrometry |
| VA | vitamin A |
| WC | waist circumference |
| WHO | World Health Organization |
| WHtR | waist-to-hip ratio |
| y | years |
| Zn | zinc |
References
- Meek, J.Y.; Noble, L. Technical Report: Breastfeeding and the Use of Human Milk. Pediatrics 2022, 150, e2022057989. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Smith, E.R.; Lee, S.E.; Vargas, A.J.; Bremer, A.A.; Raiten, D.J. The Need to Study Human Milk as a Biological System. Am. J. Clin. Nutr. 2021, 113, 1063–1072. [Google Scholar] [CrossRef]
- Bode, L.; Raman, A.S.; Murch, S.H.; Rollins, N.C.; Gordon, J.I. Understanding the Mother-Breastmilk-Infant “Triad”. Science 2020, 367, 1078–1080. [Google Scholar] [CrossRef]
- Verduci, E.; Giannì, M.L.; Vizzari, G.; Vizzuso, S.; Cerasani, J.; Mosca, F.; Zuccotti, G.V. The Triad Mother-Breast Milk-Infant as Predictor of Future Health: A Narrative Review. Nutrients 2021, 13, 486. [Google Scholar] [CrossRef]
- Petersohn, I.; Hellinga, A.H.; van Lee, L.; Keukens, N.; Bont, L.; Hettinga, K.A.; Feskens, E.J.M.; Brouwer-Brolsma, E.M. Maternal Diet and Human Milk Composition: An Updated Systematic Review. Front. Nutr. 2023, 10, 1320560. [Google Scholar] [CrossRef]
- Zaidi, Y.; Stroh, R.; Moran, N.E. Systematic Review of Carotenoid Concentrations in Human Milk and Infant Blood. Nutr. Rev. 2022, 80, 2029–2050. [Google Scholar] [CrossRef]
- Rahmannia, S.; Arena, G.; Murray, K.; Sakinah, A.D.; Thariqi, Y.A.; Diana, A.; Hickling, S. A Scoping Review of Methodologies Exploring Diet and Health Outcomes in Lactating Women: What Has Been Done and Where to Next? Nutr. Rev. 2025, nuae228. [Google Scholar] [CrossRef]
- Wingrove, K.; Lawrence, M.A.; McNaughton, S.A. A Systematic Review of the Methods Used to Assess and Report Dietary Patterns. Front. Nutr. 2022, 9, 892351. [Google Scholar] [CrossRef]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for the Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef]
- Lotfi, K.; Saneei, P.; Hajhashemy, Z.; Esmaillzadeh, A. Adherence to the Mediterranean Diet, Five-Year Weight Change, and Risk of Overweight and Obesity: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2022, 13, 152–166. [Google Scholar] [CrossRef]
- Hareer, L.W.; Lau, Y.Y.; Mole, F.; Reidlinger, D.P.; O’Neill, H.M.; Mayr, H.L.; Greenwood, H.; Albarqouni, L. The Effectiveness of the Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease: An Umbrella Review. Nutr. Diet. 2024, 82, 8–41. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An Updated Systematic Review and Meta-Analysis on Adherence to Mediterranean Diet and Risk of Cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef]
- Altun, A.; Brown, H.; Szoeke, C.; Goodwill, A.M. The Mediterranean Dietary Pattern and Depression Risk: A Systematic Review. Neurol. Psychiatry Brain Res. 2019, 33, 1–10. [Google Scholar] [CrossRef]
- Fu, J.; Tan, L.J.; Lee, J.E.; Shin, S. Association between the Mediterranean Diet and Cognitive Health among Healthy Adults: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 946361. [Google Scholar] [CrossRef]
- Romero-Robles, M.A.; Ccami-Bernal, F.; Ortiz-Benique, Z.N.; Pinto-Ruiz, D.F.; Benites-Zapata, V.A.; Casas Patiño, D. Adherence to Mediterranean Diet Associated with Health-Related Quality of Life in Children and Adolescents: A Systematic Review. BMC Nutr. 2022, 8, 57. [Google Scholar] [CrossRef]
- Godos, J.; Guglielmetti, M.; Ferraris, C.; Frias-Toral, E.; Domínguez Azpíroz, I.; Lipari, V.; Di Mauro, A.; Furnari, F.; Castellano, S.; Galvano, F.; et al. Mediterranean Diet and Quality of Life in Adults: A Systematic Review. Nutrients 2025, 17, 577. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Ruiz-Ródenas, N.; Herranz-Chofre, I.; Sánchez-SanSegundo, M.; de la Cruz Serrano Delgado, V.; Hurtado-Sánchez, J.A. Adherence to the Mediterranean Diet in Pregnancy and Its Benefits on Maternal-Fetal Health: A Systematic Review of the Literature. Front. Nutr. 2022, 9, 813942. [Google Scholar] [CrossRef]
- Biagi, C.; Di Nunzio, M.; Bordoni, A.; Gori, D.; Lanari, M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients 2019, 11, 997. [Google Scholar] [CrossRef]
- Di Maso, M.; Bravi, F.; Ferraroni, M.; Agostoni, C.; Eussen, S.R.B.M.; Decsi, T.; Quitadamo, P.A.; Tonetto, P.; Peila, C.; Profeti, C.; et al. Adherence to Mediterranean Diet of Breastfeeding Mothers and Fatty Acids Composition of Their Human Milk: Results From the Italian MEDIDIET Study. Front. Nutr. 2022, 9, 891376. [Google Scholar] [CrossRef]
- Sims, C.R.; Saben, J.L.; Martinez, A.; Sobik, S.R.; Crimmins, M.R.; Bulmanski, J.E.; Turner, D.; Furst, A.; Jansen, L.T.; Bode, L.; et al. A Mediterranean Diet Plan in Lactating Women with Obesity Reduces Maternal Energy Intake and Modulates Human Milk Composition—A Feasibility Study. Front. Nutr. 2024, 11, 1303822. [Google Scholar] [CrossRef] [PubMed]
- Zielinska-Pukos, M.A.; Kopiasz, Ł.; Hamulka, J. The Effect of Maternal Overweight/Obesity on Serum and Breastmilk Leptin, and Its Associations with Body Composition, Cardiometabolic Health Indices, and Maternal Diet: The BLOOM Study. Metabolites 2024, 14, 221. [Google Scholar] [CrossRef]
- Karbasi, S.; Mohamadian, M.; Naseri, M.; Khorasanchi, Z.; Zarban, A.; Bahrami, A.; Ferns, G.A. A Mediterranean Diet Is Associated with Improved Total Antioxidant Content of Human Breast Milk and Infant Urine. Nutr. J. 2023, 22, 11. [Google Scholar] [CrossRef]
- Gila-Díaz, A.; Carrillo, G.H.; Arribas, S.M.; Ramiro-Cortijo, D. Healthy Habits and Emotional Balance in Women during the Postpartum Period: Differences between Term and Preterm Delivery. Children 2021, 8, 937. [Google Scholar] [CrossRef]
- Flor-Alemany, M.; Migueles, J.H.; Alemany-Arrebola, I.; Aparicio, V.A.; Baena-García, L. Exercise, Mediterranean Diet Adherence or Both during Pregnancy to Prevent Postpartum Depression—GESTAFIT Trial Secondary Analyses. Int. J. Environ. Res. Public Health 2022, 19, 14450. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Pavlidou, E.; Dakanalis, A.; Antasouras, G.; Vorvolakos, T.; Mentzelou, M.; Serdari, A.; Pandi, A.L.; Spanoudaki, M.; Alexatou, O.; et al. Postpartum Depression Is Associated with Maternal Sociodemographic and Anthropometric Characteristics, Perinatal Outcomes, Breastfeeding Practices, and Mediterranean Diet Adherence. Nutrients 2023, 15, 3853. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Marti, A.; Martinez, J.A.; Martín-Moreno, J.M. Mediterranean Diet and Reduction in the Risk of a First Acute Myocardial Infarction: An Operational Healthy Dietary Score. Eur. J. Nutr. 2002, 41, 153–160. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Gila-Díaz, A.; Arribas, S.M.; López de Pablo, Á.L.; López-Giménez, M.R.; Phuthong, S.; Ramiro-Cortijo, D. Development and Validation of a Questionnaire to Assess Adherence to the Healthy Food Pyramid in Spanish Adults. Nutrients 2020, 12, 1656. [Google Scholar] [CrossRef]
- Stendell-Hollis, N.R.; Thompson, P.A.; West, J.L.; Wertheim, B.C.; Thomson, C.A. A Comparison of Mediterranean-Style and Mypyramid Diets on Weight Loss and Inflammatory Biomarkers in Postpartum Breastfeeding Women. J. Women’s Health 2013, 22, 48–57. [Google Scholar] [CrossRef]
- de La Torre, N.G.; Assaf-Balut, C.; Varas, I.J.; Del Valle, L.; Durán, A.; Fuentes, M.; Del Prado, N.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; et al. Effectiveness of Following Mediterranean Diet Recommendations in the Real World in the Incidence of Gestational Diabetes Mellitus (GDM) and Adverse Maternal-Foetal Outcomes: A Prospective, Universal, Interventional Study with a Single Group. the St Carlos Study. Nutrients 2019, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Hashim, M.; Hasan, H.; Abbas, N.; Obaid, R.R.S.; Al Ghazal, H.; Naja, F. Adherence to the Mediterranean Diet during Pregnancy Is Associated with Lower Odds of Excessive Gestational Weight Gain and Postpartum Weight Retention: Results of the Mother-Infant Study Cohort. Br. J. Nutr. 2022, 128, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Tabasso, C.; Mallardi, D.; Corti, Y.; Perrone, M.; Piemontese, P.; Liotto, N.; Menis, C.; Roggero, P.; Mosca, F. Adherence to the Mediterranean Diet and Body Composition of Breastfeeding Mothers: The Potential Role of Unsaturated Fatty Acids. J. Nutr. Sci. 2021, 10, e63. [Google Scholar] [CrossRef]
- Melero, V.; Arnoriaga, M.; Barabash, A.; Valerio, J.; del Valle, L.; Martin O’Connor, R.; de Miguel, M.P.; Diaz, J.A.; Familiar, C.; Moraga, I.; et al. An Early Mediterranean-Based Nutritional Intervention during Pregnancy Reduces Metabolic Syndrome and Glucose Dysregulation Rates at 3 Years Postpartum. Nutrients 2023, 15, 3252. [Google Scholar] [CrossRef]
- Flor-Alemany, M.; Acosta-Manzano, P.; Migueles, J.H.; Henriksson, P.; Löf, M.; Aparicio, V.A. Impact of Exercise Intervention Combined with Optimal Mediterranean Diet Adherence during Pregnancy on Postpartum Body Composition: A Quasi-Experimental Study—The GESTAFIT Project. Nutrients 2023, 15, 4413. [Google Scholar] [CrossRef]
- Martín-O’Connor, R.; Ramos-Levi, A.; Melero, V.; Arnoriaga-Rodriguez, M.; Barabash, A.; Valerio, J.; del Valle, L.; de Miguel, P.; Diaz, A.; Familiar, C.; et al. Early Mediterranean-Based Nutritional Intervention Reduces the Rate of Gestational Diabetes in Overweight and Obese Pregnant Women: A Post-Hoc Analysis of the San Carlos Gestational Prevention Study. Nutrients 2024, 16, 2206. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- De Koning, L.; Anand, S.S. Vascular Viewpoint. Vasc. Med. 2004, 9, 145–146. [Google Scholar] [CrossRef]
- Goulet, J.; Lamarche, B.; Nadeau, G.; Lemieux, S. Effect of a Nutritional Intervention Promoting the Mediterranean Food Pattern on Plasma Lipids, Lipoproteins and Body Weight in Healthy French-Canadian Women. Atherosclerosis 2003, 170, 115–124. [Google Scholar] [CrossRef]
- Naja, F.; Hwalla, N.; Itani, L.; Baalbaki, S.; Sibai, A.; Nasreddine, L. A Novel Mediterranean Diet Index from Lebanon: Comparison with Europe. Eur. J. Nutr. 2015, 54, 1229–1243. [Google Scholar] [CrossRef]
- Agnoli, C.; Krogh, V.; Grioni, S.; Sieri, S.; Palli, D.; Masala, G.; Sacerdote, C.; Vineis, P.; Tumino, R.; Frasca, G.; et al. A Priori-Defined Dietary Patterns Are Associated with Reduced Risk of Stroke in a Large Italian Cohort. J. Nutr. 2011, 141, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Che, X.; Hong, X.; Gross, S.; Pearson, C.; Bartell, T.; Wang, X.; Wang, G. Maternal Mediterranean-Style Diet Adherence during Pregnancy and Metabolomic Signature in Postpartum Plasma: Findings from the Boston Birth Cohort. J. Nutr. 2024, 154, 846–855. [Google Scholar] [CrossRef]
- Zielinska-Pukos, M.A.; Michalska-Kacymirow, M.; Kurek, E.; Bulska, E.; Grabowicz-Chądrzyńska, I.; Wesołowska, A.; Hamulka, J. Breastmilk Mineral Composition among Well-Educated Mothers from Central Poland—Associations with Maternal Dietary Intake, Dietary Patterns and Infant Psychomotor Development. J. Trace Elem. Med. Biol. 2024, 83, 127393. [Google Scholar] [CrossRef]
- Rhee, D.K.; Ji, Y.; Hong, X.; Pearson, C.; Wang, X.; Caulfield, L.E. Mediterranean-Style Diet and Birth Outcomes in an Urban, Multiethnic, and Low-Income Us Population. Nutrients 2021, 13, 1188. [Google Scholar] [CrossRef]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean Diet and Incidence of and Mortality from Coronary Heart Disease and Stroke in Women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef]
- Krusinska, B.; Hawrysz, I.; Wadolowska, L.; Slowinska, M.A.; Biernacki, M.; Czerwinska, A.; Golota, J.J. Associations of Mediterranean Diet and a Posteriori Derived Dietary Patterns with Breast and Lung Cancer Risk: A Case-Control Study. Nutrients 2018, 10, 470. [Google Scholar] [CrossRef]
- Sánchez, C.; Fente, C.; Barreiro, R.; López-Racamonde, O.; Cepeda, A.; Regal, P. Association between Breast Milk Mineral Content and Maternal Adherence to Healthy Dietary Patterns in Spain: A Transversal Study. Foods 2020, 9, 659. [Google Scholar] [CrossRef]
- Antasouras, G.; Papadopoulou, S.K.; Alexatou, O.; Papandreou, D.; Mentzelou, M.; Migdanis, A.; Psara, E.; Migdanis, I.; Chrysafi, M.; Tyrovolas, S.; et al. Adherence to the Mediterranean Diet during Pregnancy: Associations with Sociodemographic and Anthropometric Parameters, Perinatal Outcomes, and Breastfeeding Practices. Medicina 2023, 59, 1547. [Google Scholar] [CrossRef]
- Krešić, G.; Dujmović, M.; Mandić, M.L.; Delaš, I. Relationship between Mediterranean Diet and Breast Milk Fatty Acid Profile: A Study in Breastfeeding Women in Croatia. Dairy Sci. Technol. 2013, 93, 287–301. [Google Scholar] [CrossRef]
- Codini, M.; Tringaniello, C.; Cossignani, L.; Boccuto, A.; Mirarchi, A.; Cerquiglini, L.; Troiani, S.; Verducci, G.; Patria, F.F.; Conte, C.; et al. Relationship between Fatty Acids Composition/Antioxidant Potential of Breast Milk and Maternal Diet: Comparison with Infant Formulas. Molecules 2020, 25, 2910. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Hernández, S.; Esteban-Muñoz, A.; Samaniego-Sánchez, C.; Giménez-Martínez, R.; Miralles, B.; Olalla-Herrera, M. Study of the Phenolic Compound Profile and Antioxidant Activity of Human Milk from Spanish Women at Different Stages of Lactation: A Comparison with Infant Formulas. Food Res. Int. 2021, 141, 110149. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Grabowski, A.; Baylin, A.; Ellsworth, L.; Richardson, J.; Kaciroti, N.; Sturza, J.; Miller, A.L.; Gearhardt, A.N.; Lumeng, J.C.; Gregg, B. Maternal Mediterranean Diet During Lactation and Infant Growth. Breastfeed. Med. 2024, 19, 848–856. [Google Scholar] [CrossRef]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A Systematic Review and Meta-Analysis of Dietary Patterns and Depression in Community-Dwelling Adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef]
- Murakami, K.; Sasaki, S. Dietary Intake and Depressive Symptoms: A Systematic Review of Observational Studies. Mol. Nutr. Food Res. 2010, 54, 471–488. [Google Scholar] [CrossRef]
- Gilbody, S.; Lightfoot, T.; Sheldon, T. Is Low Folate a Risk Factor for Depression? A Meta-Analysis and Exploration of Heterogeneity. J. Epidemiol. Community Health 2007, 61, 631–637. [Google Scholar] [CrossRef]
- Amini, S.; Jafarirad, S.; Amani, R. Postpartum Depression and Vitamin D: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2019, 59, 1514–1520. [Google Scholar] [CrossRef]
- Appleton, K.M.; Hayward, R.C.; Gunnell, D.; Peters, T.J.; Rogers, P.J.; Kessler, D.; Ness, A.R. Effects of N-3 Long-Chain Polyunsaturated Fatty Acids on Depressed Mood: Systematic Review of Published Trials. Am. J. Clin. Nutr. 2006, 84, 1308–1316. [Google Scholar] [CrossRef]
- Ventriglio, A.; Sancassiani, F.; Contu, M.P.; Latorre, M.; Di Slavatore, M.; Fornaro, M.; Bhugra, D. Mediterranean Diet and Its Benefits on Health and Mental Health: A Literature Review. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 156–164. [Google Scholar] [CrossRef]
- Kaluza, J.; Lozynska, K.; Rudzinska, J.; Granda, D.; Sicinska, E.; Szmidt, M.K. Mediterranean-Style Diet and Other Determinants of Well-Being in Omnivorous, Vegetarian, and Vegan Women. Nutrients 2023, 15, 725. [Google Scholar] [CrossRef] [PubMed]
- Baskin, R.; Hill, B.; Jacka, F.N.; O’Neil, A.; Skouteris, H. The Association Between Diet Quality and Mental Health During the Perinatal Period. A Systematic Review. Appetite 2015, 91, 41–47. [Google Scholar] [CrossRef]
- Chatzi, L.; Melaki, V.; Sarri, K.; Apostolaki, I.; Roumeliotaki, T.; Georgiou, V.; Vassilaki, M.; Koutis, A.; Bitsios, P.; Kogevinas, M. Dietary Patterns during Pregnancy and the Risk of Postpartum Depression: The Mother-Child “Rhea” Cohort in Crete, Greece. Public Health Nutr. 2011, 14, 1663–1670. [Google Scholar] [CrossRef]
- Hamazaki, K.; Matsumura, K.; Tsuchida, A.; Kasamatsu, H.; Tanaka, T.; Ito, M.; Inadera, H.; Japan Environment and Children’s Study Group. Dietary Intake of Fish and N-3 Polyunsaturated Fatty Acids and Risk of Postpartum Depression: A Nationwide Longitudinal Study—The Japan Environment and Children’s Study (JECS). Psychol. Med. 2020, 50, 2416–2424. [Google Scholar] [CrossRef]
- Opie, R.S.; Uldrich, A.C.; Ball, K. Maternal Postpartum Diet and Postpartum Depression: A Systematic Review. Matern. Child Health J. 2020, 24, 966–978. [Google Scholar] [CrossRef]
- Cao, L.; Liu, Y.; Liang, X.; Zheng, Y.; Li, W.; Yan, J.; Huang, G. Association between Dietary Patterns during the Third Trimester and the Risk of Postpartum Depression in China. J. Affect. Disord. 2020, 264, 370–375. [Google Scholar] [CrossRef]
- Bayes, J.; Schloss, J.; Sibbritt, D. Effects of Polyphenols in a Mediterranean Diet on Symptoms of Depression: A Systematic Literature Review. Adv. Nutr. 2020, 11, 602–615. [Google Scholar] [CrossRef]
- Dalfra’, M.G.; Burlina, S.; Lapolla, A. Weight Gain during Pregnancy: A Narrative Review on the Recent Evidences. Diabetes Res. Clin. Pract. 2022, 188, 109913. [Google Scholar] [CrossRef]
- Schauberger, C.W.; Rooney, B.L.; Brimer, L.M. Factors That Influence Weight Loss in the Puerperium. Obstet. Gynecol. 1992, 79, 424–429. [Google Scholar] [CrossRef]
- Wahabi, H.A.; Fayed, A.A.; Tharkar, S.; Esmaeil, S.A.; Bakhsh, H. Postpartum Weight Retention and Cardiometabolic Risk among Saudi Women: A Follow-Up Study of RAHMA Subcohort. BioMed Res. Int. 2019, 2019, 2957429. [Google Scholar] [CrossRef]
- Catalano, P.M.; Shankar, K. Obesity and Pregnancy: Mechanisms of Short Term and Long Term Adverse Consequences for Mother and Child. BMJ 2017, 356, j1. [Google Scholar] [CrossRef] [PubMed]
- Neville, C.E.; McKinley, M.C.; Holmes, V.A.; Spence, D.; Woodside, J.V. The Effectiveness of Weight Management Interventions in Breastfeeding Women—A Systematic Review and Critical Evaluation. Birth 2014, 41, 223–236. [Google Scholar] [CrossRef]
- Cano-Ibáñez, N.; Martínez-Galiano, J.M.; Luque-Fernández, M.A.; Martín-Peláez, S.; Bueno-Cavanillas, A.; Delgado-Rodríguez, M. Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy. Int. J. Environ. Res. Public Health 2020, 17, 7908. [Google Scholar] [CrossRef] [PubMed]
- Al Wattar, B.H.; Dodds, J.; Placzek, A.; Beresford, L.; Spyreli, E.; Moore, A.; Gonzalez Carreras, F.J.; Austin, F.; Murugesu, N.; Roseboom, T.J.; et al. Mediterranean-Style Diet in Pregnant Women with Metabolic Risk Factors (ESTEEM): A Pragmatic Multicentre Randomised Trial. PLoS Med. 2019, 16, e1002857. [Google Scholar] [CrossRef]
- Silva-del Valle, M.A.; Sánchez-Villegas, A.; Serra-Majem, L. Asociación Entre El Seguimiento de La Dieta Mediterránea Con El Sobrepeso y La Obesidad En Gestantes de Gran Canaria. Nutr. Hosp. 2013, 28, 654–659. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Pisa, P.T.; Norris, S.A. The Influence of Maternal Dietary Patterns on Body Mass Index and Gestational Weight Gain in Urban Black South African Women. Nutrients 2017, 9, 732. [Google Scholar] [CrossRef]
- Zhang, Y.; Xia, M.; Weng, S.; Wang, C.; Yuan, P.; Tang, S. Effect of Mediterranean Diet for Pregnant Women: A Meta-Analysis of Randomized Controlled Trials. J. Matern.-Fetal Neonatal Med. 2022, 35, 4824–4829. [Google Scholar] [CrossRef]
- Asbee, S.M.; Jenkins, T.R.; Butler, J.R.; White, J.; Elliot, M.; Rutledge, A. Preventing Excessive Weight Gain During Pregnancy Through Dietary and Lifestyle Counseling: A Randomized Controlled Trial. Obstet. Gynecol. 2009, 113, 305–312. [Google Scholar] [CrossRef]
- Walker, L.O. Predictors of Weight Gain at 6 and 18 Months after Childbirth: A Pilot Study. J. Obstet. Gynecol. Neonatal Nurs. 1996, 25, 39–48. [Google Scholar] [CrossRef]
- Shao, H.H.; Hwang, L.C.; Huang, J.P.; Hsu, H.Y. Postpartum Weight Retention Risk Factors in a Taiwanese Cohort Study. Obes. Facts 2018, 11, 37–45. [Google Scholar] [CrossRef]
- Fadzil, F.; Shamsuddin, K.; Puteh, S.E.W.; Tamil, A.M.; Ahmad, S.; Hayi, N.S.A.; Samad, A.A.; Ismail, R.; Shauki, N.I.A. Predictors of Postpartum Weight Retention among Urban Malaysian Mothers: A Prospective Cohort Study. Obes. Res. Clin. Pract. 2018, 12, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Loy, S.L.; Cheung, Y.B.; Marjorelee, C.; Chia, A.; Han, C.Y.; Godfrey, K.M.; Chong, Y.-S.; Shek, L.P.-C.; Tan, K.H.; Lek, N.; et al. Maternal Night-Eating and Lower Diet Quality during Pregnancy Are Associated with Substantial Postpartum Weight Retention. Proc. Nutr. Soc. 2020, 79, E102. [Google Scholar] [CrossRef]
- Agnoli, C.; Sieri, S.; Ricceri, F.; Giraudo, M.T.; Masala, G.; Assedi, M.; Panico, S.; Mattiello, A.; Tumino, R.; Giurdanella, M.C.; et al. Adherence to a Mediterranean Diet and Long-Term Changes in Weight and Waist Circumference in the EPIC-Italy Cohort. Nutr. Diabetes 2018, 8, 22. [Google Scholar] [CrossRef]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The Effect of Mediterranean Diet on Metabolic Syndrome and Its Components: A Meta-Analysis of 50 Studies and 534,906 Individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef]
- Tortosa, A.; Bes-Rastrollo, M.; Sanchez-Villegas, A.; Javier Basterra-Gortari, F.; Nũnez, J.M.; Nũnez-Cordoba, N.; Martinez-Gonzalez, M.A. Mediterranean Diet Inversely Associated With the Incidence of Metabolic Syndrome The SUN Prospective Cohort. Diabetes Care 2007, 30, 2957–2959. [Google Scholar] [CrossRef]
- Razquin, C.; Martinez, J.A.; Martinez-Gonzalez, M.A.; Corella, D.; Santos, J.M.; Marti, A. The Mediterranean Diet Protects against Waist Circumference Enlargement in 12Ala Carriers for the PPARγ Gene: 2 Years’ Follow-Up of 774 Subjects at High Cardiovascular Risk. Br. J. Nutr. 2009, 102, 672–679. [Google Scholar] [CrossRef]
- Deeb, S.S.; Fajas, L.; Nemoto, M.; Pihlajamäki, J.; Mykkänen, L.; Kuusisto, J.; Laakso, M.; Fujimoto, W.; Auwerx, J. A Pro12Ala Substitution in PPARγ2 Associated with Decreased Receptor Activity, Lower Body Mass Index and Improved Insulin Sensitivity. Nat. Genet. 1998, 20, 284–287. [Google Scholar] [CrossRef]
- Stuebe, A.M.; Rich-Edwards, J.W. The Reset Hypothesis: Lactation and Maternal Metabolism. Am. J. Perinatol. 2009, 26, 81–88. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxid. Med. Cell Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Gesteiro, E.; Rodríguez Bernal, B.; Bastida, S.; Sánchez-Muniz, F.J. Maternal Diets with Low Healthy Eating Index or Mediterranean Diet Adherence Scores Are Associated with High Cord-Blood Insulin Levels and Insulin Resistance Markers at Birth. Eur. J. Clin. Nutr. 2012, 66, 1008–1015. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Garcia-Arellano, A.; Estruch, R.; Marquez-Sandoval, F.; Corella, D.; Fiol, M.; Gómez-Gracia, E.; Viñoles, E.; Arós, F.; Herrera, C.; et al. Components of the Mediterranean-Type Food Pattern and Serum Inflammatory Markers among Patients at High Risk for Cardiovascular Disease. Eur. J. Clin. Nutr. 2008, 62, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Papazian, T.; Serhal, A.; Hout, H.; Younes, H.; Tayeh, G.A.; Azouri, J.; Lteif, F.H.M.; Kesrouani, A.; Khabbaz, L.R. Discrepancies among Different Tools Evaluating Mediterranean Diet Adherence during Pregnancy, Correlated to Maternal Anthropometric, Dietary and Biochemical Characteristics. Clin. Nutr. 2019, 38, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Wiens, F.; Decarli, A.; Dal Pont, A.; Agostoni, C.; Ferraroni, M. Impact of Maternal Nutrition on Breast-Milk Composition: A Systematic Review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef]
- Samur, G.; Topcu, A.; Turan, S. Trans Fatty Acids and Fatty Acid Composition of Mature Breast Milk in Turkish Women and Their Association with Maternal Diet’s. Lipids 2009, 44, 405–413. [Google Scholar] [CrossRef]
- Moro, G.E.; Bertino, E.; Bravi, F.; Tonetto, P.; Gatta, A.; Quitadamo, P.A.; Salvatori, G.; Profeti, C.; Di Nicola, P.; Decarli, A.; et al. Adherence to the Traditional Mediterranean Diet and Human Milk Composition: Rationale, Design, and Subject Characteristics of the MEDIDIET Study. Front. Pediatr. 2019, 7, 66. [Google Scholar] [CrossRef]
- Scopesi, F.; Ciangherotti, S.; Lantieri, P.B.; Risso, D.; Bertini, I.; Campone, F.; Pedrotti, A.; Bonacci, W.; Serra, G. Maternal Dietary PUFAs Intake and Human Milk Content Relationships during the First Month of Lactation. Clin. Nutr. 2001, 20, 393–397. [Google Scholar] [CrossRef]
- Antonakou, A.; Skenderi, K.P.; Chiou, A.; Anastasiou, C.A.; Bakoula, C.; Matalas, A.L. Breast Milk Fat Concentration and Fatty Acid Pattern during the First Six Months in Exclusively Breastfeeding Greek Women. Eur. J. Nutr. 2013, 52, 963–973. [Google Scholar] [CrossRef]
- Enstad, S.; Cheema, S.; Thomas, R.; Fichorova, R.N.; Martin, C.R.; O’Tierney-Ginn, P.; Wagner, C.L.; Sen, S. The Impact of Maternal Obesity and Breast Milk Inflammation on Developmental Programming of Infant Growth. Eur. J. Clin. Nutr. 2021, 75, 180–188. [Google Scholar] [CrossRef]
- Andreas, N.J.; Hyde, M.J.; Gale, C.; Parkinson, J.R.C.; Jeffries, S.; Holmes, E.; Modi, N. Effect of Maternal Body Mass Index on Hormones in Breast Milk: A Systematic Review. PLoS ONE 2014, 9, e115043. [Google Scholar] [CrossRef]
- Păduraru, L.; Dimitriu, D.C.; Avasiloaiei, A.L.; Moscalu, M.; Zonda, G.I.; Stamatin, M. Total Antioxidant Status in Fresh and Stored Human Milk from Mothers of Term and Preterm Neonates. Pediatr. Neonatol. 2018, 59, 600–605. [Google Scholar] [CrossRef]
- Zielinska, M.A.; Hamulka, J.; Wesolowska, A. Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients 2019, 11, 193. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Lyden, E.; Furtado, J.; Van Ormer, M.; Anderson-Berry, A. A Comparison of Nutritional Antioxidant Content in Breast Milk, Donor Milk, and Infant Formulas. Nutrients 2016, 8, 681. [Google Scholar] [CrossRef]
- Karbasi, S.; Bahrami, A.; Asadi, Z.; Shahbeiki, F.; Naseri, M.; Zarban, A.; Ferns, G.A. The Association of Maternal Dietary Quality and the Antioxidant-Proxidant Balance of Human Milk. Int. Breastfeed. J. 2022, 17, 56. [Google Scholar] [CrossRef]
- Devaney, B.; Ziegler, P.; Pac, S.; Karwe, V.; Barr, S.I. Nutrient Intakes of Infants and Toddlers. J. Am. Diet. Assoc. 2004, 104, 14–21. [Google Scholar] [CrossRef]
- Amati, F.; Hassounah, S.; Swaka, A. The Impact of Mediterranean Dietary Patterns during Pregnancy on Maternal and Offspring Health. Nutrients 2019, 11, 1098. [Google Scholar] [CrossRef]
- Assaf-Balut, C.; de la Torre, N.G.; Fuentes, M.; Durán, A.; Bordiú, E.; Del Valle, L.; Valerio, J.; Jiménez, I.; Herraiz, M.A.; Izquierdo, N.; et al. A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester Is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study. Nutrients 2019, 11, 66. [Google Scholar] [CrossRef]
- Chatzi, L.; Rifas-Shiman, S.L.; Georgiou, V.; Joung, K.E.; Koinaki, S.; Chalkiadaki, G.; Margioris, A.; Sarri, K.; Vassilaki, M.; Vafeiadi, M.; et al. Adherence to the Mediterranean Diet during Pregnancy and Offspring Adiposity and Cardiometabolic Traits in Childhood. Pediatr. Obes. 2017, 12, 47–56. [Google Scholar] [CrossRef]
- Xu, J.; Wang, H.; Bian, J.; Xu, M.; Jiang, N.; Luo, W.; Zu, P.; Yin, W.; Zhu, P. Association between the Maternal Mediterranean Diet and Perinatal Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2024, 15, 100159. [Google Scholar] [CrossRef]
- Dai, F.; Wang, P.; Li, Q.; Zhang, L.; Yu, L.; Wu, L.; Tao, R.; Zhu, P. Mediterranean Diet during Pregnancy and Infant Neurodevelopment: A Prospective Birth Cohort Study. Front. Nutr. 2023, 9, 1078481. [Google Scholar] [CrossRef]
- Ganjeh, B.J.; Mirrafiei, A.; Jayedi, A.; Mirmohammadkhani, M.; Emadi, A.; Ehsani, F.; Shab-Bidar, S. The Relationship between Adherence to the Mediterranean Dietary Pattern during Early Pregnancy and Behavioral, Mood and Cognitive Development in Children under 1 Year of Age: A Prospective Cohort Study. Nutr. Neurosci. 2024, 27, 726–733. [Google Scholar] [CrossRef]
- Innis, S.M. Impact of Maternal Diet on Human Milk Composition and Neurological Development of Infants. Am. J. Clin. Nutr. 2014, 99, 734S–741S. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, M.A.; Hamulka, J.; Grabowicz-Chadrzyńska, I.; Bryś, J.; Wesolowska, A. Association between Breastmilk LC PUFA, Carotenoids and Psychomotor Development of Exclusively Breastfed Infants. Int. J. Environ. Res. Public Health 2019, 16, 1144. [Google Scholar] [CrossRef] [PubMed]
- Leghi, G.E.; Middleton, P.F.; Muhlhausler, B.S. A Methodological Approach to Identify the Most Reliable Human Milk Collection Method for Compositional Analysis: A Systematic Review Protocol. Syst. Rev. 2018, 7, 122. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Type of Criteria | Criteria |
|---|---|
| Inclusion |
|
| Exclusion |
|
| No. | Author and Year | Study Design, Name | Study Size, Country | Sample Characteristic (Special Features, Age) | Dietary Assessment/ Intervention, Timing | Mediterranean Diet Assessment | Outcome (Measures, Methods, Timing of Assessment) | Effect of the Mediterranean Diet |
|---|---|---|---|---|---|---|---|---|
| 1 | Gila-Díaz et al., 2021 [24] | Cross-sectional study | n = 55 Spain | n = 30 term deliveries n = 25 preterm deliveries 34.0 (31.5–37.0) y | AP-Q (graphic representation of MED diet questionnaire) 28 d postpartum | AP-Q (11 components) | Stress (PSS); overall positive attitude (LOT); postpartum depression (EPDS) 2×: 14 d and 6 m postpartum | ↑ positivity (14 d and 6 m) ↔ postpartum depression, stress |
| 2 | Flor-Alemany et al., 2022 [25] | RCT GESTAFIT | Spain n = 85 | n = 46 exercise intervention n = 39 control 33.4 ± 4.2 y | FFQ 16 Hbd | Mediterranean Food Pattern (8 components) | Postpartum depression (EPDS) 6 wk postpartum | ↓ postpartum depression |
| 3 | Papadopoulou et al., 2023 [26] | Cross-sectional study | Greece n = 3941 | 33.2 ± 5.6 y | 3–6 m postpartum | MedDietScore (11 components) | Postpartum depression (EPDS) 3–6 m postpartum | ↓ postpartum depression |
| No. | Author and Year | Study Design, Name | Study Size, Country | Sample Characteristic (Special Features, Age) | Dietary Assessment/Intervention, Timing | Mediterranean Diet Assessment | Outcome (Measures, Methods, Timing of Assessment) | Effect of the Mediterranean Diet |
|---|---|---|---|---|---|---|---|---|
| 1 | Stendell-Hollis et al., 2013 [30] | RCT | n = 102 USA | 74% EBF 27.2–4.9 kg/m2 29.7 ± 4.6 y | MED (28 g walnuts/d, 1–2 tbs EVOO/d) vs. MyPyramid FFQ (153 items), 24-h dietary recall Baseline and 4 m | MED score (9 components) | Anthropometry (BIA) and metabolic outcomes Baseline (2 wk) and after intervention (6 m) | ↓ weight, BMI, WC, hip circumference, WHtR, %FM |
| 2 | de la Torre et al., 2019 [31] | Intervention study | n = 384 (postpartum) Spain | 18% GDM 33.2 ± 4.9 y | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | MEDAS (14 components) | Maternal anthropometry and metabolic outcomes 12–14 wk post-partum | ↔ weight, BMI, WC |
| 3 | Radwan et al., 2021 [32] | Observational study MISC | n = 150 United Arab Emirates | 98% BF for 2 m 84% BF for 6 m | FFQ (86 items) 3rd trimester | aMED (8 components), LMD (9 components) | Weight changes across pregnancy and postpartum period 2 and 6 m postpartum | ↓ PPWR |
| 4 | Tabasso et al., 2021 [33] | Cross-sectional study | n = 147 Italy | 33 ± 6.5–34.5 ± 4.3 y | EPIC-ffq 30 ± 10 d postpartum | IMI (11 components) | Anthropometric and body composition assessment (BOD POD) 30 ± 10 d postpartum | ↔ weight, BMI ↓ %FM, FMI |
| 5 | Melero et al., 2023 [34] | RCT San Carlos Cohort | n = 1400 (postpartum) Spain | 29–37 y | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | Adapted MEDAS (12 components) | Anthropometry and metabolic outcomes 3 m and 3 y postpartum | 3 m postpartum: ↓ BMI 3 y postpartum: ↓ weight, BMI, WC ↔ FM (kg) |
| 6 | Flor-Alemany et al., 2023 [35] | RCT GESTAFIT | n = 83 Spain | n = 43 exercise intervention n = 40 control 33.4 ± 4.2 y | FFQ 16 Hbd | Mediterranean Food Pattern (8 components) | Body composition (DXA) 6th wk postpartum | ↑ lean mass ↓ FM, android FM, android to gynoid FM |
| 7 | Martín-O’Connor et al., 2024 [36] | RCT | n = 453 Spain | prepregnancy overweight | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | MEDAS (14 components) | Anthropometry and metabolic outcomes 3 m and 3 y postpartum | 3 m postpartum: ↔ BMI, WC, FM 3 y postpartum: ↑ weight loss ↓ WC ≥ 89.5 cm ↔ BMI, WC, FM |
| 8 | Sims et al., 2024 [21] | within-subject intervention study | n = 13 USA | EBF Obesity 32.8 ± 3.8 y | Med diet (2 ready-to-eat meals + EVOO) 4 weeks 3-day food records, HEI | MedDiet Score (11 components) | Anthropometry (BOD POD) and metabolic outcomes Baseline, 2 wk and 4 wk | ↓ weight, BMI, FMI ↔ FFMI |
| No. | Author and Year | Study Design | Study Size, Country, Name | Sample Characteristic (Special Features, Age) | Dietary Assessment/ Intervention, Timing | Mediterranean Diet Assessment | Outcome (Measures, Methods, Timing of Assessment) | Effect of the Mediterranean Diet |
|---|---|---|---|---|---|---|---|---|
| 1 | Stendell-Hollis et al., 2013 [30] | RCT | n = 102 USA | 74% EBF 27.2–4.9 kg/m2 29.7 ± 4.6 y | MED (28 g walnuts/d, 1–2 tbs EVOO/d) vs. MyPyramid FFQ (153 items), 24 h dietary recall Baseline and 4 m | MED score (9 components) | Plasma FAs (GC), inflammatory biomarkers (ELISA) 4 m | ↑ LA, ALA, ω-3, ω-3/ω-6 ratio ↓ ω-6/ω-3 ratio, TNF-α ↔ IL-6 |
| 2 | de la Torre et al., 2019 [31] | Intervention study | n = 384 (postpartum) Spain | 18% GDM 33.2 ± 4.9 y | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | MEDAS (14 components) | Metabolic outcomes 12–14 wk postpartum | ↔ FG, insulin, HOMA-IR, HbA1c, sBP, C, HDL-C, LDL-C, TG |
| 3 | Melero et al., 2023 [34] | RCT San Carlos Cohort | n = 1400 (postpartum) Spain | 29–37 y | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | Adapted MEDAS (12 components) | Metabolic outcomes 3 m and 3 y postpartum | 3 m postpartum: ↓ C, LDL-C, HDL-C, apo-B, CRP, FG, insulin, HOMA-IR 3 m postpartum: ↓ C, LDL-C, apo-B, CRP, insulin, HOMA-IR, dBP, MetS components ↔ glucose |
| 4 | Che et al., 2024 [43] | Cohort Boston Birth | n = 1410 USA | 28.2 (22.9–33.5) y | 21–72 h postpartum | MedDiet Score | Plasma metabolite profile (LC-MS) 24–72 h postpartum | ↑ triacylglycerols, phosphatidylcholines plasmalogen, phosphatidylserine, phosphatidylethanolamine, methionine sulfoxide, VA ↓ threonine, tropane, adenosine |
| 5 | Martín-O’Connor et al., 2024 [36] | RCT | n = 453 Spain | prepregnancy overweightness | Educational intervention (12–14 Hbd): >40 mL EVOO and/or nuts | MEDAS (14 components) | Metabolic outcomes 3 m and 3 y postpartum | 3 m postpartum: ↓ LDL-C ↔ MetS components 3 y postpartum: ↔ C, HDL-C, TG, sBP, dBP, MetS components ↓ impaired FG |
| 6 | Sims et al., 2024 [21] | within-subject intervention study | n = 13 USA | EBF Obesity 32.8 ± 3.8 y | MED diet (2 ready-to-eat meals + EVOO) 4 weeks 3-day food records, HEI | MedDiet Score (11 components) | Metabolic outcomes, inflammatory biomarkers Baseline, 2 wk and 4 wk | ↓ C, HDL-C, LDL-C, ↔ leptin, insulin, CRP, IL-6, IL-8, TNF-α |
| 7 | Zielinska-Pukos et al., 2024a [22] | Case–control BLOOM | n = 40 Poland | n = 20 NW n = 20 OW/OB 32.4 ± 3.9 y | FFQ (61 food items) 15.05 ± 1.2 w | Polish-aMED (8 components) | Serum leptin (ELISA) 15.5 ± 1.2 w | ↑ leptin (in NW) |
| No. | Author and Year | Study Design, Name | Study Size, Country | Sample Characteristic (Special Features, Age) | Dietary Assessment/Intervention, Timing | Mediterranean Diet Assessment | Human Milk Collection Protocol | Outcome (Measures, Methods, Timing of Assessment) | Effect of the Mediterranean Diet |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Antasouras et al., 2023 [49] | Cross-sectional study | n = 5688 Greece | 35.1 ± 4.8 y | The third trimester of pregnancy | MedDiet Score (11 components) | N/A | Rates of EBF | ↑ EBF for 4 months |
| Human milk composition | |||||||||
| 1 | Krešić et al., 2013 [50] | Cross-sectional study | n = 83 Croatia | 31.80 ± 4.60 y Fully BF | Two consecutive 24 h recalls 5th to 25th lactation wk | No details | 5 mL of post-feeding human milk expressed manually from one breast between 10 and 12 a.m. 5–25 wk of lactation | FAs profile (GC) | ↑ LA, DHA, OA, palmitic acid ↔ AA |
| 2 | Codini et al., 2020 [51] | Cross-sectional study | n = 30 Italy | 31.7 ± 5.1 y Healthy milk donors | No | Evaluated by interview (no details) | Standardized procedure (no details) Samples were submitted to Holder pasteurization | FA profile (GC), antioxidant potential (ORAC) | ↑ SFA, PUFA, antioxidant potential |
| 3 | Sánchez et al., 2020 [48] | Observational cross-sectional study | n = 75 Spain | 35.5 ± 4.0 y | No 0.8–59 m postpartum | MEDAS (14 components) | 25 mL of prefeed milk was expressed (manually/using a breast pump). No details on the time of collection 0.8–59 m postpartum | Mineral composition (ICP-MS) | ↑ Se ↔ Na, K, Ca, Ca/P, Mg, Fe |
| 4 | Sánchez-Hernández et al., 2021 [52] | Observational cross-sectional study | n = 18 Spain | 31.4 (23.0–39.0) y Participants with medium and high adherence | No | MED questionnaire (14 components) | Colostrum (1–5 days, Marmet manual extraction technique). Transitional milk (6–15 days) and mature milk (after 15 days) pre- and post-feed milk was expressed by pump | Phenolic compounds (UPLC-MS/MS), total phenolic compound (Folin assay), antioxidant activity (DPPH, ABTS, FRAP) | ↑ total phenolic compound, antioxidant activity |
| 5 | Di Maso et al., 2022 [20] | Observational study MEDIDIET | n = 282 Italy | 33 ± 4 y EBF 6 ± 1 wk postpartum | FFQ (78 items) | MedDiet Score (9 components) | 30–50 mL of foremilk expressed using a breast pump after breakfast and before lunch, from 1 to 3 h after a previous BF session 6 ± 1 wk postpartum | FA profile (GC) | ↓ SFA, palmitic acid, stearic acid, AA, ω-6/ω-3, LA/ALA ↑ MUFA, OA, erucic, PUFA ω-3, ALA, EPA, DHA, DPA, DHA/AA |
| 6 | Karbasi et al., 2023 [23] | Cross-sectional study | n = 350 Iran | Mother: 29.5 ± 5.9 y Infants: 1–6 m | FFQ (65 items) | MedDiet Score (8 components) | 2 × 20 mL of pre-feeding human milk manually expressed between 7 and 10 a.m. 1–6 m | Protein (Bradford protein assay), TGs and Ca (colorimetric method), total antioxidant activity (FRAP, DPPH, TBARS) | ↑ protein, DPPH, FRAP ↓ triglycerides ↔ Ca, thiol |
| 7 | Sims et al., 2024 [21] | within-subject intervention study | n = 13 USA | EBF Obesity 32.8 ± 3.8 y n = 8 male infants | MED diet (2 ready-to-eat meals + EVOO) 4 weeks 3-day food records, HEI | MedDiet Score (11 components) | 4 mL of milk from full breast across all feedings across 24 h pooled into one sample Before each study visit | Macronutrients and energy value (MIRIS HM Analyzer), Leptin insulin, CRP, IL-6, IL-8, TNF-α (ELISA) HMOs (HPLC, pre- and post-intervention milk) | ↔ macronutrients, energy value, HMOs, insulin, IL-6, CRP ↓ leptin, IL-8, TNF-α |
| 8 | Zielinska-Pukos et al., 2024a [22] | Case–control BLOOM | n = 40 Poland | n = 20 NW n = 20 OW/OB 32.4 ± 3.9 y | FFQ (61 food items) 15.05 ± 1.2 w | Polish-Amed (8 components) | An equal volume of pre- and post-feeding milk was expressed during one feeding from four time periods across 24 h 15.05 ± 1.2 w | Leptin in skimmed milk (ELISA) | ↓ leptin (in OW/OB) |
| 9 | Zielinska-Pukos et al., 2024b [44] | Observational study | n = 43 Poland | 31.3 ± 3.6 y | FFQ (61 items) First month of lactation | Polish-aMED Scores (8 components) | An equal volume of pre- and post-feeding milk was expressed during one feeding from four time periods across 24 h First month of lactation | Mineral composition (ICP-MS) | ↑ Ca, Zn ↔ Fe, P |
| No. | Author and Year | Study Design, Name | Study Size, Country | Sample Characteristic (Special Features, Age) | Dietary Assessment/Intervention, Timing | Mediterranean Diet Assessment | Outcome (Measures, Methods, Timing of Assessment) | Effect of the Mediterranean Diet |
|---|---|---|---|---|---|---|---|---|
| 1 | Karbasi et al., 2023 [23] | Cross-sectional study | n = 350 Iran | Mother: 29.5 ± 5.9 y Infants: 1–6 m | FFQ (65 items) | MedDiet Score (8 components) 1–6 m | Infant morning urine anti-oxidant status (DPPH, FRAP) 1–6 m of life | ↑ urine antioxidants |
| 2 | Sims et al., 2024 [21] | within-subject intervention study | n = 13 USA | EBF Obesity 32.8 ± 3.8 y n = 8 male infants | MED diet (2 ready-to-eat meals + EVOO) 4 weeks 3-day food records, HEI | MedDiet Score (11 components) | Infant anthropometry and body composition (quantitative nuclear magnetic resonance) baseline, 2 wk, and 4 wk of the intervention | ↔ weight-for-age, length-for-age, weight-for-length z-scores, FFMI, FMI |
| 3 | Grabowski et al., 2024 [54] | Prospective observational study, ABC Baby | N = 167 USA | 31.6 ± 4.5 y 49% male infants | FFQ (135 items) 2 wk or 2 m postpartum | MedDiet Score (two versions: 8 and 9 components) | Infant anthropometry (WHO standards), flank skinfold thickness 6 m | ↔ weight-for-age, length-for-age ↓ flank skinfold thickness |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baglayici, R.; Hamulka, J.; Zielinska-Pukos, M.A. Mediterranean Diet Outcomes Across the Mother–Milk–Infant Triad: A Narrative Review. Nutrients 2025, 17, 1760. https://doi.org/10.3390/nu17111760
Baglayici R, Hamulka J, Zielinska-Pukos MA. Mediterranean Diet Outcomes Across the Mother–Milk–Infant Triad: A Narrative Review. Nutrients. 2025; 17(11):1760. https://doi.org/10.3390/nu17111760
Chicago/Turabian StyleBaglayici, Rabia, Jadwiga Hamulka, and Monika A. Zielinska-Pukos. 2025. "Mediterranean Diet Outcomes Across the Mother–Milk–Infant Triad: A Narrative Review" Nutrients 17, no. 11: 1760. https://doi.org/10.3390/nu17111760
APA StyleBaglayici, R., Hamulka, J., & Zielinska-Pukos, M. A. (2025). Mediterranean Diet Outcomes Across the Mother–Milk–Infant Triad: A Narrative Review. Nutrients, 17(11), 1760. https://doi.org/10.3390/nu17111760