
Perceptions and Acceptability of a Low Phytate: Iron Molar Ratio Biofortified Bean and Sweet Potato Dish Among Pregnant Women in Rural Uganda

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Participants and Sample Size Determination
2.3. Sampling Procedure
2.4. Inclusion and Exclusion Criteria of Study Participants
2.5. Pilot Study
2.6. Ingredients for the Preparation of the Study Composite Dishes
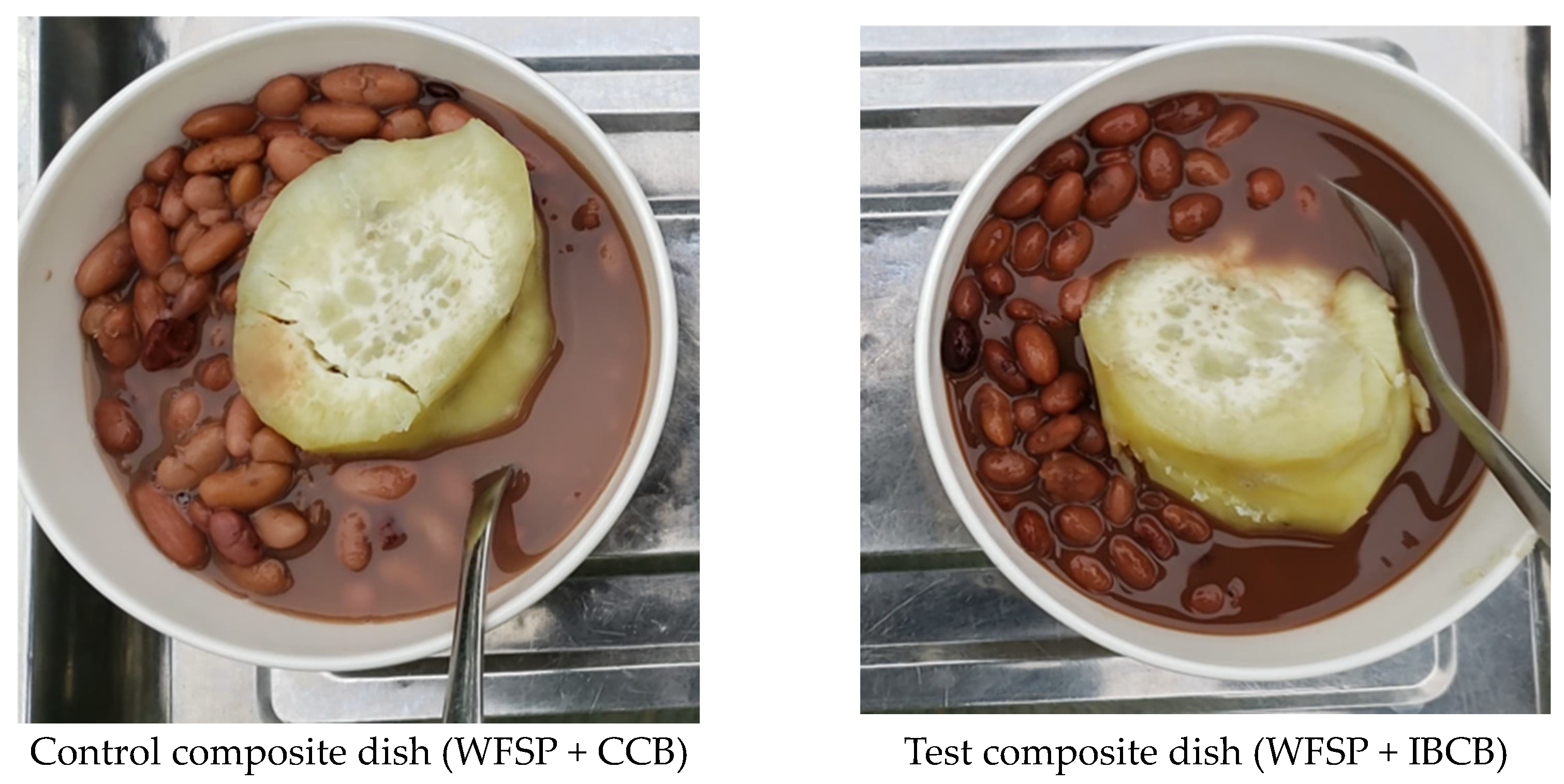
2.7. Preparation of Test and Control Composite Dishes
2.8. Iron, Polyphenol, Phytate Composition, and Phytate: Iron Molar Ratio of Cooked Study Common Bean
2.9. Measurement of Study Variables
2.9.1. Measurement of Sensory Acceptability
2.9.2. Measurement of Pregnant Women’s Perceptions
2.10. Data Analysis
2.10.1. Analysis of Quantitative Data Generated from Sensory Acceptability Measurements
2.10.2. Analysis of Qualitative Data Generated from Focus Group Discussions
2.11. Ethical Considerations
3. Results
3.1. Background Characteristics of Study Participants and Composite Dishes
3.2. Sensory Acceptability of the Study Composite Dishes
3.3. Perceptions on the Consumption of Study Composite Foods
3.3.1. Sensory Acceptability Attributes
“I thought that both dishes were composed of WFSP and CCB. If you had not said that one dish was for WFSP + CCB and the other was for WFSP + IBCB, I wouldn’t have noticed that the two varieties of common bean in either WFSP + IBCB or WFSP + CCB were any different in color, texture, smell, and taste.” (A woman at 6 months gestation)
“…. it is hard to accept that IBCB is different from CCB because both have a similar smell, colour, taste, and texture.” (A woman at 4 months gestation)
“.. you wonder why sometimes health workers do not want to tell us the truth. How could someone say that IBCB is a different variety from CCB, yet both varieties are similar in smell, colour, taste, and texture.” (A woman at 8 months gestation)
“Someone may wonder why we are wasting time on this. We all tasted, touched, saw, and smelled on both IBCB and CCB. I could not find any difference in the two common bean varieties in terms of smell, colour, texture, and taste.”
3.3.2. Feasibility to Prepare Iron-Biofortified Common Bean for Household Consumption
“… one major problem with common beans is that they take a long time to cook. You end up using a lot of fuel. I would like to know whether this IBCB variety takes a shorter period to get ready after cooking compared to CCB.” (A woman at 6 months gestation)
“…. I hate cooking common bean because it consumes a lot of fuel and time to become ready. I would only use IBCB if it cooked faster than the CCB.” (A woman at 8 months gestation)
“We realized that IBCB was similar to CCB in all the sensory properties. It is likely that they also have similar cooking times. Trust me, IBCB should have a long cooking time like CCB.” (A woman at 8 months gestation)
“Common bean will always be common bean, whether IBCB or CCB variety. All varieties of common beans consume a lot of fuel and hence take a long time to cook. I will never cook common beans unless I feel I have excess firewood to waste.” (A teenager at 8 months gestation)
“… buying a half kilogram of common bean is cheaper (3000 Uganda shillings) than buying a half kilogram of beef (6500 Uganda shillings). However, cooking common beans is more costly than cooking beef because you will use fuel worth 5000 Uganda shillings in the former and 1000 Uganda shillings in the latter. Moreover, you will cook common beans for more than 3 hours compared to beef, which can be cooked between 30 to 45 minutes. If you calculate the fuel and time needed to prepare common beans compared to meat, common beans are too expensive.”
“… you see when you are pregnant, you need to cook fast and rest. However, cooking common beans takes a longer time. This will prevent me from cooking common beans.” (A prime gravida teenager at 6 months gestation)
“… no one should ever deceive you about the cooking time of the common bean. All common bean varieties, whether IBCB or CCB, take a long time to cook, nearly 4 to 5 hours to cook. However, there are some techniques that you can use to make common beans softer so that they can cook faster. For example, you can soak them in water overnight for about 8 hours. Trust, me, soaked beans will cook faster for 2 hours compared to the non-soaked beans, which may cook for 4 to 5 hours.” (A gravida 4 at 7 months gestation)
“Besides soaking in water, there is a certain type of salt called “ekisula”. This type of salt softens the common bean. You just get a pinch of salt, “ekisula”, you put it the boiling common bean, within an hour the common beans will be ready for human consumption.” (A gravida 3 at 4 months gestation)
3.3.3. Availability of Iron-Biofortified Common Beans in the Market and Local Farmers
“……… tell us where that IBCB variety can be available to buy it. Are the IBCB varieties available in the same market where we buy the CCB?” (A prime gravida at 6 months gestation)
“Are these IBCB grown here in our district? If so, please let us know the specific part of the district. I am asking all this because if it is grown within our district, it can be easy to buy directly from the local farmers. You see, buying common beans from local farmers can be cheaper compared to someone who buys from the retail market.” (A gravida 2 at 7 months gestation)
3.3.4. Affordability of Iron-Biofortified Common Bean
“How much is the cost of IBCB compared to CCB? Is IBCB cheaper than CCB? I would buy for my household consumption if it is offered at an affordable price from the local market.” (A woman at 4 months gestation)
“… We are subsistence farmers, and most of the food for our household consumption is accessed from our garden. I need to know the cost of the IBCB seeds so that we can buy them for planting season after season. I will plant them if they are either cheaper than the CCB or they are of the same cost as CCB.” (A woman at 8 months gestation)
“…. growing IBCB in our gardens would be the best option. However, it might be expensive in the long run if it is either easily attacked by pests and diseases or not drought-resistant. To what extent are the IBCB drought and pest-resistant compared to our local CCB?” (A woman at 7 months of gestation)
“… I guess IBCB are genetically modified foods (GMFs). You know, GMFs, including IBCB varieties, are not like our local CCB varieties. I suspect these IBCB varieties are easily attacked by pests compared to our CCB. This means that one will incur more costs on buying pesticides if you grow the IBCB.” (A woman at 5 months gestation)
3.3.5. Sustainable Supply of Iron-Biofortified Common Bean
“….. I would consume the IBCB if I could find it any time I needed it. The challenge is to go to the market and you don’t find the IBCB any time you may need to cook it for household consumption.” (A woman at 5 months gestation)
“.. I remember the Ministry of Agriculture officials sensitized us about the benefits of consuming IBCB. This happened about three years before I migrated to this district. However, I could not find the IBCB on the local market whenever I wanted them. It would be important that as you introduce these IBCB to us also put effort into ensuring that they are always available on the market season after season so that people can either consume them or grow them in their farm household.” (A woman at 8 months gestation)
“… health workers and agricultural extension workers always tend to introduce biofortified foods to us. However, these biofortified foods only appear once on the market when their funded project or programme is running. The sad reality is that when the programme ends, you will never find these biofortified foods again in the local community. I doubt whether this IBCB will be available in our community season after season.” (A woman at 5 months gestation)
3.3.6. Nutritional Value and Health Benefits for Pregnancy Outcomes
“Are there any health benefits of consuming IBCB during pregnancy? I will only consider eating IBCB combined with WFSP or any other staple cereal or tuber if I know that IBCB has more health benefits for my fetus and myself than CCB.” (A prime gravida at 6 months gestation)
“I don’t see any difference in the sensory attributes between WFSP + IBCB and WFSP + CCB. Therefore, I would only choose to eat WFSP prepared with IBCB when I am sure that IBCB will improve birth outcomes of my newborn, such as a good childbirth weight and my general good health.” (A woman at 6 months gestation)
“… I think IBCB has nutrients that have health benefits, such as the formation of blood for the pregnant woman and the fetus. Before I migrated to this district, I was sensitized that IBCB has a certain nutrient that helps in the formation of blood. However, I have forgotten the name of the nutrient. Since a pregnant woman needs a lot of blood, I would consume IBCB during pregnancy to increase the amount of my blood.” (A woman at 5 months gestation)
4. Discussion
Study Strengths and Limitations
5. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANC | antenatal care |
| ASFs | animal source foods |
| CCB | conventional common bean |
| FGDs | focus group discussion |
| GMFs | genetically modified foods |
| IBCB | iron-biofortified common bean |
| IDA | iron deficiency anemia |
| LMICs | low- and middle-income countries |
| RDA | Recommended Dietary Allowance |
| WFSP | white-fleshed sweet potato |
| WRA | women of reproductive age |
References
- Brittenham, G.M.; Moir-Meyer, G.; Abuga, K.M.; Datta-Mitra, A.; Cerami, C.; Green, R.; Pasricha, S.R.; Atkinson, S.H. Biology of Anemia: A Public Health Perspective. J. Nutr. 2023, 153, S7–S28. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendations on Maternal and Newborn Care for a Positive Postnatal Experience; World Health Organization: Geneva, Switzerland, 2022.
- Chaparro, C.M.; Suchdev, P.S. Anemia Epidemiology, Pathophysiology, and Etiology in Low- and Middle-Income Countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Gardner, W.M.; Razo, C.; McHugh, T.A.; Hagins, H.; Vilchis-Tella, V.M.; Hennessy, C.; Taylor, H.J.; Perumal, N.; Fuller, K.; Cercy, K.M.; et al. Prevalence, Years Lived with Disability, and Trends in Anaemia Burden by Severity and Cause, 1990–2021: Findings from the Global Burden of Disease Study 2021. Lancet Haematol. 2023, 10, e713–e734. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Paciorek, C.J.; Flores-Urrutia, M.C.; Borghi, E.; Namaste, S.; Wirth, J.P.; Suchdev, P.S.; Ezzati, M.; Rohner, F.; Flaxman, S.R.; et al. National, Regional, and Global Estimates of Anaemia by Severity in Women and Children for 2000–19: A Pooled Analysis of Population-Representative Data. Lancet Glob. Health 2022, 10, e627–e639. [Google Scholar] [CrossRef]
- Baingana, R.K.; Enyaru, J.K.; Tjalsma, H.; Swinkels, D.W.; Davidsson, L. The Aetiology of Anaemia during Pregnancy: A Study to Evaluate the Contribution of Iron Deficiency and Common Infections in Pregnant Ugandan Women. Public Health Nutr. 2015, 18, 1423–1435. [Google Scholar] [CrossRef] [PubMed]
- Glahn, R.P.; Wiesinger, J.A.; Lung’aho, M.G. Iron Concentrations in Biofortified Beans and Nonbiofortified Marketplace Varieties in East Africa Are Similar. J. Nutr. 2020, 150, 3013–3023. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Talegawkar, S.A.; Merialdi, M.; Caulfield, L.E. Dietary Intakes of Women during Pregnancy in Low- and Middle-Income Countries. Public Health Nutr. 2013, 16, 1340–1353. [Google Scholar] [CrossRef]
- Petry, N.; Egli, I.; Zeder, C.; Walczyk, T.; Hurrell, R. Polyphenols and Phytic Acid Contribute to the Low Iron Bioavailability from Common Beans in Young Women. J. Nutr. 2010, 140, 1977–1982. [Google Scholar] [CrossRef]
- Byamugisha, J.; Adero, N.; Kiwanuka, T.S.; Nalwadda, C.K.; Ntuyo, P.; Namagembe, I.; Nabunya, E.; Nakirijja, E.; Mwadime-Ngolo, R.; Mukasa, D.C.; et al. The Effect of Blister Packaging Iron and Folate on Adherence to Medication and Hemoglobin Levels among Pregnant Women at National Referral Hospital Antenatal Clinics in a Low to Middle Income Country: A Randomised Controlled Trial (The IFAd Trial). BMC Pregnancy Childbirth 2022, 22, 179. [Google Scholar] [CrossRef]
- Hummel, M.; Talsma, E.F.; Taleon, V.; Londoño, L.; Brychkova, G.; Gallego, S.; Raatz, B.; Spillane, C. Iron, Zinc and Phytic Acid Retention of Biofortified, Low Phytic Acid, and Conventional Bean Varieties When Preparing Common Household Recipes. Nutrients 2020, 12, 658. [Google Scholar] [CrossRef]
- Petry, N.; Egli, I.; Campion, B.; Nielsen, E.; Hurrell, R. Genetic Reduction of Phytate in Common Bean (Phaseolus vulgaris L.) Seeds Increases Iron Absorption in Young Women. J. Nutr. 2013, 143, 1219–1224. [Google Scholar] [CrossRef]
- Vasconcelos, M.W.; Gruissem, W.; Bhullar, N.K. Iron Biofortification in the 21st Century: Setting Realistic Targets, Overcoming Obstacles, and New Strategies for Healthy Nutrition. Curr. Opin. Biotechnol. 2017, 44, 8–15. [Google Scholar] [CrossRef]
- Bouis, H.E.; Saltzman, A. Improving Nutrition through Biofortification: A Review of Evidence from HarvestPlus, 2003 through 2016. Glob. Food Sec. 2017, 12, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Glahn, R.P.; Noh, H. Redefining Bean Iron Biofortification: A Review of the Evidence for Moving to a High Fe Bioavailability Approach. Front. Sustain. Food Syst. 2021, 5, 682130. [Google Scholar] [CrossRef]
- Turner, R.E. Nutrition in Pregnancy. In Modern Nutrition in Health and Disease; Ross, A.C., Caballero, B., Cousins, R.J., Tucker, K.L., Ziegler, T.R., Eds.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2014; ISBN 9781605474618. [Google Scholar]
- World Health Organization. Iron Supplementation in Postpartum Women; World Health Organization: Geneva, Switzerland, 2016.
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016.
- Astuti, C.N.K.; Prasetyo, B.; Setyowati, D. The Effect of Iron Tablets’ Side Effects on the Level of Compliance to Consuming Iron Tablets in Pregnant Woman: A Systematic Review. World J. Adv. Res. Rev. 2023, 17, 395–403. [Google Scholar] [CrossRef]
- Ba, D.M.; Ssentongo, P.; Kjerulff, K.H.; Na, M.; Liu, G.; Gao, X.; Du, P. Adherence to Iron Supplementation in 22 Sub-Saharan African Countries and Associated Factors among Pregnant Women: A Large Population-Based Study. Curr. Dev. Nutr. 2019, 3, nzz120. [Google Scholar] [CrossRef]
- Kiwanuka, T.S.; Ononge, S.; Kiondo, P.; Namusoke, F. Adherence to Iron Supplements among Women Receiving Antenatal Care at Mulago National Referral Hospital, Uganda-Cross-Sectional Study. BMC Res. Notes 2017, 10, 510. [Google Scholar] [CrossRef]
- Young, M.F.; Griffin, I.; Pressman, E.; McIntyre, A.W.; Cooper, E.; McNanley, T.; Harris, Z.L.; Westerman, M.; O’Brien, K.O. Utilization of Iron from an Animal-Based Iron Source Is Greater than That of Ferrous Sulfate in Pregnant and Nonpregnant Women. J. Nutr. 2010, 140, 2162–2166. [Google Scholar] [CrossRef]
- Kavle, J.A.; Landry, M. Addressing Barriers to Maternal Nutrition in Low- and Middle-Income Countries: A Review of the Evidence and Programme Implications. Matern. Child Nutr. 2018, 14, e12508. [Google Scholar] [CrossRef]
- Tako, E.; Beebe, S.E.; Reed, S.; Hart, J.J.; Glahn, R.P. Polyphenolic Compounds Appear to Limit the Nutritional Benefit of Biofortified Higher Iron Black Bean (Phaseolus vulgaris L.). Nutr. J. 2014, 13, 28. [Google Scholar] [CrossRef]
- Petry, N.; Egli, I.; Gahutu, J.B.; Tugirimana, P.L.; Boy, E.; Hurrell, R. Phytic Acid Concentration Influences Iron Bioavailability from Biofortified Beans in Rwandese Women with Low Iron Status. J. Nutr. 2014, 144, 1681–1687. [Google Scholar] [CrossRef]
- HarvestPlus Iron Bean. Available online: https://bpi.harvestplus.org/bpi_cropmaps.html?id=c1 (accessed on 18 June 2022).
- Birol, E.; Foley, J.; Aytekin, D. Biofortification: The Evidence A Summary of Multi-Disciplinary Research to Help Inform Transformation of Food Systems through the Adoption and Scaling of Nutrient-Enriched Staple Food Crops. 2021. Available online: https://www.harvestplus.org/wp-content/uploads/2021/12/Biofortification_The-Evidence.pdf#:~:text=This%20document%20provides%20a%20summary%20of%20peer-reviewed%20research,deliver%20affordable%20and%20accessible%20nutritious%20food%20for%20all (accessed on 19 June 2022).
- Siwela, M.; Pillay, K.; Govender, L.; Lottering, S. Biofortified Crops for Combating Hidden Hunger in South Africa: Availability, Acceptability, Micronutrient Retention and Bioavailability. Foods 2020, 9, 815. [Google Scholar] [CrossRef]
- Huey, S.L.; Krisher, J.T.; Bhargava, A.; Friesen, V.M.; Konieczynski, E.M.; Mbuya, M.N.N.; Mehta, N.H.; Monterrosa, E.; Nyangaresi, A.M.; Mehta, S. Sensory Acceptability of Biofortified Foods and Food Products: A Systematic Review. Nutr. Rev. 2023, 82, 892–912. [Google Scholar] [CrossRef] [PubMed]
- Uganda Bureau of Statistics; Inner City Fund. Uganda Demographic and Health Survey 2016; Uganda Bureau of Statistics: Kampala, Uganda; ICF: Rockville, MD, USA, 2018. Available online: https://dhsprogram.com/pubs/pdf/FR333/FR333.pdf (accessed on 17 June 2022).
- Buzigi, E.; Pillay, K.; Siwela, M.; Mkhwanazi, B.; Ngidi, M.; Ssozi, J.; Mahinda, B.M.; Isingoma, E.B. Lactating Mothers’ Perceptions and Sensory Acceptability of a Provitamin A Carotenoid–Iron-Rich Composite Dish Prepared from Iron-Biofortified Common Bean and Orange-Fleshed Sweet Potato in Rural Western Uganda. Food Sci. Nutr. 2024, 12, 3949–3963. [Google Scholar] [CrossRef] [PubMed]
- Uganda Bureau of Statistics; Inner City Fund. Uganda Demographic and Health Survey 2016: Key Indicators Report; Uganda Bureau of Statistics: Kampala, Uganda; ICF: Rockville, MD, USA, 2017. Available online: https://www.health.go.ug/sites/default/files/Demographic%20and%20Health%20Survey.pdf (accessed on 26 September 2023).
- Stone, H.; Sidel, J.L. Sensory Evaluation Practices, 3rd ed.; Taylor, S.L., Ed.; Elsevier: Amsterdam, The Netherlands; Academic Press: Cambridge, MA, USA, 2004; ISBN 0126726906. [Google Scholar]
- Lawless, H.T.; Heymann, H. Sensory Evaluation of Food: Priciples and Practises. Food Science Text Series, 2nd ed.; Springer Science+Business Media: New York, NY, USA, 2010; ISBN 978-1-4419-6487-8. [Google Scholar]
- Stewart, A. Basic Statistics and Epidemiology: A Practical Guide, 4th ed.; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2016; ISBN 9781498783545. [Google Scholar]
- Cingi, C.; Muluk, N.B.; Özel, H.E. (Eds.) ENT Diseases: Diagnosis and Treatment During Pregnancy and Lactation; Springer Nature: Cham, Switzerland, 2022; ISBN 9783031053030. [Google Scholar]
- London, V.; Grube, S.; Sherer, D.M.; Abulafia, O. Hyperemesis Gravidarum: A Review of Recent Literature. Pharmacology 2017, 100, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.; Platt, J. Nausea and Vomiting in Pregnancy. Integr. Med. Third Ed. 2012, e2, 491–497. [Google Scholar] [CrossRef]
- Agmon, N.; Sade, S.; Pariente, G.; Rotem, R.; Weintraub, A.Y. Hyperemesis Gravidarum and Adverse Pregnancy Outcomes. Arch. Gynecol. Obstet. 2019, 300, 347–353. [Google Scholar] [CrossRef]
- Durazzo, A.; Camilli, E.; D’Addezio, L.; Sette, S.; Marconi, S.; Piccinelli, R.; Le Donne, C.; Turrini, A.; Marletta, L. Italian Composite Dishes: Description and Classification by LanguaLTM and FoodEx2. Eur. Food Res. Technol. 2020, 246, 287–295. [Google Scholar] [CrossRef]
- National Crops Resources Research Institute NaCRRI Scientists Reap Big on Intellectual Property from Commercialization of Crop Varieties. Available online: https://naro.go.ug/nacrri-scientists-reap-big-on-intellectual-property-from-commercialization-of-crop-varieties/ (accessed on 29 September 2023).
- Buzigi, E.; Pillay, K.; Siwela, M. Effect of Cooking Locally Available Common Bean (Obwelu) on Iron and Zinc Retention, and Pumpkin (Sweet Cream) on Provitamin A Carotenoid Retention in Rural Uganda. Food Sci. Nutr. 2020, 8, 5916–5925. [Google Scholar] [CrossRef]
- Madrera, R.R.; Negrillo, A.C.; Valles, B.S.; Fernández, J.J.F. Phenolic Content and Antioxidant Activity in Seeds of Common Bean (Phaseolus vulgaris L.). Foods 2021, 10, 864. [Google Scholar] [CrossRef]
- Ma, G.; Jin, Y.; Piao, J.; Kok, F.; Guusje, B.; Jacobsen, E. Phytate, Calcium, Iron, and Zinc Contents and Their Molar Ratios in Foods Commonly Consumed in China. J. Agric. Food Chem. 2005, 53, 10285–10290. [Google Scholar] [CrossRef]
- Amico, K.L.; Wieland, M.L.; Weis, J.A.; Sullivan, S.M.; Nigon, J.A.; Sia, I.G. Capacity Building through Focus Group Training in Community-Based Participatory Research. Educ. Health 2011, 24, 638. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample Sizes for Saturation in Qualitative Research: A Systematic Review of Empirical Tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- HarvestPlus HarvestPlus Biofortified Crops Map and Table Updated with 2020 Data—HarvestPlus. Available online: https://www.harvestplus.org/harvestplus-biofortified-crops-map-and-table-updated-with-2020-data/ (accessed on 8 April 2025).
- Murekezi, A.; Oparinde, A.; Birol, E. Consumer Market Segments for Biofortified Iron Beans in Rwanda: Evidence from a Hedonic Testing Study. Food Policy 2017, 66, 35–49. [Google Scholar] [CrossRef]
- Pérez, S.; Oparinde, A.; Birol, E.; Gonzalez, C.; Zeller, M. Consumer Acceptance of an Iron Bean Variety in Northwest Guatemala: The Role of Information and Repeated Messaging. Agric. Food Econ. 2018, 6, 14. [Google Scholar] [CrossRef]
- Beintema, J.J.S.; Luis, S.G.; Talsma, J.R.E.F. Scaling-up Biofortified Beans High in Iron and Zinc through the Feeding Program: A Sensory Acceptance Study with Schoolchildren from Two Departments in Southwest Colombia. Food Sci. Nutr. 2018, 6, 1138–1145. [Google Scholar] [CrossRef]
- Choo, E.; Dando, R. The Impact of Pregnancy on Taste Function. Chem. Senses 2017, 42, 279–286. [Google Scholar] [CrossRef]
- Petry, N.; Rohner, F.; Gahutu, J.B.; Campion, B.; Boy, E.; Tugirimana, P.L.; Zimmerman, M.B.; Zwahlen, C.; Wirth, J.P.; Moretti, D. In Rwandese Women with Low Iron Status, Iron Absorption from Low-Phytic Acid Beans and Biofortified Beans Is Comparable, but Low-Phytic Acid Beans Cause Adverse Gastrointestinal Symptoms. J. Nutr. 2016, 146, 970–975. [Google Scholar] [CrossRef]
- Govender, L.; Pillay, K.; Derera, J.; Siwela, M. Acceptance of a Complementary Food Prepared with Yellow, Provitamin A-Biofortified Maize by Black Caregivers in Rural KwaZulu-Natal. S. Afr. J. Clin. Nutr. 2014, 27, 217–221. [Google Scholar] [CrossRef]
- Govender, L.; Pillay, K.; Siwela, M.; Modi, A.T.; Mabhaudhi, T. Consumer Perceptions and Acceptability of Traditional Dishes Prepared with Provitamin A-Biofortified Maize and Sweet Potato. Nutrients 2019, 11, 1577. [Google Scholar] [CrossRef] [PubMed]
- Buzigi, E.; Pillay, K.; Siwela, M.; Mkhwanazi, B.; Ngidi, M. Food Production Diversity Based on Food Groups Is Associated with Minimum Dietary Diversity and Dietary Diversity among Lactating Mothers Residing in Subsistence Farming Households in Rural Kyankwanzi District, Uganda. BMC Public Health 2025, 25, 1020. [Google Scholar] [CrossRef] [PubMed]
- Wiesinger, J.A.; Cichy, K.A.; Tako, E.; Glahn, R.P. The Fast Cooking and Enhanced Iron Bioavailability Properties of the Manteca Yellow Bean (Phaseolus vulgaris L.). Nutrients 2018, 10, 1609. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.J.; Gallego-Castillo, S.; Talsma, E.F.; Álvarez, D. The Acceptance of Zinc Biofortified Rice in Latin America: A Consumer Sensory Study and Grain Quality Characterization. PLoS ONE 2020, 15, e0242202. [Google Scholar] [CrossRef]
- Lim, C.Y.; In, J. Considerations for Crossover Design in Clinical Study. Korean J. Anesthesiol. 2021, 74, 293–299. [Google Scholar] [CrossRef]
- Lim, J. Hedonic Scaling: A Review of Methods and Theory. Food Qual. Prefer. 2011, 22, 733–747. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable (Units) | IBCB/100 g $ | CCB/100 g |
|---|---|---|
| Iron (mg, mean ± SD) | 9.5 ± 0.3 a | 5.1 ± 0.2 b |
| Total polyphenols (mg GAE, mean ± SD) | 572 ± 10 a | 453 ± 12 b |
| Phytate (mg, mean ± SD) | 1321 ± 10 a | 982 ± 20 b |
| Phytate: iron molar ratio | 12:1 a | 16:1 b |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Adolescent | ||
| Yes (10–19 years old) | 24 | 23.1 |
| No (≥20 years old) | 80 | 76.9 |
| Completed primary education | ||
| Yes | 30 | 28.8 |
| No | 74 | 71.2 |
| Trimester | ||
| Second | 49 | 47.1 |
| Third | 55 | 52.8 |
| Household head | ||
| Male | 89 | 85.6 |
| Female | 15 | 15.4 |
| Subsistence farmer | ||
| Yes | 91 | 87.5 |
| No | 13 | 12.5 |
| Sensory Attribute | Acceptable | Chi-Square | p-Value | |
|---|---|---|---|---|
| Yes, n(%) | No, n(%) | |||
| Color | 0.338 | 0.56 | ||
| WFSP + IBCB WFSP + CCB | 103(99.0) 102(98.1) | 1(1.0) 2(1.9) | ||
| Texture | 0.000 | 1.00 | ||
| WFSP + IBCB | 101(97.1) | 03(2.9) | ||
| WFSP + CCB | 101(97.1) | 03(2.9) | ||
| Aroma | 1.045 | 0.307 | ||
| WFSP + IBCB | 98(94.2) | 06(5.8) | ||
| WFSP + CCB | 101(97.1) | 03(2.9) | ||
| Taste | 0.243 | 0.62 | ||
| WFSP + IBCB | 94(90.4) | 10(9.6) | ||
| WFSP + CCB | 96(92.3) | 08(7.7) | ||
| Overall acceptability | 0.116 | 0.73 | ||
| WFSP + IBCB | 100(96.2) | 04(3.8) | ||
| WFSP + CCB | 99(95.2) | 05(4.8) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buzigi, E.; Pillay, K.; Siwela, M.; Mkhwanazi, B.; Ngidi, M.; Mahinda, B.M. Perceptions and Acceptability of a Low Phytate: Iron Molar Ratio Biofortified Bean and Sweet Potato Dish Among Pregnant Women in Rural Uganda. Nutrients 2025, 17, 1641. https://doi.org/10.3390/nu17101641
Buzigi E, Pillay K, Siwela M, Mkhwanazi B, Ngidi M, Mahinda BM. Perceptions and Acceptability of a Low Phytate: Iron Molar Ratio Biofortified Bean and Sweet Potato Dish Among Pregnant Women in Rural Uganda. Nutrients. 2025; 17(10):1641. https://doi.org/10.3390/nu17101641
Chicago/Turabian StyleBuzigi, Edward, Kirthee Pillay, Muthulisi Siwela, Blessing Mkhwanazi, Mjabuliseni Ngidi, and Babra Muhindo Mahinda. 2025. "Perceptions and Acceptability of a Low Phytate: Iron Molar Ratio Biofortified Bean and Sweet Potato Dish Among Pregnant Women in Rural Uganda" Nutrients 17, no. 10: 1641. https://doi.org/10.3390/nu17101641
APA StyleBuzigi, E., Pillay, K., Siwela, M., Mkhwanazi, B., Ngidi, M., & Mahinda, B. M. (2025). Perceptions and Acceptability of a Low Phytate: Iron Molar Ratio Biofortified Bean and Sweet Potato Dish Among Pregnant Women in Rural Uganda. Nutrients, 17(10), 1641. https://doi.org/10.3390/nu17101641