
Longitudinal Associations Between Maternal Anemia and Breastfeeding Practices on Infant Hemoglobin Levels in the Lao People’s Democratic Republic
 , ,
, , Highlights
- Our GEE model analyzed the relationship between repeated measures of maternal anemia and infant Hb levels over time.
- Maternal anemia during pregnancy and the postpartum period was associated with lower infant Hb levels in the first year of life.
- Among postpartum anemic mothers, adherence to breastfeeding recommendations may help mitigate the negative impact of maternal anemia on infant Hb levels.
- The present study is the first in Lao PDR and Southeast Asia to examine the longitudinal effects of maternal anemia on infant Hb levels while considering breastfeeding practices.
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Infant Hemoglobin: Outcome Variable
2.3. Maternal Anemia: Exposure Variable
2.4. Compliance with Breastfeeding Recommendations
2.5. Statistical Analysis
3. Results
3.1. Demographics
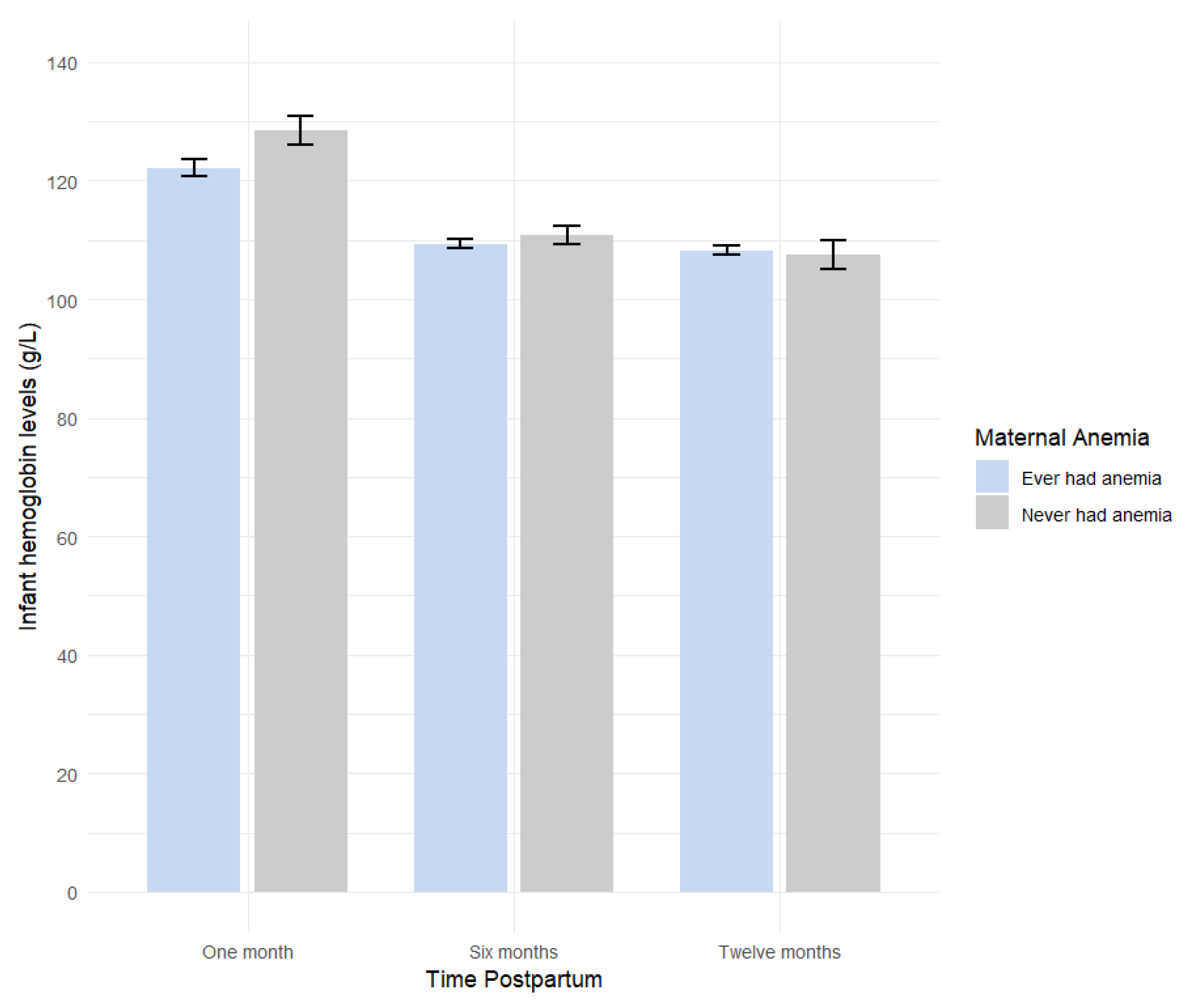
3.2. Infant Hemoglobin Trend over Time
3.3. Association Between Maternal Anemia and Infant Hb Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CI | Confidence interval |
| EBF | Exclusive breastfeeding |
| GEE | Generalized estimating equations |
| Hb | Hemoglobin |
| Lao PDR | Lao People’s Democratic Republic |
| LMIC | Low- and middle- income countries |
| RCT | Randomized control trial |
| SD | Standard deviation |
| STEB | Social Transfer for Exclusive Breastfeeding |
| VITERBI | Vientiane Multi-Generational Birth Cohort |
Appendix A

References
- World Health Organization. Anaemia. Available online: https://www.who.int/news-room/fact-sheets/detail/anaemia (accessed on 10 February 2025).
- Keokenchanh, S.; Kounnavong, S.; Tokinobu, A.; Midorikawa, K.; Ikeda, W.; Morita, A.; Kitajima, T.; Sokejima, S. Prevalence of anemia and its associate factors among women of reproductive age in Lao PDR: Evidence from a nationally representative survey. Anemia 2021, 2021, 8823030. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Observatory Data Repository/World Health Statistics. Prevalence of Anemia Among Pregnant Women (Any Age), with Hb < 110 g/L. Available online: https://genderdata.worldbank.org/en/indicator/sh-prg-anem (accessed on 1 September 2024).
- Keokenchanh, S.; Kounnavong, S.; Midorikawa, K.; Ikeda, W.; Morita, A.; Kitajima, T.; Sokejima, S. Prevalence of anemia and its associated factors among children aged 6–59 months in the Lao People’s Democratic Republic: A multilevel analysis. PLoS ONE 2021, 16, e0248969. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Kolahi, A.-A.; Noori, M.; Nejadghaderi, S.A.; Karamzad, N.; Bragazzi, N.L.; Sullman, M.J.; Abdollahi, M.; Collins, G.S.; Kaufman, J.S. Burden of anemia and its underlying causes in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019. J. Hematol. Oncol. 2021, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Guo, Y.; Lu, J.; Zhu, L.; Yan, S.; Tao, F.; Huang, K. Sex-specific association between maternal mild anemia and children’s behavioral development: A birth cohort study. Eur. Child Adolesc. Psychiatry 2024, 33, 3583–3592. [Google Scholar] [CrossRef]
- The Global Health Observatory. Edition Global Anaemia Estimates in Women of Reproductive Age, by Pregnancy Status, and in Children Aged 6–59 Months. Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed on 1 September 2024).
- Sunuwar, D.R.; Singh, D.R.; Chaudhary, N.K.; Pradhan, P.M.S.; Rai, P.; Tiwari, K. Prevalence and factors associated with anemia among women of reproductive age in seven South and Southeast Asian countries: Evidence from nationally representative surveys. PLoS ONE 2020, 15, e0236449. [Google Scholar] [CrossRef]
- Smith, T.J.; Sitthideth, D.; Tan, X.; Arnold, C.D.; Kounnavong, S.; Hess, S.Y. Nutrition and health-seeking practices during pregnancy and lactation and potential strategies to increase micronutrient intakes among women in northern Lao PDR. J. Nutr. Sci. 2022, 11, e95. [Google Scholar] [CrossRef]
- Boulom, S.; Essink, D.R.; Kang, M.-H.; Kounnavong, S.; Broerse, J.E. Factors associated with child malnutrition in mountainous ethnic minority communities in Lao PDR. Glob. Health Action 2020, 13, 1785736. [Google Scholar] [CrossRef]
- Kapheak, K.; Theerawasttanasiri, N.; Khumphoo, P.; Sriwongphan, R.; Ritthimon, W.; Chayaseng, C.; Bounmaseng, P.; Pangsri, N.; Ngampradit, Y.; Wungrath, J. A Qualitative Study of Women’s Perspectives of Antenatal Care in Rural Areas of the Lao PDR. J. Popul. Soc. Stud. 2025, 33, 803–821. [Google Scholar] [CrossRef]
- Ambulkar, R.; Bakshi, S.; Desai, M. Pregnancy: Physiological Changes and Anemia. Object. Anaesth. Rev. A Compr. Textb. Examinees 2013, 5, 5–6. [Google Scholar]
- Xiong, X.; Buekens, P.; Alexander, S.; Demianczuk, N.; Wollast, E. Anemia during pregnancy and birth outcome: A meta-analysis. Am. J. Perinatol. 2000, 17, 137–146. [Google Scholar] [CrossRef]
- Abu-Ouf, N.M.; Jan, M.M. The impact of maternal iron deficiency and iron deficiency anemia on child’s health. Saudi Med. J. 2015, 36, 146. [Google Scholar] [CrossRef] [PubMed]
- Neef, V.; Choorapoikayil, S.; Hof, L.; Meybohm, P.; Zacharowski, K. Current concepts in postpartum anemia management. Curr. Opin. Anesthesiol. 2024, 37, 234–238. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Breastfeeding. Available online: http://www.who.int/nutrition/topics/exclusive_breastfeeding/en/ (accessed on 2 October 2024).
- Basrowi, R.W.; Zulfiqqar, A.; Sitorus, N.L. Anemia in Breastfeeding Women and Its Impact on Offspring’s Health in Indonesia: A Narrative Review. Nutrients 2024, 16, 1285. [Google Scholar] [CrossRef]
- Sonephet, S.; Kounnavong, S.; Zinsstag, L.; Vonaesch, P.; Sayasone, S.; Siengsounthone, L.; Odermatt, P.; Fink, G.; Wallenborn, J.T. Social Transfers for Exclusive Breastfeeding (STEB) Intervention in Lao People’s Democratic Republic: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2024, 13, e54768. [Google Scholar] [CrossRef]
- Wallenborn, J.T.; Sinantha-Hu, M.; Ouipoulikoune, V.; Kounnavong, S.; Siengsounthone, L.; Probst-Hensch, N.; Odermatt, P.; Sayasone, S.; Fink, G. Vientiane Multigenerational Birth Cohort Project in Lao People’s Democratic Republic: Protocol for Establishing a Longitudinal Multigenerational Birth Cohort to Promote Population Health. JMIR Res. Protoc. 2024, 13, e59545. [Google Scholar] [CrossRef]
- Rappaport, A.I.; Karakochuk, C.D.; Hess, S.Y.; Whitehead, R.D., Jr.; Namaste, S.M.; Dary, O.; Parker, M.E.; Neufeld, L.M.; Larson, L.M.; Newton, S. Variability in haemoglobin concentration by measurement tool and blood source: An analysis from seven countries. J. Clin. Pathol. 2021, 74, 657–663. [Google Scholar] [CrossRef]
- World Health Organization. Guideline on Haemoglobin Cutoffs to Define Anaemia in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2024. [Google Scholar]
- Christensen, R.D.; Bahr, T.M.; Tweddell, S.M.; Ohls, R.K.; Henry, E. Diagnosing Anemia in Neonates: An Evidence-Based Approach. NeoReviews 2023, 24, e343–e355. [Google Scholar] [CrossRef]
- Davidson, E.M.; Scoullar, M.J.; Peach, E.; Morgan, C.J.; Melepia, P.; Opi, D.H.; Supsup, H.; Hezeri, P.; Philip, W.; Kabiu, D. Quantifying differences in iron deficiency-attributable anemia during pregnancy and postpartum. Cell Rep. Med. 2023, 4, 101097. [Google Scholar] [CrossRef]
- The DHS Program. Hemoglobin Collection at The DHS Program: Impact of Updated WHO Guidelines on DHS Program Anemia Data; The DHS Program: Rockville, MD, USA, 2024. [Google Scholar]
- World Health Organization. The Optimal Duration of Exclusive Breastfeeding: A Systematic Review; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Ford, C. Getting Started with Generalized Estimating Equations; University Virginia Library: Charlottesville, VA, USA, 2023. [Google Scholar]
- Colombia University. Repeated Measures Analysis. Available online: https://www.publichealth.columbia.edu/research/population-health-methods/repeated-measures-analysis (accessed on 1 November 2024).
- Gaillard, R.; Eilers, P.H.; Yassine, S.; Hofman, A.; Steegers, E.A.; Jaddoe, V.W. Risk factors and consequences of maternal anaemia and elevated haemoglobin levels during pregnancy: A population-based prospective cohort study. Paediatr. Perinat. Epidemiol. 2014, 28, 213–226. [Google Scholar] [CrossRef]
- Orlandini, C.; Torricelli, M.; Spirito, N.; Alaimo, L.; Di Tommaso, M.; Severi, F.M.; Ragusa, A.; Petraglia, F. Maternal anemia effects during pregnancy on male and female fetuses: Are there any differences? J. Matern. Fetal Neonatal Med. 2017, 30, 1704–1708. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Højsgaard, S.; Halekoh, U.; Yan, J. The R package geepack for generalized estimating equations. J. Stat. Softw. 2006, 15, 1–11. [Google Scholar]
- Zhang, Y.; Jin, L.; Liu, J.-m.; Ye, R.; Ren, A. Maternal hemoglobin concentration during gestation and risk of anemia in infancy: Secondary analysis of a randomized controlled trial. J. Pediatr. 2016, 175, 106–110.e102. [Google Scholar] [CrossRef] [PubMed]
- Heesemann, E.; Mähler, C.; Subramanyam, M.; Vollmer, S. Pregnancy anaemia, child health and development: A cohort study in rural India. BMJ Open 2021, 11, e046802. [Google Scholar] [CrossRef]
- Abioye, A.I.; McDonald, E.A.; Park, S.; Ripp, K.; Bennett, B.; Wu, H.W.; Pond-Tor, S.; Sagliba, M.J.; Amoylen, A.J.; Baltazar, P.I. Maternal anemia type during pregnancy is associated with anemia risk among offspring during infancy. Pediatr. Res. 2019, 86, 396–402. [Google Scholar] [CrossRef]
- Meinzen-Derr, J.K.; Guerrero, M.L.; Altaye, M.; Ortega-Gallegos, H.; Ruiz-Palacios, G.M.; Morrow, A.L. Risk of infant anemia is associated with exclusive breast-feeding and maternal anemia in a Mexican cohort. J. Nutr. 2006, 136, 452–458. [Google Scholar] [CrossRef]
- Shukla, A.K.; Srivastava, S.; Verma, G. Effect of maternal anemia on the status of iron stores in infants: A cohort study. J. Fam. Community Med. 2019, 26, 118–122. [Google Scholar]
- Raj, S.; Faridi, M.; Rusia, U.; Singh, O. A prospective study of iron status in exclusively breastfed term infants up to 6 months of age. Int. Breastfeed. J. 2008, 3, 1–7. [Google Scholar] [CrossRef]
- Murray, M.; Murray, A.B.; Murray, N.; Murray, M.B. The effect of iron status of Nigerien mothers on that of their infants at birth and 6 months, and on the concentration of Fe in breast milk. Br. J. Nutr. 1978, 39, 627–630. [Google Scholar] [CrossRef]
- Reinbott, A.; Jordan, I.; Herrmann, J.; Kuchenbecker, J.; Kevanna, O.; Krawinkel, M.B. Role of breastfeeding and complementary food on hemoglobin and ferritin levels in a cambodian cross-sectional sample of children aged 3 to 24 months. PLoS ONE 2016, 11, e0150750. [Google Scholar] [CrossRef]
- Marques, R.F.; Taddei, J.A.; Lopez, F.A.; Braga, J.A. Breastfeeding exclusively and iron deficiency anemia during the first 6 months of age. Rev. Assoc. Méd. Bras. 2014, 60, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Calvo, E.B.; Galindo, A.C.; Aspres, N.B. Iron status in exclusively breast-fed infants. Pediatrics 1992, 90, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Buck, S.; Rolnick, K.; Nwaba, A.A.; Eickhoff, J.; Mezu-Nnabue, K.; Esenwah, E.; Mezu-Ndubuisi, O.J. Longer Breastfeeding Associated with Childhood Anemia in Rural South-Eastern Nigeria. Int. J. Pediatr. 2019, 2019, 9457981. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Sun, M.; Wu, T.; Li, J.; Shi, H.; Wei, Y. The association between maternal anemia and neonatal anemia: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2024, 24, 677. [Google Scholar] [CrossRef]
- Sangkhae, V.; Nemeth, E. Placental iron transport: The mechanism and regulatory circuits. Free Radic. Biol. Med. 2019, 133, 254–261. [Google Scholar] [CrossRef]
- Faridi, M.; Singh, O.; Rusia, U. Mother’s iron status, breastmilk iron and lactoferrin–are they related? Eur. J. Clin. Nutr. 2006, 60, 903–908. [Google Scholar]
- Widness, J.A. Pathophysiology of anemia during the neonatal period, including anemia of prematurity. Neoreviews 2008, 9, e520–e525. [Google Scholar] [CrossRef]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low-and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Muleviciene, A.; Sestel, N.; Stankeviciene, S.; Sniukaite-Adner, D.; Bartkeviciute, R.; Rascon, J.; Jankauskiene, A. Assessment of risk factors for iron deficiency anemia in infants and young children: A case–control study. Breastfeed. Med. 2018, 13, 493–499. [Google Scholar] [CrossRef]
- Wang, F.; Liu, H.; Wan, Y.; Li, J.; Chen, Y.; Zheng, J.; Huang, T.; Li, D. Age of complementary foods introduction and risk of anemia in children aged 4–6 years: A prospective birth cohort in China. Sci. Rep. 2017, 7, 44726. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 252) | WHO Breastfeeding Recommendations | p-Value 1 | ||
|---|---|---|---|---|---|
| Followed (n = 43) | Partially Followed (n = 59) | Did Not Follow (n = 150) | |||
| n (%) or mean (s.d.) 2 | |||||
| Age (years) 2 | 27.4 (5.5) | 27.6 (6.0) | 27.3 (5.8) | 27.4 (5.2) | 0.21 |
| Age (categorized) | 0.95 | ||||
| Younger than 25 | 74 (29.7) | 12 (28.6) | 19 (33.3) | 43 (28.6) | |
| Between 25 and 30 | 88 (35.3) | 14 (33.3) | 20 (35.1) | 54 (36.0) | |
| Older than 30 | 87 (34.9) | 16 (38.1) | 18 (31.6) | 53 (35.3) | |
| Marital Status | 0.95 | ||||
| Married or cohabitating | 228 (91.6) | 39 (92.9) | 52 (91.2) | 137 (91.3) | |
| Not Married | 21 (8.4) | 3 (7.1) | 5 (8.8) | 13 (8.7) | |
| Maternal education | 0.69 | ||||
| Primary or no education | 64 (25.7) | 14 (33.3) | 13 (22.8) | 37 (24.7) | |
| Secondary | 100 (40.2) | 15 (35.7) | 26 (45.6) | 59 (39.3) | |
| Tertiary | 85 (34.1) | 13 (31.0) | 18 (31.6) | 54 (36.0) | |
| District in Vientiane | 0.41 | ||||
| Chanthabuly | 26 (10.8) | 1 (2.4) | 7 (12.3) | 18 (12.0) | |
| Pakngum | 57 (23.7) | 13 (30.9) | 15 (26.3) | 33 (22.0) | |
| Sangthong | 58 (24.0) | 12 (28.6) | 16 (28.1) | 34 (22.7) | |
| Sikhottabong | 100 (41.5) | 16 (38.1) | 19 (33.3) | 65 (43.3) | |
| Household wealth index | 0.35 | ||||
| 1st quartile | 50 (19.8) | 13 (30.2) | 12 (20.3) | 25 (16.7) | |
| 2nd quartile | 45 (17.9) | 9 (20.9) | 12 (20.3) | 24 (16.0) | |
| 3rd quartile | 52 (20.6) | 6 (14.0) | 15 (25.4) | 31 (20.7) | |
| 4th quartile | 72 (28.6) | 10 (23.3) | 16 (27.1) | 46 (30.7) | |
| 5th quartile | 33 (13.1) | 5 (11.6) | 4 (6.78) | 24 (16.0) | |
| Iron supplementation | 0.63 | ||||
| Yes | 226 (90.8) | 39 (92.9) | 53 (93.0) | 134 (89.3) | |
| No | 23 (9.2) | 3 (7.14) | 4 (7.0) | 16 (10.7) | |
| Alcohol intake | 0.92 | ||||
| Yes | 57 (22.9) | 10 (23.8) | 14 (24.6) | 33 (22.0) | |
| No | 192 (77.1) | 32 (76.2) | 43 (75.4) | 117 (78.0) | |
| Maternal BMI 2 | 25.0 (6.3) | 24.8 (4.6) | 24.4 (4.6) | 25.3 (7.3) | 0.50 |
| Variable | Overall | WHO Breastfeeding Recommendations | ||||||
|---|---|---|---|---|---|---|---|---|
| Followed | Partially Followed | Did Not Follow | ||||||
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| Anemic at Pregnancy | −0.92 (3.30, 1.47) | 0.45 | −4.13 (−8.50, 0.24) | 0.06 | −0.30 (−4.76, 4.16) | 0.89 | 0.09 (−3.25, 3.44) | 0.96 |
| Anemia at PP | −3.30 (−7.99, 1.39) | 0.17 | 7.34 (−3.41, 18.08) | 0.18 | −13.09 (−22.47, −3.70) | 0.01 | −3.11 (−8.94, 2.72) | 0.30 |
| Time | ||||||||
| One month PP | Reference | |||||||
| Six months PP | −14.97 (−18.52, −11.42) | 0.00 | −11.80 (−19.81, −3.80) | 0.00 | −15.99 (−22.84, −9.13) | 0.00 | −15.92 (−20.69, −11.15) | 0.00 |
| Twelve months PP | −16.63 (−20.53, −12.74) | 0.00 | −17.13 (−24.59, −9.68) | 0.00 | −21.86 (−31.42, −12.30) | 0.00 | −13.99 (−18.59, −9.39) | 0.00 |
| PP Anemia × Time Interaction | ||||||||
| Anemia at one month PP | Reference | |||||||
| Anemia at six months PP | 1.97 (−3.38, 7.32) | 0.47 | −6.06 (−18.88, 6.77) | 0.35 | 13.52 (2.31, 24.72) | 0.02 | 1.56 (−5.11, 8.22) | 0.65 |
| Anemia at twelve months PP | 2.47 (−3.03, 7.98) | 0.38 | −6.36 (−18.04, 5.32) | 0.29 | 14.94 (2.39, 27.49) | 0.02 | −0.05 (−6.49, 6.40) | 0.99 |
| Variable | Overall | WHO Breastfeeding Recommendations | ||||||
|---|---|---|---|---|---|---|---|---|
| Followed | Partially Followed | Did Not Follow | ||||||
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| Anemic at Pregnancy | −1.89 (−4.48, 0.70) | 0.15 | −4.56 (−10.73, 1.62) | 0.15 | −2.52 (−7.27, 2.24) | 0.30 | −0.61 (−4.12, 2.90) | 0.73 |
| Anemia at PP | −3.25 (−7.86, 1.36) | 0.17 | 7.87 (−2.21, 17.94) | 0.13 | −13.30 (−22.61, −3.99) | 0.01 | −3.58 (−9.35, 2.19) | 0.22 |
| Time | ||||||||
| One month PP | Reference | |||||||
| Six months PP | −14.94 (−18.47, −11.42) | 0.00 | −12.13 (−19.87, −4.40) | 0.00 | −15.90 (−22.86, −8.94) | 0.00 | −15.97 (−20.73, −11.21) | 0.00 |
| Twelve months PP | −16.64 (−20.53, −12.75) | 0.00 | −15.50 (−23.74, −9.27) | 0.00 | −22.45 (−32.09, −12.81) | 0.00 | −14.20 (−18.81, −9.59) | 0.00 |
| PP Anemia × Time Interaction | ||||||||
| Anemia at one month PP | Reference | |||||||
| Anemia at six months PP | 1.90 (−3.46, 7.26) | 0.49 | −4.94 (−17.72, 7.85) | 0.45 | 13.26 (1.83, 24.69) | 0.02 | 1.55 (−5.15, 8.26) | 0.65 |
| Anemia at twelve months PP | 2.49 (−3.00, 7.98) | 0.37 | −7.71 (−18.99, 3.57) | 0.18 | 16.32 (3.52, 29.13) | 0.01 | 0.37 (−6.11, 6.85) | 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoury, S.M.; Karimian-Marnani, N.; Sonephet, S.; Fink, G.; Wallenborn, J.T. Longitudinal Associations Between Maternal Anemia and Breastfeeding Practices on Infant Hemoglobin Levels in the Lao People’s Democratic Republic. Nutrients 2025, 17, 1703. https://doi.org/10.3390/nu17101703
Khoury SM, Karimian-Marnani N, Sonephet S, Fink G, Wallenborn JT. Longitudinal Associations Between Maternal Anemia and Breastfeeding Practices on Infant Hemoglobin Levels in the Lao People’s Democratic Republic. Nutrients. 2025; 17(10):1703. https://doi.org/10.3390/nu17101703
Chicago/Turabian StyleKhoury, Stephanie M., Najmeh Karimian-Marnani, Souliviengkham Sonephet, Günther Fink, and Jordyn T. Wallenborn. 2025. "Longitudinal Associations Between Maternal Anemia and Breastfeeding Practices on Infant Hemoglobin Levels in the Lao People’s Democratic Republic" Nutrients 17, no. 10: 1703. https://doi.org/10.3390/nu17101703
APA StyleKhoury, S. M., Karimian-Marnani, N., Sonephet, S., Fink, G., & Wallenborn, J. T. (2025). Longitudinal Associations Between Maternal Anemia and Breastfeeding Practices on Infant Hemoglobin Levels in the Lao People’s Democratic Republic. Nutrients, 17(10), 1703. https://doi.org/10.3390/nu17101703