
Predictors of Vitamin D Status in Religious and Intermittent Fasting: A Comparative Study in Orthodox Nuns and Women from the General Population

 ,
,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Study Populations
2.3. Dietary Regimens
2.4. Anthropometric and Biochemical Assessment
2.5. Dietary Intake and Sun Exposure
2.6. Statistical Analysis
- Model 1: Demographic and anthropometric parameters (age, BMI, calcium and vitamin D intake, and sun exposure);
- Model 2: Model 1 plus total and visceral fat, as obtained by BIA analysis;
- Model 3: Μodel 2 plus PTH and insulin concentrations.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Management of endocrine disease: Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Antonopoulou, V.; Karalazou, P.; Thisiadou, K.; Mitrofanova, E.; Mulrooney, H.; Petróczi, A.; Zebekakis, P.; et al. Effects of orthodox religious fasting versus combined energy and time restricted eating on body weight, lipid concentrations and glycaemic profile. Int. J. Food Sci. Nutr. 2021, 72, 82–92. [Google Scholar] [CrossRef]
- Michael, A.; Baye, K. Ethiopian orthodox fasting is associated with weight reduction and body composition changes among healthy adults: A prospective cohort study. Sci. Rep. 2023, 13, 7963. [Google Scholar] [CrossRef] [PubMed]
- Georgakouli, K.; Siamata, F.; Draganidis, D.; Tsimeas, P.; Papanikolaou, K.; Batrakoulis, A.; Gatsas, A.; Poulios, A.; Syrou, N.; Deli, C.K.; et al. The Effects of Greek Orthodox Christian Fasting during Holy Week on Body Composition and Cardiometabolic Parameters in Overweight Adults. Diseases 2022, 10, 120. [Google Scholar] [CrossRef]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Dimakopoulos, G.; Karalazou, P.; Thisiadou, K.; Makedou, K.; Zebekakis, P.; Kotsa, K. Implementation of Christian Orthodox fasting improves plasma adiponectin concentrations compared with time-restricted eating in overweight premenopausal women. Int. J. Food Sci. Nutr. 2022, 73, 210–220. [Google Scholar] [CrossRef]
- Greek National Dietary Guidelines for Adults. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/greece/en/ (accessed on 12 December 2024).
- WHO Global Database on Body Mass Index. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/body-mass-index (accessed on 12 December 2024).
- Tanita Academy Understanding Your Measurements. Available online: http://tanita.eu/ (accessed on 12 December 2024).
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Wallace, A.; Gibson, S.; de la Hunty, A.; Lamberg-Allardt, C.; Ashwell, M. Measurement of 25-hydroxyvitamin D in the clinical laboratory: Current procedures, performance characteristics and limitations. Steroid Biochem. Mol. Biol. 2010, 121, 10–17. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semi-quantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Glanz, K.; Yaroch, A.L.; Dancel, M.; Saraiya, M.; Crane, L.A.; Buller, D.B.; Manne, S.; O’riordan, D.L.; Heckman, C.J.; Hay, J.; et al. Measures of sun exposure and sun protection practices for behavioral and epidemiologic research. Arch. Dermatol. 2008, 144, 217–222. [Google Scholar] [CrossRef]
- Galchenko, A.V.; Rizzo, G.; Baroni, L. Nutrient Intakes in Vegans, Lacto-Ovo-Vegetarians, Orthodox Fasters, and Omnivores in Russia: A Cross-Sectional Study. Foods 2025, 14, 1062. [Google Scholar] [CrossRef]
- Leucuta, D.C.; Dumitrascu, D.L.; Bangdiwala, S.I.; Palsson, O.S.; Sperber, A.D. Effect of Vegan Diet During Greek-Orthodox Religious Fasting on Symptoms of Disorders of Gut-Brain Interaction. J. Gastrointest. Liver Dis. 2025, 34, 40–46. [Google Scholar] [CrossRef]
- Gholampoor, N.; Sharif, A.H.; Mellor, D. The effect of observing religious or faith-based fasting on cardiovascular disease risk factors: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2024, 34, 1097–1109. [Google Scholar] [CrossRef]
- Rodopaios, N.E.; Poulios, E.; Papadopoulou, S.K.; Alexatou, O.; Koulouri, A.A.; Kafatos, A.G.; Papaliagkas, V.; Psara, E.; Giannakoula, A.; Tsourouflis, G.; et al. Association of Christian Orthodox Fasting with Sociodemographic, Anthropometric and Lifestyle Factors and Serum Biochemical Indices: A Cross-Sectional Study on Patients with Metabolic Diseases. Metabolites 2024, 14, 67. [Google Scholar] [CrossRef]
- Kokkinopoulou, A.; Katsiki, N.; Pagkalos, I.; Rodopaios, N.E.; Koulouri, A.A.; Vasara, E.; Papadopoulou, S.K.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.G. Consumption of Ultra-Processed Food and Drink Products in a Greek Christian Orthodox Church Fasting Population. Nutrients 2023, 15, 4907. [Google Scholar] [CrossRef]
- Karras, S.N.; Michalakis, K.; Katsiki, N.; Kypraiou, M.; Vlastos, A.; Anemoulis, M.; Koukoulis, G.; Mouslech, Z.; Talidis, F.; Tzimagiorgis, G.; et al. Interrelations of Leptin and Interleukin-6 in Vitamin D Deficient and Overweight Orthodox Nuns from Northern Greece: A Pilot Study. Nutrients 2025, 17, 1144. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Michalakis, K.; Tekos, F.; Skaperda, Z.; Vardakas, P.; Ziakas, P.D.; Kypraiou, M.; Anemoulis, M.; Vlastos, A.; Tzimagiorgis, G.; et al. Effects of Religious Fasting on Markers of Oxidative Status in Vitamin D-Deficient and Overweight Orthodox Nuns versus Implementation of Time-Restricted Eating in Lay Women from Central and Northern Greece. Nutrients 2024, 16, 3300. [Google Scholar] [CrossRef]
- Koppold, D.A.; Breinlinger, C.; Hanslian, E.; Kessler, C.; Cramer, H.; Khokhar, A.R.; Peterson, C.M.; Tinsley, G.; Vernieri, C.; Bloomer, R.J.; et al. International consensus on fasting terminology. Cell Metab. 2024, 36, 1779–1794.e4. [Google Scholar] [CrossRef]
- Xia, J.; Tu, W.; Manson, J.E.; Nan, H.; Shadyab, A.H.; Bea, J.W.; Cheng, T.D.; Hou, L.; Song, Y. Race-specific associations of 25-hydroxyvitamin D and parathyroid hormone with cardiometabolic biomarkers among US white and black postmenopausal women. Am. J. Clin. Nutr. 2020, 112, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Yalla, N.; Bobba, G.; Guo, G.; Stankiewicz, A.; Ostlund, R. Parathyroid hormone reference ranges in healthy individuals classified by vitamin D status. J. Endocrinol. Investig. 2019, 42, 1353–1360. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Yakout, S.; Bukhari, I.; Khattak, M.N.K.; Al-Saleh, Y.; Aljohani, N.; Al-Attas, O.S.; Alokail, M. Parathyroid hormone in relation to various vitamin D metabolites in adult females. Medicine 2017, 96, e8071. [Google Scholar] [CrossRef]
- Callegari, E.T.; Garland, S.M.; Gorelik, A.; Reavley, N.J.; Wark, J.D. Predictors and correlates of serum 25-hydroxyvitamin D concentrations in young women: Results from the Safe-D study. Br. J. Nutr. 2017, 118, 263–272. [Google Scholar] [CrossRef]
- Sempos, C.T.; Lindhout, E.; Heureux, N.; Hars, M.; Parkington, D.A.; Dennison, E.; Durazo-Arvizu, R.; Jones, K.S.; Wise, S.A. Towards harmonization of directly measured free 25-hydroxyvitamin D using an enzyme-linked immunosorbent assay. Anal. Bioanal. Chem. 2022, 414, 7793–7803. [Google Scholar] [CrossRef] [PubMed]
- Tsuprykov, O.; Elitok, S.; Buse, C.; Chu, C.; Krämer, B.K.; Hocher, B. Opposite correlation of 25-hydroxy-vitamin D- and 1,25-dihydroxy-vitamin D-metabolites with gestational age, bone- and lipid-biomarkers in pregnant women. Sci. Rep. 2021, 11, 1923. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.N.; Chactoura, J.; Nohra, F.; Diogenes, M.E.L.; Bezerra, F.F. Free and Bioavailable Fractions of Vitamin D: Association with Maternal Characteristics in Brazilian Pregnant Women. J. Nutr. Metab. 2020, 2020, 1408659. [Google Scholar] [CrossRef] [PubMed]
- Preka, E.; Wan, M.; Price, K.L.; Long, D.A.; Aitkenhead, H.; Shroff, R. Free 25-hydroxyvitamin-D concentrations are lower in children with renal transplant compared with chronic kidney disease. Pediatr. Nephrol. 2020, 35, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Toldy, E.; Salamon, A.; Kálmán, B.; Ágota, K.; Horváth, D.; Lőcsei, Z. Prognostic Relevance of Circulating 25OHD Fractions for Early Recovery and Survival in Patients with Hip Fracture. J. Clin. Med. 2018, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Sauer, C.G.; Loop, M.S.; Venkateswaran, S.; Tangpricha, V.; Ziegler, T.R.; Dhawan, A.; McCall, C.; Bonkowski, E.; Mack, D.R.; Boyle, B.; et al. Free and Bioavailable 25-Hydroxyvitamin D Concentrations are Associated With Disease Activity in Pediatric Patients With Newly Diagnosed Treatment Naive Ulcerative Colitis. Inflamm. Bowel Dis. 2018, 24, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Battista, C.; Guarnieri, V.; Carnevale, V.; Baorda, F.; Pileri, M.; Garrubba, M.; Salcuni, A.S.; Chiodini, I.; Minisola, S.; Romagnoli, E.; et al. Vitamin D status in primary hyperparathyroidism: Effect of genetic background. Endocrine 2017, 55, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Książek, A.; Zagrodna, A.; Lombardi, G.; Słowińska-Lisowska, M. Seasonal changes in free 25-(OH)D and vitamin D metabolite ratios and their relationship with psychophysical stress markers in male professional football players. Front. Physiol. 2023, 14, 1258678. [Google Scholar] [CrossRef] [PubMed]
- Alonso, N.; Zelzer, S.; Eibinger, G.; Herrmann, M.; Vitamin, D. Metabolites: Analytical Challenges and Clinical Relevance. Calcif. Tissue Int. 2023, 112, 158–177. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Li, S.; Wang, J.; Zheng, D.; Zhang, H.; Yu, W.; Zhu, L.; Liu, Z.; Yang, X.; Yang, L. Threshold for Relationship between Vitamin D and Parathyroid Hormone in Chinese Women of Childbearing Age. Int. J. Environ. Res. Public Health 2021, 18, 13060. [Google Scholar] [CrossRef] [PubMed]
- Shan, X.; Cao, Y.; Zhang, H.; Zhao, X.; Li, S.; Hu, Y.; Yang, L. Free and bioavailable 25-hydroxyvitamin D thresholds for bone metabolism and their associations with metabolic syndrome in Chinese women of childbearing age. Front. Nutr. 2023, 10, 1131140. [Google Scholar] [CrossRef]
- Gong, M.; Wang, K.; Sun, H.; Wang, K.; Zhou, Y.; Cong, Y.; Deng, X.; Mao, Y. Threshold of 25(OH)D and consequently adjusted parathyroid hormone reference intervals: Data mining for relationship between vitamin D and parathyroid hormone. J. Endocrinol. Investig. 2023, 46, 2067–2077. [Google Scholar] [CrossRef]
- Povaliaeva, A.; Zhukov, A.; Bogdanov, V.; Bondarenko, A.; Senko, O.; Kuznetsova, A.; Kodryan, M.; Ioutsi, V.; Pigarova, E.; Rozhinskaya, L.; et al. Evaluation of the age-specific relationship between PTH and vitamin D metabolites. Bone Rep. 2024, 22, 101800. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | Monastic Group (n = 40) | General Population (n = 45) | p-Value |
|---|---|---|---|
| Age (years) | 52.4 ± 17.5 | 49.6 ± 14.3 | 0.314 |
| Years in monastery (years) | 18.6 ± 14.1 | — | — |
| Calcium intake (mg/day) | 467.5 ± 34 | 678 ± 69 | 0.034 |
| Vitamin D intake (IU/day) | 245 ± 11 | 267 ± 18 | 0.23 |
| Sunshine exposure (hours/week) | 4.23 ± 1.2 | 11.2 ± 3.8 | <0.01 |
| BMI | 27.3 ± 4.9 | 25.9 ± 3.8 | 0.151 |
| Body fat (%) | 36.0 ± 7.8 | 34.1 ± 6.1 | 0.220 |
| Visceral fat | 7.7 ± 3.9 | 6.1 ± 2.7 | 0.031 |
| Insulin (μIU/mL) | 11.3 ± 10.6 | 8.4 ± 6.9 | 0.081 |
| PTH (pg/mL) | 42.0 ± 15.1 | 24.6 ± 8.2 | <0.01 |
| 25(OH)D (ng/mL) | 22.5 ± 8.7 | 26.4 ± 9.1 | 0.062 |
| Glucose (mg/dL) | 92.4 ± 9.5 | 89.8 ± 8.7 | 0.129 |
| Calcium (mg/dL) | 9.1 ± 0.3 | 9.4 ± 0.3 | 0.914 |
| Phosphate (mg/dL) | 3.7 ± 0.5 | 3.9 ± 0.4 | 0.087 |
| Predictor | Coefficient | p-Value |
|---|---|---|
| Age (years) | 0.064 | 0.665 |
| BMI | 3.015 | 0.210 |
| Calcium intake (mg/d) | 0.980 | 0.435 |
| Vitamin D intake (IU/d) | 0.142 | 0.123 |
| Sunshine exposure (h/w) | 1.381 | 0.171 |
| Calcium (mg/dL) | 0.054 | 0.779 |
| Phosphate (mg/dL) | −0.217 | 0.528 |
| Predictor | Coefficient | p-Value |
|---|---|---|
| Age (years) | −0.726 | 0.215 |
| BMI | −0.055 | 0.985 |
| Calcium intake (mg/d) | 0.812 | 0.061 |
| Vitamin D intake (IU/d) | 0.143 | 0.056 |
| Sunshine exposure (h/w) | 0.109 | 0.064 |
| Calcium (mg/dL) | 0.123 | 0.708 |
| Phosphate (mg/dL) | −0.278 | 0.412 |
| Body fat (%) | −1.571 | 0.101 |
| Visceral fat | 7.495 | 0.140 |
| Predictor | Orthodox Nuns β (p-Value) | General Population β (p-Value) |
|---|---|---|
| Age (years) | −0.032 (0.784) | −0.017 (0.852) |
| BMI | −0.044 (0.725) | −0.039 (0.791) |
| Calcium intake (mg/day) | 0.129 (0.214) | 0.119 (0.178) |
| Vitamin D intake (IU/day) | 0.086 (0.341) | 0.101 (0.229) |
| Sun exposure (h/week) | 0.121 (0.261) | 0.144 (0.191) |
| Calcium (mg/dL) | 0.045 (0.737) | 0.061 (0.698) |
| Phosphate (mg/dL) | −0.084 (0.611) | −0.112 (0.493) |
| Body fat (%) | −0.091 (0.438) | −0.073 (0.502) |
| Visceral fat | 0.115 (0.301) | 0.132 (0.227) |
| Insulin (μIU/mL) | 0.398 (0.422) | 0.790 (0.231) |
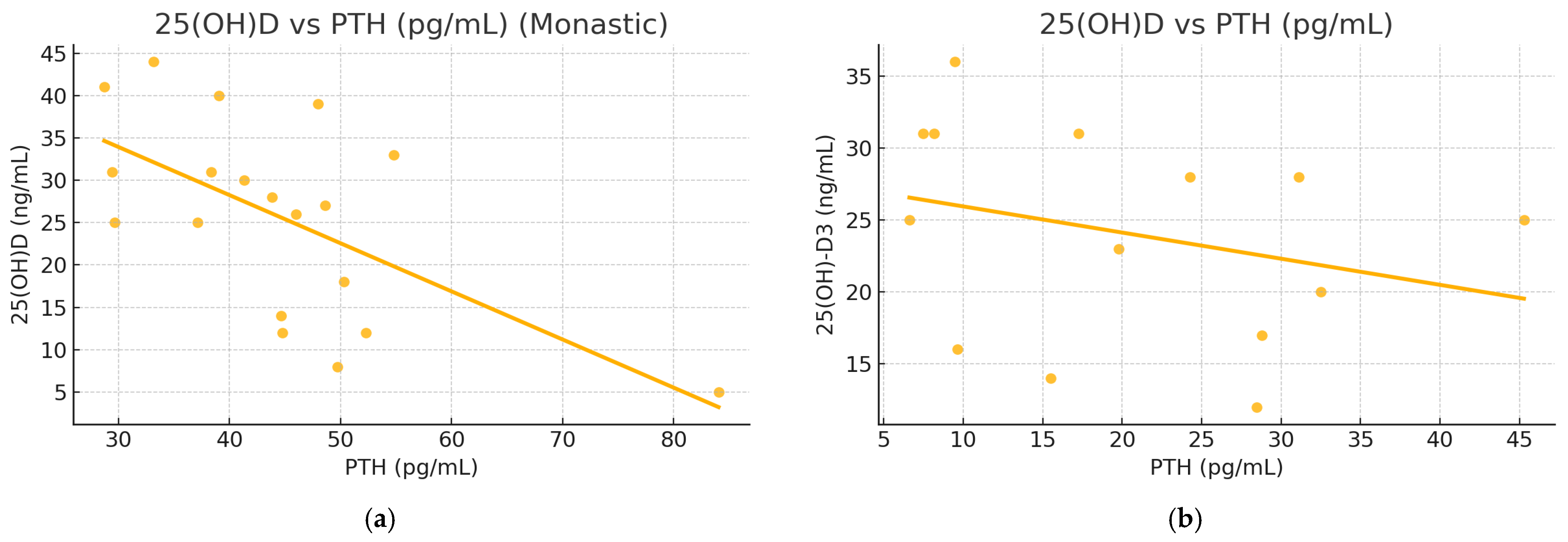
| PTH (pg/mL) | −0.489 (0.013) | −0.549 (0.038) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karras, S.N.; Michalakis, K.; Kypraiou, M.; Vlastos, A.; Anemoulis, M.; Koukoulis, G.; Mouslech, Z.; Talidis, F.; Haitoglou, C.; Michos, G.; et al. Predictors of Vitamin D Status in Religious and Intermittent Fasting: A Comparative Study in Orthodox Nuns and Women from the General Population. Nutrients 2025, 17, 1656. https://doi.org/10.3390/nu17101656
Karras SN, Michalakis K, Kypraiou M, Vlastos A, Anemoulis M, Koukoulis G, Mouslech Z, Talidis F, Haitoglou C, Michos G, et al. Predictors of Vitamin D Status in Religious and Intermittent Fasting: A Comparative Study in Orthodox Nuns and Women from the General Population. Nutrients. 2025; 17(10):1656. https://doi.org/10.3390/nu17101656
Chicago/Turabian StyleKarras, Spyridon N., Konstantinos Michalakis, Maria Kypraiou, Antonios Vlastos, Marios Anemoulis, Georgios Koukoulis, Zadalla Mouslech, Filotas Talidis, Costas Haitoglou, Georgios Michos, and et al. 2025. "Predictors of Vitamin D Status in Religious and Intermittent Fasting: A Comparative Study in Orthodox Nuns and Women from the General Population" Nutrients 17, no. 10: 1656. https://doi.org/10.3390/nu17101656
APA StyleKarras, S. N., Michalakis, K., Kypraiou, M., Vlastos, A., Anemoulis, M., Koukoulis, G., Mouslech, Z., Talidis, F., Haitoglou, C., Michos, G., Papanikolaou, E. G., Skoutas, D., Georgopoulos, N., & Tzimagiorgis, G. (2025). Predictors of Vitamin D Status in Religious and Intermittent Fasting: A Comparative Study in Orthodox Nuns and Women from the General Population. Nutrients, 17(10), 1656. https://doi.org/10.3390/nu17101656