
Plasma Bacterial Metabolites in Crohn’s Disease Pathogenesis and Complications

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
- -
- Written informed consent to participate in this study;
- -
- Patients with Crohn’s disease and a control group—adults.
- -
- Age < 18 years;
- -
- Failure to express informed consent to participate in this research study.
2.1. Metabolite (Short-Chain Fatty Acids, TMAO Profile) Profiling
2.2. Statistical Analysis
3. Results
3.1. Clinical Manifestation of CD with Analysis of Correlation (BMI, Time of Diagnosis, Duration, CRP)
3.1.1. Inflammation Status
3.1.2. Crohn’s Disease Complications
3.2. Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IBDs | inflammatory bowel diseases |
| CD | Crohn’s disease |
| UC | ulcerative colitis |
| AA | acetic acid |
| BA | butyric acid |
| CA | caproic acid |
| IBA | isobutyric acid |
| LA | lactic acid |
| 2MeBA | 2-methylbutyric acid |
| PA | propionic acid |
| VA | valeric acid |
| GPC | glycerophosphorylcholine |
| TMA | trimethylamine |
| TMAO | trimethylamine N-oxide |
| ROC | receiver operating characteristic |
| GM | gut microbiota |
| GPRs | G-protein-coupled receptors |
| HDAC | histone deacetylase |
| EEN | exclusive enteral nutrition |
| CDED | CD elimination diet |
| PEN | partial enteral nutrition |
References
- Montrose, J.A.; Kurada, S.; Fischer, M. Current and future microbiome-based therapies in inflammatory bowel disease. Curr. Opin. Gastroenterol. 2024, 40, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Paidimarri, S.P.; Ayuthu, S.; Chauhan, Y.D.; Bittla, P.; Mirza, A.A.; Saad, M.Z.; Khan, S. Contribution of the Gut Microbiome to the Perpetuation of Inflammation in Crohn’s Disease: A Systematic Review. Cureus 2024, 16, e67672. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zheng, J.; Sun, Q.; Zhang, M.; Liu, C.; Su, Q.; Zhang, L.; Xu, Z.; Lu, W.; Ching, J.; Tang, W.; et al. Noninvasive, microbiome-based diagnosis of inflammatory bowel disease. Nat. Med. 2024, 30, 3555–3567. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sun, M.; Du, B.; Shi, Y.; Lu, Y.; Zhou, Y.; Liu, B. Combined Signature of the Fecal Microbiome and Plasma Metabolome in Patients with Ulcerative Colitis. Med. Sci. Monit. 2019, 25, 3303–3315. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lavelle, A.; Sokol, H. Gut microbiota-derived metabolites as key actors in inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Andrzejewska, M.; Dereziński, P.; Kokot, Z.; Grzymisławski, M. Metabolomics and proteomics in the diagnosis of inflammatory bowel dis-eases. Forum Zaburzeń Metab. 2016, 7, 141–151. [Google Scholar]
- De Preter, V. Metabolomics in the clinical diagnosis of inflammatory bowel disease. Dig. Dis. 2015, 33 (Suppl. S1), 2–10. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Lv, T.; Dong, S.; Cui, Z.; Luo, X.; Jia, B.; Jeon, C.; Zhang, J. Association between intestinal microbiome and inflammatory bowel disease: Insights from bib-liometric analysis. Comput. Struct. Biotechnol. J. 2022, 20, 1716–1725. [Google Scholar] [CrossRef]
- De Freitas Lins Neto, M.; Ximenes Verdi, G.; de Oliveria Veras, A.; Veras, M.D.O.; Caetano, L.C.; Ursulino, J.S. Use of metabolomics to the diagnosis of inflammatory bowel disease. Arq. Gastroenterol. 2020, 57, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Cai, Y.; Yao, H.; Lin, C.; Xie, Y.; Tang, S.; Zhang, A. Small molecule metabolites: Discovery of biomarkers and thera-peutic targets. Signal Transduct. Target. Ther. 2023, 8, 132. [Google Scholar] [CrossRef]
- Kim, K.; Lee, Y.; Chae, W.; Cho, J.Y. An improved method to quantify short-chain fatty acids in biological samples using gas chromatography-mass spectrometry. Metabolites 2022, 12, 525. [Google Scholar] [CrossRef]
- Kul, S.; Caliskan, Z.; Guvenc, T.S.; Celik, F.B.; Sarmis, A.; Atici, A.; Konal, O.; Akıl, M.; Cumen, A.S.; Bilgic, N.M.; et al. Gut microbiota-derived metabolite trimethylamine N-oxide and biomarkers of inflammation are linked to endothelial and coronary microvascular function in patients with inflammatory bowel disease. Microvasc. Res. 2022, 146, 104458. [Google Scholar] [CrossRef]
- Papa, A.; Santini, P.; De Lucia, S.S.; Maresca, R.; Porfidia, A.; Pignatelli, P.; Gasbarrini, A.; Violi, F.; Pola, R. Gut dysbiosis-related thrombosis in inflammatory bowel disease: Potential disease mechanisms and emerging therapeutic strategies. Thromb. Res. 2023, 232, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Laryushina, Y.; Samoilova-Bedych, N.; Turgunova, L.; Kozhakhmetov, S.; Alina, A.; Suieubayev, M.; Mukhanbetzhanov, N. Alterations of the Gut Microbiome and TMAO Levels in Patients with Ulcerative Colitis. J. Clin. Med. 2024, 13, 5794. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, M.; Buey, B.; Grasa, L.; Mesonero, J.E.; Latorre, E. Protective role of short-chain fatty acids on intestinal oxidative stress induced by TNF-α. Cell Stress Chaperon- 2024, 29, 769–776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fu, Y.; Lyu, J.; Wang, S. The role of intestinal microbes on intestinal barrier function and host immunity from a metabolite perspective. Front. Immunol. 2023, 14, 1277102. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Shang, J.; Liu, L.; Tang, Z.; Meng, X. Strains producing different short-chain fatty acids alleviate DSS-induced ulcerative colitis by regulating intestinal microecology. Food Funct. 2022, 13, 12156–12169. [Google Scholar] [CrossRef] [PubMed]
- Onyszkiewicz, M.; Gawrys-Kopczynska, M.; Konopelski, P.; Aleksandrowicz, M.; Sawicka, A.; Koźniewska, E.; Samborowska, E.; Ufnal, M. Butyric acid, a gut bacteria metabolite, lowers arterial blood pressure via colon–vagus nerve signaling and GPR41/43 receptors. Pflugers Arch. 2019, 471, 1441–1453. [Google Scholar] [CrossRef]
- Maksymiuk, K.M.; Szudzik, M.; Gawryś-Kopczyńska, M.; Onyszkiewicz, M.; Samborowska, E.; Mogilnicka, I.; Ufnal, M. Trimethylamine, a gut bacteria metabolite and air pollutant, increases blood pressure and markers of kidney damage including proteinuria and KIM-1 in rats. J. Transl. Med. 2022, 20, 470. [Google Scholar] [CrossRef]
- Kolho, K.-L.; Pessia, A.; Jaakkola, T.; de Vos, W.M.; Velagapudi, V. Faecal and serum metabolomics in paediatric inflammatory bowel disease. J. Crohn’s Colitis 2016, 11, 321–334. [Google Scholar] [CrossRef]
- Jaworska, K.; Konop, M.; Bielinska, K.; Hutsch, T.; Dziekiewicz, M.; Banaszkiewicz, A.; Ufnal, M. Inflammatory bowel disease is associated with increased gut-to-blood penetration of short-chain fatty acids: A new, non-invasive marker of a functional intestinal lesion. Exp. Physiol. 2019, 104, 1226–1236. [Google Scholar] [CrossRef] [PubMed]
- Jagt, J.Z.; Verburgt, C.M.; de Vries, R.; de Boer, N.K.H.; Benninga, M.A.; de Jonge, W.J.; van Limbergen, J.E.; de Meij, T.G.J. Faecal metabolomics in paediatric inflammatory bowel disease: A systematic review. J. Crohn’s Colitis 2022, 16, 1777–1790. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, J.; Kulecka, M.; Zawada, I.; Żeber-Lubecka, N.; Paziewska, A.; Graca-Pakulska, K.; Dąbkowski, K.; Skubisz, K.; Cybula, P.; Ambrożkiewicz, F.; et al. The gastric microbiota in patients with Crohn’s disease; a preliminary study. Sci. Rep. 2021, 11, 17866. [Google Scholar] [CrossRef] [PubMed]
- Svolos, V.; Hansen, R.; Nichols, B.; Quince, C.; Ijaz, U.Z.; Papadopoulou, R.T.; Edwards, C.A.; Watson, D.; Alghamdi, A.; Brejnrod, A.; et al. Treatment of active Crohn’s disease with an ordinary food-based diet that replicates exclusive enteral nutrition. Gastroenterology 2019, 156, 1354–1367.e6. [Google Scholar] [CrossRef] [PubMed]
- Dąbek-Drobny, A.; Kaczmarczyk, O.; Woźniakiewicz, M.; Paśko, P.; Dobrowolska-Iwanek, J.; Woźniakiewicz, A.; Piątek-Guziewicz, A.; Zagrodzki, P.; Zwolińska-Wcisło, M. Association between fecal short-chain fatty acid levels, diet, and body mass index in patients with inflammatory bowel disease. Biology 2022, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Ambrozkiewicz, F.; Karczmarski, J.; Kulecka, M.; Paziewska, A.; Niemira, M.; Zeber-Lubecka, N.; Zagorowicz, E.; Kretowski, A.; Ostrowski, J. In search for interplay between stool microRNAs, microbiota and short chain fatty acids in Crohn disease—A preliminary study. BMC Gastroenterol. 2020, 20, 307. [Google Scholar] [CrossRef]
- Marques, J.G.; Shokry, E.; Frivolt, K.; Werkstetter, K.J.; Brückner, A.; Schwerd, T.; Koletzko, S.; Koletzko, B. Metabolomic signatures in pediatric Crohn’s disease patients with mild or qui-escent disease treated with partial enteral nutrition: A feasibility study. SLAS Technol. 2021, 26, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Colgan, S.P.; Wang, R.X.; Hall, C.H.T.; Bhagavatula, G.; Lee, J.S. Revisiting the "starved gut" hypothesis in inflammatory bowel disease. Immunome-tabolism 2023, 5, e0016. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.A.; Ogawa, S.A.; Chau, L.; Whelan, K.A.; Hamilton, K.E.; Chen, J.; Tan, L.; Chen, E.Z.; Keilbaugh, S.; Fogt, F.; et al. Mitochondrial dysfunction in inflammatory bowel disease alters intestinal epithelial metabolism of hepatic acylcarnitines. J. Clin. Investig. 2021, 131, e133371. [Google Scholar] [CrossRef]
- Russo, E.; Giudici, F.; Fiorindi, C.; Ficari, F.; Scaringi, S.; Amedei, A. Immunomodulating activity and therapeutic effects of short chain fatty acids and tryptophan post-biotics in inflammatory bowel disease. Front. Immunol. 2019, 22, 2754. [Google Scholar] [CrossRef]
- Niccolai, E.; Boem, F.; Russo, E.; Amedei, A. The gut–brain axis in the neuropsychological disease model of obesity: A classical movie revised by the emerging director “microbiome”. Nutrients 2019, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Säemann, M.D.; Böhmig, G.A.; Österreicher, C.H.; Burtscher, H.; Parolini, O.; Diakos, C.; Stöckl, J.; Hörl, W.H.; Zlabinger, G.J. Anti-inflammatory effects of sodium butyrate on human monocytes: Potent inhibition of IL-12 and up-regulation of IL-10 production. FASEB J. 2000, 14, 2380–2382. [Google Scholar] [CrossRef] [PubMed]
- Eder, P. The utility of biomarkers in the assessment of the inflammatory bowel disease activity—Practical issues. Gastroen-Terologia Klin. 2018, 10, 52–63. [Google Scholar]
- Ghiboub, M.; Penny, S.; Verburgt, C.M.; Boneh, R.S.; Wine, E.; Cohen, A.; Dunn, K.A.; Pinto, D.M.; Benninga, M.A.; de Jonge, W.J.; et al. Metabolome changes with diet-induced remission in pediatric crohn’s disease. Gastroenterology 2022, 163, 922–936.e15. [Google Scholar] [CrossRef] [PubMed]
- Osaki, H.; Jodai, Y.; Koyama, K.; Omori, T.; Horiguchi, N.; Kamano, T.; Funasaka, K.; Nagasaka, M.; Nakagawa, Y.; Shibata, T.; et al. Clinical response and changes in the fecal microbiota and metabolite levels after fecal microbiota transplantation in patients with inflammatory bowel disease and recurrent Clostridioides difficile infection. Fujita Med. J. 2021, 7, 87–98. [Google Scholar] [CrossRef]
- Kaczmarczyk, O.; Dąbek-Drobny, A.; Woźniakiewicz, M.; Paśko, P.; Dobrowolska-Iwanek, J.; Woźniakiewicz, A.; Piątek-Guziewicz, A.; Zagrodzki, P.; Mach, T.; Zwolińska-Wcisło, M. Fecal levels of lactic, succinic and short-chain fatty acids in patients with ulcerative colitis and crohn disease: A pilot study. J. Clin. Med. 2021, 10, 4701. [Google Scholar] [CrossRef] [PubMed]
- Rogler, G.; Singh, A.; Kavanaugh, A.; Rubin, D.T. Extraintestinal manifestations of inflammatory bowel disease: Current concepts, treatment, and implications for disease management. Gastroenterology 2021, 161, 1118–1132. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, D.; Mao, M.; Liu, W.; Wang, Y.; Liang, Y.; Cao, W.; Zhong, X. Betaine ameliorates acute sever ulcerative colitis by inhibiting oxidative stress induced inflammatory pyroptosis. Mol. Nutr. Food Res. 2022, 66, e2200341. [Google Scholar] [CrossRef]
- Zhao, N.; Yang, Y.; Chen, C.; Jing, T.; Hu, Y.; Xu, H.; Wang, S.; He, Y.; Liu, E.; Cui, J. Betaine supplementation alleviates dextran sulfate sodium-induced colitis via regulating the inflammatory response, enhancing the intestinal barrier, and altering gut microbiota. Food Funct. 2022, 13, 12814–12826. [Google Scholar] [CrossRef]
- Gallagher, K.; Catesson, A.; Griffin, J.L.; Holmes, E.; Williams, H.R.T. Metabolomic analysis in inflammatory bowel disease: A systematic review. J. Crohn’s Colitis 2021, 15, 813–826. [Google Scholar] [CrossRef]
- Liu, H.; Xu, M.; He, Q.; Wei, P.; Ke, M.; Liu, S. Untargeted serum metabolomics reveals specific metabolite abnormalities in patients with Crohn’s disease. Front. Med. 2022, 9, 814839. [Google Scholar] [CrossRef] [PubMed]
- Limketkai, B.N.; Hamideh, M.; Shah, R.; Sauk, J.S.; Jaffe, N. Dietary Patterns and Their Association With Symptoms Activity in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2022, 28, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Hashash, J.G.; Elkins, J.; Lewis, J.D.; Binion, D.G. AGA Clinical Practice Update on Diet and Nutritional Therapies in Patients with Inflammatory Bowel Disease: Expert Review. Gastroenterology 2024, 166, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Sasson, A.N.; Ananthakrishnan, A.N.; Raman, M. Diet in Treatment of Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2021, 19, 425–435.e3. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Crohn’s Disease | Control | |
|---|---|---|
| Number | 29 | 30 |
| Sex (male/female) | 13/16 | 10/20 |
| Age | 33.7 ± 14 | 41.8 ± 14 |
| BMI—body mass index [kg/m2] | 23.4 ± 4.9 | 31.7 ± 6.5 |
| WBC—white blood cell [tys/µL] | 7.8 ± 2.8 | 6.5 ± 1.2 |
| RBC—red blood cell [mln/µL] | 4.5 ± 0.7 | 4.8 ± 0.5 |
| HGB hemoglobin [g/dL] | 12.6 ± 1.9 | 14.3 ± 1.3 |
| HCT—hematocrit [%] | 37.6 ± 4.9 | 41.4 ± 3.3 |
| PLT platelet count [tys/µL] | 289.1 ± 91.2 | 276.2 ± 48.4 |
| MCV mean corpuscular volume [fL] | 84.1 ± 7.7 | 85.5 ± 4.7 |
| ALT—alanine aminotransferase [U/L] | 19.0 ± 8.6 | NA |
| AST—aspartate aminotransferase [U/L] | 22.1 ± 6.9 | NA |
| GGTP—gamma-glutamyl transferase [U/L] | 16.7 ± 10.6 | NA |
| Creatinine [mg/dL] | 0.8 ± 0.1 | 0.8 ± 0.1 |
| CRP—C-Reactive Protein [mg/L] | 15.4 ± 21.1 | NA |
| Remission, n [%] | 16 [55.2] | - |
| Family burden, n [%] | 15 [51.7] | 14 [46.7] |
| Age of diagnosis, n [%] | ||
| ≤16 | 8 [27.6] | - |
| 17–40 | 16 [55.2] | - |
| 40 | 5 [17.2] | - |
| Disease duration [years] | ||
| ≤1 | 3 [10.3] | |
| 1–5 | 5 [17.2] | |
| 5–10 | 13 [44.8] | |
| >10 | 8 [27.6] | |
| Operations | 16 [55.2] | |
| Treatment (current): | ||
| Immunosuppressants- | 16 [55.17] | |
| Glucocorticoids- | 9 [31.03] | |
| Biological therapy- | 14 [48.28] | |
| Aminosalicylic acid (ASA) | 26 [89.66] | |
| Inflammation of upper digestive tract (esophagus, stomach, duodenum) | 16 [55.2] | |
| Location, n [%] | ||
| Ileal | 4 [13.8] | - |
| Colonic | 5 [17.2] | - |
| Ileocolonic | 20 [69.0] | - |
| H. pylori infection, n [%] | 8 [27.6] | - |
| Smoking status, n [%] | ||
| Current-smoker | 5 [17.2] | 0 |
| Ex-smoker | 4 [13.8] | 1 [3.0] |
| Never-smoker | 20 [68.9] | 29 [97.0] |
| (a) | ||
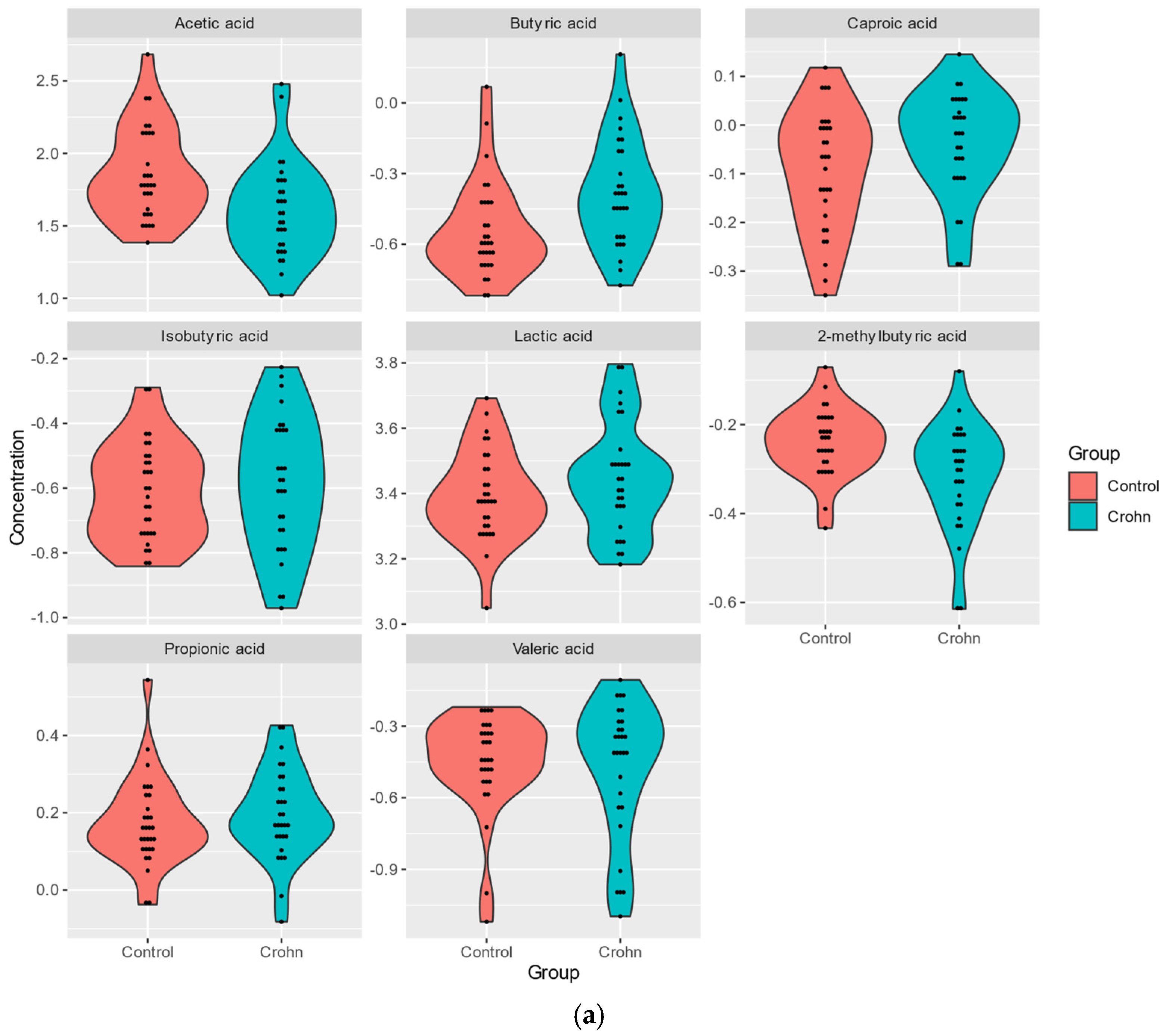
| SCFA Metabolites | p-Value | FC Control/Crohn’s |
| AA | 0.004 | 1.696 |
| BA | 0.004 | 0.682 |
| 2MeBA | 0.008 | 1.168 |
| CA | 0.080 | 0.892 |
| PA | 0.262 | 0.948 |
| LA | 0.294 | 0.863 |
| IBA | 0.510 | 0.905 |
| VA | 0.722 | 0.973 |
| (b) | ||
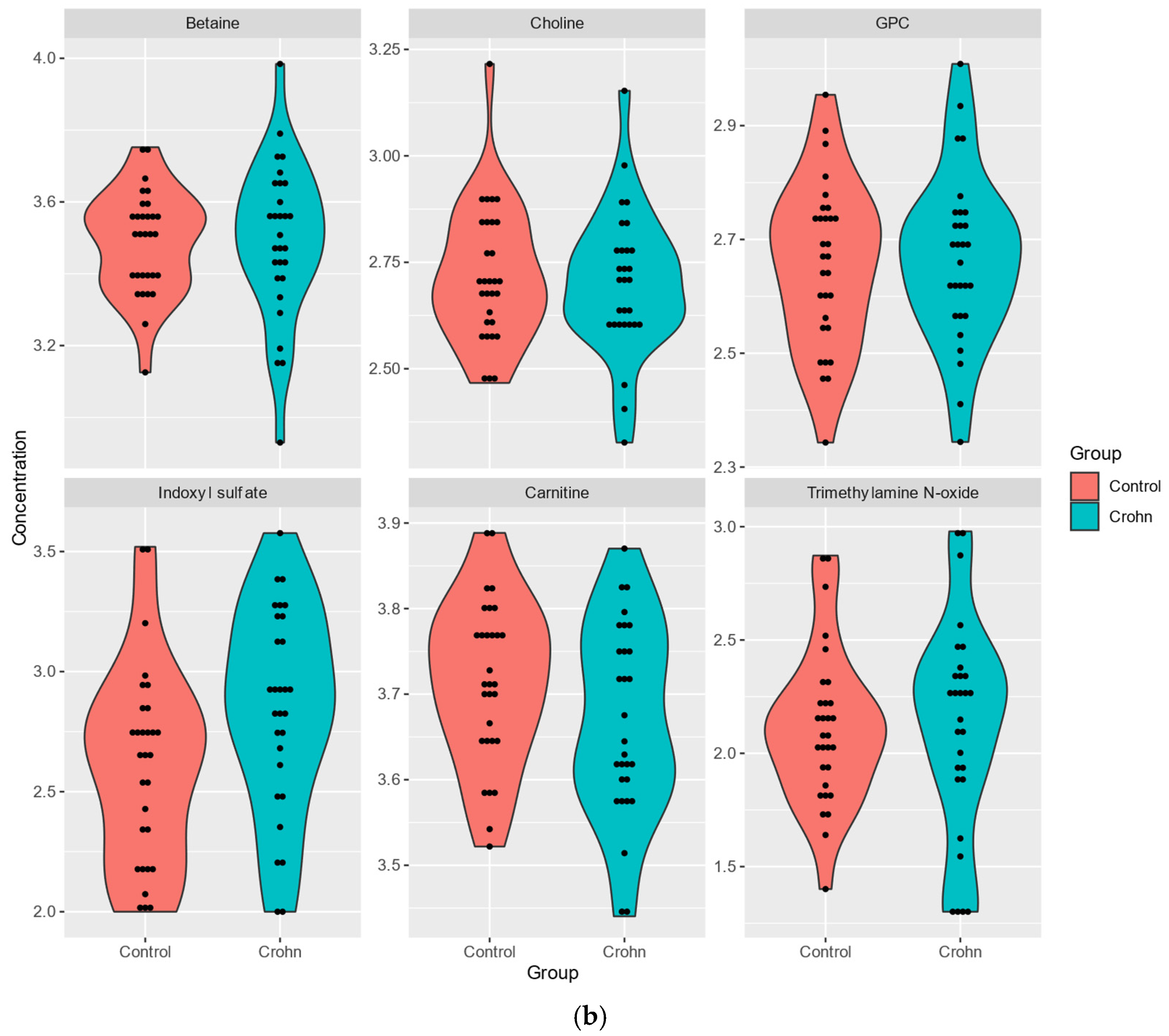
| Metabolite of TMAO Panel | p-Value | FC Control/Crohn’s |
| Indoxyl sulfate | 0.023 | 0.624 |
| carnitine | 0.121 | 1.103 |
| TMAO | 0.539 | 0.816 |
| betaine | 0.679 | 0.926 |
| GPC | 0.863 | 0.966 |
| choline | 0.958 | 1.033 |
| Disease Behavior Structuring/Inflammatory | p-Value | FC |
|---|---|---|
| AA | 0.983 | 0.645 |
| BA | 0.199 | 0.690 |
| betaine | 0.308 | 1.028 |
| CA | 0.199 | 1.107 |
| choline | 0.308 | 0.789 |
| GPC | 0.812 | 0.948 |
| IBA | 0.268 | 0.840 |
| Indoxyl sulfate | 0.0484 | 0.515 |
| carnitine | 0.268 | 0.890 |
| LA | 0.0251 | 0.753 |
| 2MeBA | 0.88 | 0.987 |
| PA | 0.589 | 0.913 |
| TMAO | 0.0829 | 0.423 |
| VA | 0.742 | 0.966 |
| Metabolite | p-Value | FC |
|---|---|---|
| AA | 0.668 | 1.730 |
| BA | 0.071 | 0.489 |
| betaine | 0.717 | 0.906 |
| CA | 0.371 | 1.121 |
| choline | 0.717 | 1.029 |
| GPC | 0.0832 | 1.439 |
| IBA | 0.272 | 0.764 |
| Indoxyl sulfate | 0.0423 | 0.578 |
| carnitine | 0.818 | 1.003 |
| LA | 0.192 | 1.219 |
| 2MeBA | 0.272 | 1.127 |
| PA | 0.371 | 0.863 |
| TMAO | 0.0227 | 0.286 |
| VA | 1 | 0.958 |
| Inflammation of Upper Digestive Tract | p-Value | FC | Inflammation of Upper Digestive Tract—Duodenum | p-Value | FC |
|---|---|---|---|---|---|
| AA | 0.199 | 0.843 | AA | 0.084 | 1.122 |
| BA | 0.249 | 0.776 | BA | 0.492 | 0.846 |
| betaine | 0.983 | 0.916 | betaine | 0.947 | 0.922 |
| CA | 0.170 | 1.110 | CA | 0.642 | 1.017 |
| choline | 0.232 | 0.766 | choline | 0.438 | 0.825 |
| GPC | 0.714 | 0.898 | GPC | 0.021 | 0.727 |
| IBA | 0.779 | 0.972 | IBA | 0.340 | 1.235 |
| Indoxyl sulfate | 0.017 | 0.514 | Indoxyl sulfate | 0.046 | 0.539 |
| carnitine | 0.215 | 0.873 | carnitine | 0.035 | 0.827 |
| LA | 0.199 | 0.765 | LA | 0.122 | 0.733 |
| 2MeBA | 0.650 | 0.907 | 2MeBA | 0.492 | 0.895 |
| PA | 0.056 | 0.801 | PA | 0.055 | 0.813 |
| TMAO | 0.020 | 0.370 | TMAO | 0.023 | 0.519 |
| VA | 0.554 | 0.956 | VA | 0.637 | 1.185 |
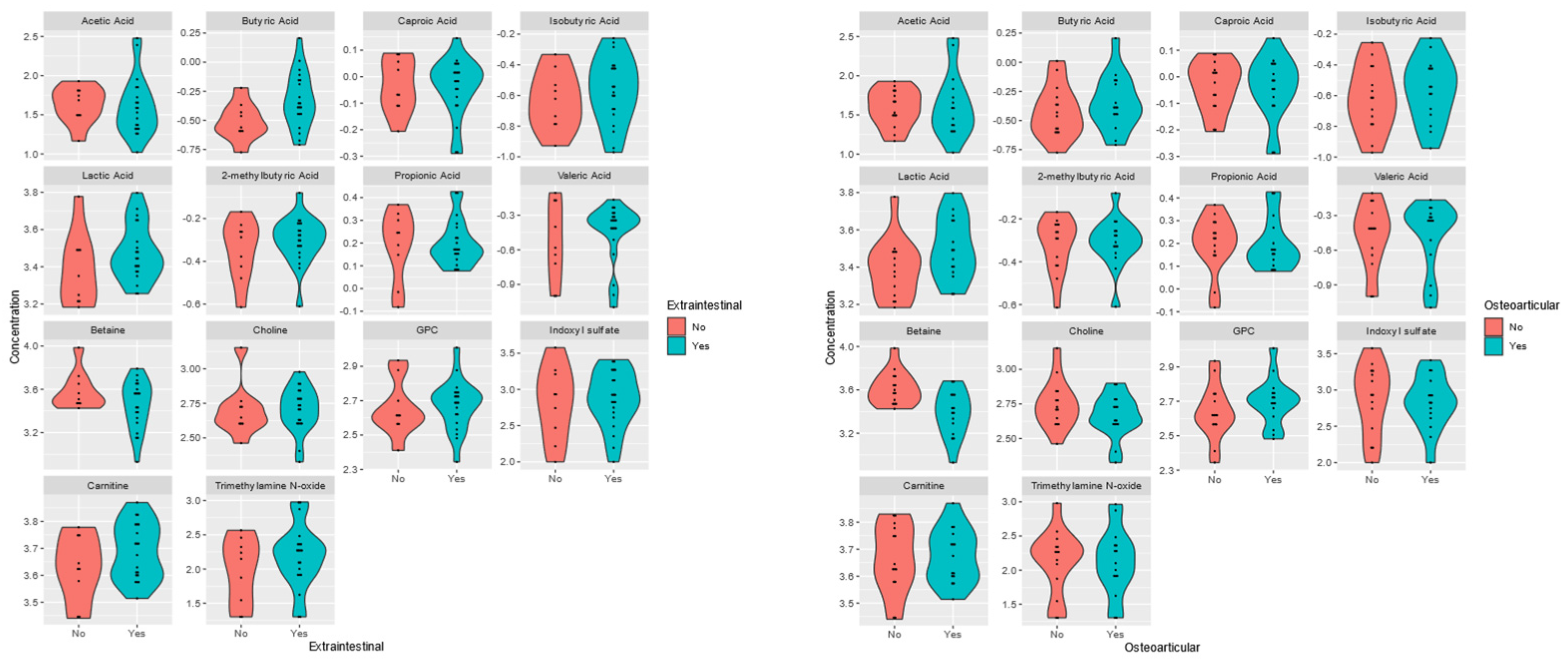
| Complications/Manifestations of CD | Perianal (n = 15) | Extraintestinal (n = 20) | Osteoarticular (n = 15) | |||
|---|---|---|---|---|---|---|
| Metabolite | p-Value | FC | p-Value | FC No/Yes | p-Value | FC No/Yes |
| AA | 0.112 | 1.17 | 0.532 | 0.778 | 0.847 | 0.647 |
| BA | 0.041 | 0.64 | 0.044 | 0.602 | 0.425 | 0.822 |
| betaine | 0.683 | 1.15 | 0.253 | 1.323 | 0.002 | 1.647 |
| CA | 0.847 | 1.04 | 0.945 | 1.007 | 1.000 | 1.003 |
| carnitine | 0.134 | 0.85 | 0.317 | 0.873 | 0.847 | 0.990 |
| choline | 0.561 | 1.00 | 0.417 | 1.033 | 0.400 | 1.238 |
| GPC | 0.983 | 0.98 | 0.501 | 0.969 | 0.331 | 0.885 |
| IBA | 0.914 | 1.04 | 0.501 | 0.839 | 0.591 | 0.895 |
| indoxyl | 0.879 | 1.11 | 0.962 | 1.126 | 0.631 | 1.290 |
| LA | 0.112 | 0.83 | 0.183 | 0.842 | 0.093 | 0.777 |
| 2MeBA | 0.310 | 0.93 | 0.532 | 0.917 | 0.880 | 0.981 |
| PA | 0.270 | 0.90 | 0.627 | 1.008 | 0.505 | 1.006 |
| TMAO | 0.444 | 0.72 | 0.383 | 0.585 | 0.878 | 0.956 |
| VA | 0.88 | 0.637 | 0.940 | 0.600 | 0.982 | |
| Biological Therapy; n = 14 | Glucocorticoid Therapy; n = 9 | Aminosalicylates; n = 26 | Immunosuppressants;n = 16 | |||||
|---|---|---|---|---|---|---|---|---|
| Metabolite | p-Value | FC | p-Value | FC | p-Value | FC | p-Value | FC |
| AA | 0.652 | 1.00 | 0.835 | 1.50 | 0.660 | 2.52 | 0.746 | 1.01 |
| BA | 0.652 | 0.86 | 0.764 | 0.80 | 0.350 | 0.64 | 0.374 | 1.45 |
| betaine | 0.377 | 0.80 | 0.562 | 1.12 | 0.281 | 0.72 | 0.914 | 0.95 |
| CA | 0.014 | 0.82 | 0.501 | 1.08 | 0.710 | 1.05 | 0.846 | 1.01 |
| choline | 0.033 | 0.78 | 0.049 | 1.28 | 0.350 | 0.75 | 0.948 | 0.98 |
| GPC | 0.217 | 0.82 | 0.444 | 1.16 | 0.067 | 0.68 | 0.475 | 0.93 |
| IBA | 0.377 | 1.19 | 0.472 | 0.89 | 0.660 | 0.88 | 0.503 | 1.20 |
| Indoxyl sulfate | 0.810 | 0.83 | 0.099 | 0.64 | 0.452 | 1.24 | 0.497 | 0.75 |
| carnitine | 0.949 | 1.00 | 0.234 | 1.12 | 0.429 | 0.84 | 0.682 | 0.95 |
| LA | 1.000 | 1.02 | 0.085 | 1.22 | 0.516 | 0.78 | 0.101 | 1.24 |
| 2MeBA | 0.112 | 0.87 | 0.116 | 1.16 | 0.761 | 1.03 | 0.092 | 0.87 |
| PA | 0.914 | 0.97 | 0.764 | 0.99 | 0.281 | 0.81 | 0.423 | 1.09 |
| TMAO | 0.844 | 1.15 | 0.085 | 0.36 | 0.886 | 0.78 | 0.645 | 1.23 |
| VA | 0.793 | 1.02 | 0.524 | 1.13 | 0.197 | 1.50 | 0.693 | 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deskur, A.; Ambrożkiewicz, F.; Samborowska, E.; Błogowski, W.; Sulikowski, T.; Białek, A.; Zawada, I.; Dąbkowski, K.; Mitrus, J.; Karczmarski, J.; et al. Plasma Bacterial Metabolites in Crohn’s Disease Pathogenesis and Complications. Nutrients 2025, 17, 74. https://doi.org/10.3390/nu17010074
Deskur A, Ambrożkiewicz F, Samborowska E, Błogowski W, Sulikowski T, Białek A, Zawada I, Dąbkowski K, Mitrus J, Karczmarski J, et al. Plasma Bacterial Metabolites in Crohn’s Disease Pathogenesis and Complications. Nutrients. 2025; 17(1):74. https://doi.org/10.3390/nu17010074
Chicago/Turabian StyleDeskur, Anna, Filip Ambrożkiewicz, Emilia Samborowska, Wojciech Błogowski, Tadeusz Sulikowski, Andrzej Białek, Iwona Zawada, Krzysztof Dąbkowski, Joanna Mitrus, Jakub Karczmarski, and et al. 2025. "Plasma Bacterial Metabolites in Crohn’s Disease Pathogenesis and Complications" Nutrients 17, no. 1: 74. https://doi.org/10.3390/nu17010074
APA StyleDeskur, A., Ambrożkiewicz, F., Samborowska, E., Błogowski, W., Sulikowski, T., Białek, A., Zawada, I., Dąbkowski, K., Mitrus, J., Karczmarski, J., Cybula, P., Paziewska, A., & Starzyńska, T. (2025). Plasma Bacterial Metabolites in Crohn’s Disease Pathogenesis and Complications. Nutrients, 17(1), 74. https://doi.org/10.3390/nu17010074