
Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age
 , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Assessment of Neonatal 25(OH)D3
2.4. Eczema Definitions
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Study Population
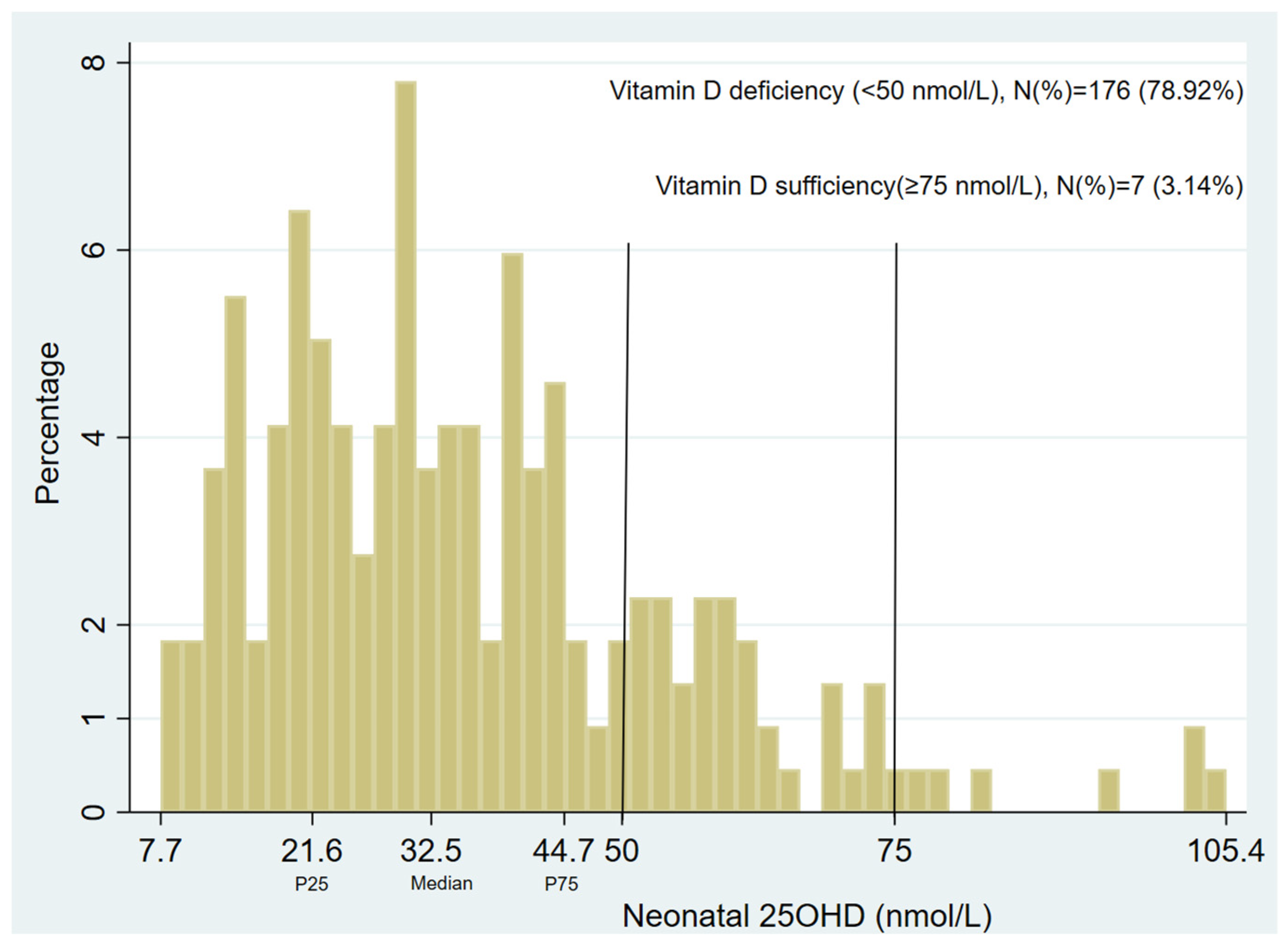
3.2. Neonatal Vitamin D Status
3.3. Neonatal Vitamin D Levels and 12-Month Prevalent Eczema at Age 1, 6, 12, 18, or 25 Years
3.4. Neonatal Vitamin D and Longitudinal Eczema Phenotypes up to 12 and 25 Years
3.5. Eczema/Sensitization Phenotypes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 25(OH)D3 | 25-hydroxyvitamin D3 |
| SPT | skin prick testing |
| aMOR | adjusted multinomial odds ratio |
| VDR | vitamin D receptors |
| MACS | Melbourne Atopy Cohort Study |
| DBS | dried blood spots |
| LC/MS | liquid chromatography–tandem mass spectrometry |
| BIC | Bayesian information criterion |
| GEE | generalized estimation equation |
| DAG | directed acyclic graph |
| VCGS | Victorian Clinical Genetics Services |
| SES | socio-economic status |
| HREC | Human Research Ethics Committee |
References
- Johansson, S.G.O.; Bieber, T.; Dahl, R.; Friedmann, P.S.; Lanier, B.Q.; Lockey, R.F.; Motala, R.; Ortega Martell, J.A.O.; Platts-Mills, T.A.E.; Ring, J.; et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J. Allergy Clin. Immunol. 2004, 113, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.J. Molecular mechanisms in atopic eczema: Insights gained from genetic studies. J. Pathol. 2017, 241, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Bieber, T. Atopic Dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Osborne, N.J.; Ukoumunne, O.C.; Wake, M.; Allen, K.J. Prevalence of eczema and food allergy is associated with latitude in Australia. J. Allergy Clin. Immunol. 2012, 129, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Poole, A.; Song, Y.; Brown, H.; Hart, P.H.; Zhang, G. Cellular and molecular mechanisms of vitamin D in food allergy. J. Cell. Mol. Med. 2018, 22, 3270–3277. [Google Scholar] [CrossRef]
- Plum, L.A.; DeLuca, H.F. The Functional Metabolism and Molecular Biology of Vitamin D Action. Clin. Rev. Bone Miner. Metab. 2009, 7, 20–41. [Google Scholar] [CrossRef]
- Heine, G.; Niesner, U.; Chang, H.-D.; Steinmeyer, A.; Zugel, U.; Zuberbier, T.; Radbruch, A.; Worm, M. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur. J. Immunol. 2008, 38, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Kay, J.; Gawkrodger, D.J.; Mortimer, M.J.; Jaron, A.G. The prevalence of childhood atopic eczema in a general population. J. Am. Acad. Dermatol. 1994, 30, 35–39. [Google Scholar] [CrossRef] [PubMed]
- de Lusignan, S.; Alexander, H.; Broderick, C.; Dennis, J.; McGovern, A.; Feeney, C.; Flohr, C. The epidemiology of eczema in children and adults in England: A population-based study using primary care data. Clin. Exp. Allergy 2021, 51, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J. Vitamin D and the Development of Atopic Eczema. J. Clin. Med. 2015, 4, 1036–1050. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, Á.; Hourihane, J.O.B.; Malvisi, L.; Irvine, A.D.; Kenny, L.C.; Murray, D.M.; Kiely, M.E. Antenatal vitamin D exposure and childhood eczema, food allergy, asthma and allergic rhinitis at 2 and 5 years of age in the atopic disease-specific Cork BASELINE Birth Cohort Study. Allergy 2018, 73, 2182–2191. [Google Scholar] [CrossRef] [PubMed]
- Baïz, N.; Dargent-Molina, P.; Wark, J.D.; Souberbielle, J.-C.; Annesi-Maesano, I. Cord serum 25-hydroxyvitamin D and risk of early childhood transient wheezing and atopic dermatitis. J. Allergy Clin. Immunol. 2014, 133, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.P.; Palmer, D.; Zhang, G.; Prescott, S.L. Cord blood 25-hydroxyvitamin D3 and allergic disease during infancy. Pediatrics 2012, 130, e1128–e1135. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Sullivan, T.R.; Skeaff, C.M.; Smithers, L.G.; Makrides, M. Higher cord blood 25-hydroxyvitamin D concentrations reduce the risk of early childhood eczema: In children with a family history of allergic disease. World Allergy Organ. J. 2015, 8, 28. [Google Scholar] [CrossRef]
- Jones, A.P.; D‘Vaz, N.; Meldrum, S.; Palmer, D.J.; Zhang, G.; Prescott, S.L. 25-hydroxyvitamin D3 status is associated with developing adaptive and innate immune responses in the first 6 months of life. Clin. Exp. Allergy 2015, 45, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Chawes, B.L.; Bonnelykke, K.; Jensen, P.F.; Schoos, A.M.M.; Heickendorff, L.; Bisgaard, H. Cord blood 25(OH)-vitamin D deficiency and childhood asthma, allergy and eczema: The COPSAC2000 birth cohort study. PLoS ONE 2014, 9, e99856. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.; Li, Y.; Shen, S.; Qiu, X.; Chang, C.-L.; Koplin, J.J.; Perrett, K.P.; Dharmage, S.C.; Lodge, C.J.; Lowe, A.J. Is antenatal or early-life vitamin D associated with eczema or food allergy in childhood? A systematic review. Clin. Exp. Allergy 2023, 53, 511–525. [Google Scholar] [CrossRef]
- Rabbani, S.; Afaq, S.; Fazid, S.; Khattak, M.I.; Yousafzai, Y.M.; Habib, S.H.; Lowe, N.; Ul-Haq, Z. Correlation between maternal and neonatal blood Vitamin D level: Study from Pakistan. Matern. Child. Nutr. 2021, 17, e13028. [Google Scholar] [CrossRef] [PubMed]
- van der Pligt, P.F.; Ellery, S.J.; de Guingand, D.L.; Abbott, G.; Della Gatta, P.A.; Daly, R.M. Maternal plasma vitamin D levels across pregnancy are not associated with neonatal birthweight: Findings from an Australian cohort study of low-risk pregnant women. BMC Pregnancy Childbirth 2023, 23, 67. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bachanier, L.B.; Zeiger, R.S.; et al. Six-Year Follow-up of a Trial of Antenatal Vitamin D for Asthma Reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Chawes, B.L.; Bonnelykke, K.; Stokholm, J.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.-M.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Effect of Vitamin D3 supplementation during pregnancy on risk of persistent wheeze in the offspring: A randomized clinical trial. JAMA J. Am. Med. Assoc. 2016, 315, 353–361. [Google Scholar] [CrossRef]
- El-Heis, S.; D’Angelo, S.; Curtis, E.M.; Healy, E.; Moon, R.J.; Crozier, S.R.; Inskip, H.; Cooper, C.; Harvey, N.C.; Godfrey, K.M.; et al. Maternal antenatal vitamin D supplementation and offspring risk of atopic eczema in the first 4 years of life: Evidence from a randomized controlled trial. Br. J. Dermatol. 2022, 187, 659–666. [Google Scholar] [CrossRef]
- Goldring, S.T.; Griffiths, C.J.; Martineau, A.R.; Robinson, S.; Yu, C.; Poulton, S.; Kirby, J.C.; Stocks, J.; Hooper, R.; Shaheen, S.O.; et al. Prenatal vitamin d supplementation and child respiratory health: A randomised controlled trial. PLoS ONE 2013, 8, e66627. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Vitamin D Status. 2023. Available online: https://www.health.gov.au/resources/pregnancy-care-guidelines/part-g-targeted-maternal-health-tests/vitamin-d-status#references (accessed on 1 June 2023).
- ACOG Vitamin D: Screening and Supplementation during Pregnancy. The American College of Obstetricians and Gynecologists 2011. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2011/07/vitamin-d-screening-and-supplementation-during-pregnancy (accessed on 24 January 2023).
- WHO Guideline. Vitamin D Supplementation in Pregnant Women; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Haider, S.; Granell, R.; Curtin, J.A.; Holloway, J.W.; Fontanella, S.; Arshad, S.H.; Murray, C.S.; Cullinan, P.; Turner, S.; Roberts, G.; et al. Identification of eczema clusters and their association with filaggrin and atopic comorbidities: Analysis of five birth cohorts. Br. J. Dermatol. 2023, 190, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Lopez, D.J.; Lodge, C.J.; Bui, D.S.; Waidyatillake, N.T.; Abramson, M.J.; Perret, J.L.; Su, J.C.; Erbas, B.; Svanes, C.; Dharmage, S.C.; et al. Establishing subclasses of childhood eczema, their risk factors and prognosis. Clin. Exp. Allergy 2022, 52, 1079–1090. [Google Scholar] [CrossRef] [PubMed]
- Thacher, T.D.; Clarke, B.L. Vitamin D insufficiency. Mayo Clin. Proc. 2011, 86, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.J.; Lodge, C.J.; Allen, K.J.; Abramsin, M.J.; Matheson, M.C.; Thomas, P.S.; Barton, C.A.; Bennett, C.M.; Erbas, B.; Svanes, C.; et al. Cohort Profile: Melbourne Atopy Cohort study (MACS). Int. J. Epidemiol. 2017, 46, 25–26g. [Google Scholar] [CrossRef] [PubMed]
- VCGS Newborn Bloodspot Screening Test. Available online: https://www.vcgs.org.au/tests/newborn-bloodspot-screening (accessed on 11 May 2021).
- Kvaskoff, D.; Ko, P.; Simila, H.A.; Eyles, D.W. Distribution of 25-hydroxyvitamin D3 in dried blood spots and implications for its quantitation by tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012, 901, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B.; Muthén, L.K. Integrating Person-Centered and Variable-Centered Analyses: Growth Mixture Modeling With Latent Trajectory Classes. Alcohol. Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef]
- Smith, C.A.; Sun, C.; Pezic, A.; Rodda, C.; Cameron, F.; Allen, K.; Craig, M.E.; Carlin, J.; Dwyer, T.; Lucas, R.M.; et al. Determinants of Neonatal Vitamin D Levels as Measured on Neonatal Dried Blood Spot Samples. Neonatology 2017, 111, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Morley, R.; Anderson, C.; Ko, P.; Burne, T.; Permezel, M.; Mortensen, P.B.; Norgaard-Pedersen, B.; Hougard, D.M.; McGarth, J.J. The utility of neonatal dried blood spots for the assessment of neonatal vitamin D status. Paediatr. Perinat. Epidemiol. 2010, 24, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, S.U.; Collier, F.; Pezic, A.; O’Hely, M.; Clarke, M.; Tang, M.L.K.; Burgner, D.; Vuillermin, P.; Ponsoboy, A.-L.; Barwon Infant Study Investigator Group. Maternal and Cord Blood 25-Hydroxyvitamin D3 Are Associated with Increased Cord Blood and Naive and Activated Regulatory T Cells: The Barwon Infant Study. J. Immunol. 2021, 206, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Suaini, N.H.A.; Loo, E.X.-L.; Peters, R.L.; Yap, G.C.; Allen, K.J.; Van Bever, H.; Martino, D.J.; Neo Goh, A.E.; Dharmage, S.C.; Colega, M.T.; et al. Children of Asian ethnicity in Australia have higher risk of food allergy and early-onset eczema than those in Singapore. Allergy 2021, 76, 3171–3182. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.J.; Koplin, J.J.; Ponsonby, A.L.; Gurrin, L.C.; Wake, M.; Vuillermin, P.; Martin, P.; Matherson, M.; Lowe, A.; Robinson, M.; et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef]
- Tanaka, K.; Miyake, Y.; Furukawa, S.; Arakawa, M. Pre- and Postnatal Smoking Exposure and Risk of Atopic Eczema in Young Japanese Children: A Prospective Prebirth Cohort Study. Nicotine Tob. Res. 2017, 19, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Susanto, N.H.; Lowe, A.J.; Salim, A.; Koplin, J.J.; Tang, M.L.K.; Suani, N.H.A.; Ponsonby, A.-L.; Allen, K.J.; Dharmage, S.C.; Erbas, B. Associations between grass pollen exposures in utero and in early life with food allergy in 12-month-old infants. Int. J. Env. Health Res. 2022, 32, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Xepapadaki, P.; Papadopoulos, N.G. Viral infections and allergies. Immunobiology 2007, 212, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Renz, H.; Skevaki, C. Early life microbial exposures and allergy risks: Opportunities for prevention. Nat. Rev. Immunol. 2021, 21, 177–191. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Estimates | Prevalent Eczema Age | |||||
|---|---|---|---|---|---|---|
| 1 Year | 2 Years | 6 Years | 12 Years | 18 Years | 25 Years | |
| n/N † | 70/220 | 63/214 | 26/174 | 25/155 | 47/196 | 32/122 |
| Unadjusted associations | ||||||
| OR (95% CI) | 1.05 (0.90–1.22) | 0.86 (0.72–1.02) | 0.86 (0.67–1.10) | 0.89 (0.69–1.14) | 1.13 (0.99–1.28) | 1.04 (0.88–1.22) |
| p-value | 0.539 | 0.087 | 0.239 | 0.361 | 0.067 | 0.648 |
| Adjusted associations (Model 1) ‡ | ||||||
| OR (95% CI) | 1.06 (0.90–1.24) | 0.86 (0.72–1.03) | 0.87 (0.67–1.12) | 0.91 (0.71–1.17) | 1.03 (0.85–1.26) | 0.94 (0.74–1.20) |
| p-value | 0.489 | 0.091 | 0.275 | 0.484 | 0.741 | 0.623 |
| Additionally adjusted for the season of birth (Model 2) § | ||||||
| OR (95% CI) | 1.04 (0.87–1.24) | 0.80 (0.65–0.98) | 0.81 (0.60–1.08) | 0.86 (0.65–1.14) | 1.01 (0.81–1.27) | 0.87 (0.67–1.14) |
| p-value | 0.658 | 0.032 | 0.155 | 0.301 | 0.909 | 0.318 |
| Estimates | Longitudinal Eczema Subclasses | ||||
|---|---|---|---|---|---|
| Early-Onset Persistent | Early-Onset- Resolving | Mid-Onset Persistent | Mid-Onset- Resolving | Minimal/No Eczema | |
| n/N † | 22/223 | 18/223 | 25/223 | 4/223 | 154/223 |
| Unadjusted associations | |||||
| MOR (95% CI) | 0.75 (0.57–0.98) | 1.22 (0.98–1.52) | 0.98 (0.81–1.18) | 0.73 (0.40–1.31) | 1.00 (Reference) |
| p-value | 0.039 | 0.073 | 0.828 | 0.282 | - |
| Adjusted associations (Model 1) ‡ | |||||
| aMOR ¶ (95% CI) | 0.74 (0.56–0.98) | 1.30 (1.05–1.62) | 0.97 (0.79–1.19) | 0.66 (0.35–1.24) | 1.00 (Reference) |
| p-value | 0.036 | 0.016 | 0.787 | 0.196 | - |
| Additionally adjusted for the season of birth (Model 2) § | |||||
| aMOR (95% CI) | 0.75 (0.55–1.02) | 1.21 (0.93–1.56) | 0.89 (0.70–1.13) | 0.68 (0.38–1.23) | 1.00 (Reference) |
| p-value | 0.068 | 0.150 | 0.351 | 0.206 | - |
| Estimates | Longitudinal Eczema Subclass | |||
|---|---|---|---|---|
| Early-Onset Persistent | Early-Onset-Resolving | Mid-Onset Persistent | Minimal/No Eczema | |
| n/N † | 21/223 | 20/223 | 31/223 | 151/223 |
| Unadjusted associations | ||||
| MOR (95% CI) | 0.76 (0.58–1.01) | 1.13 (0.89–1.43) | 1.03 (0.85–1.24) | 1.00 (Reference) |
| p-value | 0.055 | 0.305 | 0.750 | - |
| Adjusted associations (Model 1) ‡ | ||||
| aMOR ¶ (95% CI) | 0.76 (0.58–1.01) | 1.18 (0.93–1.50) | 1.03 (0.84–1.25) | 1.00 (Reference) |
| p-value | 0.057 | 0.170 | 0.780 | - |
| Additionally adjusted for the season of birth (Model 2) § | ||||
| aMOR (95% CI) | 0.76 (0.55–1.04) | 1.05 (0.86–1.42) | 0.96 (0.75–1.22) | 1.00 (Reference) |
| p-value | 0.088 | 0.444 | 0.730 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, R.; Lodge, C.J.; Koplin, J.J.; Lopez, D.J.; Erbas, B.; Abramson, M.J.; Eyles, D.; Ponsonby, A.-L.; Wjst, M.; Allen, K.; et al. Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age. Nutrients 2024, 16, 1303. https://doi.org/10.3390/nu16091303
Zeng R, Lodge CJ, Koplin JJ, Lopez DJ, Erbas B, Abramson MJ, Eyles D, Ponsonby A-L, Wjst M, Allen K, et al. Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age. Nutrients. 2024; 16(9):1303. https://doi.org/10.3390/nu16091303
Chicago/Turabian StyleZeng, Rong, Caroline J. Lodge, Jennifer J. Koplin, Diego J. Lopez, Bircan Erbas, Michael J. Abramson, Darryl Eyles, Anne-Louise Ponsonby, Matthias Wjst, Katrina Allen, and et al. 2024. "Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age" Nutrients 16, no. 9: 1303. https://doi.org/10.3390/nu16091303
APA StyleZeng, R., Lodge, C. J., Koplin, J. J., Lopez, D. J., Erbas, B., Abramson, M. J., Eyles, D., Ponsonby, A.-L., Wjst, M., Allen, K., Dharmage, S. C., & Lowe, A. J. (2024). Neonatal Vitamin D and Associations with Longitudinal Changes of Eczema up to 25 Years of Age. Nutrients, 16(9), 1303. https://doi.org/10.3390/nu16091303