
Risk of Gluten Cross-Contamination Due to Food Handling Practices: A Mini-Review


 , ,
, ,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
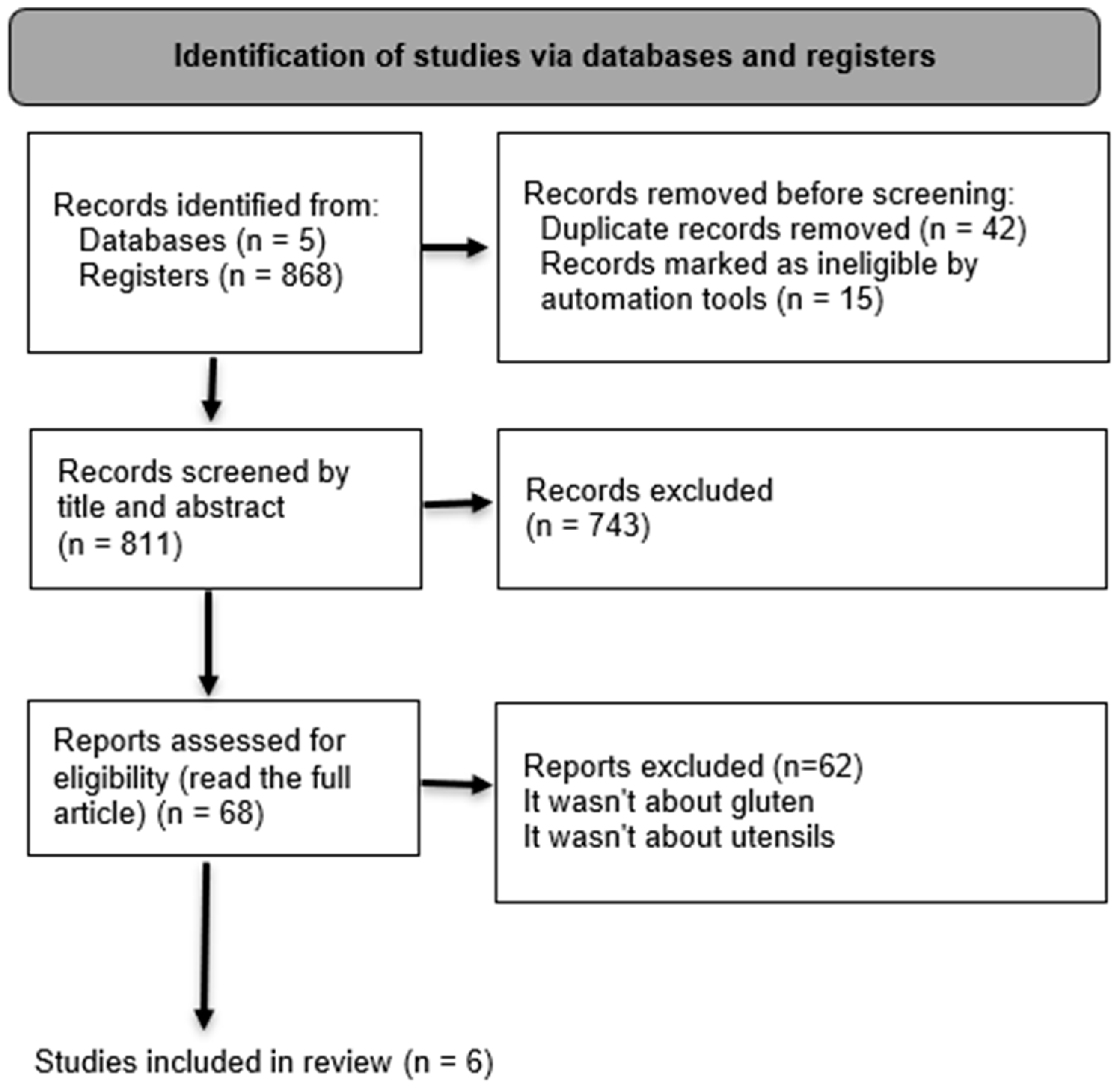
2.1. Search Strategy
2.2. Eligibility
2.3. Studies Selection
2.4. Data Collection
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Mosca, A.C.; Pellegrini, N. Toward an innovative gluten-free diet. In Biotechnological Strategies for the Treatment of Gluten Intolerance; Elsevier: Amsterdam, The Netherlands, 2021; pp. 131–153. ISBN 978-0-12-821594-4. [Google Scholar]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current guidelines for the management of celiac disease: A systematic review with comparative analysis. World J. Gastroenterol. 2022, 28, 154–175. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Hill, I.D.; Semrad, C.; Kelly, C.P.; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2023, 118, 59–76. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.; Leffler, D.; Catassi, C.; Green, P.; Kelly, C.; Ahuja, V.; Makharia, G. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Guennouni, M.; Elmoumou, L.; Admou, B.; Hazime, R.; Elkhoudri, N.; Hakmaoui, A.; Bourrahouat, A.; Hilali, A. Detection of gluten content in both naturally and labelled gluten-free products available in Morocco. J. Verbraucherschutz Leb. 2022, 17, 137–144. [Google Scholar] [CrossRef]
- Fasano, A. All disease begins in the (leaky) gut: Role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Research 2020, 9, 69. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef]
- Lindfors, K.; Ciacci, C.; Kurppa, K.; Lundin, K.; Makharia, G.; Mearin, M.; Murray, J.; Verdu, E.; Kaukinen, K. Coeliac disease. Nat. Rev. Dis. Primer 2019, 5, 3. [Google Scholar] [CrossRef]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; et al. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Tye-Din, J.A.; Daveson, A.J.M.; Ee, H.C.; Goel, G.; MacDougall, J.; Acaster, S.; Goldstein, K.E.; Dzuris, J.L.; Neff, K.M.; Truitt, K.E.; et al. Elevated serum interleukin-2 after gluten correlates with symptoms and is a potential diagnostic biomarker for coeliac disease. Aliment. Pharmacol. Ther. 2019, 50, 901–910. [Google Scholar] [CrossRef]
- Wieser, H. Chemistry of gluten proteins. Food Microbiol. 2007, 24, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Zandonadi, R.; Botelho, R.; Gandolfi, L.; Ginani, J.; Montenegro, F.; Pratesi, R. Green Banana Pasta: An Alternative for Gluten-Free Diets. J. Acad. Nutr. Diet. 2012, 112, 1068–1072. [Google Scholar] [CrossRef]
- Syage, J.A.; Murray, J.A.; Green, P.H.R.; Beach, N. Latiglutenase Improves Symptoms in Seropositive Celiac Disease Patients While on a Gluten-Free Diet. Dig. Dis. Sci. 2017, 62, 2428–2432. [Google Scholar] [CrossRef] [PubMed]
- Jnawali, P.; Kumar, V.; Tanwar, B. Celiac disease: Overview and considerations for development of gluten-free foods. Food Sci. Hum. Wellness 2016, 5, 169–176. [Google Scholar] [CrossRef]
- Zhu, X.; Zhao, X.-H.; Zhang, Q.; Zhang, N.; Soladoye, O.P.; Aluko, R.E.; Zhang, Y.; Fu, Y. How does a celiac iceberg really float? The relationship between celiac disease and gluten. Crit. Rev. Food Sci. Nutr. 2023, 63, 9233–9261. [Google Scholar] [CrossRef] [PubMed]
- Mocan, O.; Dumitraşcu, D.L. The broad spectrum of celiac disease and gluten sensitive enteropathy. Clujul Med. 2016, 89, 335. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.; Cellier, C.; Mulder, C.; Lundin, K. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.M.; Soltanizadeh, N.; Mirmoghtadaee, P.; Banavand, P.; Mirmoghtadaie, L. Gluten—free products in celiac disease: Nutritional and technological challenges and solutions. J. Res. Med. Sci. 2018, 23, 109. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Kyle, R.A.; Kaplan, E.L.; Johnson, D.R.; Page, W.; Erdtmann, F.; Brantner, T.L.; Kim, W.R.; Phelps, T.K.; Lahr, B.D.; et al. Increased Prevalence and Mortality in Undiagnosed Celiac Disease. Gastroenterology 2009, 137, 88–93. [Google Scholar] [CrossRef]
- Costa, A.F.; Sugai, E.; de la Paz Temprano, M.; Niveloni, S.I.; Vázquez, H.; Moreno, M.L.; Domínguez-Flores, M.R.; Muñoz-Suano, A.; Smecuol, E.; Stefanolo, J.P.; et al. Gluten immunogenic peptide excretion detects dietary transgressions in treated celiac disease patients. World J. Gastroenterol. 2019, 25, 1409–1420. [Google Scholar] [CrossRef]
- de Vargas, F.M.; Cardoso, L.T.; Didoné, A.; Lima, J.P.M.; Venzke, J.G.; de Oliveira, V.R. Celiac Disease: Risks of Cross-Contamination and Strategies for Gluten Removal in Food Environments. Int. J. Environ. Res. Public. Health 2024, 21, 124. [Google Scholar] [CrossRef]
- Shamir, R.; Heyman, M.; Koning, F.; Wijimenga, C.; Gutierrez-Achury, J.; Catassi, C.; Gatti, S.; Fasano, A.; Discepolo, V.; Korponay-Szabó, I.; et al. Celiac disease: Past, present, and future challenges: Dedicated to the memory of our friend and colleague, Prof David Branski (1944–2013). J. Pediatr. Gastroenterol. Nutr. 2014, 59, 2014. [Google Scholar] [CrossRef]
- Silvester, J.A.; Comino, I.; Kelly, C.P.; Sousa, C.; Duerksen, D.R. Most Patients With Celiac Disease on Gluten-Free Diets Consume Measurable Amounts of Gluten. Gastroenterology 2020, 158, 1497–1499.e1. [Google Scholar] [CrossRef]
- Raju, N.; Joshi, A.K.R.; Vahini, R.; Deepika, T.; Bhaskarachari, K.; Devindra, S. Gluten contamination in labelled and naturally gluten-free grain products in southern India. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2020, 37, 531–538. [Google Scholar] [CrossRef] [PubMed]
- CXS 118-1979; Standard for Foods for Special Dietary Use for Persons Intolerant to Gluten. Codex Alimentarius Commission: Rome, Italy, 2008.
- Hartmann, C.; Hieke, S.; Taper, C.; Siegrist, M. European consumer healthiness evaluation of ‘Free-from’ labelled food products. Food Qual. Prefer. 2018, 68, 377–388. [Google Scholar] [CrossRef]
- Wieser, H.; Segura, V.; Ruiz-Carnicer, Á.; Sousa, C.; Comino, I. Food safety and cross-contamination of gluten-free products: A narrative review. Nutrients 2021, 13, 2244. [Google Scholar] [CrossRef] [PubMed]
- Saturni, L.; Ferretti, G.; Bacchetti, T. The Gluten-Free Diet: Safety and Nutritional Quality. Nutrients 2010, 2, 16–34. [Google Scholar] [CrossRef]
- Rosell, C.M.; Barro, F.; Sousa, C.; Carmen, M. Cereals for developing gluten-free products and analytical tools for gluten detection. J. Cereal Sci. 2014, 59, 354–364. [Google Scholar] [CrossRef]
- Oliveira, O.; Zandonadi, R.; Gandolfi, L.; Almeida, R.; Almeida, L.; Pratesi, R. Evaluation of the Presence of Gluten in Beans Served at Self-Service Restaurants: A Problem for Celiac Disease Carriers. J. Culin. Sci. Technol. 2014, 12, 22–33. [Google Scholar] [CrossRef]
- Shah, S.; Akbari, M.; Vanga, R.; Kelly, C.P.; Hansen, J.; Theethira, T.; Tariq, S.; Dennis, M.; Leffler, D.A. Patient Perception of Treatment Burden is High in Celiac Disease Compared to Other Common Conditions. Off. J. Am. Coll. Gastroenterol. ACG 2015, 2014, 1304–1311. [Google Scholar] [CrossRef]
- Miller, K.; McGough, N.; Urwin, H. Catering gluten-free when simultaneously using wheat flour. J. Food Prot. 2016, 79, 282–287. [Google Scholar] [CrossRef]
- Falcomer, A.; Araújo, L.; Farage, P.; Monteiro, J.; Nakano, E.; Zandonadi, R. Gluten contamination in food services and industry: A systematic review. Crit. Rev. Food Sci. Nutr. 2018, 60, 479–493. [Google Scholar] [CrossRef]
- Wolf, R.; Lebwohl, B.; Lee, A.R.; Zybert, P.; Reilly, N.R.; Cadenhead, J.; Amengual, C.; Green, P.H.R. Hypervigilance to a Gluten-Free Diet and Decreased Quality of Life in Teenagers and Adults with Celiac Disease. Dig. Dis. Sci. 2018, 63, 1438–1448. [Google Scholar] [CrossRef]
- Weisbrod, V.; Silvester, J.; Raber, C.; McMahon, J.; Coburn, S.; Kerzner, B. Preparation of Gluten-Free Foods Alongside Gluten-Containing Food May Not Always Be as Risky for Celiac Patients as Diet Guides Suggest. Gastroenterology 2020, 158, 273–275. [Google Scholar] [CrossRef]
- Parsons, K.; Brown, L.; Clark, H.; Allen, E.; McCammon, E.; Clark, G.; Oblad, R.; Kenealey, J. Gluten cross-contact from common food practices and preparations. Clin. Nutr. 2021, 40, 3279–3287. [Google Scholar] [CrossRef]
- Korth, N.; Taylor, S.L.; Clarke, J.L. Gluten Cross-Contact in Restaurant-Scale Pasta Cooking. J. Food Prot. 2021, 84, 2159–2162. [Google Scholar] [CrossRef]
- Thompson, T.; Lyons, T.B.; Keller, A.; Jaffe, N.; Emerson-Mason, L. Gluten-Free Foods Cooked in Shared Fryers With Wheat: A Pilot Study Assessing Gluten Cross Contact. Front. Nutr. 2021, 8, 652039. [Google Scholar] [CrossRef]
- Studerus, D.; Hampe, E.I.L.G.; Fahrer, D.; Wilhelmi, M.; Vavricka, S.R. Cross-contamination with gluten by using kitchen utensils: Fact or fiction? J. Food Prot. 2018, 81, 1679–1684. [Google Scholar] [CrossRef]
- Vincentini, O.; Izzo, M.; Maialetti, F.; Gonnelli, E.; Neuhold, S.; Silano, M. Risk of Cross-Contact for Gluten-Free Pizzas in Shared-Production Restaurants in Relation to Oven Cooking Procedures. J. Food Prot. 2016, 79, 1642–1646. [Google Scholar] [CrossRef]
- R-Biopharm AG. RIDASCREEN® Gliadina, Art. No. R7001. Instructions. 2012. Available online: https://food.r-biopharm.com/wp-content/uploads/r7001-gliadin-2021-10-11.pdf (accessed on 11 October 2021).
- Akobeng, A.K.; Thomas, A.G. Systematic review: Tolerable amount of gluten for people with coeliac disease. Aliment. Pharmacol. Ther. 2008, 27, 1044–1052. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year | Country | Aim | Samples | Equipment/Utensils | Test |
|---|---|---|---|---|---|
| Vincentini et al., 2016 [41] | Italy | Identify safe procedures for preparing GF foods, comparing the gluten concentration of GF pizzas prepared in different shared production pizzerias, following different procedures | Pizza | Pizza oven | ELISA * |
| Studerus et al., 2018 [40] | Switzerland | This study was conducted to determine whether cross-contamination occurs through shared domestic kitchenware and, if so, which cleaning method is most reliable for avoiding this cross-contamination | Pasta and bread | Knife, colander, spoon, and ladle | ELISA; PCR ** |
| Weisbrod et al., 2020 [36] | United States of America | Quantify gluten transfer when GF foods are prepared alongside gluten-containing foods. A secondary aim was to assess the efficacy of cleaning methods for kitchen equipment/utensils. | Pasta, bread, cupcake | Stainless steel pans, colander, toaster | ELISA |
| Parsons et al., 2020 [37] | United States of America | Determine if three common food practices lead to gluten cross-contact in gluten-free processed foods | French fries, nuggets, bread, popular sandwich spreads (mayonnaise, jelly, peanut butter) | Fryer, toaster, knife | ELISA |
| Korth et al., 2021 [38] | United States of America | Determine whether gluten transfer occurs between traditional and gluten-free pasta when cooked simultaneously in the same water | Pasta | Cooking pan | ELISA |
| Thompson et al., 2021 [39] | United States of America | To help inform consumer recommendations by assessing the gluten levels of French fries without gluten-containing ingredients cooked in fryers shared with wheat. | French fries | Fryer | ELISA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damasceno, R.P.B.; Zandonadi, R.P.; Mendes, M.; Cunha Junior, L.C.; Raposo, A.; Teixeira-Lemos, E.; Chaves, C.; Farage, P. Risk of Gluten Cross-Contamination Due to Food Handling Practices: A Mini-Review. Nutrients 2024, 16, 1198. https://doi.org/10.3390/nu16081198
Damasceno RPB, Zandonadi RP, Mendes M, Cunha Junior LC, Raposo A, Teixeira-Lemos E, Chaves C, Farage P. Risk of Gluten Cross-Contamination Due to Food Handling Practices: A Mini-Review. Nutrients. 2024; 16(8):1198. https://doi.org/10.3390/nu16081198
Chicago/Turabian StyleDamasceno, Renatta Pereira B., Renata Puppin Zandonadi, Marcela Mendes, Luis Carlos Cunha Junior, António Raposo, Edite Teixeira-Lemos, Cláudia Chaves, and Priscila Farage. 2024. "Risk of Gluten Cross-Contamination Due to Food Handling Practices: A Mini-Review" Nutrients 16, no. 8: 1198. https://doi.org/10.3390/nu16081198
APA StyleDamasceno, R. P. B., Zandonadi, R. P., Mendes, M., Cunha Junior, L. C., Raposo, A., Teixeira-Lemos, E., Chaves, C., & Farage, P. (2024). Risk of Gluten Cross-Contamination Due to Food Handling Practices: A Mini-Review. Nutrients, 16(8), 1198. https://doi.org/10.3390/nu16081198